
Abstract
South Africa has the largest HIV burden and treatment program in the world. Diversion of HIV prevention and treatment medication for recreational use—or nonmedical use for psychoactive effects—is a public health concern globally and in South Africa. Few South African studies examine recreational use of HIV antiretrovirals (ARVs). The objective of this article is to evaluate the prevalence of recreational ARV use and to identify risk and protective factors associated with use. Data are drawn from a cross-sectional household survey of N = 4399 adolescent girls and young women (AGYW) aged 15–24 years in six districts across South Africa where an evaluation of a South African combination HIV prevention for girls and young women was implemented. The use of ARVs to “get high” was reported by 8.3% of AGYW across all districts. Logistic regressions showed that those engaging in transactional sex were at two times higher odds of recreational ARV use [adjusted odds ratio (aOR) = 2.01; confidence interval (95% CI): 1.51–2.68]. Recreational ARV use was more likely among those who used pre-exposure prophylaxis (PrEP) (aOR = 2.17; 95% CI: 1.36–3.48); HIV-positive participants who were not on ARVs for treatment (aOR = 0.36; 95% CI: 0.18–0.68); and those who were not virally suppressed (aOR, no vs. yes = 2.84; 95% CI: 1.21–6.66). As ARVs become more widely available for prevention and treatment, it will be important to monitor and address the possible emergence of ARVs as a substance for misuse or abuse.
Introduction
South Africa has the largest HIV epidemic in the world, with 7.9 million people living with HIV in 2017. 1 South Africa also has the largest publicly funded HIV treatment program in the world; 62.3% of individuals living with HIV are on antiretroviral (ARV) treatment. 1 In 2016, the South African government approved the use of HIV oral pre-exposure prophylaxis (PrEP) at select clinics as part of South Africa's publicly funded HIV prevention program. 2 Rollout was first focused upon high risk adult populations, including sex workers, and then men who have sex with men, before extension to other high risk populations.
Prevention and treatment remain a public health priority in addressing the HIV epidemic in this global priority setting. Maintaining the integrity of the HIV drug supply—including halting any diversion of the HIV prevention and treatment drug supply for recreational use—is vital for public health objectives generally and HIV epidemic control specifically. For example, recreational use may compromise the limited supply of drugs available for prevention and treatment. 3 Recreational use may also contribute to concerning rates of pretreatment resistance. 4 In South Africa's National HIV Prevalence, Incidence, Behaviour and Communication Survey, 2017, HIV drug resistance was present among 55.7% of people on ARVs and among 22.8% of those who were HIV positive but ARV naive. 1 Recreational use may also contribute to an emerging substance use epidemic. ARVs, such as efavirenz, have documented neuropsychiatric effects that contribute to the sensation of getting “high” and thus have abuse potential. 5 –7 It is possible that whoonga (or wunga/nyaope)—a colloquial term used to describe ARVs as a cocktail integrated with a wide range of other substances, including household chemicals such as detergents and rat poison and illicit drugs such as marijuana and methamphetamine—may also have neuropsychiatric effects but these effects are yet to be documented through laboratory analyses.
The scientific literature on the recreational use of ARVs in South Africa is extremely limited. In South Africa, Larkan et al. conducted an ethnographic study of health care workers in the West Coast region. In this study, providers reported illicit trade of ARVs among their patients and drug dealers. 8 Rough et al. conducted a qualitative study of 43 HIV-positive, treatment-eligible adults from Soweto. In eight interviews, participants described recreational ARV use and diversion as a community phenomenon. 9 Grelotti et al. conducted a qualitative study of 22 participants who attended inkwaris or “club-events” in Durban. In 17 interviews, participants described recreational ARV use as a phenomenon in their community, including during these club-events. This was the only study identified in South Africa on this topic that included in the sample adolescents under 18 years of age. 10 Finally, Magidson et al. examined the prevalence of recreational ARV use and the association between ARV initiation on viral suppression. Data were derived from a prospective, observational cohort study of 500 ARV-eligible adults recruited from clinics in Gugulethu and Soweto. Approximately 4.8% (n = 24) reported recreational ARV use. Recreational ARV use was not significantly associated with HIV treatment initiation or viral suppression. 11 To our knowledge, there have been no published studies that have examined the phenomenon of recreational ARV use in South Africa using a representative household sample and with a focus on girls and young women.
