
Abstract
Human papillomavirus (HPV) causes anal warts and anal squamous cell carcinoma (SCC). A higher incidence of anal cancer has been found among individuals previously diagnosed with anogenital warts. We aimed to investigate the association between anal warts and the presumed anal SCC precursor high-grade squamous intraepithelial lesion (HSIL), among participants in the Study of the Prevention of Anal Cancer (SPANC). SPANC was a longitudinal study of anal HPV infections and related lesions among gay and bisexual men (GBM) age 35 years and older, in Sydney, Australia. Anal cytology and high-resolution anoscopy were performed. Logistic regression was used to investigate the association between clinically diagnosed anal warts and intra-anal composite-HSIL (cytology and/or histology) at the baseline visit. The prevalence of HSIL within biopsies from intra-anal warts was calculated. Laser capture microdissection (LCM) and HPV-genotyping was performed on HSIL lesions. Among 616 participants at study entry, 165 (26.8%) and 51 (8.3%) had intra-anal and perianal warts, respectively. Warts were associated with composite-HSIL, even after adjustment for HIV status, age, lifetime receptive anal intercourse partner number, and smoking (perianal: aOR 2.13, 95% CI 1.17–3.87, p = 0.013; intra-anal: aOR 1.69, 95% CI 1.16–2.46, p = 0.006). HSIL was detected in 24 (14.5%) of 165 biopsies from intra-anal warts. Of 17 HSIL lesions, 16 (94.1%) had high-risk HPV detected by LCM. Anal warts were common. Prevalent anal warts were associated with composite-HSIL. HSIL may be detected within biopsies of intra-anal warts. Anal warts may be a useful addition to risk stratification for HSIL among GBM.
Introduction
Human papillomaviruses (HPV) cause anal warts 1 and anal squamous cell carcinoma (SCC). 2 The incidence of anal SCC has been increasing in many countries for several decades, 3 prompting calls for an anal cancer screening program to be considered among those individuals at highest risk. 4 HIV-positive men and women are at a higher risk of anal cancer than the general population, but the risk is highest among HIV-positive gay and bisexual men (GBM). 4 –6
Most anal SCC, and its precursor high-grade squamous intraepithelial lesion (HSIL), is associated with HPV genotypes with high oncogenic potential [high-risk HPV (HRHPV)]. 7,8 Anal wart is defined as a papillary proliferation with low-grade cytopathic features of HPV infection. 9 Anal warts are associated with HPV genotypes with low oncogenic potential [low-risk HPV (LRHPV)]. Anal warts are mostly diagnosed by visual inspection and guidelines recommend that biopsy is performed only if lesions are atypical 10 and/or are refractory to treatment. 11
A Danish registry study reported an association between a previous diagnosis of anogenital warts and subsequent risk of anal cancer. 12 Also, a number of studies report HSIL detection in biopsies or tissue sections from surgically excised intra-anal warts, 13 –18 however, these reports predate publication of the “Lower Anogenital Squamous Terminology (LAST) Standardization Project,” which provided consensus for histopathological nomenclature of HPV-associated lesions. Another more recent study found HSIL within one-fifth of biopsies from intra-anal condylomatous lesions in HIV-positive GBM. 19 Our aim was to investigate the association between anal warts and the detection of HSIL at baseline among HIV-negative and HIV-positive participants in the Study of Prevention of Anal Cancer (SPANC).
Methods
SPANC was a longitudinal study of HPV infection and related anal lesions among GBM age 35 years and older, in Sydney, Australia. The methodology of SPANC has previously been published. 20 Briefly, between September 2010 and August 2015, men who reported sex with another man in their lifetime were recruited predominantly from gay community social events/organizations and by participant referral. Men who reported previous high-resolution anoscopy (HRA) and/or anal cancer, were excluded. Self-reported anal symptoms did not affect study eligibility. Due to the possibility that previous diagnoses of anal abnormalities may affect clinician interpretation of anal lesions, only data from the baseline visit were included in the analysis.
