
Abstract
Prior sexually transmitted infections (STIs) are associated with higher rates of subsequent human immunodeficiency virus (HIV) infection, but the influence of prior STIs on perceived vulnerability to HIV remains unclear. We aimed to assess this relationship, hypothesizing that a prior STI diagnosis is associated with higher self-assessed vulnerability to HIV. We performed a cross-sectional study of men and transgender individuals who have sex with men screening for HIV prevention trials in Philadelphia. An unadjusted regression analysis found no significant association between prior STI and HIV risk perception (p = 0.71) or HIV anxiety (p = 0.32). Multivariate logistic regression models that controlled for predetermined potential cofounders known to impact HIV risk—such as condom use, preexposure prophylaxis use, and demographics—also failed to show statistically significant associations between prior STI and HIV risk perception (p = 0.87) or HIV anxiety (p = 0.10). Furthermore, there was no effect modification by HIV preventive behaviors on the relationship between prior STI and HIV vulnerability. These data suggest that a gap exists between how clinicians may attribute individual HIV risk and how individuals view their own vulnerability at a given moment in time. Future research should focus on the dynamic relationship between perceived HIV vulnerability, STI diagnosis, and adoption of preventive behavior to determine better, individualized targets for HIV prevention interventions.
Introduction
Adoption of and adherence to oral preexposure prophylaxis (PrEP), a highly effective medication regimen that prevents human immunodeficiency virus (HIV) infections, 1 is suboptimal in the United States. 2 –4 One potential individual-level barrier to both uptake and adherence is low perceived HIV risk by those who are eligible to take PrEP. Risk perception is an element in multiple theories of behavior change, which hypothesize that a person must sense vulnerability to a particular disease to adopt behaviors that mitigate the chances of acquiring that disease. 5,6 Qualitative and quantitative research in diverse populations has tied higher HIV risk perception to increased levels of PrEP interest, 7 PrEP initiation, 8 and PrEP adherence. 4,9
However, the factors that correspond with higher versus lower perceived vulnerability to HIV are still uncertain. Qualitative research with men who have sex with men (MSM) demonstrates that risk perception is affected by an individual's emotional state, partner type, and subjective interpretations of a partner's likely HIV status. 10,11 Whether “objective” high-risk experiences, such as prior sexually transmitted infections (STIs), 12,13 also influence risk perception is less clear. Research into the association of prior STI and risk perception has produced mixed results. One survey by MacKellar et al. of 2788 HIV-negative or unaware MSM showed that prior STI diagnosis was associated with higher HIV risk perception, even though many individuals still viewed themselves as being at low risk. 14 Alternatively, a recent study of 401 MSM at a New England STI clinic found no association between prior STI and higher HIV risk perception. 15
The growing adoption of PrEP further complicates attempts to examine the relationship between prior STI and current perceived HIV risk. For example, individuals already on PrEP may acquire a STI without any increase in their HIV vulnerability, since PrEP effectively protects against HIV. However, actual evidence for higher STI rates among PrEP users is mixed, 16 and qualitative studies show that many men continue to use condoms while taking PrEP. 17 More research is necessary to determine whether an association between a STI diagnosis and HIV risk perception exists for both PrEP and non-PrEP users.
Our primary research objective was to examine the relationship between prior STI and present HIV risk perception in a diverse, high-risk cohort of men and transgender individuals who have sex with men (both PrEP-experienced and PrEP-naive) screening for inclusion in HIV prevention trials. Secondarily, we aimed to determine the relationship between prior STI and HIV anxiety, a construct distinct from HIV risk perception that is rarely tested separately in research about HIV vulnerability. 6,18 We hypothesized that individuals with a STI in the past 12 months would have higher self-assessed HIV vulnerability—in terms of either (1) elevated risk perception and/or (2) elevated HIV anxiety—when compared to individuals without a prior STI diagnosis, after controlling for demographics and HIV protective behavior such as recent PrEP use and consistent use of condoms.
