
Abstract
Pre-exposure prophylaxis (PrEP) prevents HIV, but low rates of retention in care limit its effectiveness. We conducted a prospective survey-based study to investigate reasons for PrEP disengagement among men who have sex with men attending a sexual health clinic at a large urban academic medical center in New York City who were lost to follow up; surveys asked about current PrEP status, reasons for disengagement, attitudes toward PrEP, substance use, sexual practices, and behavioral/social determinants of health. Outreach attempts were made to 634 patients; majority of eligible participants were unable to be contacted (59%). Among those who agreed to participate (n = 175), 21% asked to re-establish care. Among those who completed the questionnaire (n = 86), 36% were taking PrEP. The most common reasons for PrEP discontinuation were cost/lack of insurance coverage (31%), decreased HIV risk perception (29%), and side effects (16%). Among those with decreased perception of risk, 62% were less sexually active, 38% were no longer engaging in anal sex, and 31% were using condoms for prevention. Participants reported that free medication (60%), having a sexual partner recommend PrEP (13%), and being able to receive PrEP from a primary care provider (13%) would encourage restarting PrEP. Findings were limited by low response rate (12% of eligible subjects completed the survey) and lack of Spanish-language questionnaires. Understanding reasons for loss-to-PrEP follow-up is essential for HIV prevention. Many people lost to follow up still desired PrEP, underscoring the importance of outreach, benefits navigators, and expansion of PrEP into primary care settings.
Introduction
Pre-exposure prophylaxis (PrEP) prevents HIV acquisition, but its effectiveness depends on adherence. 1 Many eligible patients initiate PrEP, but retention rates in PrEP programs are poor; 6 months after PrEP initiation, 35% to 74% of individuals remain in sexual health care. 2 –5
Among men who have sex with men (MSM) who discontinue PrEP or choose not to use PrEP, significant socioeconomic and racial disparities persist. Sociodemographic factors associated with lower rates of PrEP use and adherence include older age, lower level of education, and lack of insurance. 6 African American/Black and Hispanic MSM are more likely to stop PrEP than White MSM, contributing to the high HIV incidence among MSM populations of color. 7,8
Reasons for disengagement in sexual health care are multifactorial and influenced by individual psychosocial factors as well as structural barriers. The decision to stop PrEP is often driven by a decrease in self-perceived risk of HIV, but HIV incidence remains high among individuals who discontinue PrEP, suggesting that self-perception may not accurately reflect risk. 8 –11 Many programs that provide HIV prevention services also provide comprehensive health care, patient navigators, benefits navigation, mental health care, and substance use services to help engage individuals in care. 4 Systemic barriers leading to disengagement include incomplete insurance coverage for PrEP and limited availability of sexual health appointments. 2,3,8,10,11
Previous studies have investigated reasons for disengagement using retrospective chart review and case reports based on structured qualitative interviews. 2,3,11 There is a lack of prospective follow-up data on reasons for disengagement in care. In this study we present results of a survey-based study to understand the experiences and motivations of MSM who have been out of PrEP care for at least 6 months.
Methods
Program description
This study was performed in the HIV Prevention Program (HPP), a sexual health clinic at a large urban academic medical center in northern Manhattan. In the surrounding community, 72% of residents identify as Latinx or Hispanic, 20–30% of families report an annual income below the poverty line, and HIV prevalence is 2.67%. 12 HPP provides comprehensive sexual health services and prescribes PrEP in accordance with New York State Department of Health and New York City Department of Health and Mental Hygiene guidelines.
HPP offers additional clinical services, including PrEP coordinators, benefits navigators, social workers, and psychiatric providers. 4 Navigators facilitate insurance enrollment and applications for free PrEP through industry-sponsored programs and also provide adherence support through phone calls and text messages. After the initial PrEP visit, all patients on PrEP have a 1-month follow-up and appointments every 3 months thereafter.
Study description and recruitment
HPP records were reviewed to identify all MSM who initiated PrEP between July 2015 and June 2018 and had not attended a follow-up visit in 6 months or longer. Eligible participants were called by HPP providers between July 2018 and June 2019 and asked to complete an online questionnaire. Questionnaires were sent through text message or e-mail and participants who completed the survey were compensated with a $10 e-gift card. Questionnaires were only available in English.
Survey development
Survey questions were developed based on clinic experience and literature review; questionnaires were piloted and refined with input from HPP staff. Questions included current PrEP status, reasons for care disengagement, attitudes toward PrEP, substance use, sexual practices, and behavioral and social determinants of health. Responses were augmented with data routinely collected by the clinic, including demographic information, social determinants of health, sexual history, PrEP start/stop dates, visit frequency, and medication refill history.
Ethical consideration
This study was approved by the Columbia University Institutional Review Board.
