
Abstract
Poor compliance with medications is a growing concern in geriatric care and is increasingly more relevant among people living with HIV (PLWH) as they age. Our goal was to understand geriatric conditions associated with antiretroviral therapy (ART) nonadherence in a Medicare population of older PLWH. We analyzed Medicare data from PLWH aged 50 years or older who were continuously enrolled in fee-for-service Medicare from January 1, 2014 to June 30, 2015. Prevalent geriatric conditions (dementia, depression, falls, hip fracture, sensory deficits, osteoporosis, orthostatic hypotension, urinary incontinence, frailty) were identified in January 1, 2014–December 31, 2014. ART nonadherence was defined as <80% proportion of days covered (PDC) by at least two ART medications in January 1, 2015–June 30, 2015. We examined geriatric condition association with nonadherence using lowest Akaike Information Criterion multi-variate logistic models, controlling for age, sex, race, census region, substance use, Medicaid eligibility, and polypharmacy. Of 8778 PLWH, 23% (n = 2042) had <80% PDC. The average age was 60 years (standard deviation ±8), and >70% were males. In adjusted models, age was not associated with nonadherence, frailty status was the only geriatric condition associated with nonadherence [robust: reference, prefrail odds ratio (OR): 0.97, confidence interval (95% CI) 0.86–1.10, frail OR: 1.34 95% CI 1.11–1.61], and odds of nonadherence were lower for polypharmacy [OR: 0.48 (0.43–0.54)]. Our findings suggest that patient-centered care plans aimed at improving ART adherence among older PLWH would benefit from long-term surveillance; a deeper understanding of the role of frailty and polypharmacy, even at chronologically younger ages in PLWH.
Introduction
High adherence with HIV antiretroviral therapy (ART) is essential if people living with HIV (PLWH) are to achieve viral suppression and realize the full benefits of ART. ART is indicated no matter the patient's age or symptoms. 1 Older age has been associated with better ART adherence, 2 –4 but it is important to consider that older PLWH are a mix of long-term survivors and people diagnosed with HIV at older ages; 20% of new infections in the United States are among people aged 50 or older. 5 A summary of HIV cohort studies demonstrated the consistency with which older PLWH are at increased risk for comorbidities such as cardiovascular disease, dyslipidemia, and hypertension; older protease inhibitor-based ART regimens contribute to risk for cardiovascular disease 6 and the latter potentially linked to greater risk for heart attack. 7 Although HIV may be one of multiple factors to explain this elevated risk for comorbidities, PLWH with comorbid burden are younger as a cohort than people without HIV and more often have high risk behaviors such as smoking and misuse of drugs and alcohol that also make them more likely to have certain comorbidities. The summary is that >50% of PLWH are older than age 50, and they have a mix of comorbidities that may accumulate before an HIV diagnosis and subsequent ART initiation. 7,8
Accumulating comorbidities have been associated with ART nonadherence. 2,9 Particularly true for PLWH with severe illness, cognitive impairment, including deficits in executive function, and memory impairment; 3,4 having neurological or psychological impairment PLWH were 2.5 times more likely to be nonadherent. 3 However, other studies have shown contradicting associations of nonadherence with mental health conditions. 4,10 In particular Barclay et al. 4 showed higher likelihood of nonadherence among those with diagnosed depression but Mutchler et al. 10 demonstrated lower likelihood with self-reported depression among a subgroup of older Black men who have sex with men. 11 Moreover, Mann et al. 11 showed lower ART adherence for PLWH and diabetes but not with HIV and hypertension or hyperlipidemia. 11 It has been shown that increasing comorbidities raise the risk of ART nonadherence by up to 25%. 12 One recent study showed that having incrementally more comorbidities there is a complimentary reduction in likelihood of adherence. 9 However, the lack of agreement across the literature and inconsistent consideration of non-ART medication use to treat comorbidities suggest that there are nuances to these associations demanding further confirmation and exploration of other subgroups.