Studying whether there is a phenomenon of recreational ARV use in South Africa among adolescent girls and young women (AGYW) is important for three reasons. First, AGYW account for a quarter of new infections in South Africa. 12 As PrEP rolls out more broadly, AGYW are a high priority population for PrEP uptake. Increased PrEP uptake would entail increased access to HIV medication that could be diverted for recreational use. Understanding this phenomenon of recreational ARV use can guide efforts to prevent the serious public health consequences of PrEP diversion into recreational ARV use for HIV prevention service delivery. This includes sustaining and ensuring that limited availability of PrEP medication is being directed to the populations who need it most for prevention. This research on recreational ARV use can also guide the development of health communication messaging to attenuate the possibility of pretreatment resistance among uninfected AGYW who might be diverting PrEP for recreational use and who would face treatment resistance if they were to be infected with HIV later in life. Second, HIV prevalence among South African AGYW aged 15–19 years is 5.6% versus 0.7% for same aged males and among women aged 20–24 years is 15.6% versus 4.8% among same aged males. 1 Because of the disproportionate prevalence of HIV in this population, access to ARVs for treatment is higher and, along with it, the risk of diversion of ARVs for recreational use. Understanding this phenomenon more can guide efforts to prevent the negative consequences of diversion of HIV treatment as it relates to the poor clinical outcomes tied to nonadherence and increased risk for onward HIV transmission from AGYW to partners or children due to poor viral load suppression. Third, understanding substance use rates among adolescents and young adults is vital because this age aligns with increased risk for substance use initiation and abuse. 13 Characterizing use of emerging substances such as recreational ARV use can guide preventive intervention strategies that may help change later life trajectories. The transition from adolescence to adulthood also corresponds to increased risk for HIV and, thus, offers a particularly interesting target for examining the prevalence of recreational use of ARVs. 14
This article examines the following questions: (1) What is the prevalence of recreational ARV use among a representative household sample of AGYW? (2) What are risk and protective factors associated with recreational use of ARVs to guide future intervention efforts? This study explores a number of hypothesized risk and protective factors, drawing from previous work examining predictors of adolescent and young adult problem substance use through a socioecological framework. Previous literature identified covariates at the individual, social, and structural level that have been associated with substance use, including alcohol and drug use, risk behaviors (in this article, defined as risky sexual behaviors such as early sexual debut and transactional sex), and poverty, 15,16 and guided our choice of hypothesized factors to examine (3) What is the prevalence of recreational ARV according to the following: PrEP and care cascade (PrEP use, HIV status, treatment initiation, and viral suppression)?
Methods
Sampling design
Data are drawn from a cross-sectional representative household survey of N = 4399 AGYW aged 15–24 years that took place from 2017 to 2018. The study design and methods are described in depth in other publications. 17,18 This survey comprised the first of two serial surveys designed to detect an anticipated 33% reduction in HIV incidence in an evaluation of a South African combination HIV prevention intervention for AGYW aged 10–24 years. This $67 million combination HIV prevention intervention was delivered from 2016 to 2019 and was funded by the Global Fund to Fight AIDS, TB, and Malaria over 3 years in 10 districts in which girls and young women were at highest risk for HIV across South Africa. The goals of the intervention were to: (1) decrease HIV incidence; (2) decrease teenage pregnancy; (3) increase retention in school; (4) decrease gender-based violence; and (5) increase economic opportunities. The intervention package included the following behavioral, biomedical, and structural HIV prevention programs: (1) access to comprehensive HIV, TB, and sexual and reproductive health services and commodities; (2) rights-based sexual and reproductive health education; (3) support to keep adolescent girls in school, including homework help; (4) therapeutic services for abused children; (5) financial literacy and career development; (6) vocational programs to promote economic empowerment; and (7) interventions to maximize social support and social capital. In addition, there was a (8) conditional cash incentive program that was rolled out in two districts.
A stratified cluster sampling design was used to select participants for the survey. The 10 intervention districts were considered as the primary strata. The sample size per district was designed to be proportional to the AGYW in the subdistrict areas or wards selected for intervention. Intervention areas were mapped onto the available census small areas layer (SAL) sampling areas. A sampling frame of households was compiled for each district based on the 2011 census SALs. The SAL sampling frames were cross-checked with other sources and mapped with aerial photography to make sure that they were accurate and up-to-date. The sampling frame was further informed by the latest Geo Terra Image counts, other district council estimates, and StatsSA's most current midyear estimates of population numbers per province, according to the province boundaries, race, 5-year age groups, and gender. For each SAL, information was available about the number of households and number of individuals by gender, population group, and age.