Participants completed a computer-assisted self-interview (ACASI QDS, Bethesda, MD), which included questions about demographic factors, smoking, HIV-status, sexual behaviors, and history of anal warts. Anal swabs were collected for cytology and HPV detection. HRA (including application of 3% acetic acid and Lugol's iodine) was performed by one of six anoscopists. Before involvement in SPANC, all study anoscopists were required to undergo formal training, observe at least 25 HRA procedures, and then perform at least 50 HRAs under direct supervision of an experienced anoscopist. 20 Individual anoscopist results were also reviewed as part of a quarterly quality assurance program. Using a standardized data collection tool, the location (described by intra-anal “octant”), clinical features, and overall clinical impression of each anal lesion was recorded. For this analysis, anal lesions with a clinical impression of “wart” or “papillary lesion” or “exophytic LSIL” at the time of HRA were considered as wart diagnoses (and henceforth referred to as “warts”), irrespective of subsequent histology. Biopsy of any suspected squamous intraepithelial lesion (SIL) was performed. HPV genotyping was performed using Roche Linear Array (Roche Molecular Systems, Alameda, CA) and the Anyplex™ II (Seegene, Inc., Seoul, Korea) assay. Specimens positive for any HRHPV type on either Linear Array or Anyplex were considered positive. HRHPV types were defined as: HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68. 21 Anal cytology was reported according to the Bethesda System 22 and biopsies were reviewed in accordance with the LAST Project. 9 Cytology/histology “composite” groups were used. 23 Participants were diagnosed as “composite-negative” if there was no SIL detected on cytology and/or histology, or, if there were no suspected HPV-associated lesions and no biopsy collected. Where SIL was detected, participants were diagnosed with “composite-low grade squamous intraepithelial lesion (LSIL),” “composite-atypical squamous cells cannot exclude HSIL (ASCH),” or “composite-HSIL,” according to the highest grade of disease present at cytology and/or histology.
Laser capture microdissection (LCM) allows the detection of HPV types within individual histological lesions. As has been previously described, 24 LCM and HPV-detection/genotyping was performed on SPANC biopsy specimens with histologically confirmed HSIL.
Statistical analysis
Descriptive statistics were used to calculate the proportion of men who reported a history of anal warts and the prevalence of perianal and intra-anal warts at HRA. The proportion of participants within each composite group with prevalent intra-anal and perianal warts was calculated. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of intra-anal and perianal warts for the detection of composite-HSIL were calculated. Logistic regression analyses were performed to investigate the association between the detection of intra-anal and perianal warts at HRA with the outcome composite HSIL. Analyses were adjusted a priori for HIV status, age, and number of lifetime receptive anal intercourse (RAI) partners (previously identified as independent predictors of composite-HSIL 25 ), and current cigarette smoking. Further analyses among HIV participants included the following variables: Number of years since HIV diagnosis (<10, 10–20, >20 years), most recent CD4+ T lymphocyte count (<200, 201–500, >500 cells/mm3), nadir CD4+ T lymphocyte count (<200, 201–500, >500 cells/mm3), and latest HIV viral load (<50 or >50 copies/mL). Excluding lesions where there was a documented concomitant clinical impression of either HSIL and/or flat LSIL within the same octant, the prevalence of histologically confirmed HSIL within biopsies taken from intra-anal warts was calculated. The prevalence of HRHPV genotypes detected within histologically confirmed HSIL lesions (following LCM) was calculated.
Ethics approval for the conduct of the SPANC study was obtained from the St. Vincent's Hospital Ethics Committee (HREC/09/SVH/168). All participants provided informed consent.
