
Abstract
Food insecurity (FI) contributes to HIV-related morbidity and mortality, but the mechanisms whereby FI negatively impacts HIV health are untested. We tested the hypothesis that FI leads to poor HIV clinical outcomes through nutritional, mental health, and behavioral paths. We analyzed data from Women's Interagency HIV Study (WIHS) among 1803 women living with HIV (WLWH) (8225 person-visits) collected from 2013 to 2015 biannually from nine sites across the United States participating in the WIHS. FI was measured with the US Household Food Security Survey Module. Outcomes included HIV viral nonsuppression, CD4 cell counts, and physical health status (PHS). We used longitudinal logistic and linear regression models with random effects to examine associations adjusting for covariates and path analysis to test nutritional, mental health, and behavioral paths. Increasing severity of FI was associated with unsuppressed viral load, lower CD4 counts, and worse PHS (all p < 0.05). Report of FI 6 months earlier was independently associated with most outcomes after adjusting for concurrent FI. For viral nonsuppression, the nutritional and behavioral paths accounted for 2.09% and 30.66% of the total effect, with the mental health path operating via serial mediation through the behavioral path. For CD4 count, the mental health and behavioral paths accounted for 15.21% and 17.0% of the total effect, respectively. For PHS, depressive symptoms accounted for 60.2% of the total effect. In conclusion, FI is associated with poor health among WLWH through different paths depending on the outcome. Interventions should target FI and its behavioral and mental health mechanisms to improve HIV outcomes.
Introduction
Food insecurity (FI), defined as having uncertain or limited availability of nutritionally adequate or safe food or the inability to procure food in socially acceptable ways, 1 affects 11.1% of US households, 2 and disproportionately impacts the households of racial/ethnic minorities and people living with HIV (PLWH). 3 FI is associated with worse physical health status (PHS), 4 decreased viral suppression, 3,5 worse immunologic status, 4,6 increased acute care use, 7 and increased mortality. 8 While some studies have been longitudinal, few assessed the temporal association between FI and HIV outcomes or effects of persistent exposure to FI on HIV outcomes. Similarly, few studies have assessed whether there is a dose–response relationship between FI severity and HIV outcomes.
While models have postulated the mechanisms through which FI affects HIV health outcomes, 3,9 no studies have comprehensively tested any of these mechanisms empirically. Understanding paths is critical to inform intervention development. This is because there are different programmatic and policy options for improving FI such as income transfer for food (e.g., Supplemental Nutrition Assistance Program), provision of prepared meals (e.g., soup kitchens, warm meal delivery), augmentation of the food supply (e.g., food pantries, food packages), vocational training programs, and increasing social security and unemployment benefits. These strategies may variably improve different aspects of FI (i.e., poor food quantity/quality, food supply anxiety, procuring foods in socially acceptable ways).
Elucidating the most important mechanisms will help select the most appropriate FI interventions for specific populations or health problems and improve the effectiveness of these programs. Understanding paths may also inform the type of supportive interventions—such as mental health services or adherence counseling—to pair with FI interventions, and can help address challenges such as dependency, stigma, or anxiety associated with receipt of food aid. 9,10
Most studies that have investigated health effects of FI among PLWH in resource rich settings have been comprised almost entirely of men. 3,7,11 Yet, women are at higher risk for FI in the United States and elsewhere, 9,12,13 and consequences of FI may differ by sex. For example, studies have shown that food-insecure women may engage in risky sexual behavior to cope with FI and are also at a higher risk for violence. 12,14 The mechanisms for how FI negatively affects health may also differ by gender. Consistent with this, one study in Uganda found that FI was associated with depressive symptoms among women and not men, 15 and depression may be an important mechanism through which FI worsens HIV outcomes. 9
To address these important gaps in the literature, we conducted a 3-year longitudinal study in the Women's Interagency HIV Study (WIHS) to understand the associations and temporal relationships of FI with HIV clinical outcomes among women. Drawing upon our published conceptual framework, 9,10 we assessed the nutritional, behavioral, and mental health mechanisms, through which FI may impact these outcomes. We hypothesized that (1) women with FI would have worse HIV clinical outcomes, and those with persistent FI would fare the worst; (2) there would be a dose–response relationship between increasing severity of FI and HIV outcomes; and (3) health behaviors and mental health would be the most important mediators of the negative impacts of FI.