Geriatric conditions are a subgroup within comorbidities that are also accumulating among older PLWH. There is relative lack of literature examining geriatric conditions associated with ART nonadherence, which potentially misses an opportunity for improving health care. Geriatricians specialize in treatment of geriatric conditions and have been incorporated into select HIV clinics around the world. 13,14 Despite these programs being highly heterogeneous in their goals, care linkages, and overall implementation, 14 geriatric care in HIV clinics has been well received by patients. 13 Yet, universal implementation of geriatric assessments and treatment of geriatric conditions are not included as standard for older PLWH, particularly if they are thought to be of younger chronologic ages than more traditional geriatric patients. 14 To that end, a previous study found that 23.1% of older adults have at least two geriatric conditions, 15 while more than half of aged 50+ people with HIV have at least two geriatric conditions. 16 –18
Geriatric conditions, including but not limited to frailty, depression, and dementia, are distinguished from other comorbidities in that any one geriatric condition can result from multiple pathways of organ system dysregulation or impairment. 19 In conjunction with comorbidities, 20 accumulating geriatric conditions amount to reduced physiologic reserve or frailty. 16,19,21 Frailty is a geriatric condition in its own right. One way it can be measured is using a deficit accumulation frailty index (FI), which represents the total burden of age-related health deficits and is dynamic in time. 22,23 Among PLWH, frailty has been shown to result from long-term ART, an AIDS diagnosis, and cognitive impairment. 24 As geriatric conditions accumulate so too do the medications to treat them resulting in polypharmacy, which is often considered a geriatric condition unto itself. Older PLWH are predisposed to polypharmacy and take approximately three more medications than age-matched non-HIV infected individuals. 12,17,25,26 Polypharmacy has been linked to nonadherence with certain medications, but not ART. 27
Further developing an understanding of geriatric conditions among PLWH means greater opportunities for clarifying the role of geriatrics in HIV care, including anticipating and/or preventing issues with ART adherence as the HIV population ages. To that end, geriatric conditions are more often studied as outcomes. For example, viremic HIV, long-term ART, and older age are independently associated with osteoporosis, 28 and polypharmacy is associated with frailty. 29 However, as previously noted, geriatric conditions may exist before HIV diagnoses and ART initiation; if comorbidities are associated with nonadherence it is possible that geriatric conditions are as well. Clarifying the role of geriatric conditions within the literature examining associations with nonadherence will be important for resource allocation and strategic approaches to geriatric HIV care.
The objective of this study was to understand whether geriatric conditions are associated with ART nonadherence among a Medicare population of older PLWH. We hypothesized that the presence of frailty and other geriatric conditions will be associated with ART nonadherence.
Methods
Data sources
We used an enhanced 5% sample of 2014–2016 Centers for Medicare and Medicaid Services (CMS) claims data, which ensures that anyone who enters the sample stays in the sample for longitudinal follow-up. These data include the following: chronic conditions data warehouse (CCW) files, the master beneficiary summary file, Medicare Part A inpatient claims, Medicare Part B outpatient claims, and Part D prescription claims. The CCW captures historical data on first diagnosis of chronic conditions, even that predate these data.
Population
PLWH were identified as anyone in 3 years of data having at least one of the following: (1) one diagnosis for HIV or AIDS in inpatient claims or (2) two diagnoses at least 90 days apart in outpatient claims or (3) at least two antiretroviral medications prescribed in the 6 months before the index date (n = 20,572); this enables capture of anyone without diagnosis codes. We excluded a total of 10,015; that included anyone younger than 50 (n = 5971), deceased before the index date (n = 439), hospital or nursing home inpatients at the index date (n = 322), who lived outside of the 50 US states in 2015 (n = 1332), or who were not eligible for Medicare (A, B, D) continuously from January 1, 2014 to June 30, 2015 (n = 5277). Medicare eligibility ensures longitudinal follow-up. We also excluded anyone with no ART after the index date (n = 1779) because we are defining adherence as medication implementation (definition details below). 30 Our final sample included 8778 PLWH on January 1, 2015, the index date.
