
Abstract
HIV nonoccupational postexposure prophylaxis (nPEP) has been prescribed to men who have sex with men (MSM) for decades, but the global situation of nPEP implementation among this population remains unclear. To understand nPEP awareness, uptake, and factors associated with uptake among MSM, we searched PubMed, Scopus, Embase, the Cochrane Library, and Web of Science for studies reporting nPEP implementation among MSM published before May 19, 2019. We estimated pooled rates and their 95% confidence intervals (CIs) of awareness, uptake using a random-effects model. We identified 74 studies: 3 studies (4.1%) from upper-middle-income regions and 71 (95.9%) from high-income regions. The pooled rate of nPEP awareness and uptake was 51.6% (95% CI 40.6–62.5%) and 6.0% (5.0–7.1%), respectively. Pooled uptake rate was higher in upper-middle-income regions [8.9% (7.8–10.0%)] than in high-income regions [5.8% (4.8–6.9%)]. Unprotected anal sex was the most common exposure (range: 55.0–98.6%, median: 62.9%). Pooled completion of nPEP was 86.9% (79.5–92.8%). Of 19,546 MSM prescribed nPEP, 500 HIV seroconversions (2.6%) were observed. Having risky sexual behaviors and history of sexually transmitted infections were associated with higher nPEP uptake, whereas insufficient knowledge, underestimated risk of exposure to HIV, lack of accessibility, and social stigma might hinder nPEP uptake. Awareness and uptake of nPEP among MSM worldwide are low. Further efforts are needed to combat barriers to access nPEP, including improving accessibility and reducing stigma. Seroconversions post-nPEP uptake suggest that joint prevention precautions aside from nPEP are needed for high-risk MSM. More evidence from low-income and middle-income regions is needed.
Introduction
Men who have sex with men (MSM) are disproportionately affected by HIV worldwide. 1 The high rates of HIV among MSM in both the resource-rich and resource-poor countries are among MSM of color. For example, in the United States, one in five (23%) MSM are living with HIV, whereas one in three (39%) black/African MSM are living with HIV. 2 In eastern and southern Africa, 13.7% of MSM were living with HIV between 2014 and 2018. 3 In Bangkok in Thailand, Yangon in Myanmar, and Yogyakarta in Indonesia, estimated HIV prevalence among MSM ranges from 20% to 29%. 4 High HIV incidence in MSM has been consistently reported in both high-income and low-income regions. 1,5 Behavioral interventions are effective but not sufficient to reduce incident HIV transmissions in this population. 6,7 More preventive measures against HIV are needed to augment combination strategies and curb HIV epidemic among MSM.
HIV postexposure prophylaxis (PEP) is a biomedical HIV preventional strategy for HIV-negative individuals that involves a 28-day course of antiretroviral medication taken within 48–72 h after exposure. 8,9 Despite the paucity of confirmative evidence from randomized controlled trials due to ethical issues, the effectiveness of PEP in reducing HIV transmission has been consistently reported in animal transmission models 10,11 and observational studies. 12 –14 For example, a case–control study found an 81% reduction in incident HIV infection among health care workers who took PEP after being exposed to HIV-contaminated blood. 13 Accumulating unequivocal evidence on the effectiveness of occupational PEP in health care settings led to the recommendation of nonoccupational PEP (nPEP). 15,16 nPEP use has been encouraged to prevent HIV after high-risk sexual exposure like sexual assault. 17 During 2001–2013, 49.7% of 505 sexual assault survivors in a reference hospital in Brazil were eligible to use nPEP. 18 During 2015–2018, 47.9% of 1032 sexual assault cases from an emergency department in Ottawa were eligible for nPEP, among whom 90.3% were female. 19 HIV nPEP began to be prescribed to MSM in the 1990s 20 –22 and currently it has been standardized in guidelines worldwide. 8,9,17,23 –25 Globally, MSM accounted for the majority of consultations about nPEP, ranging from 56.7% to 88.1%. 22,26 –36 Medical records showed that nPEP uptake was on the rise among MSM. 22,32,37 –39 However, the rate of awareness and uptake of nPEP among MSM worldwide have not been systematically characterized. A meta-analysis published in 2014 reported the nPEP adherence among MSM. 40 Higher adherence to better regimen was reported since then. 31,41 –43 Seroconversion after nPEP among MSM was documented in the US guideline in 2016, 17 and new evidence among MSM has emerged. 28,44 –49
To better understand the role that nPEP plays in HIV prevention in MSM and inform interventions to optimize nPEP provision in this population, we did a comprehensive systematic review and meta-analysis on the awareness, uptake, and the factors associated with nPEP uptake among MSM. We also updated the adherence to nPEP and the rate of HIV seroconversion after taking nPEP in MSM based on emerging evidence.
