
Abstract
Viral suppression and postpartum retention in care have far-reaching health implications for pregnant women living with HIV and their children, yet remain public health challenges. Prenatal care presents a unique opportunity to engage pregnant women in care. The purpose of this study is to evaluate whether group prenatal care is effective in impacting these outcomes for pregnant women living with HIV. A retrospective cohort study was performed of all women living with HIV who obtained prenatal care from a community-based health center between 2013 and 2019. Women who spoke English or Spanish, remained within the system, and had not participated in group prenatal care previously were included. Women self-selected a prenatal care model: 85 selected group care and 109 elected individual care. Group prenatal care followed a standard Centering Pregnancy® curriculum with the addition of HIV-related topics. The primary outcomes of the study were viral suppression (viral load <20 copies/mL) and postpartum retention in care (attending at least one or two visits with HIV primary care within 12 months postpartum). After adjusting for potential confounding factors, women who participated in group prenatal care were significantly more likely to have at least one HIV primary care visit postpartum {adjusted odds ratio (aOR) = 2.71 [95% confidence interval (CI 1.14–6.46)]; p = 0.024}, and had a trend for achieving viral suppression by the time of delivery [aOR = 2.29 (95% CI 0.94–5.55); p = 0.068]. We have demonstrated that group prenatal care for pregnant women living with HIV is feasible and effective, with positive impacts on retention in care and viral suppression, factors that affect long-term outcomes from patients living with HIV.
Introduction
The Centers for Disease Control and Prevention estimates that there are ∼5000 annual deliveries among 258,000 women in the United States living with HIV. 1 Overall number of women living with HIV and rates of perinatal transmission have decreased. However, 66 cases of perinatal transmission still occurred in the United States in 2018, 2 with disproportionate numbers among Black and Hispanic women, and in southern states. 3 Review of perinatally acquired cases highlights missed opportunities for prevention including late diagnosis; lack of, late, or inconsistent prenatal care; and lack of appropriate antiretroviral therapy (ART). 3 –5 These missed opportunities emphasize the need for early, consistent, and specialized prenatal care for pregnant women living with HIV.
Prenatal care presents a crucial opportunity to engage women living with HIV in primary care to improve their own clinical outcomes. Engagement in prenatal care increases the likelihood of receiving ART and achieving viral suppression by delivery. 6 Further, suppression at delivery is associated with being in care, on ART, and being virally suppressed for months to years postpartum. 7 –9 Not only does viral suppression impact potential HIV-related morbidity, 10 viral rebound, 11 and drug resistance, 12 but it also influences maternal status going into subsequent pregnancies and, therefore, risk of perinatal transmission. 13,14 Despite the importance of achieving viral suppression and continuing to engage in care after delivery, 12-month postpartum retention rates in US cohorts range from 37% to 76% with clear geographic variability, 7,14 –18 and 12-month postpartum viral suppression persists in only 38–41% women. 7,17
Barriers to retention in care in this population are numerous. 19 Transportation problems, juggling work commitments and childcare schedules, depressive symptoms, perceived negative treatment by medical professionals, lack of social support, and stigma all act as obstacles to staying in care after delivery. 18,20,21 Conversely, positive family support, good relationships with health care providers, individualized case management services, and appointment reminders have all been shown to enable postpartum follow-up. 18,20,22,23
CenteringPregnancy® is a model of group prenatal care that has been proposed as a method for improving prenatal care for pregnant women. 24 It includes 10 two-hour sessions each with a pregnancy-related focus, is highly interactive, and fosters education as well as social support. Group prenatal care has been shown to increase patient satisfaction 25,26 and improve attendance at prenatal visits, 27 as well as decrease incidence of low birth weight and preterm delivery, especially in certain high-risk populations. 28 –30 It has also been shown to affect depression and perceived social support in some studies. 31 –33 Group care has been evaluated in the nonpregnant HIV population and is associated with better adherence and improved retention in care, 34 although its effect on these outcomes for pregnant women living with HIV has not been assessed. This study aims to evaluate the effects of HIV-adapted group prenatal care on viral suppression and postpartum retention in HIV-related primary care.
Methods
This was a retrospective cohort study of pregnant women living with HIV cared for at a community-based health center in Houston, Texas, who had deliveries between September 1, 2013, and July 31, 2019. Prenatal care at this health center was offered through standard individual care and an HIV-adapted Centering® group care model throughout the study time period. Demographic and outcome variables were collected through electronic medical record review. Institutional review board approval was obtained through both Baylor College of Medicine (H-32171) and Harris Health System (H-18412).