Covariates and characteristics
The 2015 master beneficiary summary file provided baseline age, race (non-Hispanic White, non-Hispanic Black, Other), sex, US census region [Northeast, South, Midwest, West (including Hawaii and Alaska)], and if a person was dually eligible for Medicaid for at least 50% of the year before the index date; Medicaid dual eligibility is the only proxy for income available in these claims data. Multi-morbidity was an indicator for having two or more conditions (other than HIV) in the CCW with diagnosis dates before the index date. Polypharmacy was calculated as five or more anatomic therapeutic chemical third level classes of drugs (ATC3) for at least 90 days in the 6 months before the index date, excluding ART drugs. History of substance use was calculated as having at CCW date before the index date for at least one of: tobacco, alcohol, opioid use disorder, or use of other drugs.
Exposures
Geriatric conditions assessed in the 1-year preceding the index date were identified by one diagnosis in inpatient claims or two diagnoses in outpatient claims at least 90 days apart. Geriatric conditions included the following: Alzheimer's and related dementias, depression, falls, hip fracture, sensory deficits (eye/ear), osteoporosis, orthostatic hypotension, and urinary incontinence. Frailty was measured using a validated claims-based FI from the 1-year look back period. Frailty categories were determined using common cut-points to classify people as robust (FI <0.15), prefrail (0.15 ≤ FI <0.25), and frail (0.25 ≤ FI). 22,23
Outcome
Nonadherence was defined as a function of dosing history or implementation of medication. 30 We measured implementation as the proportion of days covered (PDC) by at least two antiretroviral medications in the 6 months following the index date, excluding anyone without ART at the index date. 31 A PDC of 80% or better was used because of higher potency of newer medications; 2 sensitivity analyses use 85%; and 95% PDC were also performed. We chose 6 months to allow for prescriptions longer than 30 days. 32
Statistical analysis
Chi-squared test for independence determined multi-morbidity was significantly correlated (p < 0.01) with all variables, but sex, and so was not considered for multi-variate regression models. Polypharmacy and Medicaid eligibility were correlated (p < 0.01) with some, not all, model variables. They were stepped into regression models because they were adjudicated as clinically meaningful given that the focus of the study is medication and both represent factors associated with medication access 33 and adherence. 27 All geriatric conditions were assessed in logistic regression with nonadherence as the outcome. Bivariate analysis of each geriatric condition and covariates was followed by adjusted logistic regression of all geriatric conditions on nonadherence. To avoid overfitting, geriatric conditions were chosen based on lowest Akaike Information Criterion (AIC) where age, sex, race, census region, history of substance use, Medicaid eligibility, and polypharmacy were forced. This study has been approved by the Hebrew SeniorLife Institutional Review Board.
Post hoc analysis
Frailty status was the only geriatric condition in all adjusted models. To try to understand health profiles for frail and prefrail PLWH by adherence status, we calculated the difference between the proportion of nonadherent and proportion of adherent PLWH that had each of a list of geriatric and chronic conditions among the frail and among the prefrail groups.
Results
Of 8775 PLWH, the average PDC was 86% (standard deviation, 34 50.1%; median, 94%; range, 0.5%–100%; Fig. 1). Across all PLWH, 51% (n = 4512) had <95% PDC, 29% (n = 2552) has <85% PDC, 23% (n = 2042) had <80% PDC, where mean PDC was 73%, 59%, and 53%, respectively (Table 1). The average age was 60.1 years (standard deviation 7.6); nonadherent groups had mean age range 59.6 (7.5) to 59.8 (7.5). More than 70% of all nonadherent groups were males (95% PDC: 73%; 85% PDC: 72%; 80% PDC: 71%) and a plurality was Black (95% PDC: 44.9%; 85% PDC: 49.1%; 80% PDC: 51.1%). Approximately 30% of nonadherent groups had a history of substance use (95% PDC: 29%; 85% PDC: 31%; 80% PDC: 33%). Figure 2 shows the distribution of geriatric conditions among nonadherence groups where depression (95% PDC: 22%; 85% PDC: 23%; 80% PDC: 22%) and frailty status (95% PDC: prefrail: 32%, frail: 11%; 85% PDC: prefrail: 33%, frail: 12%; 80% PDC: prefrail: 32%, frail: 12%) were the most common.