Methods
Study design, participants, and setting
We performed a cross-sectional study of men and transgender individuals screening for two separate HIV Vaccine Trials Network (HVTN) and HIV Prevention Trials Network (HPTN) clinical trials conducted in Philadelphia from July 2016 to May 2018. HVTN 704/HPTN 085 aimed to assess safety and efficacy of the VCR01 broadly neutralizing monoclonal antibody. HPTN 083 aimed to evaluate the efficacy of cabotegravir, an injectable integrase inhibitor, as PrEP. To meet inclusion criteria for the trials, participants had to be aged ≥18 years, assigned male sex at birth or identify as a transgender man, and have condomless intercourse with male or transgender partners or protected anal intercourse with ≥2 male or transgender partners in the 6 months before screening. After providing informed consent to screen for the Philadelphia site's HVTN/HPTN studies, participants completed survey instruments measuring the domains described below.
Recruitment was conducted through a variety of methods, including face-to-face outreach at bars, clubs, social service organizations, and community events; advertisements on social media and geosocial applications used by MSM and transgender individuals; and through personal referrals of prior participants. The University of Pennsylvania IRB approved data collection and analysis for this project.
Measures
We initially administered the survey via paper and pencil, then switched to an online version to streamline data entry. Demographic measures included self-reported race and ethnicity, sex assigned at birth, gender identity, and age. Participants selected one of five gender categories: female, male, trans female, trans male, or other. We recorded age as a continuous variable, which we then categorized into three groups: 18–24, 25–34, and >34 years. Past STI diagnosis was assessed with the question “Have you had a STD/STI in the last 12 months?” HIV risk perception was assessed by asking participants to rate “What is your feeling about how likely you are to get infected with HIV?” on a 1–5 scale, with 1 being extremely likely and 5 being extremely unlikely. 18 For the purposes of this project, risk perception was dichotomized into high versus low, with high HIV risk perception defined as answers of “somewhat likely,” “very likely,” and “extremely likely,” consistent with prior research. 19,20 A similar Likert scale was used with the question “I worry about getting infected with HIV,” 18 which was also dichotomized into high HIV anxiety (“some of the time,” “a lot of the time” and “all of the time”) and low HIV anxiety.
Consistent condom use was assessed by asking how often participants “used a condom during anal sex,” with possible choices being “never,” “some of the time,” “most of the time,” and “all of the time.” Consistent condom use was defined as using condoms “all of the time,” as research has shown that failure to use condoms all of the time places people at elevated risk for HIV regardless of their reported frequency of intermittent condom use. 21 PrEP use in the last 6 months was assessed by combining survey responses participants gave about their PrEP use with various partner types and adding any participant who reported active PrEP use at time of screening.
Power and sample size
We targeted a sample size of ∼220 participants to achieve an alpha level of 0.05, a beta level of 0.20, and a 20-percentage point difference in the proportion of subjects with high HIV risk perception between those without a STI and those with a STI. We anticipated ∼40% of the participants at the end of the project to have high-risk perception and ∼30% to have had a prior STI based on a mid-project review of these variables in the survey data, which we conducted to clarify our goal sample size.