Across the 10 districts there were 2470 SALs targeted for the intervention, with 300,000 households in which 120,000 AGYW were residing, based on the 2011 census. A simple random sample of SALs was selected in the intervention areas in each district. A systematic random sample of 35% of the available households within each sampled SAL was selected to generate the required sample size of AGYW. All AGYW aged 15–24 years in sampled households were invited to participate. The field team identified these preselected households using aerial maps and determined the geographical coordinates using Geographical Positioning System. If the selected household was vacant, or the household head declined to complete a household listing form to determine whether there were eligible AGYW, the next household on the left was visited and assessed. The survey was completed in six districts: City of Cape Town (Western Cape), Ehlanzeni (Mpumalanga), O.R. Tambo (Eastern Cape), Tshwane (Gauteng), King Cetshwayo (KwaZulu-Natal), and Zululand (KwaZulu-Natal). The overall response rate was 61%, and it ranged from 33% in Cape Town to 78% in Zululand. The overall sample realization was 60.6% in the six completed districts. The weighted sample size was 7237 for this household-based sample of AGYW aged 15–24 years across six districts where AGYW were at highest HIV risk.
Participants and procedures
The study was approved by the South African Medical Research Council Research Ethics Committee (EC036-11/2016). AGYW were eligible for inclusion in the survey if they met the following inclusion criteria: (1) AGYW residing in household aged 15–24 years; (2) AGYW residing in household <18 years of age who had consented and whose parent, guardian, caregiver, or household representative had consented to her participation; and (3) AGYW were willing to participate in the study, undergo all study procedures, including providing blood samples, and willing to give written informed consent. AGYW were excluded if they: (1) had cognitive or mental challenges (based on the assessment of the participant's ability to comprehend the study information provided); (2) were unable to hear or speak; (3) were unable to speak English, IsiZulu, isiXhosa, Northern Sotho, Sotho, Tswana, Tsonga, Swazi, Sepedi, Afrikaans; and (4) were not available for participation between 8 AM and 9 PM. Each potentially eligible study participant was informed about the study and completed the consent form in their preferred language before enrolment. For potential participants under 18 years of age, parent/guardian/foster parent/caregiver consent was obtained before getting consent from the AGYW. Informed consent procedures were conducted in a private space, inside or outside the household, depending on the potential participant's choice. The field-worker sat with the potential participant and read the forms to her word-for-word and answered any questions for clarification from the participant.
Electronic questionnaires were developed and used with the Mobenzi Researcher data collection software suite (
Measures
All measures were translated and back-translated into local language and then pilot tested for understanding with the study population over a 2-week period. Questions on drug use—including recreational ARV use—occurred immediately after questions on alcohol use in the questionnaire.