Results
Among 617 participants enrolled in SPANC, 616 were included in this analysis. One person did not tolerate HRA and was excluded. The median age was 49 years (range 35–79) and almost all participants (n = 602, 97.7%) self-identified as “gay,” “bisexual,” or “homosexual.” Two hundred twenty-one (35.9%) participants were HIV-positive and 206 (93.6%) were taking antiretroviral treatment. Among 208 HIV-positive participants with available data, 135 (64.9%) reported their most recent CD4 count to be more than 500 cells/mm3, 63 (30.3%) reported 201–500 cells/mm3, and 10 (4.8%) reported less than 200 cells/mm3. Composite-HSIL (detected by cytology and/or histology) was diagnosed in 231 (37.5%) participants. 23
Diagnosis of warts
Of 616 participants who underwent HRA, 165 (26.8%, 97 HIV negative; 68 HIV positive) had intra-anal warts detected at HRA (described as: “wart” n = 148; “papillary lesion” n = 13; “exophytic LSIL” n = 4). Fifty-one (8.3%) participants had perianal warts, of whom 23 also had intra-anal warts. Among the 604 participants with available data, 273 (45.2%) reported a history of anal warts (150 HIV negative; 123 HIV positive), and 49 (8.1%) reported anal warts within the last year (26 HIV negative: 23 HIV positive). Of 188 participants with either perianal and/or intra-anal warts detected at HRA and available previous history data, 37 (19.7%) reported a history of anal warts within the last year.
Warts and diagnosis of SILs
The proportion of participants within each composite group with prevalent intra-anal and perianal warts is presented in Table 1. The prevalence of anal warts was higher among participants also diagnosed with composite-HSIL (perianal: 12.1%, intra-anal: 33.8%) compared with participants diagnosed as composite negative (perianal: 2.7%, intra-anal: 9.3%). HIV-positive participants with composite-HSIL were seven times more likely to have intra-anal warts than HIV-positive participants who were composite negative.
Prevalence of Perianal and Intra-Anal Warts Among Study of Prevention of Anal Cancer Participants, by Composite-Outcome Group
Row percentages used.
“Composite-negative”: no squamous intraepithelial lesion detected at cytology and/or histology, or, if there were no suspected HPV-associated lesions and no biopsy collected.
“LSIL” as highest grade of disease detected at cytology and/or histology.
“ASCH” as highest grade of disease detected at cytology and/or histology.
“HSIL” as highest grade of disease detected at cytology and/or histology.
ASCH, atypical squamous cells cannot exclude HSIL; HPV, human papillomavirus; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion.
Among HIV-positive participants with perianal warts and intra-anal warts, 15 (68.2%) and 41 (60.3%) also had composite-HSIL, respectively. Among HIV-negative participants with perianal warts and intra-anal warts, 13 (44.8%) and 37 (38.1%) also had composite-HSIL, respectively (Table 1).
The sensitivity, specificity, NPV, and PPV of the diagnosis of intra-anal and perianal warts at HRA for the detection of composite-HSIL are presented in Fig. 1. There was low sensitivity of perianal and intra-anal warts for composite-HSIL (12.1% and 33.8%, respectively). The specificity of perianal warts for composite-HSIL was high (94.0%). Compared with HIV-negative participants, the PPV of perianal and intra-anal warts was higher among HIV-positive participants (68.2% and 60.3%). Among HIV-negative participants, the NPV was higher (perianal: 69.3%; intra-anal: 52.2%) than the PPV (perianal: 46.2% and intra-anal: 38.1%). The association between perianal warts and composite-HSIL is presented in Table 2. In univariable analysis, perianal warts, HIV positivity, and higher number of lifetime RAI partners were significantly associated with composite-HSIL. In the multivariable analysis, perianal warts, HIV positivity, and higher number of lifetime RAI partners remained significant.
