
Abstract
Current guidelines recommend screening people with HIV (PWH) for bone disease using predictive tools developed for the general population, although data on PWH are scarce. In this study, we assessed the performance of FRAX and QFracture scoring systems to predict the occurrence of fragility fractures in a prospective cohort of 17,671 adults with human immunodeficiency virus (HIV) included in the HIV/AIDS research network (CoRIS) in Spain. The survival estimates of fragility fractures during follow-up were calculated and FRAX and QFracture scores were computed at cohort inclusion. For both tools, discriminatory measures and the observed-to-expected (O/E) ratios were assessed. During a follow-up time of 42,411.55 person-years, 113 fragility fractures were recorded. Areas under the curve were 0.66 [95% confidence interval (95% CI) 0.61–0.71] for FRAX and 0.67 (95% CI 0.62–0.73) for QFracture for major osteoporotic fractures, and 0.72 (95% CI 0.57–0.88) and 0.81 (95% CI 0.68–0.95) for hip fracture, respectively. The O/E was 1.67 for FRAX and 5.49 for QFracture for major osteoporotic fractures, and 11.23 for FRAX and 4.87 for QFracture for hip fractures. Moreover, O/E raised as the risk increased for both tools and in almost all age groups. When using the recommended assessment thresholds, <6% and 10% of major osteoporotic and hip fractures would have been identified, respectively. In conclusion, FRAX and QFracture displayed acceptable discrimination, although both tools significantly underestimated the risk of fragility fractures in PWH. The recommended assessment thresholds may not be appropriate for this population as they were unable to identify individuals with fragility fractures during follow-up.
Introduction
With the advances in antiretroviral therapy and the aging of people with HIV (PWH), their health care has focused on improving the long-term quality of life and preventing chronic complications associated with their condition. PWH experience a high burden of frailty that increases with advancing age and is associated with multi-morbidity and mortality rates. 1,2 In particular, frailty has been associated with the incidence of fractures in PWH, which occur more frequently than in the general population and lead to hospitalizations, detrimental quality of life, excess costs, and death. 2,3 In PWH, fragility fractures occur at an earlier age, increasing the individual and social impact of these outcomes. 3 –5 Risk factors classically associated with bone mineral density loss and fragility fractures, as well as other factors associated with chronic inflammation despite that virological suppression and coinfections may contribute to this risk. 6,7
Importantly, the use of certain antiretroviral agents such as tenofovir disoproxil fumarate (TDF) and some boosted protease inhibitors has been linked to bone loss and the risk of fractures. 8,9
In Europe, current guidelines recommend using the geographically calibrated FRAX tool to estimate the 10-year probability of major osteoporotic and hip fractures in PWH and select candidates for further diagnostic tests. 10,11 However, studies performed outside Europe suggested that FRAX underestimates the presence of bone disease even when human immunodeficiency virus (HIV) infection is considered a cause of secondary osteoporosis. 12,13 In addition, this tool only considers a minority of causes of secondary osteoporosis, included as a single factor for calculating the risk of fracture. 14,15 The QFracture score was designed to include additional fracture risk factors to those included in the FRAX tool and applies to younger people (older than 30 years). 16,17 However, it does not incorporate variables associated with HIV infection and no studies have assessed its usefulness in PWH.
Given the high risk of fractures in PWH and the controversies regarding their clinical assessment, we aimed to assess the accuracy of the FRAX and QFracture scoring systems in predicting the occurrence of fragility fractures in a Spanish national cohort of PWH.
Methods
Study population
We analyzed data from individuals prospectively included in the Spanish HIV/AIDS research network (CoRIS) between January 2, 2004, and November 30, 2019. The CoRIS is an open, prospective, multi-center cohort of adult subjects with confirmed HIV infection, naive to ART at study entry, recruited in 47 centers from 14 of the 17 autonomous regions in Spain from 2004 onward. Data are organized and standardized following the HIV Cohorts Data Exchange Protocol (HICDEP) for data collection (details at
Given that previous evidence stated that PWH have fragility fractures earlier than the general population, 5 we included individuals older than the age of 30, which is the lower limit for QFracture risk estimation. As the FRAX algorithm only allows a minimum age of 40 years, individuals aged between 30 and 40 years were assigned an age of 40 for the purposes of this analysis. 19 We excluded participants aged younger than 30 years and those with incomplete data for score calculation. All but four CoRIS centers collect information on nonacquired immunodeficiency syndrome (AIDS) events and bone fractures, whose participants were excluded from this analysis. Each individual was censored when the first of the following occurred after cohort inclusion: first event of fragility fracture, lost to follow-up, or death.