Methods
Search strategy and selection criteria
Our systematic review and meta-analysis were undertaken according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 50 and Meta-analysis of Observational Studies in Epidemiology (MOOSE) 51 guidelines. We searched the following databases for publications in English through May 19, 2019: PubMed, Scopus, Embase, the Cochrane Library, and Web of Science. We used search terms (“MSM” or “homosexual” or “gay” or “bisexual” or “men who have sex with men”) and (“PEP” or “nPEP” or “postexposure prophylaxis” or “post-exposure prophylaxis”) and (HIV or “human immunodeficiency virus”). References of retrieved full-text articles and other reviews were screened for additional eligible publications.
We included quantitative and qualitative studies that included MSM and reported one of the following information about nPEP: the rate of awareness and uptake, risk exposure of nPEP user, adherence to treatment guidelines [(1) completion: finishing 28-day drugs with or without dose missing; (2) full adherence: finishing 28-day drugs with zero dose missing], HIV seroconversion among MSM prescribed nPEP, and factors associated with nPEP uptake. Titles and abstracts of all retrieved articles were initially screened by two reviewers (Z.W. and H.Z.) independently to exclude ineligible studies, and disagreements were resolved by consensus among all investigators. Studies were excluded if MSM could not be distinguished from other populations (e.g., women and injection drug users). To ensure the high quality of included studies, we did not include conference abstracts. Studies without sufficient data to compute pooled estimates and studies with sample size <30 were included in this review but excluded from meta-analysis. In meta-analysis, we only pooled estimates measured by percentage and excluded those using different ones (i.e., median).
Data extraction
The following data were extracted: first author, year of publication, study period, research location, study design, HIV status at survey time and number of participants, nPEP relevant information (rate of awareness and uptake, risk exposure, adherence, seroconversion, and factors associated with nPEP uptake). For studies that assessed the awareness of nPEP using both “whether you have ever heard of nPEP” and more detailed questions, only the result measured by the former method was included in meta-analysis. For interventional studies aiming to promote nPEP awareness or uptake, or prospective cohort studies, only baseline data were extracted for the meta-analysis.
Quality assessment
The quality of cross-sectional data was assessed according to the criteria of observational studies recommended by the Agency of Healthcare Research and Quality (AHRQ), 52 and we applied a modified version to accommodate for this study. The quality of intervention trials and cohort studies was assessed by the Newcastle-Ottawa scale (the NOS) for cohort studies, 53 and a modified version was used. Two investigators (Z.W. and H.Z.) independently assessed the quality of each study and disagreements were resolved by discussion among all investigators.
Data analysis
For quantitative studies assessing the awareness, uptake, and completion of nPEP, we described raw rates for each study and calculated pooled point estimates with their corresponding 95% confidence intervals (CIs) with meta-analyses. We used DerSimonian–Laird inverse-variance method and Freeman–Tukey double-arcsine transformation for the proportion that was close to the margins. 54,55 A random-effects model was used to calculate pooled effect sizes because included studies differed in study design and thus we assumed a high potential for heterogeneity between included studies. 56 The I 2 statistic was used to estimate heterogeneity between included studies, with values of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. 57 Heterogeneity was explored with univariate and multi-variate meta-regression to estimate the fraction of the between-study variance (R 2 ) explained by participant and study characteristics (e.g., WHO regions, participant's HIV status). The characteristics that were significant in univariate models (p < 0.2) were included in multi-variate meta-regression. Subgroup analyses by participant and study characteristics were also conducted to investigate potential sources of heterogeneity and compare pooled estimates between subgroups. Egger's tests and funnel plots were used to test for publication bias. 58 Sensitivity analyses were conducted to detect potential outlier studies and assess the robustness of pooled association estimate by removing each estimate one at a time and recalculating the pooled estimates. For qualitative studies, we summarized the narrative results about facilitators and barriers for nPEP uptake under the thematic domains of individual and structural levels. Analyses were done using R version 3.5.2 software (package metaprop, metafor).