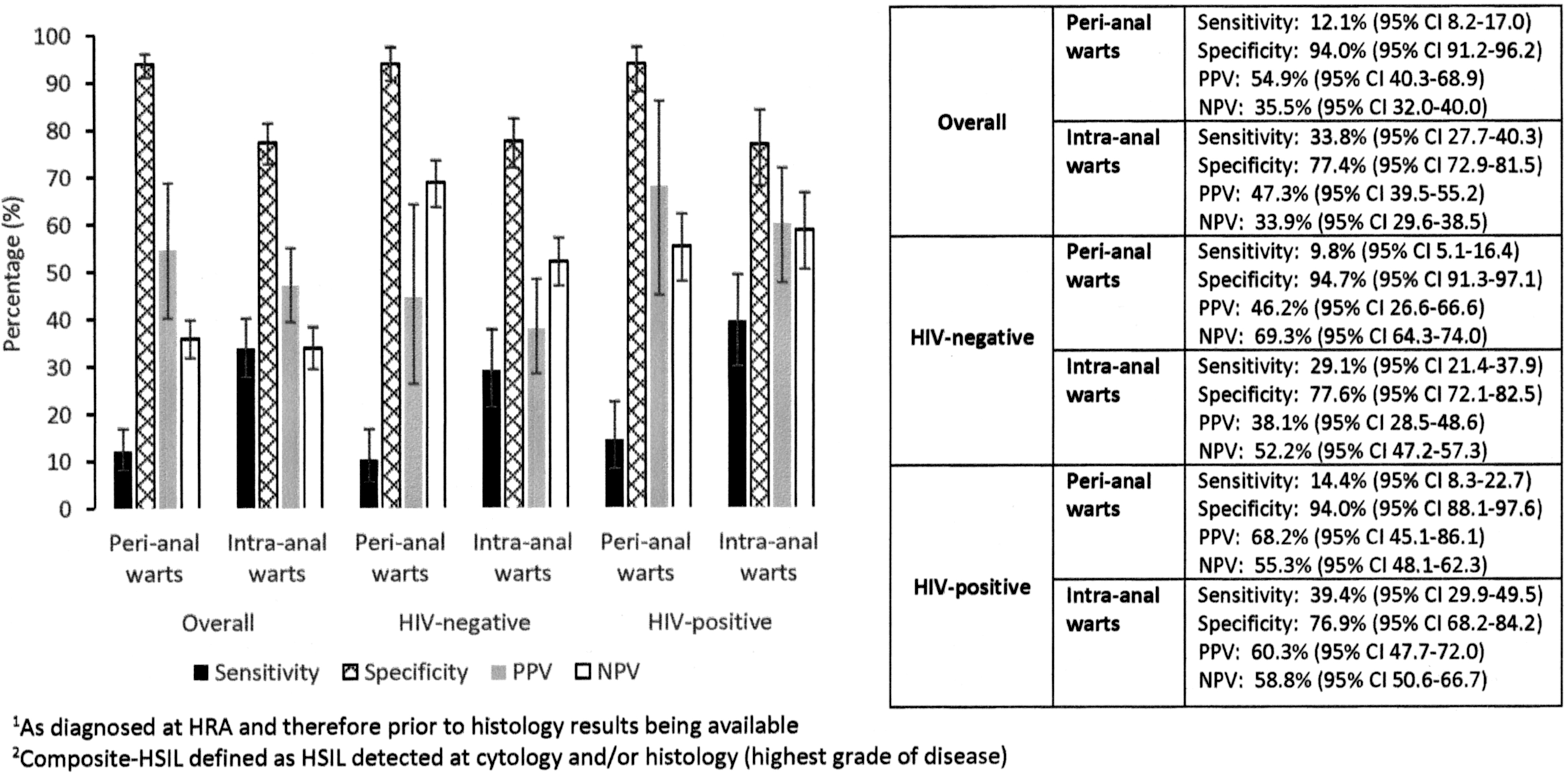
Sensitivity, specificity, PPV, and NPV of prevalent perianal and intra-anal warts 1 at HRA for the detection of composite-HSIL. 1 As diagnosed at HRA and therefore before histology results being available. 2 Composite HSIL defined as HSIL detected at cytology and/or histology (highest grade of disease). HRA, high-resolution anoscopy; HSIL, high-grade squamous intraepithelial lesion; NPV, negative predictive value; PPV, positive predictive value.