Methods
Conceptual framework
Our framework posits that FI affects HIV outcomes through nutritional, mental health, and behavioral paths (Fig. 1). 9,10,16
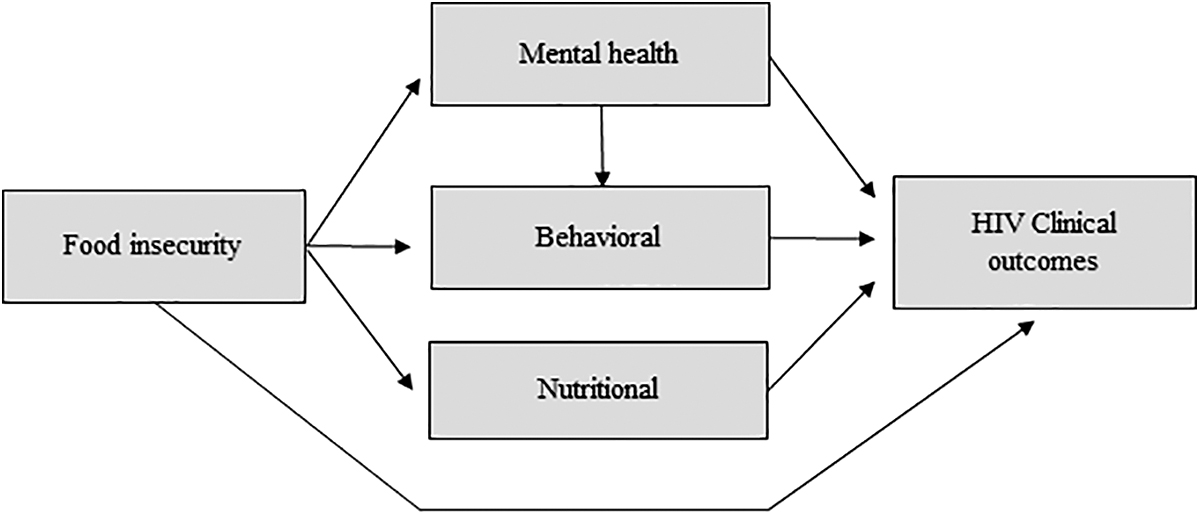
Hypothesized causal path.
Nutritional paths
Nationally representative studies of adults in North America have linked FI to inadequate dietary quality and poor nutritional status 17 –20 Weight loss, low body mass index (BMI), and low albumin have in turn been associated with disease progression and mortality in both untreated and antiretroviral therapy (ART)-treated PLWH. 9,21 FI also exerts negative effects on health through obesity, 22 when individuals are forced to cope with limited food access by consuming nutrient-poor, but energy-dense, cheaper foods. 23
Mental health paths
Qualitative studies in both PLWH and HIV-seronegative persons have identified feelings of helplessness, shame, and humiliation as central to the experience of FI. 16 Likewise, quantitative studies have confirmed an association of household FI with depression, anxiety, psychological distress, illicit substance use, 24 and worse overall mental health status. 9,13,25 Depression, poor mental health, and illicit substance use in turn predict ART nonadherence, higher viral loads, CD4+ T lymphocyte count decline, increased probability of AIDS-defining illness, and AIDS-related mortality. 9,26 –30
Behavioral paths
FI is associated with ART nonadherence, as measured by self-report, unannounced pill counts, and pharmacy refill records, 9,16,31 and with missed scheduled clinic visits. The reasons include competing demands between food and other resources, worse side effects when taking ART on empty stomachs, and stigma and discrimination while taking ART at free meal programs. 16,32 ART nonadherence and missed clinic visits, in turn, are well known determinants of worse morbidity and mortality among PLWH. 33
Study procedures
We analyzed longitudinal data from the WIHS, a multi-site prospective cohort study of women with or at risk for HIV established in 1994 to investigate the impact of HIV among women in the United States. 34 Since 1994, the WIHS has had three additional waves of recruitment in 2001–2002, 2011–2012, and 2013–2014. In the final wave of recruitment, four new sites in the Southern region of the United States were added in an attempt to enroll women representative of the age and race profiles of women living with HIV (WLWH) in the United States. 35 The WIHS currently follows women in nine sites: Bronx, NY; Brooklyn, NY; Washington, DC; Chicago, IL; San Francisco, CA; Chapel Hill, NC; Miami, FL; Birmingham, AL/Jackson, MS; and Atlanta, GA. 36 During semiannual interviews, the WIHS collects biological, clinical, demographic, and behavioral data using standardized instruments, physical examinations, and laboratory tests. Biological specimens include current CD4 count and HIV RNA viral load (measured using the TaqMan© assay).