Recreational ARV use
Recreational use of ARVs is the use of ARVs for nonmedical reasons (e.g., for treatment or prevention) with the explicit purpose of getting “high.” There are no existing validated measures of recreational ARV use or modality of use. To capture recreational use among self and others, this research asked: “Have you or someone you know ever used ARVs to get high OR another mixture of substances that you suspect may have contained ARVs to get high (this mix is sometimes called nyaope or whoonga)?” Answer options (more than one option was possible) included: (1) you; (2) someone you know; and (3) neither I nor someone I know has done this. This measure was previously used with an adolescent study population in South Africa. 19
Other substance use
A brief version of the Alcohol Use Disorders Identification Test (AUDIT-C) was used, to capture alcohol use (Cronbach's Alpha from this study: 0.79). AUDIT-C is comparable to the full AUDIT and has been used among South African populations. 20 A participant's AUDIT-C score can range from 0 to 12. Informed by the recommendation emanating from the South African study 20 was used with a cutoff score of greater than or equal to 2 to indicate hazardous drinking. An 11-item Drug Use Disorders Identification Test (DUDIT) was used, to capture drug use (Cronbach's Alpha from this study: 0.87). DUDIT captures use of drugs such as cannabis, amphetamines, cocaine, opiates, hallucinogens, thinner and other drugs, gamma hydroxybutyrate (GHB), sleeping/calming pills, pain relievers, and tobacco, but excludes alcohol and recreational ARV use. A participant's DUDIT score can range from 0 to 44. A cutoff score of greater than or equal to 2 to indicate a drug-use disorder was used, based on a recommendation emanating from a South African study. 21
HIV, ARVs, PrEP, syphilis, and other sexually transmitted infections
Biological samples were collected to test for HIV infection and syphilis. HIV tests were composed of HIV serological testing for infection and HIV-1 ribonucleic acid (RNA) viral load measurement among those HIV serologically positive. The HIV-1 RNA viral load data and antiretroviral therapy (ART) drug measurements were included in a recent infection testing algorithm to minimize the false recent rate, to determine the proportion of HIV-infected persons on ART, and those who are ART naive with detectable and undetectable viral load. LAg Assay was used to determine number and proportion of participants with recent infection for sexually transmitted infection (STIs) (syphilis). After their study participation, participants were offered home-based rapid HIV testing with immediate access to their results and a referral for ART if they test positive. Participants had access to their study laboratory test results within 2 weeks at a clinic near their home. We also asked about PrEP use with two questions: “PrEP is a new prevention method in which people who do not have HIV take a pill daily to reduce their risk of becoming infected with HIV. Before today, have you ever heard of people who do not have HIV taking PrEP to keep from getting HIV?” and “In the past 12 months have you taken PrEP to keep you from getting HIV?”
Behavioral measures
Questions about age of sex initiation and engagement in transactional sex were asked. Transactional sex was asked using the following questions: Have you even given oral, anal, or vaginal sex to someone because you expected to get or got any of these things? and In the past 12 months have you started or stayed in a relationship with a man or boy so that you could receive any of the following? Answer options could include the following: money, transport, food for myself and/or my family, clothes or shoes, shelter, school fees/school uniform, airtime, cell phone, items for children or family, cosmetics, I have not done this, I prefer not to say, and other.
Participant demographics
Questions on citizenship, population group, education, and orphanhood were included.
Statistical analysis
Descriptive statistics was used to examine prevalence of recreational ARV using the unweighted sample of N = 4399 and weighted sample of N = 7237. For the remainder of the analyses, we used the weighted sample of N = 7237 and performed survey-based analysis to provide correct population estimates of variability and to make estimates generalizable. For the main outcome, we report both weighted and unweighted data. For other analyses, percentages are calculated from weighted data. Pearson χ 2 tests were conducted to assess associations between independent variables and recreational ARV use. Adjusted and unadjusted logistic regressions were performed to identify risk and protective factors of recreational ARV use. This epidemiological profile of risk was built and informed by other models examining risk factors for substance use in similar populations. 15,16,22 For the economic status variable, a relative socioeconomic status variable was created through a cluster analysis (K-modes algorithm). This analysis focused on classifying participants into two socioeconomic groups based on their responses to the following variables: how often participants were away from home in the last 12 months, availability of flush toilet, potable water, electricity, car, computer, internet, refrigerator, stove, having money, saving money, owing money to others, and hunger. 23 Due to high collinearity between paternal, maternal, and double orphanhood, an aggregate indicator variable was included representing any type of orphan status. Syphilis status was excluded from univariate regression analysis because all individuals who reported recreational drug use tested negative for syphilis. For each risk and protective factor, a univariate logistic regression was run with recreational ARV use as the outcome of interest and a second logistic model adjusting for relative socioeconomic status and age. Hosmer–Lemeshow goodness-of-fit test was used to assess model fit. Results are presented as odds ratios (ORs) with confidence interval (95% CI) and p-values. Pearson χ 2 tests were conducted to identify whether recreational ARV use varied based on HIV positive status, PrEP use, treatment use, and viral suppression (cutoff of 1000 copies/mL). All analyses were conducted using SPSS Version 25 and R Version 4.0.1. 24,25
Results
Participant characteristics
Participant demographics
Participants were almost all South African citizens (98.8%). Most participants self-identified as “African” (89.8%). Over half of the participants reported that they were in school at the time they were surveyed (56.2%), and 84.3% of the participants in the 15–19 years age group reported that they were at school, compared to 24.3% of those in the 20–24 years age group. When asked whether their biological parents were alive, 21.2% reported that they were maternal orphans (here defined as their biological mother was not alive), 34.9% were paternal orphans (their biological father was not alive), and 11.2% reported they were “double orphans” (defined as both biological parents were not alive). Nearly 80% of participants came from a relatively low socioeconomic background (79.7%). Participant demographics are displayed in Table 1. We also examined additional possible risk and protective factors for recreational ARV use, as summarized below and displayed in Table 2.
