
Abstract
People living with human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS; PLWHA) frequently encounter antiretroviral (ARV) therapy-related problems. Clinical pharmacists with specialized training in ARV stewardship play an important role in managing these problems. However, there is a paucity of evidence to clarify the impact of clinical pharmacists' interventions on managing ARV therapy-related problems in PLWHA. Therefore, we aim to systematically review the literature to determine the nature and impact of pharmacists' interventions on managing medication-related problems in PLWHA. The review protocol was registered on International Prospective Register of Systematic Reviews (PROSPERO; CRD42020173078). Relevant records were identified from six electronic bibliographic databases (PubMed, Embase, EBSCOhost, ProQuest, Scopus, and the Cochrane Central Register) from their inception until September 2022. We included all randomized and nonrandomized interventional studies that were published in English. After the abstract and full-text screening, data were extracted from the selected studies, and the quality of the studies was assessed. The electronic database search and citation tracking identified two thousand and three citations. The review included 21 of these studies, involving 2998 PLWHA, published between 2014 and 2022. Pharmacists' interventions, working alone or in a multi-disciplinary team, comprised ARV medication review, management of adverse drug reactions (ADRs), therapeutic drug monitoring, prevention of drug interactions, and provision of drug information to PLWHA or the health care team. The pharmacist-involved interventions significantly reduced incorrect/incomplete ARV regimens, drug interactions, incorrect dosages, duplicate therapy, polypharmacy, administration errors, missing medication, wrong formulation, ADRs, and prescribing errors. Most studies reported that physicians usually accept more than 90% of the pharmacists' recommendations. ARV medication-related problems remain highly prevalent in PLWHA. Pharmacist-led interventions and stewardship significantly reduce ARV therapy-related problems in PLWHA and are widely accepted by physicians. Dedicated pharmacists with specialized training and credentialing in infectious diseases or HIV/AIDS have a great potential to improve health outcomes in PLWHA.
Introduction
Since the introduction of combination antiretroviral therapy (cART) in 1996, the human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) has metamorphosed from being a fatal illness to a chronic manageable condition. 1,2 Highly active antiretroviral therapy has significantly reduced the number of AIDS-related mortality rates; ∼650,000 people died from AIDS-related illnesses globally in 2021, compared with about 2 million people in 2004. 3 Regular use of antiretroviral (ARV) agents suppresses the viral load (VL), boosts the immune system, and helps to improve the quality of life (QoL) of people living with HIV/AIDS (PLWHA). 2,4 –6 PLWHA frequently bear the burden of chronic comorbid conditions such as diabetes, tuberculosis, hepatitis, and hypertension, and concurrent treatments pose a significant risk for medication-related problems. 7 –9
In a Swiss cohort of 1500 PLWHA, 68% of the patients received medications other than cART. 10 The most common medicines coadministered with ARV therapy were antibiotics, antidepressants, antithrombotic, and antipsychotic agents. 10 Around 40% of the participants included in this study had at least one potential drug–drug interaction (DDI) that resulted in severe, supratherapeutic drug toxicities or, conversely, in decreased efficacy of coadministered medications. 10 CYP3A4 is known to be inhibited by protease inhibitors, and administering medications that are metabolized by the CYP450 system concurrently with the former can result in drug concentrations above therapeutic levels with a consequent increase in toxicity. 11,12 In contrast, non-nucleoside reverse transcriptase inhibitors (NNRTIs) typically induce CYP450 enzymes, which can result in subtherapeutic levels of coadministered drugs that are metabolized by this pathway. 13
Medication errors in PLWHA vary widely across studies, from 5% to 86%. 14 Patients hospitalized or taking medications for opportunistic infections (OIs) or prophylaxis are at a higher risk for developing drug-induced conditions due to medication errors. 14,15 Most medication errors in PLWHA occur during hospital admissions, with more than one-third remaining uncorrected at discharge. 15,16 Managing patients with HIV/AIDS requires a comprehensive approach by a multi-disciplinary team (MDT), comprising physicians, pharmacists, nurses, and microbiologists because it is multi-faceted and challenging. 17,18 To improve the clinical and humanistic outcomes of PLWHA, the provision of pharmaceutical care (PC) services by clinical pharmacists in an MDT is highly warranted. 19,20 Pharmacists have a crucial role in shaping and achieving successful management outcomes because of their clinical and pharmacological expertise. 15,21
Several studies have documented positive outcomes of pharmacists' collaboration with physicians, nurses, and other health care professionals (HCPs). 15,22 –24 In particular, pharmacists have conducted medication use reviews, optimized drugs, managed DDIs, monitored adverse drug reactions (ADRs), and identified medication-related problems in patients with HIV/AIDS. 24 –26 PLWHA who receive treatment from an HIV expert, including a physician and a pharmacist, have better adherence, improved outcomes, decreased mortality rate, and cost containment. 19,27,28
Previous systematic reviews on the management of PLWHA have assessed the impact of pharmacist-delivered educational interventions in improving health outcomes such as adherence, VL suppression, improved CD-4 T lymphocytes, and the economic impact of pharmacist interventions (PIs). 19,27 These reviews, however, did not explore the pharmacist's role other than providing adherence education in HIV/AIDS management. To date, no published systematic study summarizes the pharmacist's role in managing ARV therapy-related problems. Antiretroviral stewardship programs (ARVSPs) have decreased medication error rates and improved other outcomes. 15,29 Therefore, we aim to systematically review the literature to determine the nature and impact of pharmacists' interventions on managing medication-related problems in PLWHA.