From April 2013 to September 2015, the Food Insecurity Sub-Study (FISS) added data on comprehensive measures of food security, dietary intake, household savings, HIV stigma, and food support among all WIHS women. The first FISS visit for WIHS women started in 2013; women in the study averaged 4.4 visits out of a possible maximum of five visits. There were 8339 eligible person-visits among WLWH during the study period, of which 114 were missing the FISS module (1.4%). A total of 8225 person-visits comprised the analytic sample (1803 unique women). Given current guidelines recommending universal ART coverage, all women, regardless of ART status, were included in the analysis.
Participants provided written informed consent at each visit and were compensated for participation. This study was approved by the Institutional Review Board at each study site's institution and by the WIHS Executive Committee.
Primary explanatory variable
FI was measured at each visit of the substudy using the 18-item US Household Food Security Survey Module (HFSSM). 37 The HFSSM is the reference measure of population food security in the United States and has been validated in populations of women and other vulnerable populations. 38,39 We used the standard HFSSM scoring algorithm to categorize individuals as having high food security (i.e., food secure) and marginal, low, or very low food security (corresponding to mild, moderate, and severe FI). 39 Cronbach's alpha for the HFSSM in this sample is 0.91, indicating high internal consistency. FI was examined both concurrently (i.e., at same visit as outcome) and using a 6-month lag (i.e., at preceding visit) to investigate the effect of both current- and previous-visit FI.
Primary outcomes
This study examined three outcomes as measures of HIV health: (1) viral nonsuppression analyzed dichotomously (suppressed vs. nonsuppressed), with the lower limit of detection of <20 copies/mL as guided by the TaqMan assay and as used in the WIHS; 40 –42 (2) CD4 cell count (continuous, cells/mm3); and (3) PHS, as a continuous measure, measured using the physical health summary score of the 21-item Medical Outcomes Study HIV Health Survey (MOS-HIV); all of the outcome measures were collected at each of the five study visits of the substudy except the PHS score, which was collected annually at three visits. 43
As a sensitivity analysis, we examined viral nonsuppression using a cutoff of <200 copies/mL as has been used in some national HIV indicators such as CDC National HIV indicator and Ryan White Reporting. We performed confirmatory factor analysis using standard scoring algorithms to develop the PHS score; the score was normalized to have a mean of 0 and a standard deviation of 1, with higher scores indicating better PHS.
Covariates
Based on previous literature 3 and our conceptual framework 9,16 linking FI and HIV health outcomes, we considered these variables as potential confounders: age in years (continuous), race/ethnicity (non-Hispanic white [reference], Hispanic, non-Hispanic black/African American, or other), education (<high school degree or equivalent vs. ≥high school degree), annual income (≤$12,000 [reference], $12,001–$24,000, $24,001–$36,000, $36,001–$75,000, >$75,000), current child dependents in household (vs. none), time on ART (years), and marital status (married/in a partnership [reference], divorced/separated/widowed, never married and not in partnership, and other). All of the covariates—both time-varying and -invariant—were measured and assessed at each visit.