Results
Overview of studies
A total of 991 publications were assessed for eligibility, of which 491 publications were deleted due to duplication, and another 352 publications were excluded after title/abstract screening, resulting in 148 publications for full-text screening. Two additional studies were identified by reviewing the reference lists of included studies and other reviews. Finally, 74 studies (77 publications) conducted between June 1998 and August 2017 were included in this review (Fig. 1). Twenty-eight studies were conducted in the Americas (21 in the United States, 5 in Canada, and 2 in Brazil), 16 in Western Pacific Region (14 in Australia and 1 each in Singapore and China Taiwan), 26 in European Region (11 in the United Kingdom, 5 in France, 2 in the Netherlands and Italy, and 1 each in Spain, Finland, Switzerland, Ireland, Denmark, and multi-European country), 2 in African region (both in South Africa), and 1 each in South-East Asia Region (Thailand) and Eastern Mediterranean Region (Israel). Of the included studies, 3 were conducted in upper-middle-income regions, 71 were from high-income regions, and none from low-income or low-middle-income regions. The 74 included studies comprised 36 cross-sectional studies, 14 cohort studies, 7 intervention trials, and 17 retrospective case note reviews. Based on the AHRQ or the NOS, 35 (45.5%) publications were of high quality and 42 (54.5%) were of moderate quality (Supplementary Tables S1 and S2). Twenty-eight studies reported nPEP awareness among MSM, 30 reported nPEP uptake, 11 reported repeated nPEP uptake, 11 described the characteristics of MSM who used nPEP, 10 reported HIV risk exposure among MSM seeking nPEP, 12 reported nPEP adherence, and 14 studies reported HIV seroconversion among MSM who had been prescribed nPEP (Supplementary Tables S3–S9).
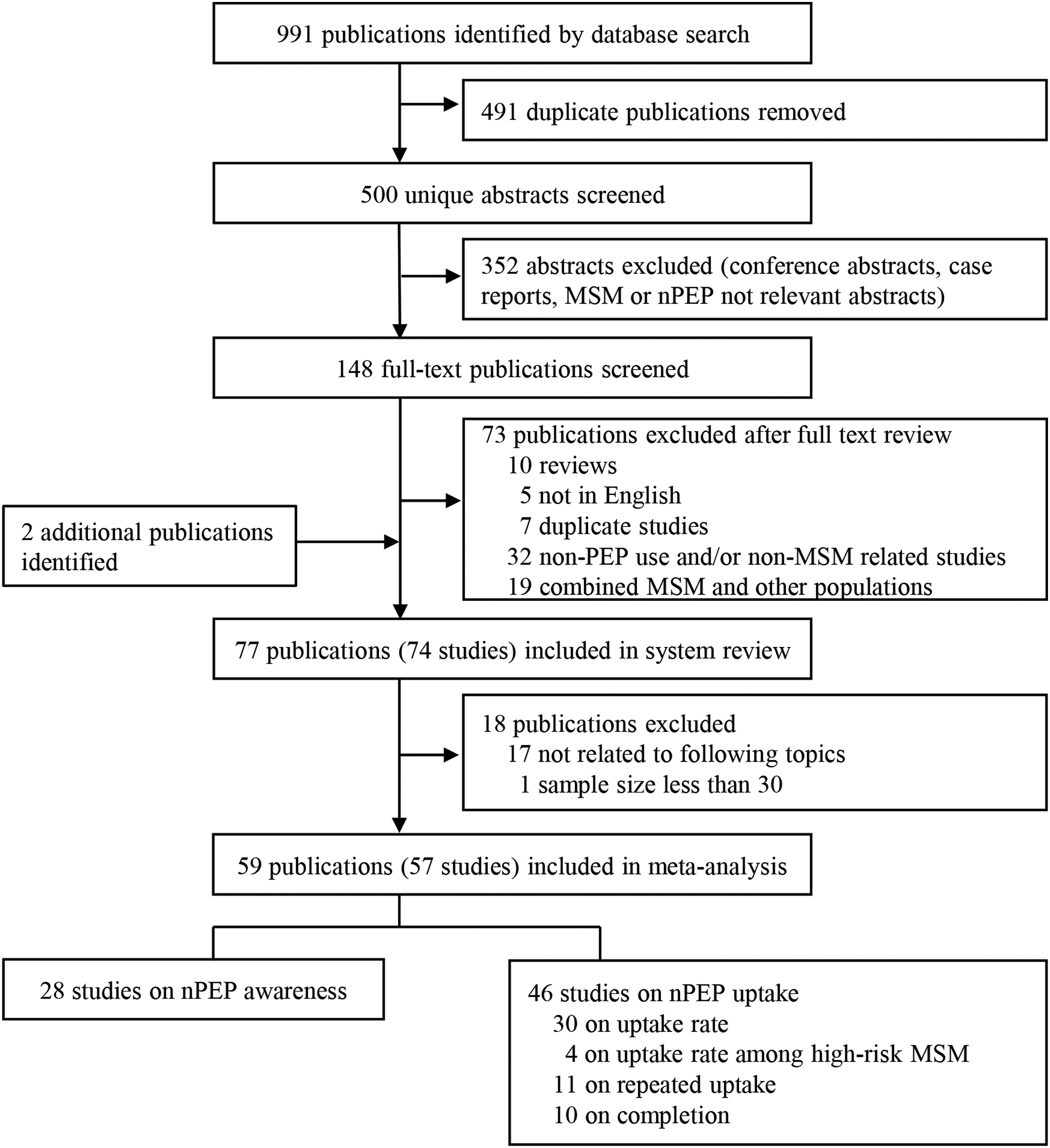
Flowchart of study selection. MSM, men who have sex with men; nPEP, nonoccupational postexposure prophylaxis.