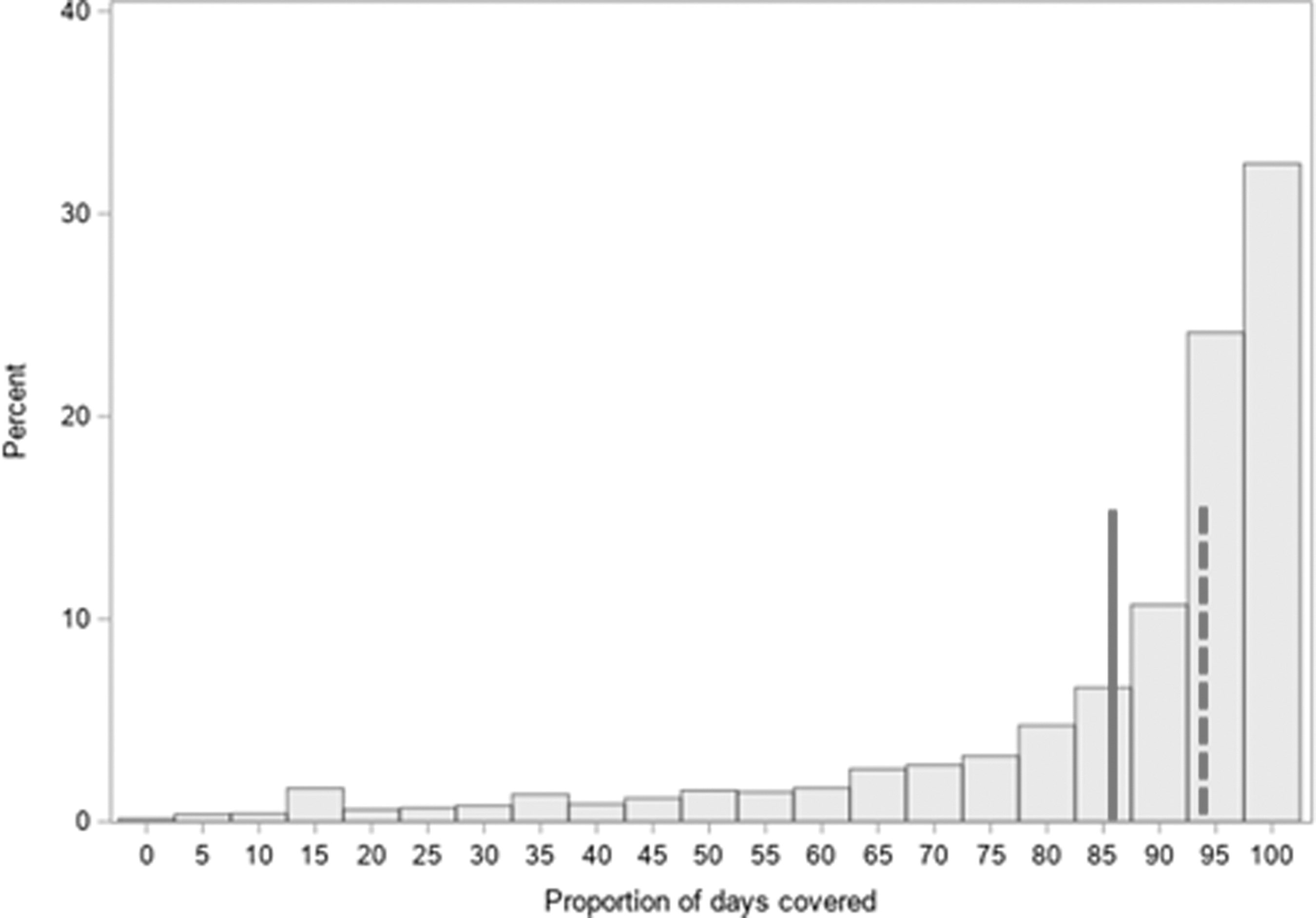
Distribution of the proportion of days covered across all older PLWH (n = 8778). The lines denote the mean (solid) and median (dotted) proportion of days covered: 86% (standard deviation 50.1%), 94%. PLWH, people living with HIV.