Potential mediators
We assessed nutritional, mental health, and behavioral mediators (Fig. 1) through which current FI may impact HIV outcomes. For the nutritional path, BMI (kg/m2) was measured during the anthropometric assessment and was included in the models as a continuous measure. Food frequency was collected annually and was measured using an adapted version of the 2000 National Health Interview Survey multifactor screener 44 and assessed as servings per day of the following food groups: fruit and vegetables, fat, carbohydrates, protein, and sugar. For the behavioral path, we assessed missed HIV clinical visits (which were not rescheduled) since the participant's last visit (yes vs. no) and ART adherence since last visit, measured by self-report (≥95% vs. <95%), which have been shown to be associated with higher odds of virologic suppression. 45,46
For the mental health path, we tested depressive symptoms as measured by the Center for Epidemiologic Studies-Depression (CES-D) scale, 47 mental health status, using the MOS-HIV, 43 both as continuous measures, as well as illicit drug use, defined as self-reported cocaine, crack, heroin, methamphetamine, hallucinogens, club drugs, nonprescribed narcotics, or any other illicit recreational drugs not including marijuana since last visit (vs. none). Based on a recent psychometric evaluation of the CES-D in WIHS that found invariance in scores between symptomatic and asymptomatic women with HIV, we used the full 18 item CES-D scale, 48 while also conducting an additional sensitivity analysis omitting somatic items from the scale as a robustness check.
Analysis
We obtained summary characteristics for the primary explanatory variable, outcomes, covariates, and hypothesized mediators by using data collected at the first visit of the WIHS FISS. We tested for interactions between race/ethnicity and food security status and found no evidence of interaction. We used multiple, two-level, longitudinal models to regress the HIV health outcomes at the current visit on FI at both current and previous visits, adjusting for covariates. For each individual, we included in the analyses all current visits, for which there was also FI assessed at the previous visit. Individual was included as a random effect to differentiate variation among and within women; current FI, previous FI, and covariates were included as fixed effects. To examine viral nonsuppression, we used logistic regression. As a robustness check, we also used a Tobit model with the logarithm of viral load accounting for the left-censored values in the undetectable range; 49 results from this model were similar to those for viral nonsuppression and are not reported.
We used linear regression models for both CD4 cell counts and PHS. We calculated the association of persistent FI (i.e., any category of FI that occurred at both the current and previous visit) by adding the natural log of the odds ratio for the current visit to the natural log for the previous visit, and then taking the exponent of the sum. This linear combination can be done with any set of two coefficients across the two visits, including declining or improving FI (e.g., marginal plus very low, low plus marginal). We show those who remained in the same two categories across visits (i.e., insecurity at two consecutive visits or very low FI at two consecutive visits).
All analyses were conducted using Stata 14 (StataCorp LP, College Station, TX). While our main analyses for all outcomes included all HIV-seropositive women in WIHS (n = 1803), results were very similar in a sensitivity analyses excluding the 116 women not on ART during the study period.
Using our conceptual framework, 9,16 we estimated nutritional, mental health, and behavioral paths (Fig. 1) through which current FI may affect HIV outcomes. We estimated individual mediation effects for all outcomes, selecting the most plausible mediators along each path based on literature and our prior work. 9,16 Given evidence that depressive symptoms may be on the causal path between FI and ART adherence, 16 we also estimated serial mediation of this path (i.e., FI→depression→adherence→HIV outcomes).
We selected the strongest mediators along each path for our final mediation models. For the nutritional path, BMI was the strongest mediator in the model with viral nonsuppression, while fruit and vegetable intake was strongest for CD4 cell count and PHS outcomes. For the behavioral and mental health paths, ART adherence and depressive symptoms, respectively, were the strongest mediators for all outcomes. We calculated the direct and indirect effects for each path by taking the products of the regression coefficients 50 of each leg of the path from fully adjusted mediation models that included one mediator from each of the three paths. Indirect effects were calculated only for paths where each leg was statistically significant (p < 0.05). We confirmed the assumption that each hypothesized mediator did not have a statistical interaction with FI for each outcome. 50
Ethics statement
This study was approved by the Institutional Review Board (IRB) at each study site's institution and by the WIHS Executive Committee. This includes the IRBs at the following institutes/organizations: Emory University, Albert Einstein College of Medicine, Montefiore Health Systems, The State University of New York Downstate Health Sciences University, Cook County Health & Hospital System (CORE Center), Rush University Medical Center, Hektoen Institute for Medical Research, Georgetown University, Maryland Department of Health, Inova Health System Foundation, University of Miami, University of California, San Francisco, University of Alabama at Birmingham, University of Mississippi Medical Center, and the University of North Carolina at Chapel Hill. Each participant consented before participating in any study activities.