Statistical analysis
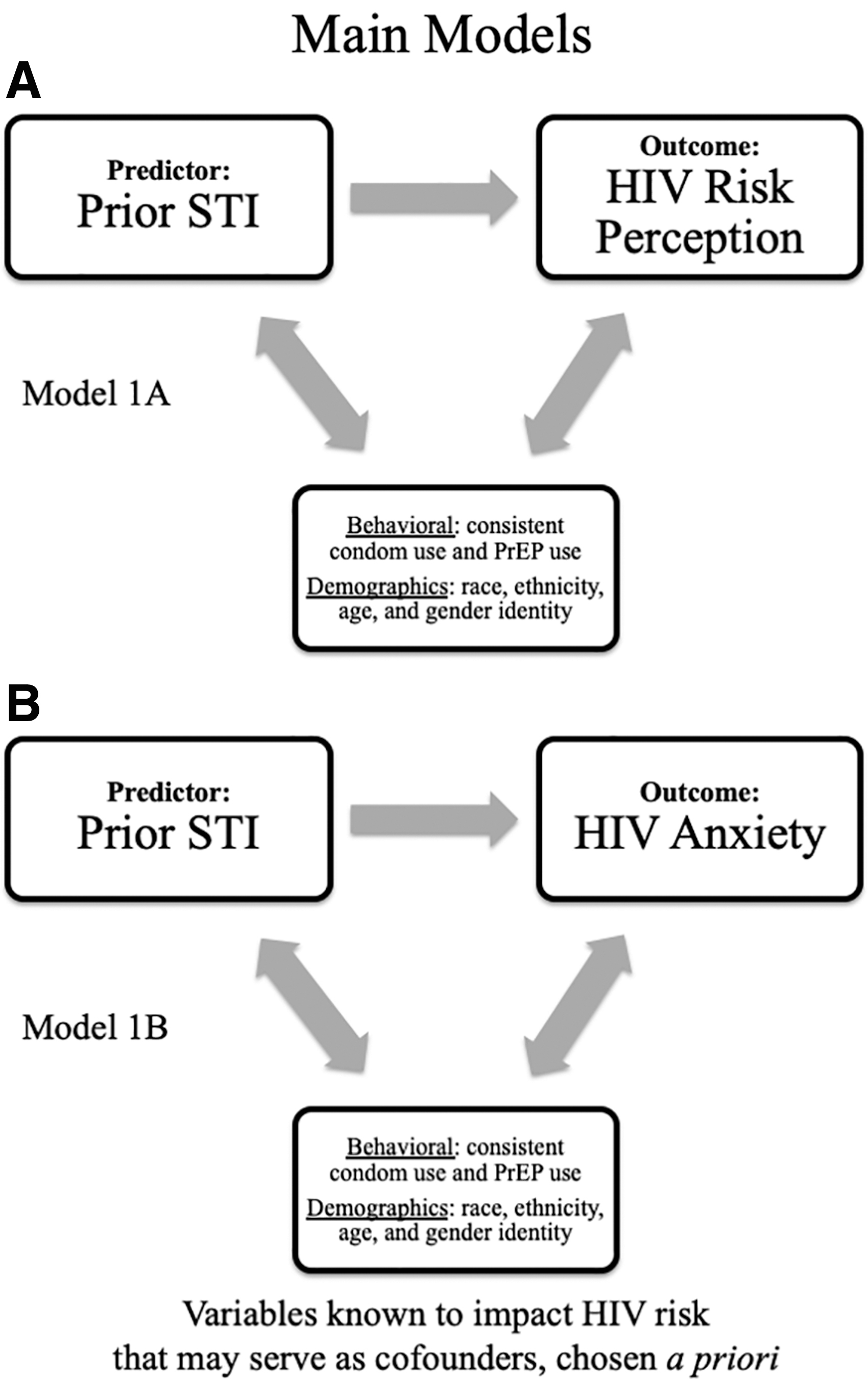
Patient demographics were reported with descriptive statistics, including means, medians, standard deviations, and interquartile ranges. Analysis for this project followed a priori models we created regarding the hypothetical connection between prior STI and self-assessed HIV vulnerability (in the form of HIV risk perception and/or HIV anxiety). Our primary model (Fig. 1A, B) hypothesized an association between a prior STI and HIV vulnerability that could potentially be masked by a number of confounders, including PrEP use, consistent condom use, age, race, ethnicity, and gender identity, which are known to impact actual HIV risk. As such, we first tested for an unadjusted association between prior STI and HIV risk perception, as well unadjusted associations between the confounding variables and our predictor and outcome variables using univariate logistic regression. We then constructed a multivariable logistic regression model that tested for associations between prior STI and risk perception while controlling for the a priori identified potential confounders. We repeated this analytic plan to examine adjusted associations between prior STI and HIV anxiety.
We also developed a secondary model (Fig. 2A, B), in which the hypothesized association between a prior STI and HIV vulnerability was modified by HIV protective behaviors. As such, we assessed the possibility of effect modification of PrEP use and consistent condom use on the relationship between prior STI and the self-assessed HIV vulnerability outcomes. All analyses were conducted on Stata15.1, College Station, TX, 2017.