Clinical risk factors and incident fragility fracture
All the variables to compute each of the scores were collected from the CoRIS database at the time of cohort inclusion. For variables that were defined differently by FRAX and QFracture (smoking status, alcohol use), we computed two separate variables. Given that only medications prescribed chronically are collected in the CoRIS database, we considered the use of steroids as each record in the database. The use of immunosuppressors (excluding antirejection medication) was considered a proxy for rheumatoid arthritis or systemic lupus erythematosus diagnosis. No information was available for parental fracture history, falls, nursing home care, history of type 1 diabetes, or estrogen use as hormone replacement therapy in women. Therefore, these variables were entered as “no” for all individuals in the analysis.
Fragility fractures were defined as those that are nontraumatic or that occurred after a casual fall as per the CoRIS registry based on medical records. Considering the definition of fractures used by QFracture and FRAX tools, we analyzed fragility fractures of the hip and other major osteoporotic fractures (clinical spine, forearm, proximal humerus). For the purpose of this study, we compared the tools among individuals with the first event of fragility fracture during follow-up.
Risk assessment tool computation
Since FRAX equations are not published by the developers, we computed the FRAX 10-year probability from the charts calibrated for Spain supplied by the official FRAX site, stratified by gender, age, body mass index (BMI), and the number of clinical risk factors, without the input of bone mineral density (
Statistics
Descriptive statistics for baseline characteristics were reported as a frequency distribution for qualitative variables, whereas normally distributed quantitative variables were described as mean ± standard deviation. The continuous non-normally distributed variables were reported as median and interquartile ranges. Chi-square test or Fisher's exact test was performed to compare categorical variables by the presence of fragility fractures. Continuous variables were compared using T-test or Wilcoxon–Mann–Whitney nonparametric test, as appropriate. The association between fragility fractures and death was estimated using a Cox proportional hazards model adjusted by age and gender.
To evaluate the ability of each tool to discriminate for the occurrence of fragility fractures during follow-up, we used the area under the receiver operating curve (AUC) and calculated the sensitivity, specificity, and positive and negative predictive values for the top 10th predicted risk in the cohort as cutoff, as previously performed in validation studies. 21,22 In addition, we determined two categories of risk for FRAX using the thresholds recommended by local guidelines for assessing fracture risk in PWH, guide bone mineral density measurement, and prompt timely referral and treatment. These assessment thresholds corresponded to a 3% and 10% 10-year estimated risk of hip and major osteoporotic fractures using the FRAX tool, respectively. 11
FRAX and QFracture provide different outputs (probability of fracture accounting for mortality rate risk and cumulative risk of fracture, respectively) and therefore, we obtained observed fracture estimates accordingly. 15,17 For FRAX, the observed 10-year major osteoporotic fracture (MOF) probability was derived from the cumulative incidence function, with death considered a competing hazard. 23 For QFracture, fracture survival estimates at 10 years were calculated using the Kaplan–Meier estimates with 95% confidence intervals (95% CI).
Then, we calculated the mean 10-year predicted fracture probabilities for FRAX and QFracture for major osteoporotic and hip fractures. Individuals were grouped into quintiles of predicted probabilities and by age. To assess the calibration of the tools, we calculated the ratio of the observed fractures to mean predicted probabilities (O/E) overall, at each quintile of predicted risk, and by age. All statistical analyses were performed using the SPSS 16.0 statistical package (SPSS, Inc., IL). All tests were two-tailed, and a p value <0.05 was considered significant.
Results
As of November 30, 2020, the CoRIS consisted of 17,671 PWH. We excluded 710 participants from HIV care units that do not report non-AIDS-related events, 5076 participants younger than 30 years at cohort inclusion, and 5820 with missing data for at least one variable in the tools (none had data on BMI, 74.33% on alcohol use, and 49.47% on smoking status). Table 1 displays the characteristics of individuals included in the current analysis versus those not included due to missing data.
Baseline Characteristics of the Individuals Included Versus Those Not Included Due to Missing Data
AIDS, acquired immunodeficiency syndrome; BMI, body mass index; HIV, human immunodeficiency virus; IQR, interquartile range; RA, rheumatoid arthritis; SD, standard deviation; SLE, systemic lupus erythematosus.
The final study population consisted of 6080 individuals (mean age 41 ± 9 years; 14.25% women, Table 2). During a follow-up time of 42,411.55 person-years, 113 first episodes of fragility fractures occurred (86 major osteoporotic fractures, 11 hip fractures, 16 at other anatomical sites), yielding an incidence rate of 2.66 (95% CI 2.22–3.20) per 1000 person-years. The incidence rate of fragility fractures increased with age in both genders (Table 3), for major osteoporotic and hip fractures (Table 4). A total of 188 (3.1%) individuals died during follow-up.
Baseline Characteristic of the Population According to the Presence of Fragility Fractures
AIDS, acquired immunodeficiency syndrome; BMI, body mass index; HIV, human immunodeficiency virus; IQR, interquartile range; RA, rheumatoid arthritis; TDF, tenofovir disoproxil fumarate; SD, standard deviation; SLE, systemic lupus erythematosus.
Age-Stratified Incidence Rate of Fragility Fractures by Gender
95% CI, 95% confidence interval.