Participant Demographics Among South African Adolescent Girls and Young Women, Aged 15–24 Years from 2017 to 2018
Risk and Protective Factors Associated with Recreational Antiretroviral Medication Use Among South African Adolescent Girls and Young Women, Aged 15–24 Years from 2017 to 2018
Participants were classified as having knowledge of being HIV+ if they declared they were HIV+ in either of the “hiv_result” or “hiv_status” variables. Moreover, they were assumed to have knowledge of their status if a laboratory test confirmed they were positive and ART metabolites were present in their blood.
The current convention is to use (at least for DBS) a cutoff of 1000 copies/mL. Anything <1000 copies/mL?: successful viral suppression if ART exposure (laboratory test) or elite controller or underestimation of viral load based on technology or quality of specimen.
ART, antiretroviral therapy; CI, confidence interval; DBS, dried blood spot; DUDIT, Drug Use Disorders Identification Test.
Prevalence of recreational ARV use
The prevalence of recreational ARV use was 8.3% among AGYW (unweighted) and 9.1% (weighted; 95% CI: 8.2–10.0). Recreational use of HIV drugs was reported across all districts surveyed, but ranged widely from 5.2% (95% CI: 4.0–6.4) to 15.9% (95% CI: 12.5–19.3) across these districts. Please refer to Table 3. Further, 9.8% of AGYW (unweighted) and 10.6% (weighted; 95% CI: 9.5–11.7) reported knowing someone who had used ARVs recreationally. There were no missing data for this survey question about recreational ARV use.
Prevalence of Recreational Use of HIV Antiretroviral Medications Among South African Adolescent Girls and Young Women, Aged 15–24 Years from 2017 to 2018
Percentages in parentheses represent total prevalence using weighted sample size.
Other substance use
Overall, 10.8% of participants drank alcohol two or more times a month (95% CI: 9.9–11.7). Among AGYW in the 15–19 age group, 9.3% drank alcohol two or more times a month, with those in the 20- to 24-year-old age group drinking significantly more at 12.8% (χ 2 = 14.2; p < 0.001). Hazardous levels of alcohol use—determined by a score of greater than or equal to 2 on the AUDIT-C scale—were reported by 27.0% of AGYW (95% CI: 25.7–28.4). There was no association between alcohol use two or more times per month and recreational ARV use (χ 2 = 1.31; p = 0.20). Hazardous levels of drug use—determined by a score of greater than or equal to 2 on the DUDIT scale, which includes drugs like marijuana but not recreational ARV use—were reported by 5.5% of AGYW (95% CI: 4.8–6.1). There was no association between drug use (this excludes alcohol and recreational ARV use) two or more times per week and recreational ARV use (χ 2 = 0.03; p = 0.82).
HIV, ARVs, syphilis, other STIs
Twelve percent (12.4%) of AGYW were HIV positive (95% CI: 11.5–13.2). Among AGYW who were HIV positive, half (50.6%; 95% CI: 46.9–54.2) were on ART (based on the detection of metabolites in the blood). Among all those living with HIV (whether they knew their status or not), 62.1% reported viral suppression (95% CI: 58.4–65.9). The prevalence of syphilis was 0.5% among all AGYW, but 0% among AGYW who reported recreational ARV use. The survey included self-reported questions about whether AGYW had been diagnosed with an STI by a doctor or nurse in the previous year and whether they had experienced STI symptoms during the past year; 10.7% of AGYW reported having been diagnosed with a STI in the past year (95% CI: 9.9–11.5). A very low number of AGYW (1.9%; 95% CI: 1.6–2.3) had taken PrEP in the last 12 months.
Behavioral measures
Over two-thirds (69.2%; 95% CI: 67.9–70.4) of AGYW had engaged in penetrative sex with nearly a 10th (8.9%; 95% CI: 7.9–9.8) who reported early age of sexual debut before 15 years. A concerning proportion of AGYW (9.5%; 95% CI: 8.7–10.2) had engaged in transactional sex.