Results
Two hundred forty-nine participants filled out the survey and 247 participants were included in the analysis, as 2 participants did not provide a response to the HIV risk perception and the HIV anxiety questions. The majority of participants were non-White men younger than the age of 35 years. Over one-quarter of the sample had an STI within the last 12 months, while rates of PrEP and consistent condom use in the sample were both low (Tables 1 and 2). Nearly half had high HIV risk perception and two-thirds had high HIV anxiety. Eighty-four participants (34%) reported both high HIV risk perception and high anxiety and 60 (23%) neither high HIV risk perception nor high HIV anxiety.
Characteristics of the Patient Population by Human Immunodeficiency Virus Risk Perception Category (n = 247)
Out of 249 total participants who filled the questionnaire, 247 are included in the study.
n = 1 did not report a prior STI.
n = 3 reported overlapping races.
n = 4 did not report Latinx ethnicity.
Too few participants to run a chi square.
n = 12 did not report recent PrEP use.
n = 3 did not report condom use.
HIV, human immunodeficiency virus; PrEP, preexposure prophylaxis; STI, sexually transmitted infection.
Characteristics of the Patient Population by Human Immunodeficiency Virus Anxiety Category (n = 247)
Out of 249 total participants who filled the questionnaire, 247 are included in the study.
n = 1 did not report HIV anxiety, hence the values in some rows may add up to one less than the total.
n = 1 did not report a prior STI.
n = 3 reported overlapping races.
n = 4 did not report Latinx ethnicity.
Too few participants to run a chi square.
n = 12 did not report recent PrEP use.
n = 3 did not report condom use.
HIV, human immunodeficiency virus; PrEP, preexposure prophylaxis; STI, sexually transmitted infection.
In the univariate regression assessing the relationship between prior STI and HIV risk perception (model 1A and Table 3), we found no significant association between prior STI and HIV risk perception [odds ratio (OR) 0.90; 95% confidence interval (95% CI) 0.51–1.58; p = 0.71]. There were no significant associations between the other a priori identified potential cofounders and HIV risk perception. We found a statistically significant unadjusted association between prior STI and recent PrEP use (OR 6.17; 95% CI 3.26–11.49; p < 0.01), with 53% of recent PrEP users reporting an STI within the past year compared to 15% of non-PrEP users. There was no association between prior STI and the other a priori identified potential confounders.
Unadjusted and Adjusted Logistic Regression of Associations with High Human Immunodeficiency Virus Risk Perception (n = 227)
Only participants who provided responses to all of the questions in the model were included in the final analysis. Hosmer-Lemeshow model goodness of fit: Chi-square (df = 8) = 4.35, p = 0.825.
Omnibus test for adjusted odds ratio: chi-square (df = 2) = 6.42, p = 0.04.
Compared to all non-Black participants.
Compared to all nontransgender women participants.
95% CI, 95% confidence interval; PrEP, preexposure prophylaxis; STI, sexually transmitted infection.
Values in bold reflect statistically significant findings.
In the final multivariable logistic regression model adjusting for age, race, ethnicity, gender, PrEP use, and condom use, there was no statistically significant association between recent STI and high perceived risk of HIV (Table 3). Being 35 years of age or older was the only covariate associated with increased HIV risk perception in the multivariate model, with these individuals having nearly threefold higher odds of high HIV risk perception (p = 0.01).
In the unadjusted analysis assessing the relationship between prior STI and HIV anxiety (model 1B), there was no association between prior STI and HIV anxiety (Table 4). We found a statistically significant association between older age and higher HIV anxiety in the unadjusted univariate regression, specifically among those 35 and older. There was no statistically significant association between HIV anxiety and the other a priori identified potential cofounders. The multivariate logistic regression model demonstrated no significant relationship between prior STI and HIV anxiety after controlling for the a priori determined demographics and protective behavior confounder (Table 4). Age ≥35 years was associated with statistically significant fivefold greater odds of increased HIV-related anxiety in the multivariate model (p < 0.01).