Univariable and Adjusted Analyses for the Association Between the Detection of Perianal Warts and the Outcome Composite High-Grade Squamous Intraepithelial Lesion
Row percentages used.
aOR, adjusted odds ratio; CI, confidence interval; HRA, high-resolution anoscopy; OR, odds ratio; RAI, receptive anal intercourse.
The association between intra-anal warts and composite-HSIL is presented in Table 3. In univariable analysis, intra-anal warts, HIV positivity and higher number of lifetime RAI partners were significantly associated with composite-HSIL. In the multivariable analysis, intra-anal warts, and higher number of lifetime RAI partners remained significant.
Univariable and Adjusted Analyses for the Association Between the Detection of Intra-Anal Warts and the Outcome Composite High-Grade Squamous Intraepithelial Lesion
Row percentages used.
aOR, adjusted odds ratio; HRA, high-resolution anoscopy; OR, odds ratio; RAI, receptive anal intercourse.
Among HIV-positive participants, in univariable analysis there was no significant association between composite-HSIL and number of years since HIV diagnosis (p = 0.654), most recent CD4+ T lymphocyte count (p = 0.174), nadir CD4+ T lymphocyte count (p = 0.164), or latest HIV viral load (p = 0.768). In multivariable analysis, following the addition of these variables, there remained a significant association between composite-HSIL and the detection of intra-anal warts (aOR 2.27 95% CI 1.16–4.45, p = 0.017), but the association between composite-HSIL and the detection of perianal warts was no longer significant (aOR 1.72 95% CI 0.58–5.09, p = 0.330). However, there were only 22 HIV-positive participants with perianal warts detected.
Clinical/histological correlation and HPV findings
Among 165 participants with anal warts, 160 had the location of anal wart recorded by intra-anal octant. Among these 160 participants, warts were detected in 260 intra-anal octants and a biopsy result was available from 212 octants (81.5%; 129 HIV negative; 83 HIV positive). Of these 212 biopsies, 47 (22.2%) were taken from an octant with a clinical impression of both wart and HSIL and/or flat LSIL and were therefore excluded (HSIL: n = 21, flat LSIL: n = 24; HSIL and flat LSIL: n = 2). The highest histological grade of SIL detected within the remaining 165 biopsies (118 participants), where the clinical impression was wart only, was 27 (16.4%) negative for SIL (HIV negative: 18.4%; HIV positive: 12.9%), 114 (69.1%) LSIL (flat and/or exophytic) (HIV negative: 71.8%; HIV positive: 82.3%) and 24 (14.5%) HSIL (HIV negative: 13.6%; HIV positive: 16.1%). Among 22 participants with HSIL detected (24 biopsies), 14 (63.6%) had at least one HRHPV type detected in the anal canal swab (1 HPV16 only; 8 other HRHPV only; 5 HPV16; and other HRHPV) and 20 (90.9%) had at least one LRHPV type detected (1 HPV6/11 only, 8 HPV6/11 and other LRHPV; 11 other LRHPV only). Following LCM, an HPV genotype was identified within 17 HSIL lesions: 3 HPV16, 13 other HRHPV types (18, 31, 33, 45, 51, 56, 58, 66, 68) and 1 “probable” HRHPV (HPV53).
Discussion
Anal warts were extremely common among SPANC participants, with one in two men having a history of anal warts and nearly one in three diagnosed with prevalent anal warts. Three quarters of anal wart diagnoses were intra-anal, without concurrent perianal warts. Clinical diagnosis of intra-anal and perianal warts was associated with concurrent composite-HSIL, even after adjustment for HIV status, age, lifetime RAI partner number, and cigarette smoking. More than two-thirds of HIV-positive participants with perianal warts had HSIL detected. Intra-anal HSIL was detected within one in seven biopsies from lesions diagnosed clinically as wart at HRA. Using LCM, a single HRHPV type was detected in nearly all HSIL lesions, and most were other HRHPV types.
