
Abstract
Unsuppressed HIV viremia damages immunity and increases the risk for secondary HIV transmission. Successful engagement of persons with HIV (PWH) into care resulting in viral suppression is vital. PWH already engaged in care, who, after achieving viral suppression, experience viral breakthrough episodes (VBEs) with a sequence of suppressed/unsuppressed/suppressed viral loads remain problematic. We examined the frequency and outcomes of PWH experiencing VBE. HIV care is provided at no cost to all patients under Alberta's universal health program. All PWH followed at Southern Alberta Clinic, Canada, with two or more viral load tests between January 1, 2010, and January 1, 2020, were evaluated. Sociodemographic, clinical, and lifestyle variables were determined along with health outcomes (CD4 levels, HIV-related hospitalizations, and HIV/AIDS-related mortality). Descriptive and multi-variable analyses were performed comparing PWH with and without VBEs. Of 2096 PWH, 386 (18%) experienced one or more VBEs. A higher risk of VBEs was seen in adjusted analyses in those diagnosed age ≤40 years. Increased risk of VBE was seen with injection drug use (46%) and in heterosexuals (56%) compared with MSM. Experience of intimate partner violence, unstable housing, homelessness, and past incarceration also increased risks by 36%, 44% 79%, and 51%, respectively. PWH with VBEs experienced lower CD4 counts (median −417/mm3 vs. 576/mm3), higher rates of HIV-related hospitalizations (16% vs. 5%), and a 67% increased risk of death (95% confidence interval 1.17–2.39) over the study period. Nearly 20% of all PWH, after achieving viral suppression, experienced VBEs. Distinct clinical, lifestyle, and life experiences predict PWH at greatest risk for more than one VBEs. Serious negative health outcomes of VBEs were identified, suggesting that novel customized care programming is required for PWH at greatest risk.
Introduction
Due to the immense benefits to both personal and public health, a person's care following a new HIV diagnosis is mainly centered on the immediate control of HIV replication through antiretroviral treatment (ART). 1 –6 The goal of ART is viral suppression. Regular viral load measurements are a key component of monitoring the success of treatment. 7 –9 Unsuppressed viral loads from erratic engagement to care and variable ART use can result, through persistent viral replication, in ongoing damage to immunity, chronic inflammation, and selection of ART-resistant mutations in addition to an increased risk of HIV transmission to others. 9 –13 Successfully engaging newly diagnosed patients into care and achieving viral suppression comprise two steps in the World Health Organization cascade of care metric. 14
Most studies on understanding viral suppression rates are cross sectional. 15 –17 Comparatively less attention, however, has been directed toward characterizing persons with HIV (PWH) longitudinally who are engaged in HIV care, but after successfully achieving viral control on ART, experience one or more episodes of viral breakthrough (i.e., >1000 copies/mL), followed by viral suppression once again [defined as a “viral breakthrough episode” (VBE)]. Characterizing these patients in care but with fluctuating suppressed/unsuppressed/suppressed periods (“sawtooth patterning” illustrated in Fig. 1) is important as VBE events may lead to HIV transmission, development of HIV resistance, and poor outcomes associated with HIV viral replication. Defining those at risk for VBE, developing strategies for preventing VBEs as well as improved understanding of the health impact of a VBE are important in the proper management of HIV care.