Results
Among 1803 WLWH in WIHS, the median age was 48 years, 72% identified as non-Hispanic black, over half (53%) had annual household incomes under $12,000. Nearly half (44%) of the women experienced any FI (defined as marginal, low, or very low food security) and over half (59%) of all women were virally suppressed (Table 1).
Characteristics of HIV+ Participants at Study Entry Into the Women's Interagency HIV Study Food Insecurity Substudy, n = 1803
Median, IQR.
ART, antiretroviral therapy; BMI, body mass index; CES-D, Center for Epidemiologic Studies-Depression; FS, food security.
Viral nonsuppression
In unadjusted models, current low and very low food security and all categories of previous FI were associated with increased odds of viral nonsuppression (Table 2). In adjusted longitudinal models with both current and previous FI, current low and very low food security were associated with 1.41 (95% CI: 1.06–1.88) and 1.85 (95% CI: 1.31–2.60) higher odds of viral nonsuppression compared to those with high food security (Table 3). Previous low and very low food security were associated with 1.39 (95% CI: 1.04–1.85) and 1.49 (95% CI: 1.07–2.07) higher odds of viral nonsuppression, respectively (all p < 0.05). Having persistently low and very low food security were associated with 1.96 (95% CI: 1.32–2.90) and 2.75 (95% CI: 1.79–4.22) higher odds of viral nonsuppression, respectively, compared to those with persistently high food security (Table 4). In the sensitivity analysis examining a cutoff of <200 copies/mL, effect sizes between current food security and viral nonsuppression were similar, although more pronounced in the very low category (results not shown).
Longitudinal Bivariate Associations Between HIV Health Outcomes and Primary Predictor and Covariates, Women's Interagency HIV Study
ART, antiretroviral therapy; CI, confidence interval; FS, food security; OR, odds ratio; SE, standard error.
Longitudinal Adjusted Models, Concurrent and Lagged Analyses, Women's Interagency HIV Study
AOR, adjusted odds ratio; ART, antiretroviral therapy; CI, confidence interval; FS, food security; SE, standard error.
Association of Persistent Food Security Over the Previous Year with Main Outcomes, Women's Interagency HIV Study
Table 4 results are the exponentiated linear combinations of the natural log of the AORs for current and prior food security within each level (i.e., marginal, low, and very low) from Table 3, that is, Persistent FS = e(ln(AORcurrent)+ln(AORprior)). Estimates, CIs, and p-values obtained through postestimation commands for linear combinations in Stata.
Models adjusted for current and previous food security, age, race/ethnicity, income, education, child dependents, time on ARTs, CD4 nadir, and marital status.
AOR, adjusted odds ratio; ART, antiretroviral therapy; CI, confidence interval; FS, food security; SE, standard error.
CD4 cell counts
In bivariate analyses, marginal and very low food security were associated with lower CD4 cell counts compared to those with high food security (Table 2). In the adjusted linear regression models, current very low food security was associated with 22.31 lower CD4+ cells (SE: 10.45; p = 0.03) compared to women with high food security (Table 3), and previous FI was not significantly associated with CD4 cell counts.
Physical health status
In bivariate analyses, there was a strong dose–response relationship between FI and lower PHS (Table 2), which remained in adjusted models (Table 3). Current marginal, low, and very low food security were associated with −0.26 (SE: 0.05), −0.37 (SE: 0.05), and −0.55 (SE: 0.07) standard deviations from the mean PHS score, respectively. Previous low and very low food security were associated with −0.23 (SE: 0.05) and −0.37 (SE: 0.06) standard deviations from the mean PHS score, that is, lower PHS. Persistently marginal, low, and very low food security were associated with −0.34 (SE: 0.067), −0.60 (SE: 0.068) and −0.92 (SE: 0.075; all p < 0.001) standard deviations from the mean PHS score (Table 5).
Test of Nutritional, Mental Health, and Behavioral Paths from Food Insecurity to HIV Health Outcomes, Women's Interagency HIV Study
Food insecurity was examined as very low food security compared to not.
Food insecurity was examined as any food insecurity compared to none.