Women were excluded if the pregnancy ended in spontaneous miscarriage, termination, or intrauterine fetal demise <30 weeks estimated gestational age (EGA) due to inability to complete full group prenatal care course in these situations; if the patient transferred care outside of the health district during her pregnancy; if her primary language was other than English or Spanish; or if she presented to care after 30 weeks EGA. Women who had engaged in CenteringHIV during a previous pregnancy were allowed to participate in group care in a subsequent pregnancy but were not eligible for the study.
If a patient only spoke a language other than English or Spanish, or presented to care after 30 weeks EGA, she was automatically assigned to individual care. Eligible patients were counseled about group (CenteringHIV) versus traditional individual care at their initial obstetric visit and self-selected their preferred mode of prenatal care. Women were encouraged to try out group prenatal care and were informed that they could withdraw and continue with individual care at any time. Because of this, many women attended at least one group prenatal care visit; however, only those women who continued with group care and completed at least three group visits were included in the CenteringHIV group for the analyses. Women in both groups, CenteringHIV and individual care, received the same support services including clinical case management and social work.
The pre-existing CenteringPregnancy prenatal curriculum was adapted for women living with HIV by adding pertinent HIV topics to each session (Table 1). Added topics included coping with an HIV diagnosis, living with HIV, HIV in pregnancy, medication adherence, importance of retention in care, HIV and contraception, HIV-specific delivery information, breastfeeding recommendations, disclosure, caring for HIV-exposed infants, finding an HIV primary care provider after delivery, linkage to pediatric infectious disease specialist for HIV testing after birth, obtaining medications, and information on pre-exposure prophylaxis for partners. Please note, a detailed curriculum is available through either the CenteringHealth Institute in Boston, MA, and from the authors for CenteringHIV.
HIV-Adapted CenteringPregnancy Curriculum
Bold indicates HIV-specific topics added to standard Centering® curriculum.
EPDS, Edinburgh Postnatal Depression Scale; IPV, intimate partner violence; PCP, primary care physician; PrEP, pre-exposure prophylaxis.
Groups comprised 4–12 women with due dates within 8 weeks of each other. Participants attended up to 10 two-hour sessions that were led by two to three facilitators including an obstetrician, nurse practitioner, and/or social worker, all with specialization in the care of women living with HIV. Facilitators had completed CenteringPregnancy facilitator training. The first 45 min of the sessions was designated for clinician-delivered individual pregnancy health assessments, whereas the remaining group time was devoted to clinician-facilitated discussions of pregnancy and HIV-related topics as outlined in Table 1.
The primary outcomes of this study were viral suppression at delivery and within 12 months postpartum, as well as retention in HIV-specific primary care during the first year postpartum. Viral suppression was defined as a viral load being “undetectable” or <20 copies/mL in our laboratory system. Viral load values were collected from the date closest to their initial obstetric intake appointment (entry to care), within 4 weeks of delivery (delivery), and the date closest to 12 months postpartum (postpartum). Postpartum retention in care was defined as at least one or two HIV primary care visit(s) within 12 months postpartum, as defined in prior publications. 16,17,35
All variables were assessed for normality. Data were summarized by mean (standard deviation) for normally distributed variables, median (interquartile range) for non-normal data, and number (%) for grouped variables. Statistical comparisons were made using chi-square/fisher exact test, t-test, and Wilcoxon rank-sum tests as appropriate.
Propensity score matching (common “PSMATCH” using statistical software SAS) was used to adjust analyses for underlying potential confounders. We performed a one-to-one matching using greedy nearest neighbor method (caliper = 0.5) using all covariates that were associated with both study treatment and outcomes. The goal of matching was to obtain similar groups of treatment and control subjects by matching individual observations on their propensity scores. Through this process, 62 patients on CenteringHIV were matched to 62 patients on individual prenatal care on their propensity score that contained age, ethnicity, education, gestational age at entry to care, history of mental health, prepregnancy ART use, and number of obstetric prenatal care visits. Matched groups were assessed for balance by plots and examining the standardized mean differences (SMDs) of the covariates used in matching. All SMDs were less than the recommended upper limit of 0.25. 36 Next, matched groups were compared on study outcomes (all binary) using conditional logistic regression analysis that is suitable for matched data. Presence of hidden bias was assessed through sensitivity analysis method detailed by Rosenbaum and Rubin. 37
Analyses were conducted in SAS Statistical Software (9.4, Cary, NC). A p value <0.05 or confidence interval (CI) excluding 1.0 was considered statistically significant.