Methods
The study was carried out following the Cochrane Handbook guidelines, 30 and the findings were reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 checklist. 31 The review protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO; CRD42020173078).
Database searches
To retrieve relevant studies, we searched six electronic bibliographic databases (i.e., PubMed, Embase, EBSCOhost, ProQuest, Scopus, and the Cochrane Central Register) from inception to September 30, 2022. Keywords used were “HIV,” “AIDS,” “pharmacist,” “pharmaceutical care,” “ARVs,” “antivirals,” “medication management,” “medication problems,” and “medication review.” We used Boolean operators “OR,” “AND”, and “NOT” to combine these terms. We also searched PubMed and EMBASE using the medical subject headings “MESH” and EMTREE (controlled vocabulary thesaurus), respectively. Due to technical differences and restrictions in each database, the search method in each database was modified as necessary. We used Google Scholar as a secondary citation monitoring resource to look for any other studies that were missed during our systematic search. We also searched the gray literature to find any relevant studies.
Selection criteria
To construct the inclusion and exclusion criteria, the PICOS (Population, Intervention, Comparator, Outcome, and Study designs) strategy was used. Studies were included if they were: (1) Pre–post, prospective, or retrospective cohorts, randomized controlled trials (RCTs), and quasiexperimental studies; (2) evaluating pharmacist (alone or within an MDT)-managed PC interventions in PLWHA; (3) measuring relevant outcomes such as identification of medication-related problems; (4) conducted among outpatients or inpatients in the hospital or community pharmacy settings; (5) and published in a peer-reviewed journal in English language only. Letters, correspondences, case studies, news articles, viewpoints, editorials, qualitative studies, and conference abstracts were excluded from the review.
Data screening and extraction
Relevant databases were searched, and citations were imported into the EndNote® citation management software. Subgroups were created for each database citation in the software. The software was used to remove duplicates. Two authors (A.A.1 and M.T.) independently assessed the titles and abstracts of all retrieved studies. A.A. conducted a thorough article screening using a preliminary screening form, and all authors independently examined it. Articles were finally included based on the authors' predetermined eligibility criteria and mutual agreement. After selecting relevant studies, A.A. independently extracted the data using a standardized Cochrane data extraction form. A second reviewer (M.T.) reviewed the extracted data for consistency and accuracy. All of the included studies' details (title, objective, publication year, and first author), country, study design, intervention details, sample size, sample components (e.g., age, gender), control group, intervention outcomes, and statistical results were extracted.
Risk of bias
The methodological quality of the included studies was assessed by A.A. and M.T. Disagreements were resolved by mutual discussion. RCT quality was assessed using the Cochrane Risk of Bias (ROB 2.0) assessment tool. 32 The quality of nonrandomized studies of interventions was evaluated through the Risk of Nonrandomized Studies of Interventions (ROBINS-I) assessment tool. 33 The National Heart, Lung, and Blood Institute (NHLBI) tool was used for quality assessment of pre–post studies with no control group. 34
Outcomes of interest
The review mainly focused on studies that reported the pharmacist's role in managing ARV medication-related problems. The details of primary and secondary outcomes that were explored in the review are provided below.