Unadjusted and Adjusted Regression of Associations with High Human Immunodeficiency Virus Anxiety (n = 226)
Only participants that provided responses to all of the questions in the model were included in the final analysis. Hosmer-Lemeshow model goodness of fit: Chi-square (df = 8) = 5.68, p = 0.683.
Omnibus test for adjusted odds ratio: chi-square (df = 2) = 11.62, p = 0.003.
Compared to all non-Black participants.
Compared to all nontransgender women participants.
95% CI, 95% confidence interval; PrEP, preexposure prophylaxis; STI, sexually transmitted infection.
Values in bold reflect statistically significant findings.
In testing the hypothesis that HIV preventive behaviors modify the effect between prior STI and HIV risk perception (model 2A), we found no statistically significant effect modification by PrEP use on the relationship between recent STI and HIV risk perception. Condom use appeared to modify the effect of a prior STI on risk perception, as those who experienced a prior STI among consistent condom users had greater odds of having HIV risk perception (OR 5.5, 95% CI 0.61–49.5) compared with noncondom users who had a prior STI (OR 0.76, 95% CI 0.43–1.38), although this difference did not reach our predefined criteria of statistical significance (p = 0.09). In testing model 2B, we found no statistically significant effect modification by PrEP use or consistent condom use on the relationship between recent STI and HIV anxiety.
Discussion
In this predominantly non-White, US-based sample of MSM and transgender individuals, there was no evidence of an association between prior STI and higher HIV risk perception or higher HIV anxiety. This lack of association suggests that those who had a STI in the past year did not sense increased vulnerability to HIV when screening into an HIV prevention clinical trial. There was no relationship between these terms whether we considered HIV protective behaviors and key demographic characteristics as potential cofounders or effect modifiers. These data are contradictory to our hypotheses and run counter to the established association between prior STI and increased risk for acquiring HIV. 12,22 Our study is one of a number of recent studies that did not identify an association between prior STIs and perception of HIV vulnerability among MSM and transgender individuals. 20,23 This study is unique in that it included a racially diverse, high-risk population of MSM comprised of both PrEP users and non-PrEP users. Moreover, the 40% of our cohort that had high-risk perception is somewhat higher than what is typically found in the literature (around 20–30% 15,19,20 ), possibly due to the fact that these individuals all agreed to participate in clinical trials aimed at HIV prevention.
One possible explanation for our results is that 30% of our cohort had taken PrEP in the last 6 months, and, given the high efficacy of PrEP in HIV prevention, these individuals may not have changed their perceived HIV vulnerability in response to a STI diagnosis. Evidence supporting this explanation was the strong association between PrEP use and STI diagnosis in this cohort. However, our study treated PrEP use as both a confounder and effect modifier and still found no association between prior STI and HIV vulnerability, suggesting that even among those individuals not on PrEP, there was no association between a prior STI diagnosis and a higher perceived vulnerability.
Another explanation for the lack of association is the inherent difficulty in measuring risk perception. Although Napper et al. developed a quantitative HIV risk perception scale, 18 many studies rely on a single question to elicit risk perception to reduce respondent burden. 14,15 This study used two question from the Napper scale that cover distinct constructs of risk perception to improve our ability to capture this phenomenon. However, it has been suggested that perceived HIV vulnerability is better elicited through in-depth conversations rather than questionnaires, as people may underreport their perceived vulnerability due to the impersonal setting of the questionnaire. 24 A reflection of this notion is that while 60 participants reported themselves to be neither at high risk for HIV nor have high HIV anxiety, they still indicated a strong desire to remain HIV-negative by expressing interest in clinical trials that would provide them access to PrEP, condoms, and HIV testing and counseling. As such, it is possible that all of the participants had some degree of HIV vulnerability in the recent past (e.g., when they decided to enroll in the study), but we failed to capture this vulnerability in our survey. The inability to capture the full extent of risk perception could be a result of our incomplete measures of HIV vulnerability, or it could be because HIV vulnerability is a mutable phenomenon that changes with one's daily life circumstances.