Results
Two hundred twenty-four women living with HIV with 272 pregnancies were followed for prenatal care in our clinic from September 1, 2013, to July 31, 2019. One hundred ninety-four women met inclusion criteria for this study; 85 elected to complete group prenatal care through CenteringHIV, whereas the other 109 obtained individual prenatal care through the traditional model (Fig. 1). Of note, there were no perinatal transmissions in either group.
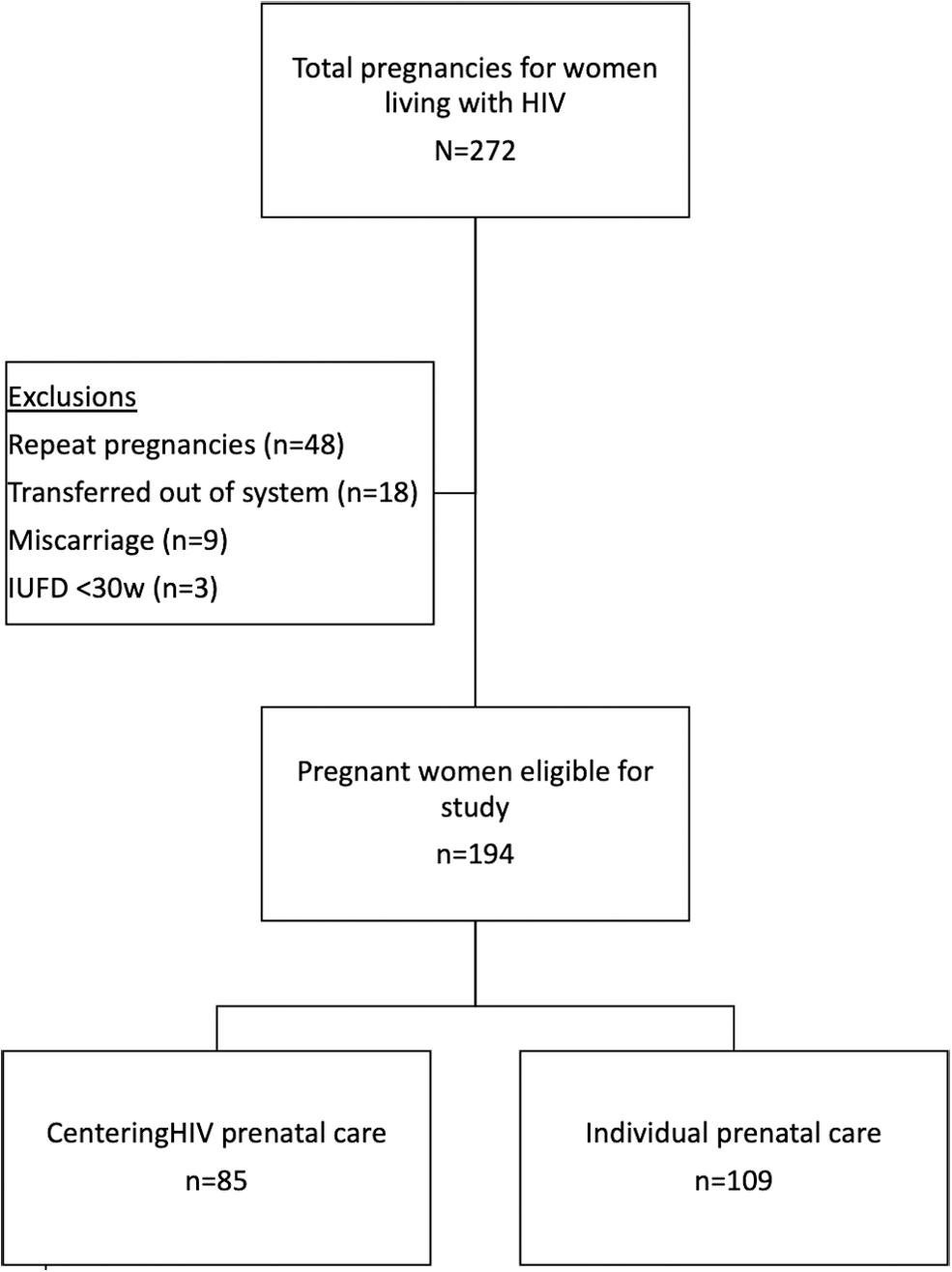
Study population. IUFD, intrauterine fetal demise.