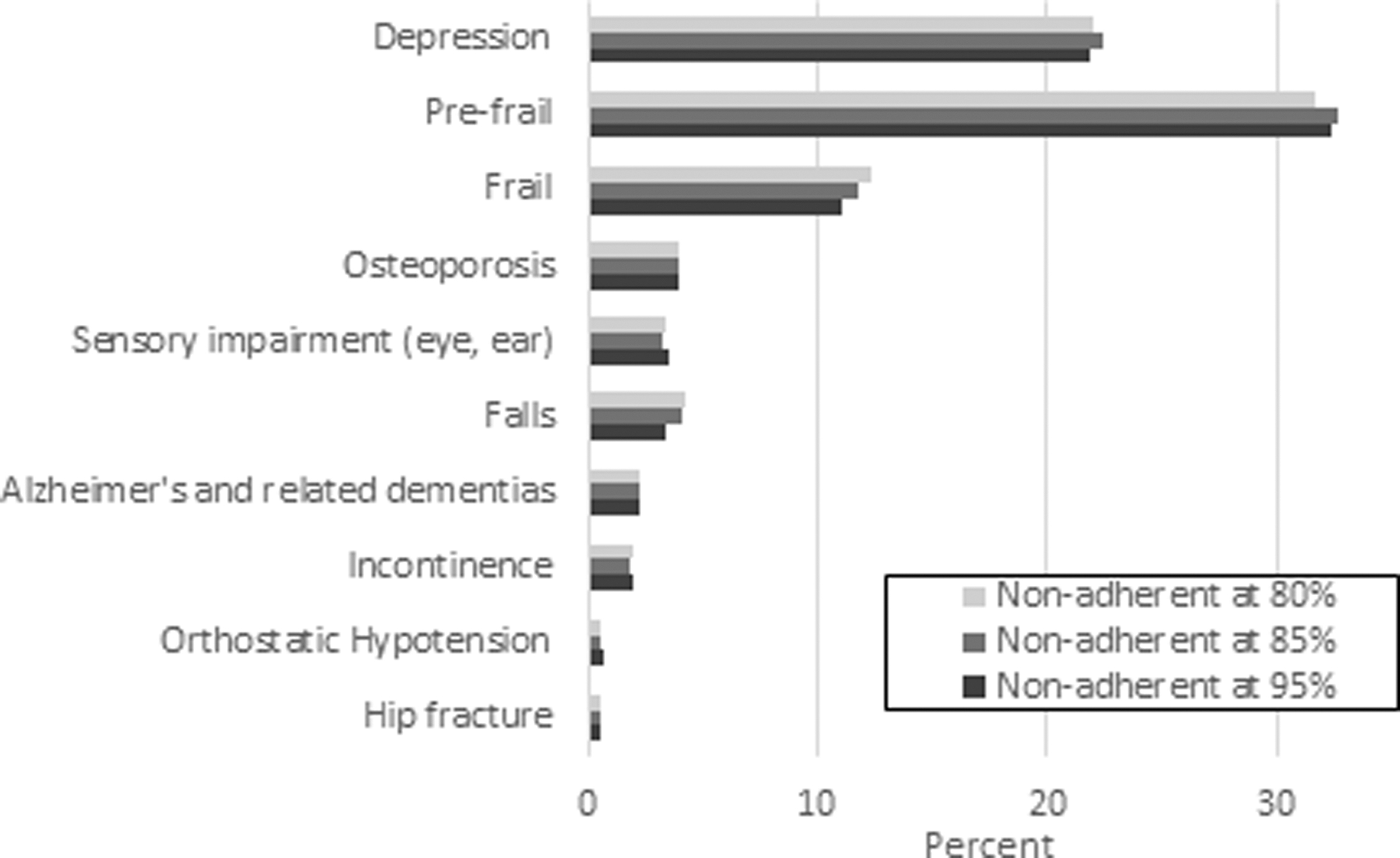
Percent of each nonadherence group having geriatric conditions.