Awareness of nPEP among MSM
Of the 28 studies 7,21,59 –85 that reported nPEP awareness among MSM, the rate of awareness ranged from 1.1% to 88.3% (median: 53.4%). After excluding one publication that did not provide sufficient data to compute pooled estimate, 60 the pooled rate of awareness of nPEP among MSM was 51.6% (95% CI 40.6–62.5%). Heterogeneity was high (I 2 = 99.9%, p < 0.01). The Egger's test (p < 0.05) and the asymmetrical funnel plot indicated publication bias (Supplementary Fig. S1). In sensitivity analyses, there were no significant differences in the pooled estimates after the removal of any one study (Supplementary Fig. S2). In the univariable meta-regression, neither participants' characteristics nor study characteristics could significantly explain the variation across studies (data not shown). In subgroup analyses (Fig. 2), awareness was not significantly varied by any characteristic explored (all p > 0.05). Nevertheless, awareness in upper-middle-income regions [62.7% (54.7–70.8%), k = 3] tended to be higher than in high-income regions [50.3% (38.5–62.4%), k = 27], although very limited data were available from African region and Southeast Asia and Latin America. Compared with the overall pooled estimate, awareness tended to be higher among HIV-positive MSM [69.6% (58.6–80.6%), k = 3] than among others.

Subgroup meta-analysis of nPEP awareness among MSM. One study could contribute more than one article, which could report more than one estimate. Each estimate was independent. MSM, men who have sex with men; nPEP, nonoccupational postexposure prophylaxis.
nPEP uptake among MSM
Rate of nPEP uptake
Of the 30 studies 7,28,44,59 –65,69–72,76 –79,84,86 –97 reporting nPEP uptake among MSM, the uptake rate ranged from 1.3% to 37.0% (median: 5.0%). After excluding one publication from the meta-analysis due to insufficient data, 60 the pooled nPEP uptake was 6.0% (95% CI 5.0–7.1%, I 2 = 99.3%, p < 0.01). The Egger's test (p < 0.05) and the asymmetrical funnel plot indicated publication bias (Supplementary Fig. S3). Sensitivity analyses indicated one study 44 could be an outlier. After excluding the study, the pooled estimate was attenuated to 5.4% (4.8–6.1%, I 2 = 98.8%, p < 0.01) (Supplementary Fig. S4). In the univariate meta-regression, region (R 2 = 34.9%, p < 0.01), recruitment method (R 2 = 6.8%, p = 0.03), and participant HIV status (R 2 = 32.8%, p < 0.01) significantly explained the variation across studies. In the multi-variate meta-regression, region, recruitment method, HIV status, and study period significantly explained the heterogeneity (data not shown). In subgroup analyses (Fig. 3), pooled estimate was higher in upper-middle-income regions [8.9% (7.8–10.0%), k = 3] than in high-income regions [5.8% (4.8–6.9%), k = 35], although three studies were available from African region and Southeast Asia and Latin America.