A previous diagnosis of warts was three times as high in this cohort of GBM (45%) than reported in an earlier study of HIV-negative GBM in Sydney (16%). 26 This may be because SPANC participants were older 20,26,27 or because SPANC included both HIV-negative and HIV-positive participants. 28,29 In addition, men previously diagnosed with anal warts may have been more likely to enrol in SPANC, as it was described to potential participants as a study of HPV-related anal lesions.
The prevalence of intra-anal warts among HIV-positive SPANC participants (31%) is consistent with the one-third prevalence found among 200 GBM attending for HIV care in France (one-quarter of whom had advanced HIV). 30 One-quarter of HIV-negative SPANC participants also had intra-anal warts, which is higher than the 8% prevalence found among 213 HIV-negative men attending an HIV testing center in the USA, although it is 30 years since this study was undertaken. 17 Our finding that three quarters of participants with prevalent anal warts did not report a history of anal warts within the last year suggests that many participants were unaware of the presence of warts, perhaps because warts are mostly asymptomatic and most participants had intra-anal warts only. Perianal warts were less common (8%) than intra-anal warts among SPANC participants. A higher prevalence of perianal warts was found among HIV-negative men who have sex with men (MSM) and transwomen (25%) in Peru, 31 which may be because SPANC participants were older, 32 or alternatively may have received recent wart treatment.
The diagnosis of intra-anal and perianal warts at HRA were both associated with the detection of concurrent composite-HSIL. In previous analyses, we identified an association between a recent history of anal lump and a higher burden of HSIL, which we hypothesized may be because of coinfection with multiple HPV types and concomitant anal warts. 33 A history of anogenital warts is associated with subsequent development of anal cancer, 12,34 which may be explained by shared risk factors for the acquisition of low and high-risk HPV types, 27,34 –37 smoking, 12,36 or differences in cell-mediated immunity. 38 However, in our analysis, the association between intra-anal warts and HSIL remained significant after adjustment for the number of RAI partners and smoking.
The detection of perianal or intra-anal warts had low sensitivity for HSIL (12% and 34%, respectively). Nearly two-thirds of HIV-positive participants with prevalent anal warts had composite-HSIL detected, which is higher than the reported PPV of HRHPV for HSIL (19–57%). 39 –41 The lower specificity of intra-anal warts (69%) when compared with the detection of perianal warts (94%) may reflect the challenges of anoscopy, 42 which is limited by the anatomy of the anal canal and coexistent anal pathology. 43
The prevalence of HSIL within biopsies from intra-anal warts in HIV-positive participants (16%) is consistent with a study of HIV-positive GBM in Amsterdam, where 18% of condylomatous intra-anal lesions biopsied had HSIL detected. 19 The prevalence among HIV-negative SPANC participants was only slightly lower (13%), despite a higher overall prevalence of composite-HSIL among HIV-positive participants. 25 To our knowledge, ours is the first study to report the prevalence of HSIL within biopsies from clinically diagnosed intra-anal warts among HIV-negative GBM. Compared with our findings, a higher prevalence of HSIL has been detected within surgically excised anal warts (HIV positive: 16–44%, 13 –15,18 HIV negative: 6–26% 13 –15 ), however, surgical management is more likely to be offered if there is a large burden of warts, and/or atypical features. Also, comparison with these studies is limited by the use of whole tissue sections for histological analysis rather than discrete biopsies of warts. These studies predated publication of the LAST consensus for histopathological nomenclature of HPV-associated lesions, which may have resulted in overestimation of the prevalence of HSIL without the routine use of biomarkers such as p16. 9,44 HSIL was found within 22% and 30% of biopsies from discrete and circumferential warts, respectively, in a study of MSM presenting for HIV testing in the USA, however, this study also predated the LAST criteria. 17 The finding of HSIL within biopsies of lesions diagnosed clinically as warts may represent the noncharacteristic or even normal mucosal appearance of a proportion of HSIL, 45,46 or may be due to areas of HSIL adjacent to wart. Coinfection of the anal canal with multiple low and high-risk HPV types is common among GBM 47 and may lead to the presence of concomitant low-grade and high-grade anal disease. Consistent with this, HRHPV was detected in nearly all HSIL lesions by LCM in this analysis. Most HSIL lesions were associated with other HRHPV types, however this should be interpreted with caution in view of the small numbers.