Age-Stratified Incidence Rate of Fragility Fractures by Site of Fracture
95% CI, 95% confidence interval.
Individuals with incident fragility fractures were older, more frequently women, with a diagnosis of AIDS, and lower nadir CD4 counts compared with PWH without fragility fractures during follow-up. Among the clinical risk factors included in the estimation tools, smoking status, alcohol use, cardiovascular disease, cancer history, use of immunosuppressors, endocrine disorders, and liver disease at baseline were more frequent in individuals with fragility fractures (Table 2). In addition, these individuals had a higher risk of death (hazard ratio = 3.61, 95% CI 2.10–6.22) compared with individuals without fractures after adjusting for age and gender.
In evaluating the discriminative performance of the tools, FRAX and QFracture had similar AUC for major osteoporotic fracture prediction using the top 10th risk as cutoff (0.66, 95% CI 0.61–0.71, and 0.67, 95% CI 0.62–0.73, respectively). The discriminatory measures for hip fracture prediction were similar between the FRAX and QFracture tools and higher than for major osteoporotic fractures. Using these cutoffs, FRAX identified 41.9% and 54.5% of PWH who went to have an incident major osteoporotic or hip fracture, and QFracture identified 44.2% and 72.7%, respectively. Both tools had specificities of more than 90% and negative predictive values of more than 99% (Table 5).
Discriminatory Measures of FRAX and QFracture Using Recommended Thresholds and Top 10% Risk Cutoffs for Each Tool
Values are percentages (95% CI), except AUC values.
Using recommended assessment thresholds for PWH (FRAX scores ≥10 for major osteoporotic fracture and ≥3 for hip fracture).
Using top 10% FRAX-predicted risk as threshold (3.7 for major osteoporotic fracture and 0.6 for hip fracture).
Using top 10% QFracture-predicted risk as threshold (1.6 for major osteoporotic fracture and 0.3 for hip fracture).
95% CI, 95% confidence interval; AUC, area under the curve; NPV, negative predictive value; PPV, positive predictive value; PWH, people with HIV.
Overall, 0.15% and 0.53% of the population had FRAX scores above the recommended assessment thresholds for major osteoporotic and hip fractures, respectively. When using these thresholds, the AUC and sensitivity of FRAX were lower for the discrimination of major osteoporotic and hip fractures than when the top 10th risk cutoffs were applied (Table 5).
The 10-year survival estimate of any fragility fracture was 8.40% (95% CI 5.44–12.87, Fig. 1) and 3.94% (95% CI 3.30–4.65) when considering the competing risk of death. Table 6 compares the observed fracture estimates at 10 years with the mean predicted risk overall and within each quintile of risk to assess the calibration of the models. For both tools, the observed rates of major osteoporotic and hip fractures significantly exceeded the predicted rates overall and as the risk increased. Particularly, the FRAX tool markedly underestimated the risk of hip fractures in every quartile of risk with O/E ratios as high as 13.7. In the age-stratified calibration analysis, most of the O/E ratios were >1, indicating an underestimation of the risk of major osteoporotic and hip fractures by both tools in almost all age groups (Fig. 2).
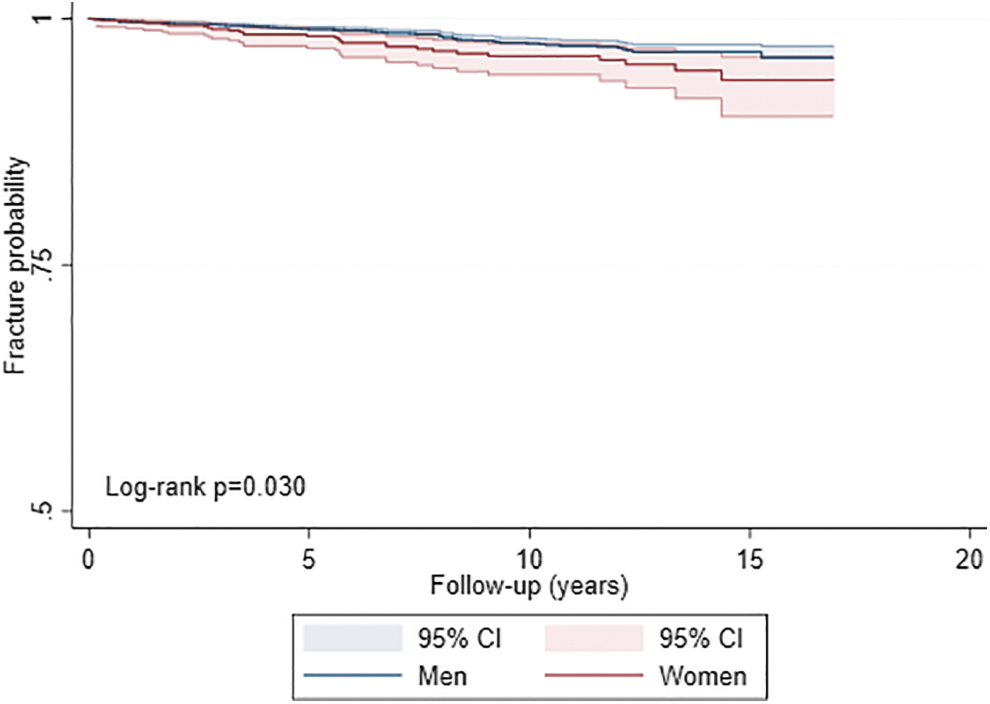
Kaplan–Meier curves for fragility fracture-free probabilities for people with HIV by gender. 95% CI, 95% confidence interval; HIV, human immunodeficiency virus.