Women who completed CenteringHIV were slightly younger, more likely to be white or Hispanic, more likely to be from Central America/Caribbean, less likely to have achieved a high school degree or equivalent, and more likely to have a history of diagnosed mental health disorder. In terms of HIV status, CenteringHIV participants also tended to be diagnosed at a younger age, before the current pregnancy, and were more likely to enter care already taking ART. Gestational age at entry to care was significantly earlier in the CenteringHIV group with 66% presenting <12 weeks EGA compared with 23% in the individual care group. See Table 2 for summary of all baseline characteristics.
Baseline Characteristics of the Study Population
Values are presented as frequency and column percentage unless otherwise noted; because of occasional missing data results, patient levels in some categoric measures add to less than the expected total.
ART, antiretroviral therapy; CHIP, Children's Health Insurance Program; SD, standard deviation.
Bold indicates significant difference between groups.
Viral suppression
Viral suppression (an undetectable viral load) did not differ between groups at entry to care (39% vs. 31%, p = 0.367). Unadjusted analyses reveal women in the CenteringHIV group were more likely to be virally suppressed both at delivery and within 12 months postpartum (Tables 3 and 5). However, after adjusting for factors identified in univariate analyses (age, education level, history of mental health disorder, EGA at entry to care, prepregnancy ART use, and number of obstetric prenatal care visits) through propensity score matching, differences for viral suppression at delivery demonstrated a positive trend, although this was not statistically significant [adjusted odds ratio (aOR) = 2.29 (95% CI 0.94–5.55), p = 0.068; (Table 5)]. CD4 counts were similar between groups at 12 months postpartum (p = 0.35).
Perinatal HIV Laboratory Results
Values are presented as frequency and column percentage unless otherwise noted.
IQR, interquartile range.
Bold indicates significant difference between groups.
Retention in care
Women in CenteringHIV attended more prenatal care visits than the individual care group (11 vs. 7 total visits, p ≤ 0.0001). The average number of CenteringHIV sessions attended by a participant was 7 (out of possible 10 total Centering sessions; Table 4). Note that additional individual appointments were scheduled between group sessions based on clinical need (resulting in difference between average 7 Centering sessions, but 10 total prenatal visits).
Perinatal Retention in Care Results
Values are presented as frequency and column percentage unless otherwise noted.
Bold indicates significant difference between groups.
Crude and Adjusted Odds Ratios for Primary Outcomes
aOR is from conditional logistic regression analysis from 62 pairs of subjects (N = 124) matched on their PS. PS contained age, education level, ethnicity, history of mental health disorder, estimated gestational age at entry to care, prepregnancy ART use, and number of obstetric prenatal care visits.
aOR, adjusted odds ratio; CI, confidence interval; OR, odds ratio; PS, propensity score.
Bold indicates significant difference between groups.
The number of women who attended at least one or two obstetric postpartum visits did not differ between the groups (Table 4).
Unadjusted analyses demonstrate increased odds of attending at least one and at least two visits with HIV primary care providers within 12 months postpartum for women participating in CenteringHIV (Tables 4 and 5). After adjusting for covariates through propensity score matching, the odds of attending at least one HIV primary care visit postpartum remained significantly increased among CenteringHIV as compared with individual care group [aOR = 2.71 (95% CI 1.14–6.46); p = 0.02; (Table 5)].
Sensitivity analysis
We examined the validity of propensity score adjustment by sensitivity analysis that essentially shows whether an unobserved covariate may change the odds of receiving treatment to a certain degree and as a result may change the findings of the study. Overall, our results indicate while there is an effect of CenteringHIV on the outcome variables, presence of hidden bias cannot be ruled out.
Discussion
Compared with individual prenatal care, women living with HIV who participated in CenteringHIV group prenatal care were significantly more likely to have at least one HIV primary care visit during the first year postpartum, and had a positive trend toward viral suppression at delivery.
Although group prenatal care has been implemented as a way to foster engagement in care and potentially impact maternal and neonatal outcomes in the general obstetric population, its use in disease-specific populations has been less well studied (one example is for women living with diabetes). 38 We know of only one other program that has evaluated the effects of the Centering model in women living with HIV. Potter et al. 39 compared Centering with traditional prenatal care and did not find improvement in viral suppression or postpartum retention in care. This could be attributed to a much smaller sample size—14 women in Centering group, which may be inadequate to show a significant difference. 39
In a previous cohort in our own institution, we demonstrated improvement in perceived social support and decreased depression after participating in CenteringHIV. 40 However, the study design was limited to assessing pre- and postparticipation scores in women who participated in CenteringHIV, without comparison with women who participated in individual prenatal care.