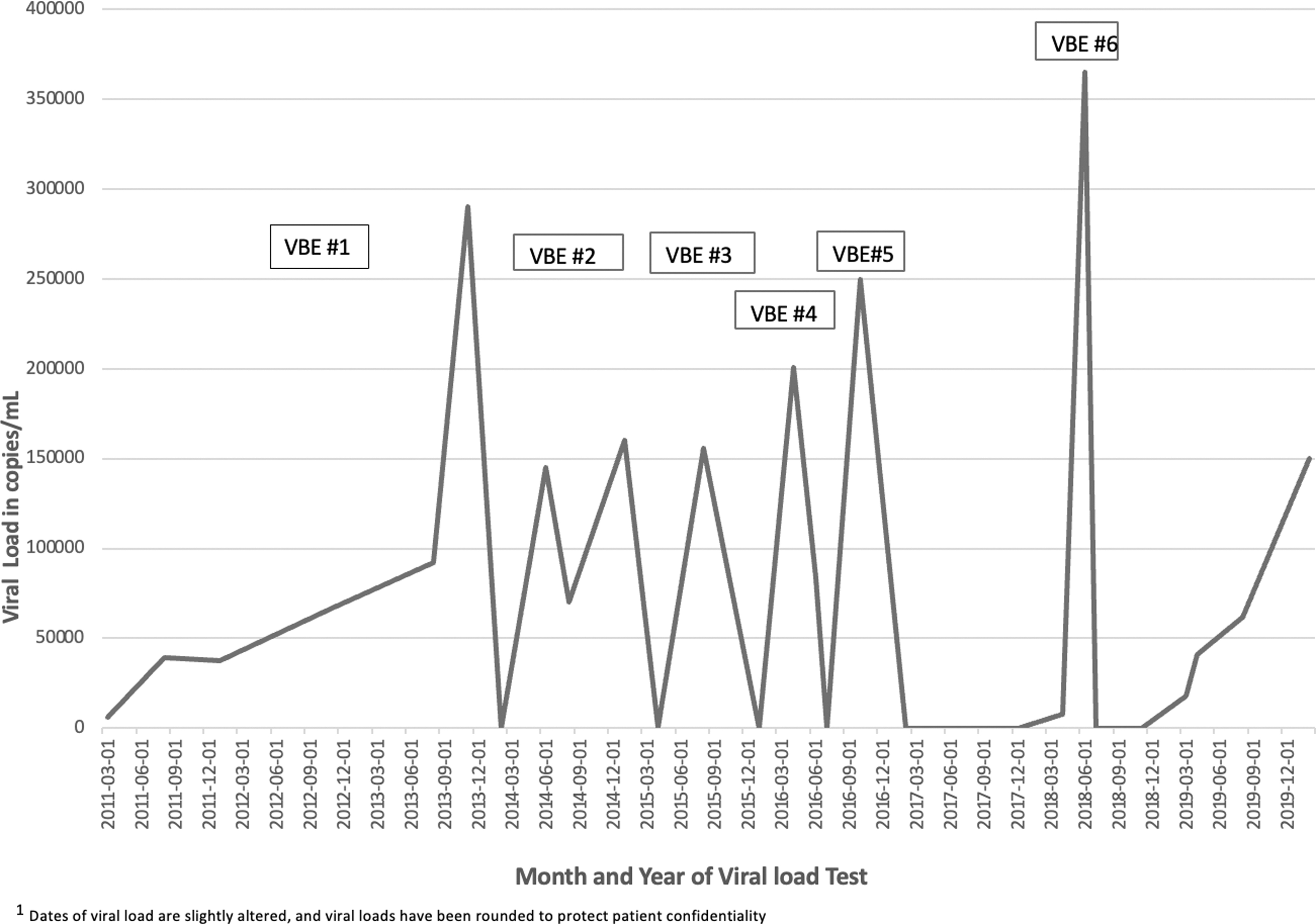
Illustration of “sawtooth patterning” (i.e., suppressed/unsuppressed/suppressed viral loads) for a patient 1 in care over 10 years. A VBE is defined as the date from an initial suppressed viral load to the next suppression. VBE, viral breakthrough episode.
We aimed to explore the frequency of VBE events among all PWH followed in HIV care within a large geographically defined cohort over a 10-year period. We compare sociodemographic, clinical, and “lifestyle” characteristics between PWH experiencing VBE with those who remained virally suppressed over the study period. We explore the timing and frequency of the VBEs and identify the clinical impact of single or multiple VBEs. Characterization of the incidence, associated risk factors, and outcomes of VBEs is needed to inform, focus, and justify preventative interventions for VBEs in PWH.