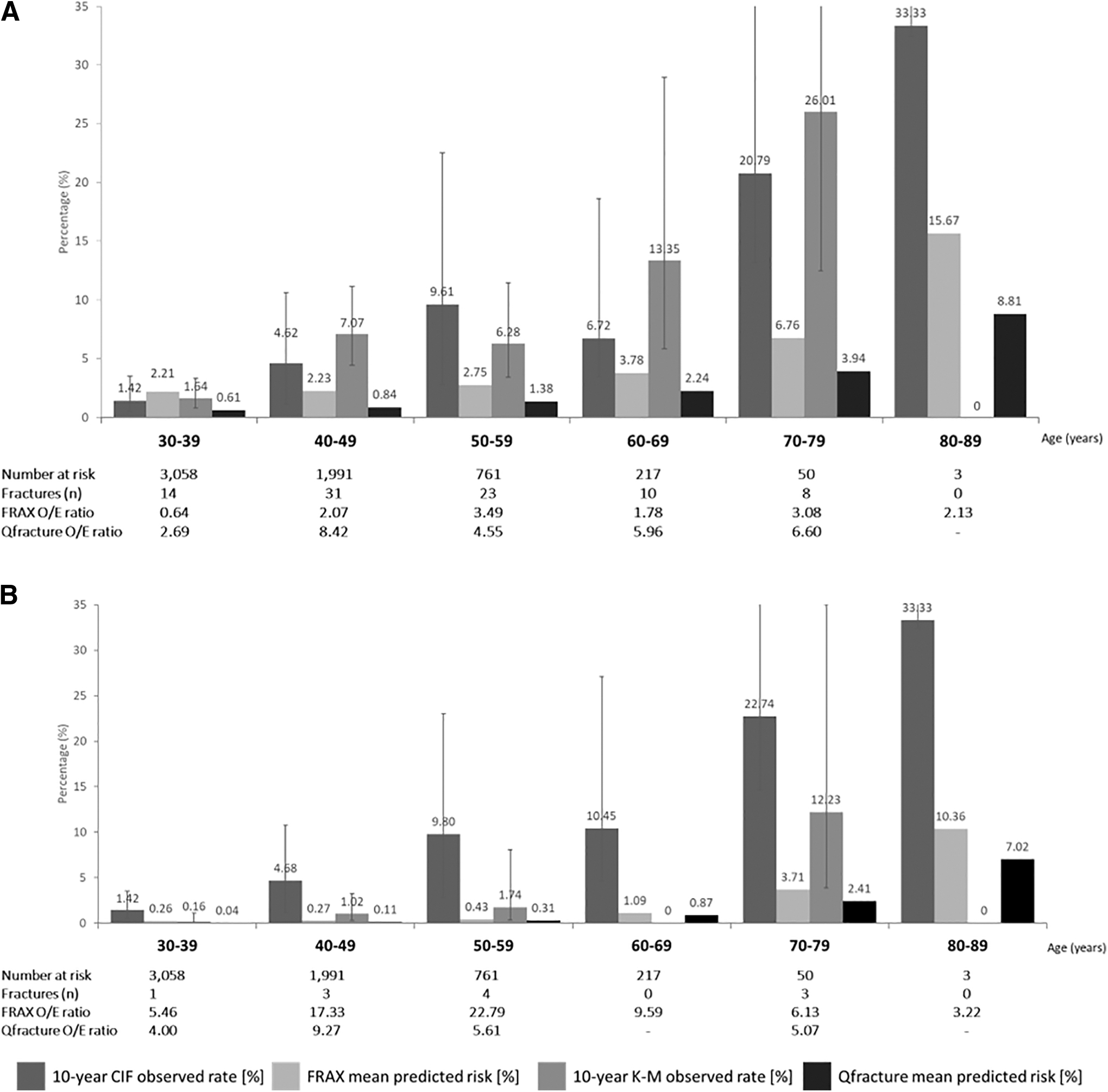
Calibration of the observed fragility fracture rates (expressed as percentages with 95% CI) versus mean FRAX and QFracture estimated risks, by age decade.