Primary outcomes
Identification and management of medication-related problems such as medication errors, incorrect combination regimen, incorrect dosage, duplicate therapy (regimens contained multiple medications of the same ARV pharmacological category) or polypharmacy, incorrect administration, omission/incomplete regimen, missing medication, safety errors, incorrect formulation, ADRs, OI prophylaxis, renal dosage adjustment, and drug interactions.
Secondary outcomes
Time to correct errors, smoking, blood pressure control, hospital readmission prevention, number of interventions accepted by physicians, adherence, VL, CD-4 count, economic impact, body mass index, and lipid control changes in PLWHA.
Data synthesis
We used the Descriptive Elements of Pharmacist Interventions Characterization Tool (DEPICT) version 2 to identify the components of PIs performed as a part of clinical pharmacy services. 35 DEPICT allows for the retrospective analysis of published studies and can be used as a reference guide to report PIs in future studies. 36 The findings of the selected RCTs, cohort studies, and pre–post intervention studies were qualitatively synthesized rather than combined for meta-analysis due to lack of consistent quantitative data, heterogeneity in settings, and methods of included studies. Text summaries and summary tables were created using the extracted data.
Results
Literature search, screening, and identification of studies
Figure 1 represents the studies' identification and screening process using the PRISMA flow diagram. Two thousand and three citations were found through electronic database searches, citation tracking of references, and records identified from other sources. Four hundred sixty-seven duplicate citations were removed, and the remaining 1536 citations were reviewed and screened for titles and abstracts. This resulted in 83 full-text articles considered for eligibility. Of those, 62 studies were excluded with reasons in the PRISMA flow diagram. Finally, 21 of these studies, involving 2998 PLWHA, published between 2014 and 2022 were included in the qualitative synthesis. 37 –57
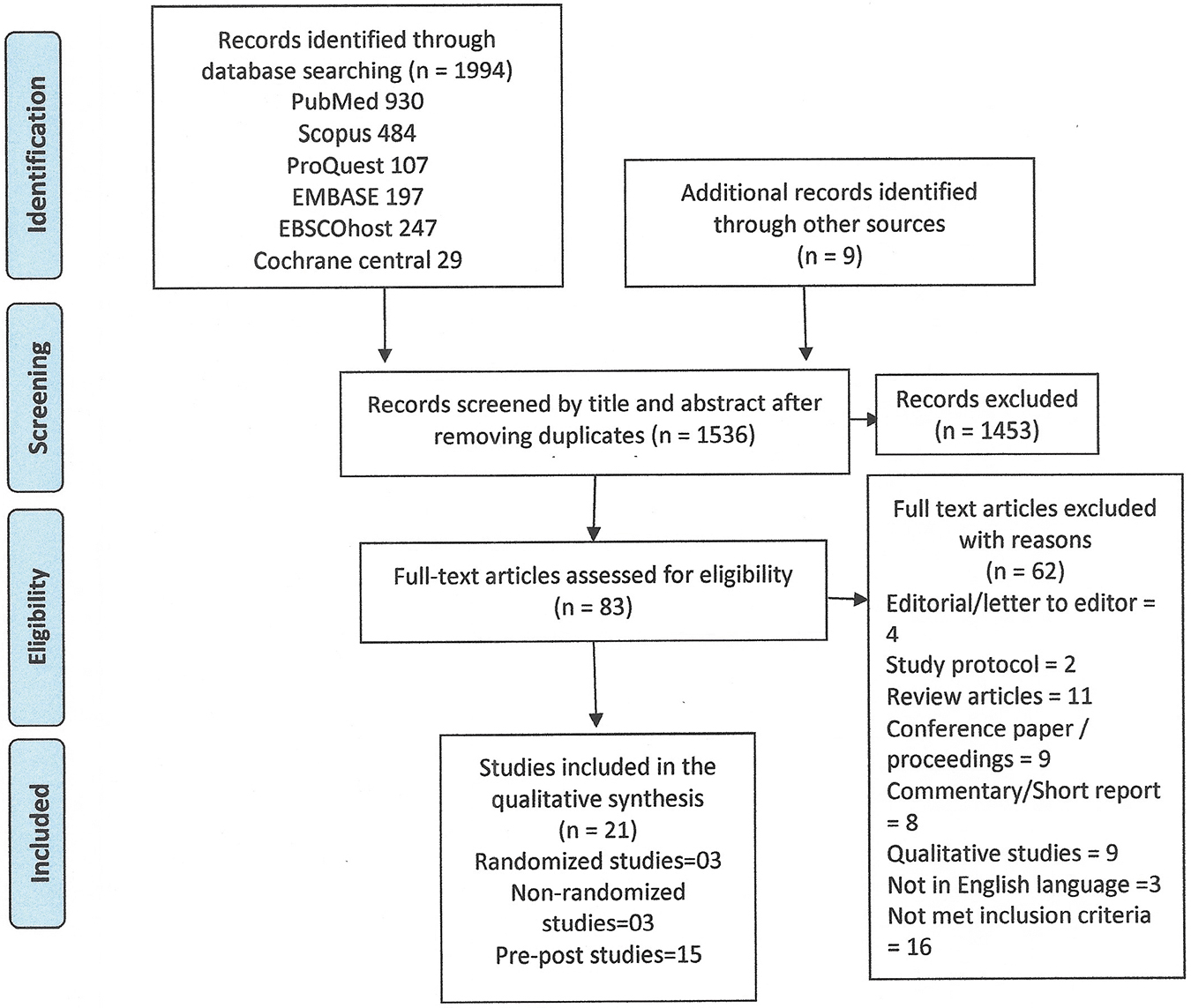
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Characteristics of the included studies