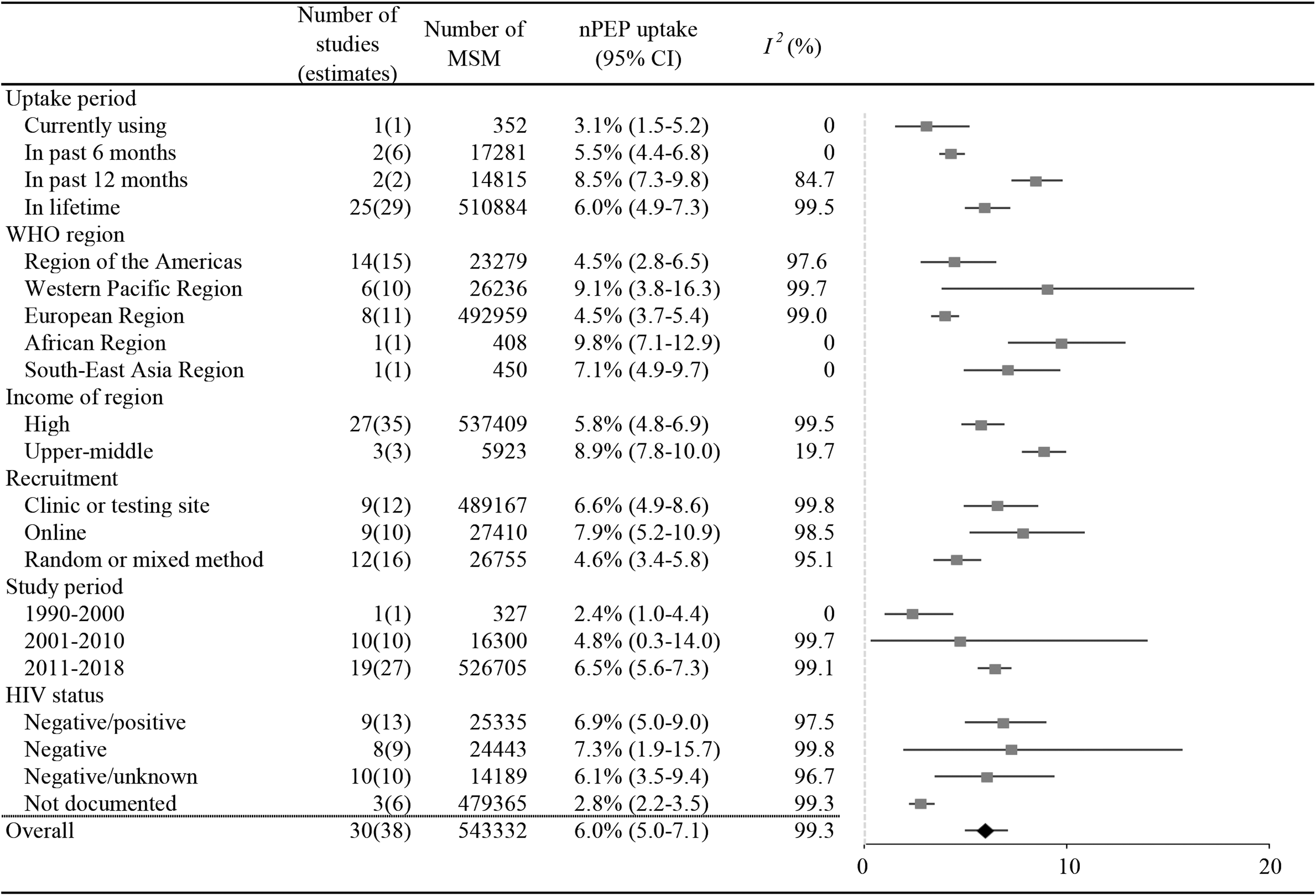
Subgroup meta-analysis of nPEP uptake among MSM. One study could contribute more than one article, which could report more than one estimate. Each estimate was independent. MSM, men who have sex with men; nPEP, nonoccupational postexposure prophylaxis.
Four studies reported the uptake of nPEP among MSM who engaged in high-risk sexual behavior. Among those who had unprotected anal intercourse with casual partners or substance use during anal sex in the past 6 months, only a minority (4.0–6.0%) used nPEP during the period. 60,64,93 Among MSM who were aware of nPEP and reported unprotected receptive anal intercourse, merely 3.2% had ever used it. 72 Overall, the pooled nPEP uptake rate among high-risk MSM was 5.0% (3.8–6.3%, I 2 = 27.1%, p = 0.25) (Supplementary Fig. S5).