Methods
Since 1989, the Southern Alberta Clinic (SAC) has, under the Canadian universal health care system, provided all PWH living in southern Alberta (catchment ∼2.25 million) exclusive, free HIV care. The closest alternate HIV care provider program is 180 km (i.e., 111 miles) distant. SAC uses a model of centralized outpatient care (i.e., single HIV clinic) but decentralized (i.e., all regional hospitals) inpatient care. The SAC database collects detailed sociodemographic, clinical, treatment, and outcome data on all PWH updated at every visit.
All patients followed at SAC with two or more viral load tests between January 1, 2010, and January 1, 2020, were evaluated. Patients were followed until they moved out of the area, died, became lost-to-follow-up, or until January 1, 2021 (i.e., the study end date). Patients who never achieved viral suppression (i.e., defined as <40 copies/mL) or, after initial viral suppression experienced a viral breakthrough but subsequently failed to re-achieve suppression during the study period were excluded. We also excluded viral blips (defined as viral loads <500 copies/mL while on treatment) as these episodes are not believed to result in immunologic damage. 18 –20
Patients were divided into two groups: patients who remained in care and virally suppressed throughout the study period, and patients in care who experienced one or more VBEs. Viral breakthrough was defined as one or more sequential viral load measurements of >1000 copies/mL. A VBE is defined as a PWH experiencing a sequence of a suppressed/unsuppressed/suppressed viral load over a sequence of viral load tests. The length of a VBE was defined as time from the last suppressed viral load (<40 copies/mL) before an unsuppressed viral load to the date of the first suppressed viral load after the viral breakthrough.
Sociodemographic variables included gender (male, female, transgender), age at HIV diagnosis, age at entry into the study, and both self-described ethnicity (Caucasian, Native/Indigenous Canadian, Black, or other), and HIV acquisition risk factor [men having sex with men (MSM), women having sex with men (WSM), persons who inject drugs (PWID), other]. Clinical variables included year of HIV diagnosis and CD4 count at HIV diagnosis. Lifestyle variables included self-reported experience of intimate partner violence (IPV), ever homelessness, ever unstable housing, ever incarcerated, ever heavy drinking (binge drinking or more than nine drinks per week), or ever recreational illegal drug use.
As many of these factors both overlap and interact, we developed a simple “difficulties score” that sums the lifestyle variable with equal weight given to each score (total score: 0 to 5). Health outcome variables during study included changes in CD4 count over study period, HIV-related hospitalizations, and HIV/AIDS-related mortality. We also examined the explanation cited by patient to pharmacy for discontinuing ART before a VBE.
Statistical analyses
Descriptive analyses were performed on sociodemographic data and risk factors for those with no VBE versus patients with one or more VBEs using chi-squared tests for categorical variables and t-tests for continuous variables. Observations with missing data (1.4%) were excluded from regression analyses. Poisson regression models with robust variance (approximating log binomial models) estimated crude and adjusted prevalence ratios (aPR) and 95% confidence intervals (CI) comparing risk factors for PWH with any VBE (vs. no VBE) during the study period. A subgroup analysis was conducted among PWH with any VBE comparing those with one VBE with those with two or more VBEs. Models were adjusted for age at HIV diagnosis, year of HIV diagnosis, sex, race/ethnicity, HIV acquisition risk, housing status, heavy drinking, recreational drug use, incarceration, and IPV.
A continuous time-to-event analysis using a Cox proportional hazards model estimated crude and adjusted hazards ratios and 95% CI for death between PWH with any (vs. no) VBE. Models were adjusted for sex, race/ethnicity, HIV acquisition risk, age at HIV diagnosis, housing status, year of HIV diagnosis, CD4 count and age at HIV diagnosis, heavy drinking, recreational drug use, incarceration, and IPV. Kaplan–Meier estimates of the 11-year survival probability by any (vs. no) VBE were calculated. p Value <0.05 with two-tailed tests was considered statistically significant. All analyses were performed using STATA version 16.0 (College Station, TX, USA).