Risk and protective factors for recreational ARV use
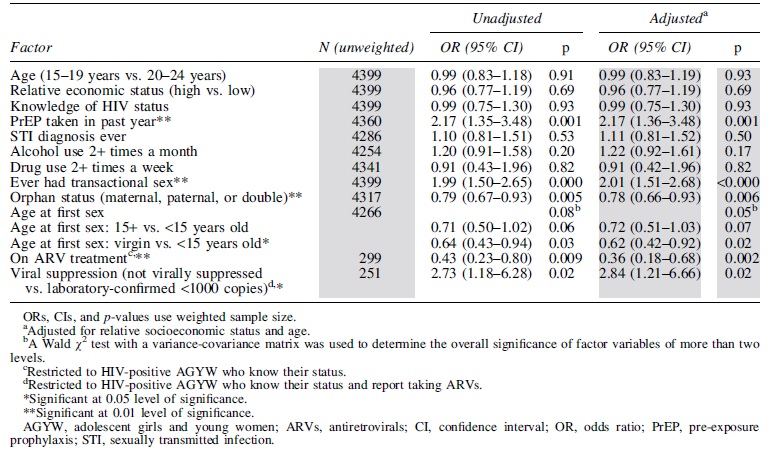
Table 4 presents univariate logistic regression results for odds of recreational ARV use, assessing hypotheses about associations between numerous explanatory variables and the outcome of interest. Those who reported taking PrEP in the past year exhibited over two times higher odds of recreational ARV use [adjusted OR (aOR) = 2.17; 95% CI: 1.36–3.48]. Similarly, those who reported ever having engaged in transactional sex exhibited over two times higher odds of recreational ARV use (aOR = 2.01; 95% CI: 1.51–2.68). In contrast, AGYW who had lost one or more parents were at over 10% lower odds of recreational ARV use (aOR = 0.78; 95% CI: 0.66–0.93). Those who knew their HIV-positive status and on ARVs were at a 60% lower odds of recreational ARV use (aOR = 0.36; CI = 0.18–0.68). Those who knew their HIV-positive status and reported being on ART but were not virally suppressed exhibited nearly three times higher odds of recreational ARV use (aOR = 2.84; CI = 1.21–6.66). Finally, those who were virgins exhibited lower odds of recreational ARV use compared to those who first had sex before the age of 15 years (aOR = 0.62; CI: 0.42–0.92). However, this three-level categorical variable was not significant overall. There was no significant association between recreational ARV use and age, relative socioeconomic status, knowledge of HIV status, STI diagnosis, alcohol use, or drug use.
Univariate Logistic Regressions for Odds of Recreational Antiretroviral Use
Associations between recreational ARV use, PrEP use, HIV status, treatment initiation, and viral suppression
Table 5 presents prevalence of recreational ARV use according to the following: PrEP and care cascade (PrEP use, HIV status, treatment initiation, and viral suppression). Recreational ARV use differed significantly by exposure to PrEP. Among AGYW who used PrEP in the last year, 17.6% reported recreational use. In contrast, among AGYW who did not use PrEP, only 8.8% reported recreational use (χ 2 = 7.27; p = 0.001). Recreational ARV use did not differ by HIV status, with a prevalence of 8.5% of laboratory-confirmed HIV positive AGYW reporting recreational use versus 9.2% of HIV negative AGYW (χ 2 = 0.31; p = 0.55). Likewise, there was no difference in prevalence among participants who knew their HIV-positive status versus those who were negative or did not know their status (9.0% vs. 9.1%, χ 2 = 0.004; p = 0.93). Among those who knew their HIV-positive status, 7.7% currently on ART reported recreational ARV use versus 16.4% of those who were not on ART (χ 2 = 5.40; p = 0.007). Finally, among those who knew their HIV-positive status and reported being on ART, those who were virally suppressed were less likely to use ARVs recreationally versus those who were not virally suppressed (6.3% vs. 15.3%, χ 2 = 3.98; p = 0.01).
Recreational Antiretroviral Use by Pre-Exposure Prophylaxis Use, HIV Status, Treatment Initiation, and Viral Suppression
Category percentages and χ 2 tests use weighted sample size.