Descriptive Statistics by Nonadherence Threshold
Multi-morbidity = having ≥2 conditions other than geriatric conditions with diagnosis dates before January 1, 2015 in the chronic condition data warehouse files.
PDC covered where nonadherence was defined as <95%, 85%, or 80% of days in the 6 months after January 1, 2015 covered by 2+ antiretroviral medications.
PDC, proportion of days covered; PLWH, people living with HIV; SD, standard deviation.
Tables 2 and 3 show the bivariate and main analyses, respectively. The main adjusted logistic regression used <80% PDC as the threshold for nonadherence. Age was marginally not associated with nonadherence, and frailty was the only geriatric condition significantly associated with nonadherence [robust: reference, prefrail odds ratio (OR): 0.97 95% confidence interval (CI) 0.86–1.10, frail OR: 1.34, 95% CI 1.11–1.61]. No other geriatric conditions were associated with nonadherence; despite that falls were included in the lowest AIC model. A history of substance use (OR 1.59, 95% CI 1.41–1.79) and races compared to White were associated with increased odds of nonadherence (Black OR: 1.77, 95% CI 1.57–2.00; Hispanic OR: 1.20, 95% CI 1.02–1.42; Other races OR: 1.85, 95% CI 1.36–2.50). These findings persisted in sensitivity analyses (Table 4).
Bivariate Logistic Regression Across Three Thresholds for Nonadherence
Bold = p value <0.05.
PDC, proportion of days covered; Ref., reference category.
Adjusted Odds Ratios for Nonadherence Using the Cutoff <80% of Days Covered
Bold = p value <0.05.
These variables were excluded from the lowest AIC model.
Model 1 = independent effects of demographic characteristics.
Model 2 = Model 1 + independent effects of dual eligibility.
Model 3 = Model 2 + independent effects of polypharmacy.
Model 4 = Model 3 + All 9 geriatric conditions (frailty, Alzheimer's and related dementias, depression, falls, hip fracture, sensory impairment, osteoporosis, orthostatic hypotension, urinary incontinence) selected down by lowest AIC.
AIC, Akaike Information Criterion; ART, antiretroviral therapy; CI, confidence interval; dually eligible, eligible for both Medicare and Medicaid; OR, odds ratio; PDC, proportion of days covered; Ref., reference category.
Sensitivity Analysis: Multi-Variate Logistic Regression Among Different Levels of Nonadherence
Bold = p value <0.05.
PDC, proportion of days covered; Ref., reference category.
Post hoc analysis is presented in Table 5; there are four conditions among prefrail PLWH that have significantly different proportions across all adherence thresholds: polypharmacy (−12, −18, −18 or 12 and 18 percentage points lower among nonadherent than the adherent in the 95%, 85%, and 80% thresholds, respectively), cataracts (−3, −5, −5), hyperlipidemia (−7, −10, −2), and hypothyroidism (−3, −3, −5). In addition to these four, there were two more conditions (rheumatoid arthritis, benign prostatic hyperplasia) which had significantly different proportions across the nonadherent and adherent prefrail group at the 95% PDC threshold, there were eight more conditions [osteoporosis, urinary incontinence, myocardial infarction (MI), diabetes, glaucoma, ischemic heart disease, rheumatoid arthritis, benign prostatic hyperplasia] among the prefrail group at the 85% PDC threshold, and there were six more conditions [MI, chronic obstructive pulmonary disease (COPD), congestive heart failure (CHF), diabetes, ischemic heart disease, asthma] among the prefrail group at the 80% PDC threshold. Only at the lowest threshold for nonadherence were there conditions with higher prevalence in the prefrail nonadherent than the adherent groups (MI, COPD, CHF).