The strengths of this study lie in the routine use of HRA and detailed recording of anal pathology, which allowed for comparison between anoscopy findings, HPV type, clinician impression, and cytology/histology outcomes. In addition, detailed questionnaires collected data regarding previous wart diagnoses and possible cofounding factors. Our analysis is limited by the fact that only the highest grade of SIL was routinely reported and therefore we are unable to comment on the prevalence of coexistent LSIL in lesions where HSIL was detected. Anoscopists would have been more likely to biopsy warts with atypical features and therefore the proportion of HSIL may have been lower among those warts not biopsied (18.5%). However, we have attempted to minimize this bias by also investigating lesions without documented clinical suspicion of other SIL pathology. Our findings are dependent on the skill and experience of the anoscopist, and therefore may not be generalizable to other settings. Also, the size of each wart was not recorded, which limits our interpretation of wart burden.
In conclusion, anal warts were common among SPANC participants. Anal warts were highly predictive of composite-HSIL, even after adjustment for age, HIV status, smoking, and lifetime number of RAI partners. Nearly two-thirds of HIV-positive SPANC participants with anal warts also had HSIL. Current guidelines recommend biopsy of anal warts only if they are atypical or refractory to treatment, however, our findings suggest that HSIL may be detected within one in seven biopsies from lesions diagnosed clinically as warts. The presence of anal warts may be a useful addition to the risk stratification for the likelihood of intra-anal HSIL among HIV-positive GBM.
Footnotes
Author Contributions
S.L.G., I.M.P., K.P., F.J., R.J.H., C.L., J.M.R., C.K.F., S.M.G., A.C., A.E.G., and D.J.T. made substantial contributions to the study conception and design, critical review of the article and final approval of the version to be published. In addition, S.L.G., I.M.P., K.P., and D.J.T. contributed to data analysis and drafting the article.
Acknowledgments
The authors thank all the participants. In addition to the coauthors of this article, the SPANC study team includes Annabelle Farnsworth, Clare Biro, Adele Richards, Julia Thurloe, Deborah Ekman, Ross McDonald, Marjorie Adams, Sepehr Tabrizi, Samuel Phillips, Monica Molano Luque, Simon Comben, Kirsten McCaffery, Kirsten Howard, Patrick Kelly, Daniel Seeds, Andrew Carr, Lance Feeney, Russ Gluyas, Garrett Prestage, Matthew Law, Brian Acraman, Patrick McGrath, Robert Mellor, Piero Pezzopane, Rick Varma, Julian Langton-Lockton, and Winnie Tong.
Author Disclosure Statement
A.E.G. has received honoraria and research funding from CSL Biotherapies, honoraria and travel funding from Merck, and research funding from Gilead. C.K.F. has received research funding from CSL and Merck, and owns shares in CSL Biotherapies. S.M.G. has received advisory board fees, grant support through her institution from Merck, lecture fees from Merck for work performed in her own time, and is an active member of the Merck Global Advisory Board as well as the Merck Scientific Advisory Board. K.P. has received consultancy fees from ViiV Healthcare. R.J.H. has received research funding from CSL, Merck, and Hologic. I.M.P. has received travel funding from Sequiris. For the remaining authors none was declared.
Funding Information
SPANC was supported by the National Health and Medical Research Council (Grant No. 568971) and the Cancer Council New South Wales (Grant No. 13-11). Cytologic testing materials were provided by Hologic Pty Ltd. The Kirby Institute is affiliated with the Faculty of Medicine, University of New South Wales, and funded by the Australian Government of Health and Aging.