This study was approved by the University of Calgary Conjoint Health Research Ethics Board as a quality improvement initiative (Ethics ID REB15-0929_REN8).
Results
Characteristics of the study population
Between January 1, 2010, and January 1, 2020, 2475 PWH in care at SAC received at least two viral load tests. Of these, 2096 met the study inclusion criteria. Throughout the study period, 1710 (82%) patients maintained uninterrupted viral suppression over 15,453 years of follow-up. However, 386 (18%) PWH, after initially achieving suppression, experienced one or more VBEs (Table 1): 240 (11%) had only one VBE, whereas 146 (7%) experienced multiple VBEs (100 had two episodes, 29 had three episodes, 11 had four episodes, 5 had five episodes, and 1 patient had six VBEs).
Sociodemographic, Clinical, and Lifestyle Characteristics of Patients Followed at the Southern Alberta Clinic (January 1, 2010, to January 1, 2020) with Two or More Viral Load Tests
All p values comparing no VBE with any VBE were <0.001.
All p values comparing one VBE, two or more VBEs, and no VBE were <0.001.
Heavy drinking = males: more than nine drinks per week, females: more than six drinks per week, or binge drinking = six or more drinks at single setting.
Recreational drug use = single or multiple uses of recreational drugs per week.
IPV: either current, past (as adult), and/or as children (<18 years of age).
Stable housing = renting or own; homelessness = no fixed address; unstable = living in shelters, shared supported housing, short-term stays with friends/family.
Incarcerated either provincially or nationally, either short term or long term.
Difficulties score: total of ever IPV, unstable housing, incarcerated, heavy drinking, and recreational drug use (one patient each = 5 points total).
IPV, intimate partner violence; IQR, interquartile range; MSM, men having sex with men; WSM/MSW, heterosexual sex; PWID; persons who inject drugs; SD, standard deviation; VBE, viral breakthrough episode (i.e., suppressed/unsuppressed/suppressed viral load).
The median length of a VBE for patients with only one VBE was 325 [interquartile range (IQR) 246–360] days; for patients with two or more VBEs, the median length was 375 (285–425) days. For PWH with multiple VBEs, the median number of days spent virally suppressed between VBE was 625 days but varied widely with IQR of 335–1066 days. On each occasion, the individual managed to successfully recapture viral control demonstrating both interest and an ability to reconnect to care and take ART successfully.
Risk factors for experiencing a VBE
When compared with patients maintaining viral suppression, PWH with VBEs were both younger at their HIV diagnosis (median age 31 vs. 35 years) and age at entry into the study (39 vs. 43 years; p < 0.001) and had been living with HIV longer with a median year of diagnosis 2004 versus 2006 (Table 1) compared with patients without any VBE. There was no difference between those with (vs. without) VBE based on initial CD4 count (338/mm3 vs. 342/mm3; p = 0.56). The most common (i.e., >70%) reason noted for discontinuation of ART before a VBE was “patient's decision,” with physician's recommendation (12%) and/or mental health issues (11%) that contributed to nonadherence also cited (data not shown).
In crude analyses, females were 51% (95% CI 1.25–1.83) more likely to experience a VBE compared with males; however, following adjustment, this association attenuated to a statistically nonsignificant 17% increase (95% CI 0.94–1.46; Table 2). In crude analyses, Indigenous PWH had a 95% increased risk of experiencing a VBE compared with Caucasian PWH; however, this association attenuated to no difference in adjusted analyses. In adjusted analyses, individuals who were diagnosed with HIV younger were at higher risk of experiencing a VBE compared with those diagnosed >40 years old. PWID had a 46% increased risk of VBE and those with WSM/MSW HIV acquisition risk had a 56% increased risk, compared with MSM PWH.