Calibration of 10-Year Observed Versus Predicted Fragility Fracture Rates, Overall and by Quintile of Predicted Risk
Ten-year observed fracture rates were derived from the CIF with death considered a competing hazard for FRAX tool and from Kaplan–Meier estimates for QFracture.
95% CI, 95% confidence interval; CIF, cumulative incidence function; O/E, observed-to-expected.
Calibration was next evaluated using the assessment thresholds recommended for FRAX tool. Due to the small number of individuals above the thresholds (≤0.5% of the population), CI was wider in this analysis. Nevertheless, the 10-year observed rates of major osteoporotic and hip fractures were significantly higher than the predicted rates for individuals above the assessment threshold (O/E: 4.85 and 9.62, respectively), implying underestimation of the risk even among individuals in the high-risk category. Moreover, only 5.8% and 9.1% of the major osteoporotic and hip fractures were correctly identified by the recommended assessment thresholds, respectively (Table 7).
Calibration of 10-Year Observed Versus Predicted Fragility Fracture Rates Using Recommended Assessment Thresholds for FRAX in People with Human Immunodeficiency Virus
Ten-year observed fracture rates were derived from the CIF with death considered a competing hazard.
95% CI, 95% confidence interval; CIF, cumulative incidence function; O/E, observed-to-expected.
Discussion
In this study, we present the performance of FRAX and QFracture in a large multi-center cohort of PWH. Overall, the ability of the tools to discriminate between individuals with incident fragility fractures showed acceptable values. However, both tools underestimated the 10-year rate of major osteoporotic and hip fragility fractures as the risk increased, and in almost all age groups. Further, using the assessment thresholds recommended by current guidelines, <10% of incident fragility fractures were identified.
Previous studies validated the FRAX tool in the general population of Spain and described discriminatory values expressed by the AUC that were comparable with those of the derivation cohorts. 24,25 In our study, we found that the discriminatory performance of FRAX and QFracture in PWH was similar to that reported in the general population, 15,25,26 with higher AUC values for hip fractures than for major osteoporotic fractures. Of note, although the sensitivity for the identification of fragility fractures was overall low, the high negative predictive values could be used to identify individuals with a low risk of fractures.
However, the discriminatory performance of a model does not reflect its clinical value, and calibration assessed by the agreement between the observed and the estimated number of events is needed to support decision-making. 27 In this regard, prior studies in the Spanish general population observed that FRAX underestimated the risk of fractures, particularly among the low-risk categories with O/E ratios ranging from 1.5 to 2.8. 24,25 No data are available for the performance of QFracture in Spain. In our cohort, we found consistent poor calibration for the prediction of major osteoporotic and hip fractures, with observed fracture rates up to sevenfold higher than estimated.
Although this is the first study to our knowledge evaluating the use of QFracture in PWH, other studies found that FRAX underestimated fractures in PWH, even when including HIV infection as a secondary cause of osteoporosis. 12,13 The lack of accuracy of the models may be related to the presence of additional and multiple clinical risk factors that contribute to bone disease in PWH, which are not contemplated in the FRAX or QFracture algorithms. For instance, Yang et al observed that FRAX underestimated fracture risk in women with HIV and HCV coinfection. 12 Further conditions such as vitamin D deficiency, 6 the use of certain antiretrovirals (e.g., TDF), 9 chronic kidney disease, 28,29 and cancer may be major contributors to bone fragility among PWH. 30
Bone disease constitutes one of the main clinical challenges for the aging population with HIV. The identification of individuals at high risk of fragility fractures and the application of early interventions could have a significant impact on their prevention. 31 Of clinical interest, when using the recommended assessment thresholds, <6% and 10% of major osteoporotic and hip fractures would have been identified, respectively. Overall, our results suggest that the clinical use of FRAX or QFracture under these circumstances may result in PWH at risk being denied further assessment (e.g., dual-energy X-ray absorptiometry) or treatment. Indeed, the lack of an accurate risk stratification tool may contribute to physicians' low awareness of the importance of this condition, reflected in low adherence to dual-energy X-ray absorptiometry screening. 32
Therefore, a specific fracture prediction tool that takes into account the particularities of this population is needed. In the meantime, we suggest clinicians consider that the risk of fragility fractures may be twofold greater than calculated.
Our analysis has limitations that need to be acknowledged. First, the mean age of our cohort was younger than the population in the derivation studies of FRAX and QFracture models, with a lower proportion of women. However, it is representative of the population living with HIV in high-income countries. Given that older people and women have a higher risk of fractures, it is unlikely that this fact would have changed the direction of the results. Indeed, the fracture rate among PWH aged 40–50 years in our cohort is similar to that observed in the general population more than a decade older. 21 This finding reinforces previous observations of premature onset of age-related diseases, including fragility fractures, in PWH. 3,5
Second, we have no data on some variables that might have increased the predicted risk such as a parenteral history of fractures. Although the percentage of individuals with a high risk of major osteoporotic fracture by FRAX was similar to that reported in other studies in PWH (0.3%). 33 Last, given that the FRAX equation has not been published, we used charts calibrated for Spain supplied by the official FRAX site. Since we found similar AUCs to previous validation studies, it is unlikely that this would have significantly affected the results.