Eleven studies 22,28,45,47,63,76,98 –102 reported repeated nPEP uptake (those who used nPEP more than once). The rate ranged from 5.5% to 40.8% (median: 18.0%), whereas the corresponding study duration ranged from 2.4 to 16.1 years. The pooled repeated uptake rate was 17.9% (14.2–21.5%, I 2 = 96.7%, p < 0.01) (Supplementary Fig. S6).
Risk exposure among nPEP users
Ten studies recorded HIV risk exposure that motivated MSM to use nPEP. Unprotected anal sex was the most common type of exposure (range: 55.0–98.6%, median: 62.9%), 41,45,47,99,101,103 –105 and unprotected receptive anal intercourse (range: 35.0–88.4%; median: 59.6%) 41,45,47,99,101,103 –106 was more frequent than unprotected insertive anal intercourse (range: 10.2–33.2%, median: 26.0%). 41,47,101,103 –106 Oral sex exposure was reported by 3.2% to 54.6% (median: 8.8%) of nPEP users. 47,101,104,106 Of the exposure in MSM, condomless sex intercourse including oral or anal ranged from 53.7% to 71.6% (median: 55.0%), 41,105,106 whereas condom failure ranged from 22.0% to 35.1% (median: 31.8%). 45,101,105,106 Only a few of the MSM prescribed nPEP were able to confirm the HIV serostatus of their partners (range: 6.8–36.7%, median: 28.4%). 35,99,101,106
Adherence to nPEP uptake and HIV seroconversion after nPEP uptake
Twelve studies 29,31,41 –43,59,99,102,107 –110 reported the proportion of MSM who completed the full 28-day course of nPEP. The completion rate of nPEP ranged from 44.4% to 94.1% (median: 90.5%). After excluding two publications from the meta-analysis due to different outcome measurement 59 or small sample size, 107 the pooled rate of completion was 86.9% (95% CI 79.5–92.8%; I 2 = 90.2%, p < 0.01) (Supplementary Fig. S7). The most common reason for premature withdrawal from nPEP was side effects, 43,102,108 such as nausea 102 and headache. 43 nPEP regimen varied in the type, number, and frequency of medicine intake. 31,41 –43,102,108 Notably, three Australian prospective cohort studies showed that once-daily emtricitabine–tenofovir-based regimen had a high completion rate (90.0–92.0%). 42,43,108 Three studies reported full adherence (range: 52.0–80.7%, median: 66.3%). 29,41,108
Fourteen studies 28,42,44 –49,69,99,101,102,108,110 reported a total of 500 HIV seroconversions among 19,546 MSM who had been prescribed nPEP. Nine of the 14 studies reported HIV incidence in MSM after nPEP uptake (range: 1.0–7.6 per 100 person-years, median: 2.2 per 100 person-years). 28,44 –47,49,69,99,101 Six of eight studies that reported the interval between nPEP initiation and HIV diagnosis indicated that the majority of seroconversions tested HIV-negative at >3 months post-nPEP uptake, 46 –49,99,101 implying that these seroconversions were unlikely due to nPEP failure.
Factors associated with nPEP uptake
Facilitators for nPEP uptake
Eleven studies examined the factors associated with nPEP uptake among MSM. 7,28,60,63,65,69,70,98,111 –113 Higher odds of nPEP uptake were associated with higher educational level, 63,70,111 older age, 63,70,111 gay identity, 70 and having health insurance. 7 Compared with nonusers, nPEP users tended to have more male sex partners 60,69,70,98,111,112 and engage in risk sexual behaviors such as inconsistent condom use 70,98,112 and having casual sex partners. 60,70 The likelihood of nPEP uptake increased with the risk of HIV transmission in their self-report sexual behaviors, 63,69 which was highest in unprotected receptive anal intercourse with HIV-infected partners. 69 nPEP users were more likely to use illicit drugs, 69,98,112 including nitrate 111 and methamphetamine, 65,111 to test for HIV 60 or sexually transmitted infections (STIs), 60 and to have been diagnosed with STIs, 70 such as chlamydia, 28,111 gonorrhea, 28,111 and syphilis 28 (Table 1).
Facilitators for Nonoccupational Postexposure Prophylaxis Use Among Men Who Have Sex with Men
aOR, adjusted odds ratio; aPRR, adjusted prevalence rate ratio; HR, hazard ratio; ND, not documented; STI, sexually transmitted infection.