Results
In total, 634 patients, 54% of all MSM who initiated PrEP during the study period, were identified as lost to follow up for unknown reasons at least 6 months after initiating PrEP. Over 800 calls were made to eligible participants. Participants could receive up to three outreach calls. The majority of eligible participants were unable to be contacted by phone (59%). In total, 175 (25%) agreed to participate and, of those, 86 (12% of all eligible participants) completed the questionnaire (Fig. 1).
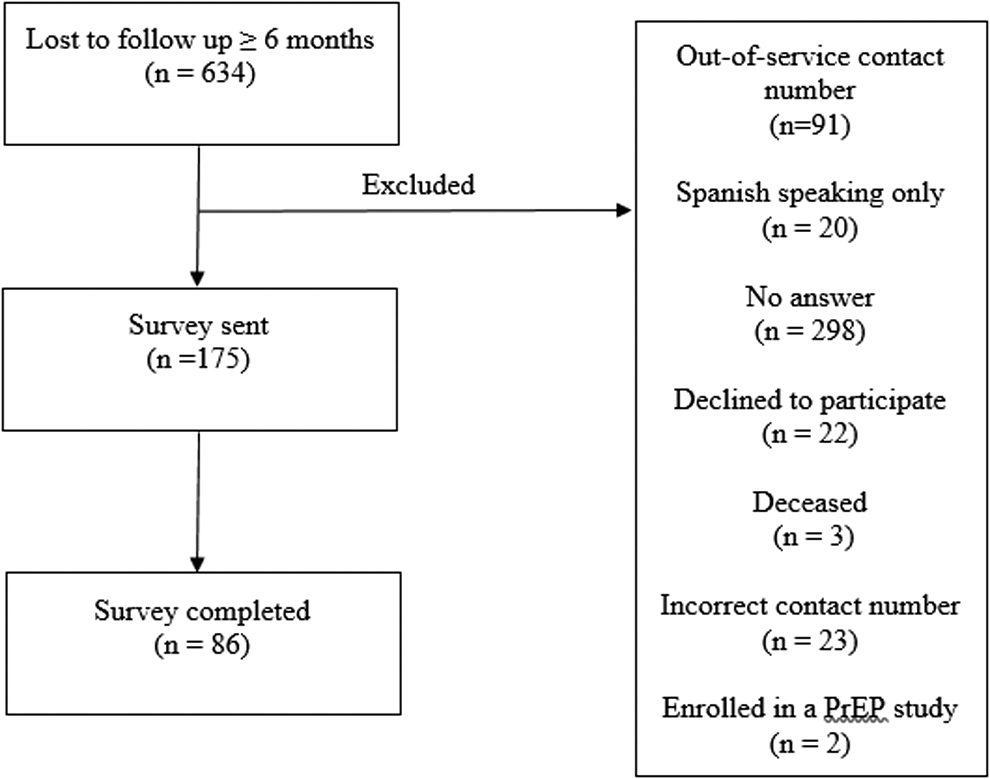
Flow diagram of study inclusion. PrEP, pre-exposure prophylaxis.
The median age of all participants was 30 years old (range, 20–68 years old). Twenty (23%) self-identified as African American/Black and 26 (30%) identified as Hispanic. The majority had health insurance (72%), although a significant proportion had experienced a recent insurance change (41%). Majority reported earning <$40,000 per year (90%) (Table 1). Fear of acquiring HIV was the most commonly reported motivation for first starting PrEP (56%), followed by recommendation from a friend (29%) (Table 2).
Demographic and Behavioral Characteristics of Pre-Exposure Prophylaxis Users Lost to Follow Up, n (%), Median (Interquartile Range)
Variables with a significant p value (p < 0.05) are shown in bold.
PrEP, pre-exposure prophylaxis.
Reasons for Initially Starting Pre-Exposure Prophylaxis Among Pre-Exposure Prophylaxis Users Lost to Follow Up
Variables with a significant p value (p < 0.05) are shown in bold.
PrEP, pre-exposure prophylaxis.
Fifty-five patients (64%) had stopped taking PrEP at time of survey; 31 (36%) reported actively taking PrEP despite having no visits or refills from HPP during the prior 6 months. Individuals continuing PrEP reported receiving prescriptions from their primary care provider, moving out of the area and establishing care with a new provider, changing clinics locally, and/or using a friend's medication.
Patients who were not taking PrEP were less likely to have PrEP insurance coverage than those who were still taking PrEP (62% vs. 90%, p = 0.005). The number of sexual partners and the number of new sexual partners in the 30-day period before survey completion were higher in patients who continued PrEP (median 1.0 vs. 3.0, p = 0.002; median 0.5 vs. 2.0, p = 0.003, respectively). Sexual position preferences, condom use, and anal sex after alcohol consumption did not differ significantly based on PrEP usage at time of survey. Participants taking PrEP did report higher use of amyl nitrites (52% vs. 18%, p = 0.001), but other substance use did not differ significantly.