In conclusion, given that controversy persists regarding which strategy to use for bone disease risk stratification among PWH, our study highlights the poor calibration of FRAX in this population. Although QFracture incorporates other risk factors and can be used in younger populations compared with FRAX, we show that it also underestimates fracture risk. Importantly, currently recommended assessment thresholds are not useful in identifying PWH at high risk of fragility fractures, precluding them from accessing interventions to reduce this risk. Overall, the results of our study emphasize the need for a predictive score developed for PWH.
Footnotes
Acknowledgments
This study would not have been possible without the collaboration of all the patients, medical and nursing staff, and data managers who have taken part in the project.
CoRIS Members' Information:
Executive committee:
Santiago Moreno, Inma Jarrín, David Dalmau, M. Luisa Navarro, M. Isabel González, Federico Garcia, Eva Poveda, Jose Antonio Iribarren, Félix Gutiérrez, Rafael Rubio, Francesc Vidal, Juan Berenguer, Juan González, M. Ángeles Muñoz-Fernández.
Fieldwork data management and analysis:
Inmaculada Jarrín, Cristina Moreno, Marta Rava, Rebeca Izquierdo.
BioBanK HIV Hospital General Universitario Gregorio Marañón:
M Ángeles Muñoz-Fernández, Elba Mauleón.
Hospital General Universitario de Alicante (Alicante):
Joaquín Portilla, Irene Portilla, Esperanza Merino, Gema García, Iván Agea, José Sánchez-Payá, Juan Carlos Rodríguez, Livia Giner, Sergio Reus, Vicente Boix, Diego Torrus, Verónica Pérez, Julia Portilla.
Hospital Universitario de Canarias (San Cristóbal de la Laguna):
Juan Luís Gómez, Jehovana Hernández, Ana López Lirola, Dácil García, Felicitas Díaz-Flores, M. Mar Alonso, Ricardo Pelazas, M. Remedios Alemán.
Hospital Universitario Central de Asturias (Oviedo):
Víctor Asensi, M. Eugenia Rivas, Tomás Suarez-Zarracina, Eulalia Valle-Garay, Javier Díaz.
Hospital Universitario 12 de Octubre (Madrid):
Federico Pulido, Rafael Rubio, Otilia Bisbal, M. Asunción Hernando, David Rial, María de Lagarde, Octavio Arce, Adriana Pinto, Laura Bermejo, Mireia Santacreu, Roser Navarro, Candela Gonzalez.
Servicio de Enfermedades Infecciosas. Hospital Universitario Donostia. Instituto de Investigación BioDonostia (Donostia-San Sebastián):
Jose Antonio Iribarren, M. José Aramburu, Xabier Camino, Miguel Ángel von Wichmann, Miguel Ángel Goenaga, M. Jesús Bustinduy, Harkaitz Azkune, Maialen Ibarguren, Xabier Kortajarena, Ignacio Álvarez-Rodriguez, Leire Gil, Lourdes Martínez.
Hospital General Universitario De Elche (Elche):
Félix Gutiérrez, Mar Masiá, Catalina Robledano, Sergio Padilla, Javier Garcia Abellán, Paula Mascarell, Araceli Adsuar, Rafael Pascual, Mar Carvajal, Marta Fernández, José Alberto García, Ángela Botella, Alba de la Rica, Carolina Ding, Lidia García-Sánchez, Nuria Ena, Xavier Barber, Vanessa Agullo, Reyes Pascual, Guillermo Telenti, Lucia Guillén, Leandro López, Jennifer Vallejo, Nieves Gonzalo-Jimenez, Montserrat Ruiz, Antonio Galiana.
Hospital Universitari Germans Trias i Pujol (Can Ruti) (Badalona):
Roberto Muga, Arantza Sanvisens, Daniel Fuster.
Hospital General Universitario Gregorio Marañón (Madrid):
Juan Berenguer, Isabel Gutierrez, Juan Carlos López, Margarita Ramírez, Belén Padilla, Paloma Gijón, Teresa Aldamiz-Echevarría, Francisco Tejerina, Cristina Diez, Leire Pérez, Chiara Fanciulli, Saray Corral.
Hospital Universitari de Tarragona Joan XXIII (Tarragona):
Francesc Vidal, Anna Martí, Joaquín Peraire, Consuelo Viladés, Montserrat Vargas, Montserrat Olona, Anna Rull, Verónica Alba, Elena Yeregui, Jenifer Masip, Graciano García-Pardo, Frederic Gómez Bertomeu, Sonia Espineira.
Hospital Universitario y Politécnico de La Fe (Valencia):
Marta Montero, Sandra Cuéllar, Marino Blanes, María Tasias, Eva Calabuig, Miguel Salavert, Juan Fernández, Inmaculada Segarra.