Models adjusted for current and previous food security, age, race/ethnicity, income, education, child dependents, time on ARTs, CD4 nadir, illicit drug use, and marital status
Fruit and vegetable intake was the primary mediator on the nutritional path investigated for CD4 count and physical health status, however, the paths were not statistically significant. BMI was the primary mediator on the nutritional path investigated for viral nonsuppression.
ART, antiretroviral therapy; BMI, body mass index; CES-D, Center for Epidemiologic Studies-Depression.
Mediation
The mediators accounted for 40.53% of the total effect of FI on viral nonsuppression (Table 5 and Fig. 2). The indirect paths through nutrition and behavior accounted for 2.09% and 30.66% of the association of FI with viral nonsuppression, respectively. Although the indirect path from FI to viral nonsuppression through mental health was not statistically significant, the indirect path from FI through mental health and then ART adherence was significant and accounted for 7.78% of the total effect of FI on viral nonsuppression.
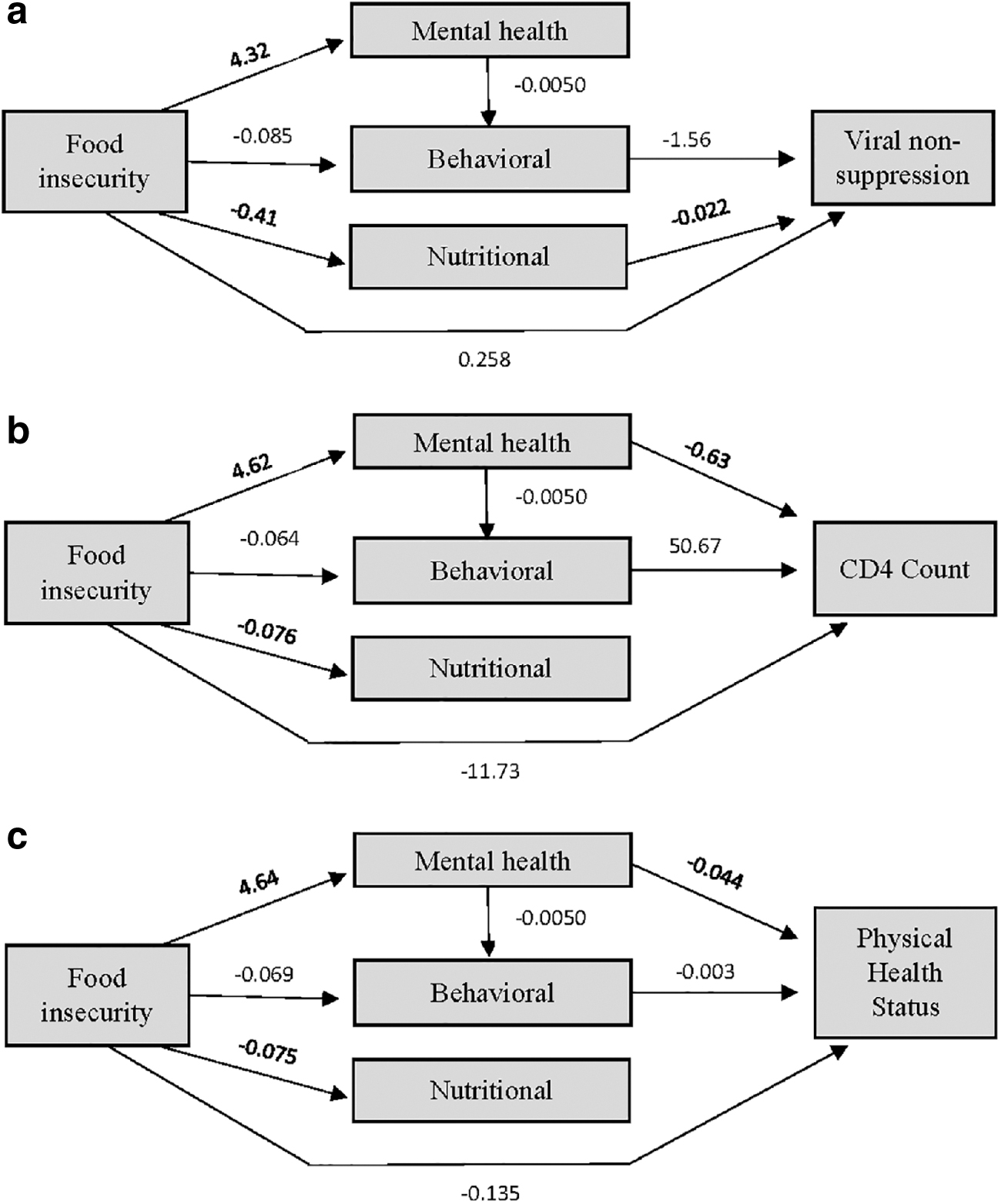
Paths from food security to HIV health outcomes.