Barriers to nPEP uptake
Engaging in high-risk sexual behavior did not necessarily entail nPEP. 114 MSM decided whether to take nPEP based on their risk assessment on HIV exposure. 115,116 A qualitative interview with 15 nPEP using MSM in the United Kingdom found that prior negligence of nPEP occurred when the risk of HIV infection was considered not high enough. 115 In a study among 200 MSM in Brazil who received 4-day nPEP pills and guidance, 10 of 11 participants who seroconverted did not initiate nPEP after unprotected sex for the following reasons: believing that their regular partners were HIV-negative or the risk of HIV transmission was not high enough to initiate nPEP. 102
Apart from personal factors, accessibility also affected nPEP initiation among MSM. An Irish study found that less than half (45.2%) of health care providers would prescribe nPEP to MSM who met nPEP eligibility. 117 Health care providers' concerns about the potential drug resistance and risk compensation may also lead to reduced prescription. 118 Lack of guidelines on HIV nPEP use may hinder nPEP implementation in MSM. Studies showed that nPEP prescription increased after the introduction of national guidelines. 29,66
Widespread and entrenched stigma against homosexuality in many cultures adversely affects the effective utilization of HIV prevention strategies among MSM. A majority of MSM reported that they felt being judged while discussing sexual exposure with health care providers, resulting in negative nPEP experiences. 119 An American study indicated that high state-level structural stigma was significantly associated with decreased awareness and uptake of nPEP. 120
Discussion
Our review found suboptimal awareness and uptake of nPEP among MSM. There were barriers at individual and structural levels hindering nPEP uptake in MSM, although the high nPEP adherence and low HIV seroconversion were somewhat reassuring.
We found that the awareness and uptake of nPEP among MSM worldwide were suboptimal: 51.6% (40.6–62.5%) and 6.0% (5.0–7.1%), respectively. These results were dominated by studies from high-income regions (i.e., the United States, Australia, and Europe). The prevalence of HIV is greater among MSM in low-income and middle-income regions, 1 and as a result MSM in these countries are more likely to be exposed to HIV. Higher rate of exposure may lead to higher uptake of nPEP. Our findings displayed a higher nPEP awareness and uptake in middle-income regions (three studies each in Brazil, South Africa, and Thailand) than in high-income regions. However, based on a small group of studies, nPEP awareness and uptake remain less clear in low-income and middle-income regions, which have heavy burden of HIV 1 and low coverage of health services, 6 and more research should focus on these regions.
Limited knowledge of nPEP among MSM hinders nPEP uptake. 70,115 nPEP is required to be used in 72 h, so pre-existing knowledge is essential to successful initiation. Our review found slightly more than half (51.6%) of MSM were aware of nPEP. Given the fact that most of the included studies simply reported the proportion of MSM who “ever heard of nPEP”, the proportion of MSM with sufficient knowledge of nPEP such as time to initiate and venues to access would be even smaller. The national data in Finland showed 21.2% of MSM knew about nPEP but only 13.5% responded correctly to the statements about nPEP on its efficacy and prerequisites. 78 Although nPEP awareness was not universal, MSM highlighted the benefit of the chemoprophylaxis 121 and held positive attitude toward nPEP. 122,123 In response to the high demands for nPEP among MSM, campaigns to improve nPEP knowledge in this population are necessary, particularly in regions where nPEP is available but awareness is low. Moreover, in addition to potential users, HIV-infected individuals should also be educated about nPEP as some of them might recommend nPEP to their casual sex partner. 124
In addition to limited knowledge, underestimated risk could also hamper nPEP uptake. A Danish survey found a noticeable gap between the number of MSM engaging in risk sexual behaviors and nPEP prescriptions for MSM, even if these MSM were highly aware of nPEP. 22 One possible explanation of this phenomenon could be that the perceived risk by these MSM was not high enough to motivate nPEP seeking. 22,60,70,102,115 To promote appropriate nPEP seeking after unprotected sex behavior, efforts are needed to improve the ability of risk assessment among MSM. 115 The most common reason of not using nPEP among MSM was the belief that their sex partners were HIV-negative. 102,115 In the context of unprotected sex, MSM are recommended to confirm serostatus of their partners including stable partners, whether before or after sexual contact. In response to perceived low risk of potential exposure, MSM should be well informed of exposures that are worth of nPEP requests, including but not limited to unprotected anal intercourse with HIV unknown men. 8,9