Hospital Universitario La Paz/IdiPAZ (Madrid):
Juan González-García, Ana Delgado-Hierro, José Ramón Arribas, Victor Arribas, Jose Ignacio Bernardino, Carmen Busca, Joanna Cano, Julen Cardiñanos, Juan Miguel Castro, Luis Escosa, Iker Falces, Pedro Herranz, Victor Hontañón, Milagros García, Alicia González-Baeza, Ma Luz Martín-Carbonero, Mario Mayoral, Ma Jose Mellado, Rafael Micán, Rosa de Miguel, Rocío Montejano, Ma Luisa Montes, Victoria Moreno, Luis Ramos, Berta Rodés, Talía Sainz, Elena Sendagorta, Eulalia Valencia.
Hospital San Pedro Centro de Investigación Biomédica de La Rioja (CIBIR) (Logroño):
Jose Ramón Blanco, Laura Pérez-Martínez, José Antonio Oteo, Valvanera Ibarra, Luis Metola, Mercedes Sanz.
Hospital Universitario Miguel Servet (Zaragoza):
Piedad Arazo, Gloria Sampériz.
Hospital Universitari Mutua Terrassa (Terrassa):
David Dalmau, Marina Martinez, Angels Jaén, Mireia Cairó, Javier Martinez-Lacasa, Roser Font, Laura Gisbert.
Complejo Hospitalario de Navarra (Pamplona):
María Rivero, Beatriz Piérola, Maider Goikoetxea, María Gracia, Carlos Ibero, Estela Moreno, Jesús Repáraz.
Parc Taulí Hospital Universitari (Sabadell):
Gemma Navarro, Manel Cervantes Garcia, Sonia Calzado Isbert, Marta Navarro Vilasaro, Belen Lopez Garcia.
Hospital Universitario de La Princesa (Madrid):
Ignacio de los Santos, Alejandro de los Santos, Jesús Sanz, Lucio García-Fraile, Enrique Martín, Ildefonso Sánchez-Cerrillo, Marta Calvet, Ana Barrios, Azucena Bautista, Carmen Sáez, Marianela Ciudad, Ángela Gutiérrez.
Hospital Universitario Ramón y Cajal (Madrid):
Santiago Moreno, Santos del Campo, José Luis Casado, Fernando Dronda, Ana Moreno, M. Jesús Pérez, Sergio Serrano, Ma Jesús Vivancos, Javier Martínez-Sanz, Alejandro Vallejo, Matilde Sanchez, Jose Antonio Pérez-Molina, José Manuel Hermida.
Hospital General Universitario Reina Sofía (Murcia):
Enrique Bernal, Antonia Alcaraz, Joaquín Bravo, Ángeles Muñoz, Cristina Tomás, Mónica Martínez, M. Carmen Villalba.
Hospital Nuevo San Cecilio (Granada):
Federico García, Clara Martínez, José Hernández, Leopoldo Muñoz Medina, Marta Álvarez, Natalia Chueca, David Vinuesa, Adolfo de Salazar, Ana Fuentes, Emilio Guirao, Laura Viñuela, Andrés Ruiz-Sancho, Francisco Anguita.
Centro Sanitario Sandoval (Madrid):
Jorge Del Romero, Montserrat Raposo, Carmen Rodríguez, Teresa Puerta, Juan Carlos Carrió, Mar Vera, Juan Ballesteros, Oskar Ayerdi, Begoña Baza, Eva Orviz.
Hospital Clínico Universitario de Santiago (Santiago de Compostela):
Antonio Antela, Elena Losada.
Hospital Universitario Son Espases (Palma de Mallorca):
Melchor Riera, María Peñaranda, M. Angels Ribas, Antoni A. Campins, Mercedes Garcia-Gazalla, Francisco J. Fanjul, Javier Murillas, Francisco Homar, Helem H. Vilchez, Luisa Martin, Antoni Payeras.
Hospital Universitario Virgen de la Victoria (Málaga):
Jesús Santos, María López, Crisitina Gómez, Isabel Viciana, Rosario Palacios.
Hospital Universitario Virgen del Rocío (Sevilla):
Luis Fernando López-Cortés, Nuria Espinosa, Cristina Roca, Silvia Llaves.
Hospital Universitario de Bellvitge (Hospitalet de Llobregat):
Juan Manuel Tiraboschi, Arkaitz Imaz, Ana Karina Silva, María Saumoy, Sofía Catalina Scévola.
Hospital Universitario Valle de Hebrón (Barcelona):
Adrián Curran, Vicenç Falcó, Jordi Navarro, Joaquin Burgos, Paula Suanzes, Jorge García, Vicente Descalzo, Patricia Álvarez, Bibiana Planas, Marta Sanchiz, Lucía Rodríguez.
Hospital Costa del Sol (Marbella):
Julián Olalla, M. José Sánchez, Javier Pérez, Alfonso del Arco, Javier de la Torre, José Luis Prada.