Crude and Adjusted Prevalence Ratios of Risk Factors Associated with Any Viral Breakthrough Episode Compared with No Viral Breakthrough Episode (N = 2068)
Prevalence ratios were estimated using Poisson regression models with robust variance and adjusted for all variables in the table.
Bold signals statistically significant p values (<0.05).
Heavy drinking = males: more than nine drinks per week, females: more than six drinks per week, or binge drinking = six or more drinks at single setting.
Recreational drug use = single or multiple uses of recreational drugs per week.
Incarcerated either provincially or nationally, either short term or long term.
Stable housing = renting or own; homelessness = no fixed address; unstable = living in shelters, shared supported housing, short-term stays with friends/family.
IPV: either current, past (as adult), and/or as children (<18 years of age).
aPR, adjusted prevalence ratios; CI, confidence interval;
The risk of VBE was increased by 36% among those who experienced IPV (vs. never reported IPV), 44% among PWH with unstable housing and 79% among homeless (vs. PWH with stable housing), 51% among PWH who were ever incarcerated (vs. never incarcerated), 47% among PWH ever reporting heavy alcohol intake (vs. never), and 82% among PWH ever reporting illegal recreational drug use (vs. never). These differences are reflected in higher cumulative-associated lifestyle/difficulties scores when comparing PWH with (vs. without) VBE (1.76 vs. 1.01).
Risk factors for PWH with one VBE experiencing multiple VBEs
Compared with those with one VBE, PWH who experienced multiple VBEs were 36% more likely to be female (95% CI 1.06–1.76), 51% more likely to have been ever incarcerated (95% CI 1.15–1.97), 38% more likely to have ever reported IPV (95% CI 1.04–1.82), 41% more likely to have unstable housing (95% CI 1.02–1.94), and 92% more likely to ever report homelessness (95% CI 1.43–2.58) versus stable housing (Table 3). In adjusted analyses, the only characteristic that remained significantly associated with having multiple VBEs (vs. 1 VBE) was being female sex (aPR 1.44, 95% CI 1.05–1.99) and reporting homelessness (aPR 1.75, 95% CI 1.23–2.51) compared with PWH with stable housing. PWH with multiple VBEs had higher lifestyle/difficulty scores (2.09 vs. 1.57) compared with those with one VBE (Table 1).
Crude and Adjusted Prevalence Ratios of Risk Factors Associated with Experiencing Multiple Viral Breakthrough Episodes (N = 146) Compared with One Viral Breakthrough Episode (N = 240)
Prevalence ratios were estimated using Poisson regression models with robust variance and adjusted for all variables in the table.
Bold signals statistically significant p values (<0.05).
Heavy drinking = males: more than nine drinks per week, females: more than six drinks per week, or binge drinking = six or more drinks at single setting.
Recreational drug use = single or multiple uses of recreational drugs per week.
Incarcerated either provincially or nationally, either short term or long term.
Stable housing = renting or own; homelessness = no fixed address; unstable = living in shelters, shared supported housing, short-term stays with friends/family.
IPV: current, past (as adult), and/or as children (<18 years of age).
aPR, adjusted prevalence ratios; CI, confidence interval;
Long-term health outcomes associated with VBE
PWH experiencing a VBE had worse short- and long-term health outcomes than PWH with no VBE (Table 4). PWH with one or multiple VBEs experienced lower overall CD4 counts (median −447/mm3 and 335/mm3, respectively) during the study period when compared with those without VBE (576/mm3) and had lower median increases (+27/mm3 vs. +36/mm3 vs. 80/mm3, respectively) in CD4 over time. Overall, 138 PWH had HIV-related hospitalizations (97 had one admission and 41 had more than one admission). Only 4% (n = 75) of PWH without any VBE had a HIV admission in contrast to 16% (n = 63) PWH with at least one VBE. PWH with multiple VBEs were hospitalized relatively more frequently than PWH with only one VBE (18% vs. 15%).