Significant at 0.01 level of significance.
Significant at 0.05 level of significance.
ARVs, antiretrovirals; PrEP, pre-exposure prophylaxis.
We further examined the prevalence of recreational ARV use by a four-level categorical variable describing both HIV status and ART behavior to confirm these primary results. Specifically, we compare prevalence between laboratory-confirmed HIV-negative self-reported PrEP nonusers, laboratory-confirmed HIV-negative self-reported PrEP users, HIV-positive self-reported ART nonusers who know their status, and HIV-positive self-reported ART users who know their status. The prevalence among HIV-negative PrEP nonusers and users was 8.8% and 15.0%, respectively; among HIV-positive individuals who know their status, the prevalence among self-reported ART nonusers and users was 16.4% and 7.7%, respectively. With
Discussion
South Africa is an important global site of significance for exploring the possible phenomenon of recreational use of ARVs given the scale of the HIV epidemic and the large size of the national ARV treatment and growing PrEP program. Findings from this cross-sectional representative household survey indicate that recreational ARV use is a concerning phenomenon and widespread with reports of use at all sites surveyed. While the overall prevalence varied widely across sites, the overall prevalence of 8.3% among AGYW (unweighted) and 9.1% (weighted) across all sites surveyed raises serious concerns that recreational ARV use is not just from anecdotal reports or isolated to certain sites in South Africa. This concerning prevalence indicates that we may need to more systematically track and study recreational ARV use as an emerging substance use phenomenon in South Africa. All studies on recreational use of ARVs thus far in South Africa are based on self-report and, thus, introduce an element of bias. This includes the need to develop detailed measures to evaluate this phenomenon across studies, to have researchers evaluate this phenomenon using the same measures, and to develop more robust methods to verify the chemical composition of the drugs used for recreational ARV use. Findings also have implications for the clinical rollout of PrEP for HIV prevention and in distribution of HIV medication for treatment. For example, clinicians may wish to screen for recreational ARV use and explicitly discuss the dangers of this type of recreational use for the development of treatment resistance and adherence. A public health response might include broader health communication campaigns that accompany the expanded rollout of PrEP to prevent this phenomenon of recreational ARV use. To our knowledge, intervention science around this area of prevention has not yet been developed and is a major gap that needs to be filled as more research is done on this phenomenon.
When risk and protective factors associated with recreational ARV use were examined, important risk factors emerged: those engaging in transactional sex and taking PrEP in the past year were more likely to engage in recreational ARV use. The finding around PrEP use being a risk factor for recreational ARV use needs to be interpreted with caution and explored further. For example, this finding may be reflective of higher engagement in risk behavior, including substance use or may reflect increased access to ARVs that are diverted for recreational use. This finding does not suggest that PrEP not be prescribed for fear of ARV diversion, but that clinicians should consider how increased access to ARVs may need to be paired with careful health communication messaging that supports proper use of PrEP, including the importance of adherence. Several protective factors emerged. Those living with HIV who were engaged in treatment were less likely to engage in recreational ARV use. Notable was that those living with HIV and who were not engaged in treatment were more likely to engage in recreational ARV use. These differences might reflect varying motivations for health protective behaviors; decisions to not engage in treatment might correspond with higher risk behaviors such as recreational ARV use. Individuals who were not yet sexually active were also less likely to engage in recreational ARV use although the three-level factor for age at first sex was not significant overall. Finally, a third protective factor emerged, with recreational ARV use less likely among AGYW who reported orphanhood. This finding needs to be explored further. It may be that the loss of a parent or parents result in different physical, financial, and emotional consequences that attenuated risk for substance use. 26 For example, AGYW who had been orphaned may have been able to access supportive social programs that diminished risk for recreational ARV use.
Finally, the association between recreational ARV use and various aspects of the PrEP and HIV care cascade was examined. It was found that recreational ARV use was significantly more likely among those who used PrEP, but notable is that the number of individuals who used PrEP was small. It may be that PrEP users were more likely to engage in recreational ARV use because they had increased access to HIV medication for prevention. Alternatively, this pattern might reflect that AGYW engaging in PrEP were more likely to engage in higher risk activities, including condomless sex and substance use. This finding should not be used to undermine the rollout of PrEP for HIV prevention, which is a vital contribution to the biobehavioral prevention toolbox. Rather, this finding indicates that care needs to be taken in regard to program design and rollout, including messaging around uptake of PrEP, including the importance of adherence and the use of this prevention medication as prescribed. It was also found that recreational ARV use was more common among HIV positive participants who were not on ARVs for treatment and among those who were not virally suppressed. These findings indicate the need to address substance use—including specifically discouraging recreational use of ARVs—in tandem with treatment initiation and treatment adherence.