The mediators explained 38.38% of the total effect of food security on CD4 cell count. The indirect paths through mental health and behavior accounted for 15.21% and 17.0% of the total effect, respectively. Mental health mediated the path from FI to ART nonadherence, accounting for 6.13% of the total effect on CD4 cell count.
The mediators accounted for 60.2% of the total effect of food security on PHS. In these models, the only statistically significant indirect path from FI was through mental health.
Discussion
In this longitudinal study among 1803 WLWH, FI was associated with higher viral nonsuppression, lower CD4 cell counts, and worse PHS. These findings support previous research that has documented worse HIV outcomes among food insecure individuals, 3 –7,9,11 including a cross-sectional study in the same cohort, 51 and extend previous findings in several important ways. First, while most previous work from the United States has focused on populations comprised largely of men or are cross sectional, 51 we report that these associations hold in a national longitudinal sample of women with HIV. Second, associations between FI and HIV clinical outcomes were related in a dose–response manner for most outcomes. Third, both current and previous FI were independently associated with many outcomes, suggesting that past FI may have ongoing deleterious impacts even if food security status improves. Women with persistent severe FI (both current and past visit) fared the worst in terms of their HIV outcomes.
Another important advance is that we tested the mechanisms through which FI may be linked with worse HIV outcomes using a novel conceptual framework, 9 and found that FI may operate through nutritional, mental health, and behavioral mechanisms to worsen HIV health. This work is consistent with findings from intervention studies showing that food support may improve both HIV and chronic disease outcomes by improving nutrition, 52 mental health, 53 and health behaviors. 52,53 Different mediators had more salience for different clinical outcomes, suggesting that distinctive strategies may be warranted for intervention depending on the targeted outcome.
In support of previous theory and qualitative research, 9,16 the indirect effect of the nutritional path was smaller compared to that of the behavioral and mental health path in terms of their impact on virologic and immunologic outcomes. This is not an unexpected finding given that ART adherence is the most important determinant of viral suppression and positive immunologic responses, 33 and that poor mental health is an important determinant of ART nonadherence, quality of life, and worse immunologic function. 28 Likewise, we found evidence of serial mediation, with a path from FI to depression to poor adherence to worse HIV virologic and immunologic outcomes.
These findings on mechanisms may also have relevance to conditions outside of HIV. Our previously published conceptual framework suggests that similar nutritional, mental health, and behavioral mechanisms may be important for metabolic and other chronic disease outcomes. 10 In contrast to our findings with HIV outcomes, literature suggests that nutritional mechanisms may be comparatively more important in mediating the negative impact of FI on metabolic and other chronic disease outcomes. 9,54 Future work could more comprehensively assess which mechanisms are most important for other chronic disease outcomes.