Health Outcomes of Patients Followed at the Southern Alberta Clinic (January 1, 2010, to January 1, 2020) with Two or More Viral Load Tests
p Value comparing no VBE with any VBE.
Median CD4 based on the difference between the earliest and latest CD4 count for each patient during the study period.
IQR, interquartile range; PWH, persons with HIV; VBE, viral breakthrough episode (i.e., suppressed/unsuppressed/suppressed viral load).
During the study period, 139 patients (7%) died: 11 of HIV-related conditions, 117 of non-HIV-related conditions, and 11 of unknown or unreported causes. Among PWH with no VBE, overall mortality was 6%, with 5% of deaths are HIV-related. Among PWH who experienced any VBE, 12% PWH died, with 13% dying of HIV-related conditions. An overall mortality rate of 12% was seen in PWH who had multiple episodes of VBE, with 17% listing HIV as cause of death (Table 5). Over the 11 years of follow-up, the risk of death was 67% higher among PWH who experienced any VBE compared with no VBE (95% CI 1.17–2.38; Fig. 2). However, this increased mortality risk attenuated to a statistically nonsignificant 47% (95% CI 0.97–2.23) in adjusted analyses. Compared with PWH with no VBE, the adjusted risk of death was 74% (95% CI 1.10–2.77) higher among PWH who experienced one VBE and 12% greater (95% CI 0.63–2.00) among PWH who experienced multiple VBEs.
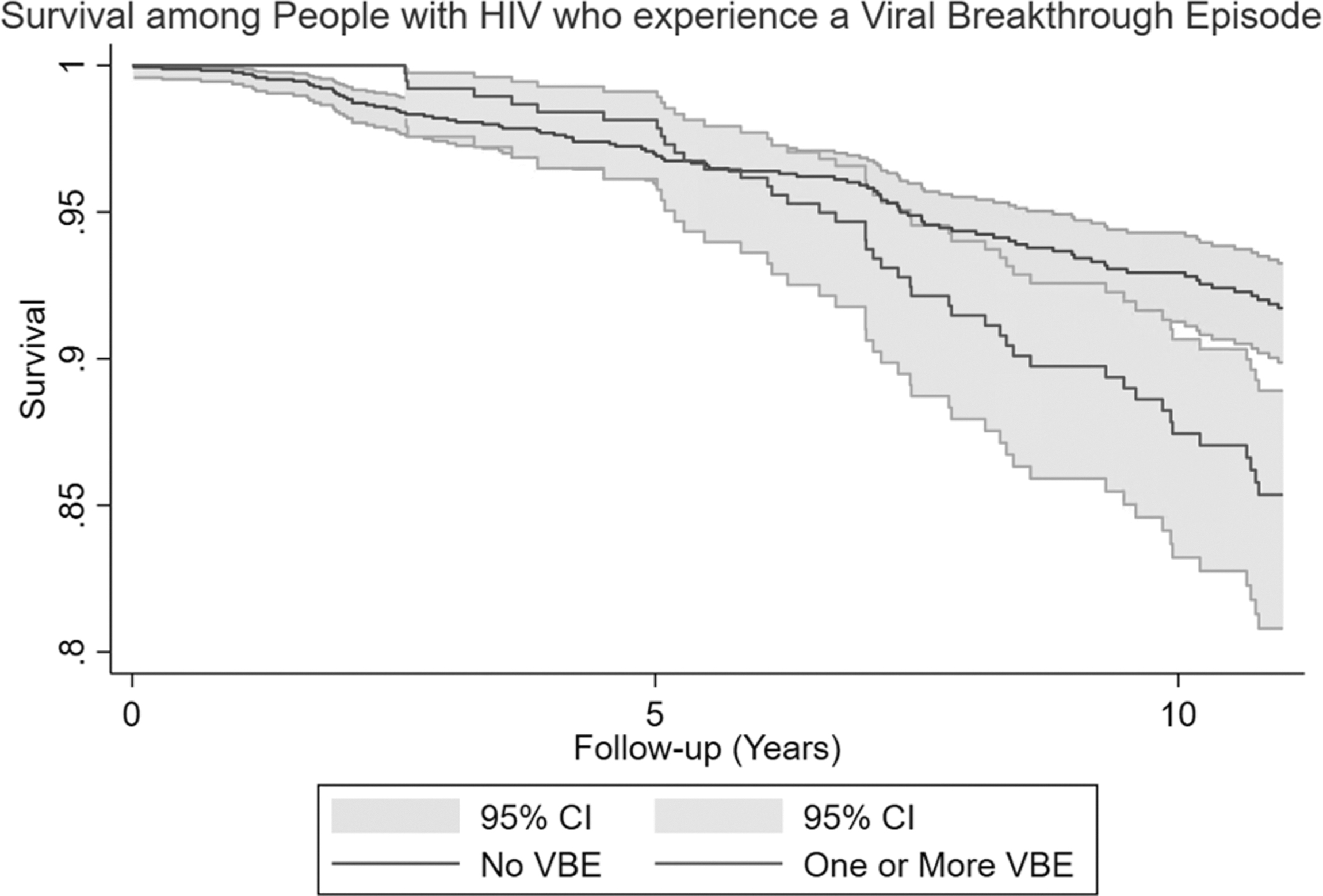
Kaplan–Meier survival graph for survival among people with HIV comparing those who experience no VBE with those who experience one or more VBEs over 11-year follow-up. (N = 2096 PWH, with 16,340 person-years of observation). PWH, persons with HIV; VBE, viral breakthrough episodes.
Hazards Ratios for Death Among Persons with HIV With and Without Viral Breakthrough Episode and by Viral Breakthrough Episode Category Between 2010 and 2021