Group prenatal care has plausibility as a mechanism to improve viral suppression and retention in care. In a recent review and discussion of the issue of postpartum retention in care, areas of need were identified to address the lack of postpartum retention among women living with HIV in the United States. 19 The five areas identified were increased provider and patient awareness of the issue of poor postpartum retention in care, improved care coordination using existing resources, involvement of perinatal case management, implementation of peer support interventions, and use of technology-based interventions to engage women in care.
CenteringHIV addresses these areas in multiple ways. Sessions in our program address the importance of postpartum retention by inviting HIV primary care physicians to come meet the patients in person during a group session. The HIV physician discusses what to expect postpartum; emphasizes the benefits of continuing postpartum care and the need for continued adherence to ART and maintenance of viral suppression for their own long-term health; and provides an opportunity for the patients to ask questions. This conversation builds on the topics of adherence and the importance of viral suppression previously discussed in other sessions, and emphasizes their impact on long-term disease control after delivery.
Perinatal case management and care coordination with outside resources are also built into our CenteringHIV curriculum by actively involving our clinical social worker in most sessions and ensuring the social worker is available afterward to address concerns. Having an experienced clinical social worker who has worked in the general HIV care system and is familiar with HIV-specific resources is invaluable. Although these same services are available to our patients who participate in individual prenatal care, the Centering model allows increased duration of contact between the social worker and the women. Centering is also a peer support intervention. Cohort studies examining Centering have revealed that participation improves postpartum care retention and health care utilization in the general obstetric population. 41,42
Finally, Centering incorporates use of available online resources in multiple ways to enhance care. Educational videos covering HIV topics such as viral load, CD4 counts, viral suppression, and intimate partner violence are incorporated into sessions as conversation starters. The Centering model enhances the quality of prenatal care for pregnant women living with HIV through a combination of the mechanisms already mentioned, and the positive results seen in this study reflect this. In our experience, group care among women living with HIV provides a safe environment to discuss HIV-related concerns, encourages social support, and normalizes HIV. Stigma has been identified as a key determinant of retention in care for persons living with HIV, 43,44 and women exposed to this model report feeling less stigmatized, which may lead to more positive health behaviors such as staying in care.
Despite potential benefits of this model, we realize that implementing group prenatal care may require modification, and may not be completely feasible in all settings, especially in areas with limited number of pregnant women living with HIV. Innovation is needed to obtain similar support structures for patients in areas where larger group meetings are not possible. Further, research needs to continue to elucidate factors contributing to suboptimal viral suppression and poor retention rates in pregnant women who are living with HIV, due to far-reaching impact of these factors on long-term individual and family health. Only then can well-designed trials of novel health interventions and prenatal care delivery models attempt to achieve improved outcomes.
There are several limitations to note that could mitigate the strength of this study's results. As a single-site cohort study, our data reflect trends in one region's patients living with HIV and may not be indicative of trends in other geographic areas. We must note again that there were significant demographic differences between the CenteringHIV group and the individual care group at baseline. For instance, women in the CenteringHIV group were more likely to be Hispanic. There are data to support that CenteringPregnancy can increase rates of postpartum health care utilization in Hispanic women, which could indicate a potential demographic skew in our results. 41 Controlling for several of these key differences between the study groups using multi-variable logistic regression revealed persistence of statistically significant results. However, the existence of variance between the two groups could conceal important traits or differences that made patients more likely to choose CenteringHIV over traditional care. Our sensitivity analysis shows that our result is sensitive to possible deviations from the identifying unconfoundedness assumption, and hence, some caution when interpreting our results is warranted. Further study is needed to better understand the factors that influence a woman's choice to participate in group prenatal care.
The majority of women in our program sought postpartum primary HIV care within our county system, which allowed us to track postpartum visits. However, a small number in both the CenteringHIV and traditional groups opted to go elsewhere and would, therefore, have fallen into the category of “no follow-up care.” We are unable to obtain viral suppression or retention in care information for these patients, which represents an additional source of bias in these data. Although this study—a retrospective analysis in which participants self-selected their treatment group—provides meaningful results, a randomized prospective trial would strengthen the investigation of potential impact on viral suppression, retention in care, and other important health outcomes.
In summary, participation in HIV-adapted group prenatal care can positively influence achievement of viral suppression and postpartum retention in care for pregnant women living with HIV. Owing to the far-reaching implications of such improvements, from improved long-term maternal health outcomes to decreased perinatal and partner transmission rates, we believe that group prenatal care should be considered for this high-risk vulnerable population.
Footnotes
Author Disclosure Statement
All included authors report no disclosures or conflicts of interest (competing interests, personal financial interests, funding, employment, or other competing interests).
Funding Information
No financial support was received for any portion of this project.