Respondents taking PrEP at time of follow-up survey were more likely to report a high self-perceived risk of acquiring HIV (45% vs. 15%, p = 0.002); no other motivations for PrEP use were significantly different between those who remained on PrEP and those who had discontinued PrEP.
Among patients no longer taking PrEP, the most common reasons for stopping were medication cost or problems with insurance (31%), decreased perception of HIV risk (29%), and side effects (16%). No patients reporting stopping PrEP due to HIV infection or to stigma associated with taking PrEP. Among patients who reported low perceived risk of HIV, 62% attributed perceived low risk to decreased sexual activity, 31% to consistent condom use, and 38% to lack of receptive anal sex (Table 3).
Reasons for Stopping Pre-Exposure Prophylaxis Among Pre-Exposure Prophylaxis Users Lost to Follow Up
Includes at least one of the below reasons for decreased perceived HIV acquisition risk.
PrEP, pre-exposure prophylaxis.
Participants were also asked about reasons to consider restarting PrEP. The most common motivations included providing PrEP free of charge (60%), recommendations from a sexual partner (13%), and making PrEP available from participant's primary care provider (13%). Six participants (11%) would consider restarting PrEP if visits were less frequent, and another six (11%) cited increased reminders from clinic team as a motivation to resume (Table 4).
Motivations to Restart Pre-Exposure Prophylaxis Among Pre-Exposure Prophylaxis Users Lost to Follow Up
PrEP, pre-exposure prophylaxis.
Of the 175 patients who agreed to participate in the survey when initially reached by phone, 37 (21%) requested to be contacted by a care coordinator to re-establish care.
Discussion
To our knowledge, we present the first published data regarding a prospective survey of out-of-care patients lost to PrEP follow-up. We found that individuals who disengaged from PrEP care are challenging to reach, but, among those able to be contacted, approximately one-third (36%) were in fact actively taking PrEP.
In alignment with prior studies, we found that cost of medication and changes in insurance factored into decisions to stop PrEP, despite the availability of health care navigators and PrEP funding support at our clinic. 11,13 –15 These findings further highlight the importance of raising awareness about support services and resources, such as industry- or grant-funded PrEP, which are available to patients at the time when insurance coverage changes.
After financial barriers, change in perceived risk of HIV acquisition was the second most frequently reported reason for stopping PrEP. Many patients described changes in behavior associated with decreased risk of HIV acquisition. Given that behavior changes over time, with periods of high sexual activity that may follow periods of lower sexual activity, counseling patients on risk, shared decision making about PrEP, and counseling about continuing engagement in regular sexual health care for those temporarily off PrEP are critical before discontinuation of PrEP. 10 For patients with changing risk factors for acquisition, on-demand PrEP, which has been shown to be effective at reducing transmission, may be another attractive option by decreasing pill burden and frequency of appointments and improving adherence. 16 –18
Substance use is an established risk factor for HIV acquisition, but the impact of drug and alcohol use on PrEP adherence remains unclear. 2,19 Our study did not show a clear relationship between substance use and PrEP engagement. It may be difficult to draw conclusions on this issue, however, given the small sample size; for example, our study only included one participant who injected drugs. Further studies are needed.
Limitations of our study include lack of Spanish-language questionnaires and low response rate to phone outreach. Barriers to contacting participants included out-of-service numbers and lack of response to voicemail messages and follow-up calls. These issues highlight the importance of establishing multiple ways to reach patients including phone, text messaging, e-mail, or social media, which may be appealing to younger patients. 20,21 When reached, nearly a fifth of patients expressed interest in having a navigator call them to schedule an appointment for re-engagement, demonstrating the importance of coordinator engagement support. Identifying loss to PrEP follow-up and HIV prevention care was imperfect, as several participants had established care with another provider.
Our findings should be interpreted in the context of other recent data investigating PrEP disengagement. Cis-female gender, younger age, and heterosexuality have been identified as risk factors for PrEP loss to follow up. 22 Although some structural barriers described in our study, particularly cost and insurance coverage, are likely generalizable contributors to sexual health disengagement, further investigation of reasons for disengagement among these key demographic groups is needed.
Our study was conducted before the COVID-19 pandemic and widespread implementation of telehealth programs. Recent data have demonstrated that patients in an HIV primary care setting are willing to attend telehealth visits, and overall visit nonattendance decreased after the pandemic transition to telehealth. 23 Telehealth may provide a promising modality to increase retention in care by reducing barriers to care and providing increased convenience for patients. 24 The effect of the implementation of telehealth on engagement in HIV prevention and sexual health programs warrants further exploration.
Reasons for disengagement combine structural and personal motivations. Understanding barriers to PrEP adherence may facilitate identification of individuals at highest risk for disengagement and implementation of interventions to promote persistence in PrEP and sexual health care.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under award numbers 5UM1AI069470-14 (M.E.S., J.Z., E.L.S., D.A.T.), K23AI150378 (J.Z.), and L30AI133789 (J.Z.).