Adjusted models include sex, race/ethnicity, HIV acquisition risk, heavy alcohol use, recreational drug use, IPV, CSC, age at HIV diagnosis, housing status, year of HIV diagnosis, CD4 count, and age at HIV diagnosis.
Continuous time-to-event analysis using Cox regression models to estimate the hazard ratio for death.
No VBE = no unsuppressed VL.
VBE = one or more unsuppressed episodes.
One VBE = only one unsuppressed episode.
Multiple VBEs = more than two unsuppressed episodes.
aHR, adjusted hazards ratios; CI, confidence interval;
Discussion
Over the past decade, while 82% of PWH within our study who had initiated ART and achieved viral suppression maintained continuous viral suppression; 18% of patients, after an initial success in achieving viral suppression, subsequently lost, and then recaptured control of viral replication. We examined both the sociodemographic and the social determinants of health of those both maintaining and failing to maintain continuous viral suppression. Viral breakthrough was more common among women (25% vs. 17% in men); women were also, after a first breakthrough event, at even great risk of second or more VBEs, with 46% experiencing additional VBEs.
Both Indigenous ethnicity and injection drug use posed higher risk for breakthroughs. While we identified a younger age at diagnosis of HIV as being more strongly associated with VBE, there may be a bias due to longer duration in care as we also identified a reduced risk of VBE among those diagnosed with HIV following 2010 compared with people diagnosed before 2000. We found that social determinant cofactors of health rather than many of the medical determinants of health had stronger association with a patient experiencing a VBE. PWH who had experienced IPV, unstable housing, and past incarceration were more likely to have one or more VBEs.