Our findings have important implications for policy and practice, and attest to the importance of addressing FI as part of comprehensive HIV care. In support of this, more HIV and chronic disease programs across the country are linking patients with medically appropriate food support. For example, the California legislature recently funded a statewide demonstration project to provide medically appropriate nutrition to food insecure, chronically ill individuals as a way to reduce morbidity and health care costs. 55 Similar interventions which seek to improve food security and nutritional status have been shown to reduce health care costs and be cost effective. 56
Given that ART nonadherence and depressive symptoms were the most salient mediators on the path from FI to worsened HIV health outcomes, multi-pronged interventions that address these mediators in addition to FI may be warranted. For instance, interventions that pair food support with adherence counseling to improve HIV indicators, or with mental health treatment to improve quality of life and overall PHS, may be most effective. In support of the need for multi-modal interventions, a recent analysis of over 1000 PLWH interviewed up to eight times between 2002 and 2015 found that the more linkages in their provider care networks (e.g., integration of housing services, food services, social services, and clinical care), the higher odds of increased viral suppression and ART adherence. 57
Interventions that address some of the root causes of FI (e.g., lack of stable livelihoods, lack of access to high-quality foods in low-income neighborhoods) may better address the mental health and behavioral mechanisms, through which FI negatively impacts health for three reasons. First, while food supplementation has been shown to be an effective intervention in many populations, including among PLWH, when people are dependent on clinics or food banks for food, they may feel ongoing anxiety about their food supply or that they are procuring their food in socially unacceptable ways. Second, experiences of stigma and discrimination are associated with receiving food stamps and other forms of food aid, 58 and when internalized, this stigma can contribute to depression and other negative mental health sequelae. 59 Third, addressing upstream causes of FI such as having a livable wage rather than midstream mediators or downstream consequences may lead to longer term and more pervasive gains, and can potentially help to interrupt the intergenerational transmission of FI and poverty.
This study had several limitations. The observational design limits causal inference. While the use of longitudinal data with lagged associations and incorporating potential mediators strengthens the plausibility of a causal connection, it is still possible that FI is partially a consequence rather than a cause of worse HIV outcomes, or that both FI and HIV outcomes are affected by common influences that could not be controlled. Our dietary measure was an imperfect measure of diet quality and did not capture macronutrient and micronutrient deficiencies, which may have underestimated the importance of nutritional mediators of FI. In addition, we did not have an objective measure of ART adherence on all WIHS women, and self-reported adherence may be susceptible to recall and social desirability bias. Finally, despite recent expansion of recruitment to include women in the US South, participants in the WIHS may not reflect US WLWH, particularly in terms of age and urban/rural residence.
In summary, these results provide strong evidence that FI is associated with poor health among WLWH in a dose–response manner and that FI influences HIV clinical outcomes via different paths depending on the outcome. Interventions should address FI and its behavioral and mental health mechanisms to improve HIV clinical outcomes.
Footnotes
Acknowledgments
We acknowledge and thank the participants in the WIHS for their contributions to the study overall and specifically to this research.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by a Women's Interagency HIV Study (WIHS) substudy grant from the National Institute of Mental Health, R01MH095683, and K24AI134326 (Weiser). Data in this article were collected by the WIHS. The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH). WIHS (Principal Investigators): UAB-MS WIHS (Michael Saag, Mirjam-Colette Kempf, and Deborah Konkle-Parker), U01-AI-103401; Atlanta WIHS (Ighovwerha Ofotokun and Gina Wingood), U01-AI-103408; Bronx WIHS (Kathryn Anastos), U01-AI-035004; Brooklyn WIHS (Howard Minkoff and Deborah Gustafson), U01-AI-031834; Chicago WIHS (Mardge Cohen and Audrey French), U01-AI-034993; Metropolitan Washington WIHS (Seble Kassaye), U01-AI-034994; Miami WIHS (Margaret Fischl and Lisa Metsch), U01-AI-103397; UNC WIHS (Adaora Adimora), U01-AI-103390; Connie Wofsy Women's HIV Study, Northern California (Ruth Greenblatt, Bradley Aouizerat, and Phyllis Tien), U01-AI-034989; WIHS Data Management and Analysis Center (Stephen Gange and Elizabeth Golub), U01-AI-042590; The WIHS is funded primarily by the National Institute of Allergy and Infectious Diseases (NIAID), with additional cofunding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), the National Cancer Institute (NCI), the National Institute on Drug Abuse (NIDA), and the National Institute on Mental Health (NIMH). Targeted supplemental funding for specific projects is also provided by the National Institute of Dental and Craniofacial Research (NIDCR), the National Institute on Alcohol Abuse and Alcoholism (NIAAA), the National Institute on Deafness and other Communication Disorders (NIDCD), and the NIH Office of Research on Women's Health. WIHS data collection is also supported by UL1-TR000004 (UCSF CTSA) and UL1-TR000454 (Atlanta CTSA).