This study has several limitations. For respondents who reported recreational use of ARVs, this study is unable to verify the concentration of ARVs or the chemical composition of ARVs if ARVs were mixed with other drugs. Nonetheless, it is concerning that participants were taking any substance with ARVs in it for recreational use. Due to the cross-sectional design, this study is unable to determine causal pathways or the directionality of associations between recreational ARV use and the various risk and protective factors that have been identified. Another potential limitation is the risk of bias in responses; reports of recreational ARV use were based on self-report and were not biologically verified. This limitation highlights that there is a paucity of validated measures for capturing the phenomenon of recreational ARV use, with a wide range of terminology being used to describe this type of substance use and also with the same term (e.g., whoonga) possibly being used to describe very different chemical compositions and amounts of drugs. Studies that focus on developing, piloting, and validating measures for recreational ARV use would be an important contribution to enhance the rigor of future study of this phenomenon. Ultimately, more rigorous methods for verifying the chemical composition of recreational ARVs need to be developed for biologically verifying that this substance has been used. We need further research to expand efforts to optimize program content (for ART counseling, adherence, PrEP) and to tailor efforts for the specific populations based on their unique risks for recreational use of ARVs; for example, it is important to discuss the dangers of diverting ARVs from treatment and prevention for recreational use of ARVs as this can challenge adherence and thus effectiveness of viral control or treatment as prevention. Despite these limitations, findings underscore that as ARVs become more widely available for prevention and treatment, it will be important to monitor and address the possible emergence of ARVs as a substance for misuse or abuse. This may be particularly vital during the transition from adolescence to adulthood with regard to prevention of problematic substance use behaviors. Advancing our knowledge on the phenomenon of recreational ARV use can guide public health efforts in several ways. This includes interventions to prevent this new form of substance use. In addition, findings can guide the effective rollout of biomedical prevention strategies such as PrEP, including by guiding efforts to develop health communication messaging that could diminish diversion of limited prevention medication to recreational use while maximizing adherence to ensure effective treatment as prevention. Finally, these findings can help to ensure that HIV medication is being used effectively for treatment. For those who are on treatment and diverting treatment for recreational use, reducing diversion for recreational ARV use would improve adherence for those living with HIV with clinical benefits, as well as prevention benefits for partners and children by reducing the probability of onward HIV transmission.
Footnotes
Authors' Contributions
All authors participated in the conception and design of the study, as well as writing of this article.
Acknowledgments
The authors acknowledge and thank the AGYW and other participants who agreed to make themselves available to take part in this research and share their views, opinions, and experiences with us.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This combination HIV prevention intervention was funded by the Global Fund to Fight AIDS, TB, and Malaria and implemented in the 10 districts by a range of government departments and civil society organizations that were appointed by the organizations responsible for the management of the AGYW program: Western Cape Department of Health, KwaZulu-Natal Treasury, Kheth'Impilo, Soul City Institute for Social Justice, and the Networking HIV and AIDS Community of Southern Africa (NACOSA). The program was aligned with the She Conquers campaign funded by the United States President's Emergency Plan for AIDS Relief (PEPFAR) and was implemented with support from the South African National AIDS Council (SANAC) through the Country Coordinating Mechanism (CCM) and the CCM Secretariat. This study has been supported by the President's Emergency Plan for AIDS Relief (PEPFAR) through the Centers for Disease Control and Prevention, under the terms of Cooperative Agreement 1U2GGH001150. Development of this publication was supported by the Social Impact Bond of the South African Medical Research Council. This work has been supported by the US Department of Health and Human Services, Centers for Disease Control and Prevention (CDC), Division of Global HIV & TB (DGHT) under the terms of Cooperative Agreement 1U2GGH001150. The work herein for Kim Jonas was made possible through funding by the South African Medical Research Council through its Division of Research Capacity Development under the intramural Postdoctoral Fellowship Programme.