Post hoc Difference Between Proportions of Nonadherent and Adherent Older People Living with HIV (PLWH) That Have Geriatric and Chronic Conditions
Bold = p value <0.05.
Values are absolute differences between the adherent and nonadherent proportions (Δ = %nonadherent − %adherent). Example interpretations: In the frail stratum and <95% PDC, the proportion of females was 9 percentage points higher in the nonadherent compared to the adherent group and the proportion dually eligible was 8 percentage points lower in the nonadherent compared to the adherent group.
Δ, difference; PDC, proportion of days covered; PLWH, people living with HIV.
Discussion
Accumulating comorbidities have been associated with nonadherence to certain medications, although it is less clear if the same effect is observed among older PLWH and ART. 2,9 Our goal was to understand if geriatric conditions, like other comorbidities, are associated with ART nonadherence in a Medicare population of older PLWH. We hypothesized that adherence to ART would be lower for older PLWH with frailty and other geriatric conditions. We found that frailty status was the only geriatric condition consistently associated with ART adherence at all thresholds for ART nonadherence. To that end, robust and prefrail people were similar, and being frail was associated with ∼30% higher likelihood of ART nonadherence.
Older PLWH make up 50% of the HIV population and nearly 20% of new infections in the United States. 5 Regardless of the debate about whether PLWH experience accelerated or accentuated aging, older PLWH are accumulating geriatric conditions at younger ages than their non-HIV counterparts; 16,35 the most prevalent in our sample were depression, prefrailty, and frailty. Polypharmacy was present in more than half, although fewer of the nonadherent than adherent had polypharmacy. To that end, frailty was associated with higher likelihood of nonadherence. Frailty, in this case, was an assessment of total burden of deficit because we used a deficit accumulation FI. 22,23 The utility of knowing frailty's relationship with nonadherence is in the opportunity to understand what deficits make up the FI; having a FI indicative of frailty does not necessarily mean the same deficits have accumulated. 36 This is particularly true because of the younger chronologic age at which PLWH begin developing geriatric conditions and the unique experiences PLWH have with intersecting effects of HIV, treatment, and aging. 35,37 Post hoc analysis demonstrated that there was greater heterogeneity between prefrail nonadherent and adherent older PLWH than among the frail group. Heterogeneity among prefrail older adults creates challenges for identifying and intervening where frailty is more homogenous in global deficits. Research has shown that one approach may be to use latent class analysis among each frailty subgroup to identify dominant deficits for targeted intervention to maintain or improve ART adherence. 36
Polypharmacy was associated with lower likelihood of nonadherence. In our sample a significantly larger proportion of the adherent group had polypharmacy, which may mean that they are high utilizers of health care, seen often by providers and have many comorbidities that each come with a treatment. 38 This agrees with our overall finding that prefrailty had lower likelihood of nonadherence and also the nonadherent prefrail groups had lower proportions of comorbidities than the adherent groups in post hoc analyses. To detect a condition in claims data, patients must be seen by a physician for that condition. Conditions that are treated and controlled reduce opportunities for additional complications. For example, orthostatic hypotension and falls have been associated in the literature and influenced by blood pressure control medications. 39 Our findings also agree with the literature showing that PLWH engaged in care do better with ART adherence and viral suppression, which may be a phenomenon pertaining to more than HIV-associated outcomes. Clearly geriatric conditions exist among an older HIV population in Medicare, but this is a specific group of older PLWH who have access to health insurance. Having health insurance has been linked to better health outcomes and disease management, including treatment adherence. Our finding that nonadherence is less likely for those with dual eligibility status demonstrated this. Therefore, factors other than having geriatric conditions and related treatments seem to also contribute to the likelihood that older PLWH would be nonadherent.