Riley et al. 21 also have documented strong association being unstable housing and unsuppressed viral loads especially among women. They advocate strongly for addressing housing needs first to deal with unsuppressed viral load issues. Dawit et al. 22 found that neighborhood factors and housing instability impact viral suppression rates among Ryan White program clients in Miami-Dade County, Florida. Our findings support their study. Siemieniuk et al. 23 found poorer health outcomes overall, including lower rates of viral suppression, among PWH who had ever experienced IPV. Less clear is the association with heavy drinking and recreational drug use with VBE, although it is suggestive of an impact. Lesko et al. 24 did find an increased risk on unsuppressed viral loads among PWH who reported recent substance use.
To determine if one or more episodes of VBE had clinical implications for an individual's health, we looked at three routine health metrics used in PWH care, namely CD4 count preservation, hospitalization, and death. Despite similar baseline CD4 counts, PWH experiencing VBE had lower CD4 counts to those with no VBE and multiple VBEs led to even lower counts. Whereas only 4% of patients who experience no VBE had one or more HIV-related hospitalizations, 16% of patients experiencing VBE had HIV-related admissions. Patients ever having experienced a VBE had nearly double the rates of all-cause mortality; 12% died compared with 6% of patients never having had a VBE. These results compliment research reported by Elvstam et al. 25,26 that show that low-level viremia is associated with increased rates of virological failure and all-cause mortality.
These findings highlight that nearly one in five PWH who are both interested in and have been successful in taking ART may struggle with ongoing suppression, but they can recapture viral replication on reengagement. This is a distinct population from the PWH who either have no interest in ART or are unable when dispensed ART to be successful in achieving suppression. Common negative social determinants of health are contributing to VBEs and a worse HIV prognosis. We suggest that intervention, particularly after one VBE, is needed to further viral breakthrough and ongoing success as these individuals have distinct social and emotional challenges that need to be addressed. 27
This study has limitations despite being both longitudinal and comprehensive for a diverse and geographically defined HIV population. PWH within our cohort may not be representative of other such populations. Our definition of what constitutes a VBE and the length of time within an episode while pragmatic and can be generalized it is not precise. We only used the social determinants of health available in our data set that may not completely reflect all the factors involved in VBEs. Further precision in exploring patient reasons for temporarily disengaging from ART.
The prior treatment guidelines may have impacted results as previously it was more common for clinicians to recommend discontinuation of therapy for certain results; however, this study should not be impacted by this as once the decision was made to initiate ART (i.e., gain viral suppression), the intention was always to continue. We did not examine how food insecurity 28 may impact HIV health outcomes, which may lead to higher rates of unsuppressed viral load. We did not measure the important area of costs to health care from VBE(s), and we did not measure any societal costs or health impact on others from secondary transmissions occurring during VBE. We also did not investigate the incidence of secondary transmissions occurring during a VBE, which might require both contact tracing and phylogenetic studies.
This study suggests to us that additional care initiatives need to be both available and offered for the PWH population on treatment and at greatest risk of VBEs. This PWH population is unique and accessible and has already successfully achieved viral suppression. Measures such as injectable ART, IPV prevention, and social support for housing may be both easy to implement and highly effective in maintaining a patient's existing successful engagement to ART. The additional cost of such interventions may be partially defrayed by saved costs from the ill-health resulting from a VBE being avoided.
We identified and characterized the 18% within our total PWH who, after successful use of ART, subsequently stopped treatment and then later successfully reengaged to ART. Social factors rather than medical factors were strongly associated with VBE. As measurable and sustained physical damage occurring during VBE, the importance is apparent for identifying those at risk for VBE and then using customized proactive interventions for VBE prevention, which would result in both improved personal and public health.
Footnotes
Authors' Contributions
M.J.G. and H.B.K.: project formulation, data collection, data analysis, construction, and writing article. R.L.: data analysis, construction, and writing article.
Author Disclosure Statement
M.J.G. has received honoraria for ad hoc participation in the National HIV Advisory Boards to Merck, Gilead, and ViiV. None of the other authors report any conflicts of interest.
Funding Information
No funding was received for this article.