Alternatively, these findings may suggest that some participants experienced a phenomenon called the “perception gap” 25 or “unrealistic optimism,” 26 in which individuals with an “objectively” high risk for a particular illness do not perceive themselves as such. This perception gap is explained by common emotional and cognitive biases and can form in anyone. Within the field of HIV, the perception gap has been demonstrated in multiple communities—from a cohort of largely heterosexual patients visiting a district health center in Philadelphia 27 to MSM enrolled in a behavior risk reduction program in San Francisco. 20 This perception gap may be especially pronounced in young MSM, with multiple qualitative studies identifying low-risk perception as a barrier to initiating or adhering to PrEP in this population. 4,7,28 Young MSM may not realize that certain risk factors—such as a STI diagnosis—serve as PrEP indications or may be overly optimistic about their ability to sustain monogamy and consistent condom usage. 29 In addition, it had been suggested that young MSM may also experience HIV treatment optimism and HIV prevention fatigue, but these findings are not universally supported. 30 Our study is one of the first studies to demonstrate that older MSM have quantitatively higher self-assessed vulnerability, with those aged >35 experiencing threefold higher odds of HIV risk perception and fivefold greater odds of HIV anxiety. Unfortunately, interventions intended to dissuade people's unrealistic optimism yield mixed results, 31 including a recent study that tested whether PrEP initiation would increase after individuals were presented with their “objective” HIV risk score. 32 As such, clinicians may be well served to move away from framing behaviors in a risk context when counseling individuals—especially younger MSM—who experience this perception gap. 33
This study has limitations as well as strengths. Since surveys may not accurately measure risk perception, we obtained a more holistic indication of HIV vulnerability using two validated measures, one that examined the participants' calculated risk of present and future HIV acquisition and one that measured their abstract sense of HIV anxiety. A second limitation of our cross-sectional data was our inability to determine the temporal relationship between STI diagnosis, PrEP uptake, and perceived HIV vulnerability. Moreover, because the recent STI variable extended as far back as 12 months, participants may not have reflected upon a remote diagnosis when considering their risk perception. Future studies may consider using tools such as ecologic momentary assessments or daily diaries to assess the dynamic relationship between these events and constructs. Similarly, while our study was sufficiently powered to examine the relationship between our independent and dependent variables of interest, our sample size may not have been large enough to find associations between our proposed confounders and dependent variables. Finally, since our sample comprised individuals interested in joining HIV prevention clinical trials, who probably had a higher sense of vulnerability than similar individuals not in the trial, these data may not be generalizable to the entire population of MSM or transgender individuals. Future studies outside of the clinical trial setting may reveal distinct patterns of HIV vulnerability and the relationship between vulnerability and different behaviors.
In conclusion, our study found no evidence of an association between prior STI and a higher self-assessed HIV vulnerability in the form of HIV risk perception or HIV-related anxiety. Future research should focus on assessing vulnerability and intervening to reduce HIV risk closer to important events, such as at the time of STI diagnosis or after having sex with an anonymous partner. In addition, interventions that motivate people to adopt protective behaviors should avoid framing their benefits in terms of reducing HIV risk alone.
Footnotes
Authors' Contributions
D.R. and S.W. conceived the presented idea. S.W., I.F., D.M., D.F., and A.D.V. developed the data collection process. D.R., S.W., R.G., and K.M. developed the analytical plan. Analysis was conducted by D.P. and D.R. D.R., S.W., and R.G. discussed the results' significance. D.R. and S.W. led the article drafting process. All authors provided critical input to the article and agree with its final version.
Acknowledgments
I express my gratitude to all participants in HVTN and HPTN clinical trials. The path to ending the HIV epidemic would be impossible without them.
Author Disclosure Statement
I.F. sits on the advisory boards for Gilead Sciences and ViiV Healthcare. These organizations were not involved in the design or execution of this study in any way. All other authors have no conflicts to declare.
Funding Information
This work was supported by the National Institute of Mental Health [K23MH119976] (Sarah Wood), NIMH F32 MH111341, Center for AIDS Research Pilot Award (P30 AI 045008), Penn Mental Health AIDS Research Center Pilot Award (P30 MH 097488).