The relevance of these findings to clinical practices extends beyond medical conditions and treatments to include demographic factors. Female sex, race/ethnic minorities, and having a history of substance use seemed to have highest risk for nonadherence, a finding consistent with the literature. 40,41 Brown et al. demonstrated that >50% of females and more than two thirds of minorities had suboptimal ART adherence. 41 The association of race with nonadherence may reflect HIV stigma and discrimination that persists in health care, 42 and substance use is a known risk factor for inconsistencies in adherence. 3,10 However, having secondary insurance might mitigate risk. Eligibility for Medicaid in addition to Medicare, as we had in 45% of this sample, can create greater access to health care, particularly nursing homes, which are otherwise not covered by Medicare and are increasingly relevant to the older HIV population. 35,43 In addition, Medicaid eligibility is indicative of meeting certain criteria, including low income which qualifies people for the low income subsidy and lower cost of prescriptions. 33
PLWH have differing life history exposures of stress, stigma, and comorbid exposures while they age compared to HIV uninfected. 21 Therefore, there is high value in exploring the potential that geriatric conditions are a subset of comorbidities associated with ART nonadherence. This extends the literature beyond general comorbidities and beyond nonadherence as the presumed cause of poor health outcomes. These findings support that frailty evaluation may need to be part of the routine clinical care of older PLWH and at ages younger than people without HIV. Brothers and Rockwood and Brañas et al. emphasized this point in their work describing the utility of frailty in optimizing geriatric HIV care. 14,44 Finally, deprescribing is an important practice in geriatrics to reduce pill burden and minimize potential for drug–drug interactions and related poor health outcomes. 12,29 However, here we show that polypharmacy in PLWH may indicate appropriate engagement in care, which is different from some literature where polypharmacy is assumed to be excessive treatment often linked to poor health outcomes. 29 More work is needed to understand the critical role of appropriate versus inappropriate polypharmacy. As a result, long-term surveillance of frailty and polypharmacy may be a first step at refining patient-centered care aimed at improving ART adherence.
Limitations
This study has several limitations that include limitations in our ability to make causal conclusions because of the cross-sectional nature of the data; we cannot rule out that poor ART adherence precedes geriatric conditions but have done our best to simulate temporality using an index date 1 year into the data time frame. Geriatric conditions selected were suggested by a geriatrician and agreed upon by all authors as pertinent to the topic. However, other conditions commonly associated with aging and multi-system dysregulation, such as diabetes, have also been shown to be associated with ART nonadherence. 16 In defining ART adherence, we used multiple threshold values of 95% commonly used in the literature, 3,31 but tried to adjust for improvements in regimens with less common thresholds of 85% and 80%. We also do not have data on key social determinants of health (other than dual eligibility for Medicaid), such as housing instability or life events such as death of a partner, which could play a role in timing of ART prescribing and how well they are able to adhere. Moreover, we did not know duration of HIV infection or treatment. We required continuous enrollment in Medicare, where longer continuous enrollment would reduce sample size, but potentially capture more prevalent conditions in 1 year look back period. Using the CCW data helped mitigate the risk of inadequate condition capture as it includes history of all conditions, even that predate the data. Finally, we could only estimate ART adherence as a function of implementation using PDC but that does not mean PLWH actually took medication.
In conclusion, adherence to ART regimens in PLWH was associated with frailty and polypharmacy. Documenting accumulated deficits in health records and claims may represent who is engaged in care and treated for geriatric conditions and HIV. These findings add to the literature calling for incorporation of frailty assessments into the care of older PLWH, even at ages younger than are traditionally associated with geriatric care.
Footnotes
Authors' Contributions
B.O.-M.: Conceptualization, Methodology, Formal analysis, Writing—Original draft preparation; I.W.: Validation, Writing—Reviewing and Editing. S.S.: Writing—Reviewing and Editing. M.M.: Writing—Reviewing and Editing; E.P.M.: Writing—Reviewing and Editing; G.O.: Formal analysis; D.H.K.: Validation, Writing—Reviewing and Editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
B.O.-M. and S.S. were supported by the Harvard Translational Research in Aging Training Program, T32 AG023480. D.H.K. was supported by R01AG071809.