Hospital General Universitario Santa Lucía (Cartagena):
Onofre Juan Martínez, Lorena Martinez, Francisco Jesús Vera, Josefina García, Begoña Alcaraz, Antonio Jesús Sánchez Guirao.
Complejo Hospitalario Universitario a Coruña (Chuac) (A Coruña):
Alvaro Mena, Angeles Castro, Berta Pernas, Pilar Vázquez, Soledad López.
Hospital Universitario Basurto (Bilbao):
Sofía Ibarra, Guillermo García, Josu Mirena, Oscar Luis Ferrero, Josefina López, M. Mar Cámara, Mireia de la Peña, Miriam Lopez, Iñigo Lopez, Itxaso Lombide, Victor Polo, Joana de Miguel.
Hospital Universitario Virgen de la Arrixaca (El Palmar):
Carlos Galera, Marian Fernández, Helena Albendin, Antonia Castillo, Asunción Iborra, Antonio Moreno, M. Angustias Merlos, Asunción Vidal.
Hospital de la Marina Baixa (La Vila Joiosa):
Concha Amador, Francisco Pasquau, Concepción Gil, Jose Tomás Algado.
Hospital Universitario Infanta Sofía (San Sebastián de los Reyes):
Inés Suarez-García, Eduardo Malmierca, Patricia González-Ruano, M. Pilar Ruiz, José Francisco Pascual, Luz Balsalobre, Ángela Somodevilla.
Hospital Universitario de Jaén (Jaén):
M. Villa López, Mohamed Omar, Carmen Herrero, M. Amparo Gómez.
Hospital Universitario San Agustín (Avilés):
Miguel Alberto de Zarraga, Desiré Pérez.
Hospital Clínico San Carlos (Madrid):
Vicente Estrada, Nieves Sanz, Noemí Cabello, Jorge Vergas, M. Jose Núñez, Iñigo Sagastagoitia, Reynaldo Homen, Ana Muñoz.
Hospital Universitario Fundación Jiménez Díaz (Madrid):
Miguel Górgolas, Alfonso Cabello, Beatriz Álvarez, Laura Prieto, Irene Carrillo, Aws Al-Hayani.
Hospital Universitario Príncipe de Asturias (Alcalá de Henares):
José Sanz, Alberto Arranz, Cristina Hernández, María Novella.
Hospital Clínico Universitario de Valencia (Valencia):
M. José Galindo, Ana Ferrer.
Hospital Reina Sofía (Córdoba):
Antonio Rivero Román, Inma Ruíz, Antonio Rivero Juárez, Pedro López, Isabel Machuca, Mario Frias, Ángela Camacho, Ignacio Pérez, Diana Corona, Ignacio Pérez, Diana Corona.
Hospital Universitario Severo Ochoa (Leganés):
Miguel Cervero, Rafael Torres.
Nuestra Señora de Valme (Sevilla):
Juan Antonio Pineda, Pilar Rincón, Juan Macías, Luis Miguel Real, Anais Corma, Marta Fernández, Alejandro Gonzalez-Serna.
Hospital Álvaro Cunqueiro (Vigo):
Eva Poveda, Alexandre Pérez, Luis Morano, Celia Miralles, Antonio Ocampo, Guillermo Pousada, Lucía Patiño.
Hospital Clínico Universitario de Valladolid (Valladolid):
Carlos Dueñas, Sara Gutiérrez, Elena Tapia, Cristina Novoa, Xjoylin Egües, Pablo Tellería.
Authors' Contributions
P.V.: Conceptualization (lead); methodology (equal); writing—original draft (equal); formal analysis (lead); and writing—review and editing (equal). J.L.C.: Conceptualization (equal); methodology (equal); writing—original draft (supporting); and writing—review and editing (equal). A.M. and M.J.V.: Conceptualization (supporting); writing—original draft (supporting); and writing—review and editing (supporting). A.M.G.: Software (equal); methodology (equal); formal analysis (equal); and writing—review and editing (supporting). R.P.G., F.G., D.C.M., P.G., and S.C.: Writing—original draft (supporting) and writing—review and editing (supporting). All the CoRIS board members: review and editing (supporting).
Data Availability
The data that support the findings of this study are available upon request.
Author Disclosure Statement
P.V. reports lecture fees from Gilead, MSD, and ViiV-Healthcare outside the submitted work. M.J.V. reports grants and lecture fees from Gilead and ViiV-Healthcare outside the submitted work. The other authors declare no competing interests.
Funding Information
The RIS cohort (CoRIS) is supported by the Instituto de Salud Carlos III through the Red Temática de Investigación Cooperativa en Sida (RD06/006, RD12/0017/0018, and RD16/0002/0006) as part of the Plan Nacional R+D+I and cofinanced by ISCIII-Subdirección General de Evaluación y el Fondo Europeo de Desarrollo Regional (FEDER).