Health care providers play an important role in optimizing the implementation of nPEP in HIV prevention. MSM considered medical service providers as a reliable source of HIV prevention strategies. 125 Unfortunately, nPEP was only informed during HIV testing and counseling, 77 indicating a missed opportunity to educate potential users. Health care providers should assess HIV risk in each context of risk behavior among their clients and ensure that high-risk individuals could benefit from nPEP. Working as the gatekeeper, health care providers are required to be well informed of nPEP guidelines and antiretroviral drugs use, 126 but several studies reported negative results. 103,117,118 Assessment of nPEP prescription in an emergency room revealed one-fifth prescription decisions did not match with exposure risk. 74,103 Intervention campaigns for promoting nPEP could involve educating health care providers about the nPEP guideline. 66
We found a higher nPEP completion [86.9% (79.5–92.8%)] among MSM than the previous meta-analysis [65.9% (55.6–75.6%)]. 40 Because PEP completion was proved to vary by different drug regimens, and emtricitabine–tenofovir together with protease inhibitor had higher completion. 127 Compared with the meta-analysis, 40 most recent studies 31,41 –43 included in our review provided nPEP regimes with higher completion. The suboptimal completion mainly attributed to serious side effects. 42,102 MSM had higher full adherence to once-daily regimen (emtricitabine–tenofovir, once daily) than twice daily regimen (emtricitabine–tenofovir, once daily; raltegravir, twice daily). 43 Adherence to nPEP regimens is necessary to optimize effectiveness. 128 Optimized regimens with good tolerability and simplified usage may improve nPEP adherence. Options for nPEP regimens have also been increasing. For example, highly potent integrase inhibitors and C-C chemokine receptor type 5 antagonists are currently under clinical trials. 33 In the future, the availability of a variety of long-acting and safer drugs could potentially help improve coverage and adherence.
nPEP users normally have a higher risk profile than nonusers, such as more sex partners, inconsistent condom use, and illicit drugs use. In addition, approximately one-sixth [17.8% (14.2–21.5%)] nPEP users repeatedly sought nPEP, indicating that many men engaged in ongoing high-risk sexual behaviors, 129 and these men should actively approach pre-exposure prophylaxis (PrEP) use. 28,48,111,114 Some studies reported that MSM seeking nPEP were more likely to have subsequent HIV seroconversion 28,63 and their risk increased stepwise with the number of nPEP courses. 28 All these factors indicate the necessity of combining nPEP with other HIV precautions, such as behavioral interventions, psychosocial support, 129 drug use intervention, 112 and PrEP. 48,116 It is worthwhile to note that PrEP might also face similar barriers (e.g., poor knowledge and stigma 130,131 ) as PEP does when it comes to their scale-up among MSM. Moreover, PrEP requires long-term adherence to chemoprophylaxis, whereas nPEP needs to be adherent for a short interval. 128 Lessons learned from nPEP might provide insight into promoting of PrEP among MSM.
Our review has limitations. First, there were very limited studies on nPEP in Africa, Latin America, and Asia. This is because nPEP is not widely accessible in developing regions. In addition, available studies from other WHO regions represented the outcomes from specific countries, which may not represent the regional level. Second, heterogeneity between all pooled estimates was high. This may be because of drastic variations in nPEP service and HIV prevention strategies in different regions, and different study-level characteristics such as sampling methods. Finally, Egger's test suggested publication bias. The pooled estimates of nPEP awareness and uptake should be considered preliminary and should be further investigated when more data become available. Low levels of follow-up HIV testing 66 and recurrent exposure to HIV 129 have been documented, suggesting that cautions should be taken to interpret HIV seroconversion as the result of nPEP failure.
Our review showed that nPEP as an effective HIV prevention strategy was underutilized worldwide and understudied among MSM in developing regions. The reasons include insufficient knowledge about nPEP, inadequate risk assessment, health care providers' reluctance to prescribe, and a lack of accessibility. These gaps need to be addressed through efforts from both nPEP users and health care providers.
Footnotes
Authors' Contributions
Z.W. and H.Z. conceived the study, designed the protocol, conducted study selection, extracted the data, and did the quality assessment. Z.W., P.L., and S.F. contributed to statistical analysis. Z.W., T.Y., and H.Z. drafted the report. H.Q., S.F., P.L., Y.Z., and H.L. revised the report. All authors contributed to writing and review of the article and approved the final version.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the National Natural Science Foundation of China (Grant No. 81703278), the Australian National Health and Medical Research Council Early Career Fellowship (Grant No. APP1092621), the Sanming Project of Medicine in Shenzhen, China (Grant No. SZSM201811071), and High Level Project of Medicine in Longhua, Shenzhen, China (Grant No. HLPM201907020105).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.