Of the 21 studies included in the review, 3 were RCTs, 44,45,48 3 were cohort studies with control groups, 41,43,47 and 15 were pre–post studies without a comparison group. 37 –40,42,46,49 –57 Most studies (14 of 21) were conducted in the United States, 37 –39,42,43,46,49 –54,56,57 followed by 3 studies in Spain, 40,44,48 2 in Brazil, 41,47 and 1 each in Japan 55 and Nigeria. 45 Participants in the studies belonged to five continents; a majority of the studies were conducted in North America, 37 –39,42,43,46,49 –54,56,57 followed by Europe, 40,44,48 South America, 41,47 Africa, 45 and Asia. 55 Except for one multi-center study, 48 the remaining studies were single-center studies. 37 –47,49 –57
All of the studies were conducted in a hospital setting, with 14 studies involving inpatients 37 –39,42,44,46,49 –54,56,57 and 7 studies involving outpatients. 40,41,43,45,47,48,55 The sample sizes of the included studies ranged from 23 44 to 349 participants. 40 The age of PLWHA ranged from 18 to 89 years. Moreover, the duration of follow-up in the studies ranged from 6 months 42,57 to 8 years. 55 The detailed characteristics of the included studies are provided in Table 1.
Characteristics of the Included Studies (n = 21)
ART, antiretroviral therapy; ARVs, antiretrovirals; ARVSP, antiretroviral stewardship program; ASP, antimicrobial stewardship; BMI, body mass index; BP, blood pressure; CG, control group; CMO, Capacity Motivation-Opportunity; CVD, cardiovascular disorders; DRP, drug-related problem; EMR, electronic medical record; HAART, highly active antiretroviral therapy; HIV/AIDS, human immunodeficiency virus/acquired immunodeficiency syndrome; ICD-10, International Classification of Diseases 10th Revision; ID, infectious disease; IG, intervention group; IQR, interquartile range; LDL, low-density lipid; LOS, length of stay; NR, not reported; OI, opportunistic infection; PBPM, protocol-based pharmacotherapy management; PC, pharmaceutical care; PGY, postgraduate year; PI, pharmacist intervention; PLWHA, people living with HIV/AIDS; Postint, postintervention phase; Preint, preintervention phase; RCT, randomized controlled trial; SD, standard deviation; TOC, transitions of care; VL, viral load.
Quality assessment of the included studies
Two RCTs had low risk of bias, while for one RCT, the risk of bias was unclear. Cohort studies with control groups were rated as moderate risk of bias (1 of 3), serious risk of bias (1 of 3), and critical risk of bias (1 of 3). Ten of the 15 pre–post studies without a control group were rated fair, while the remaining 5 were rated good. No studies were excluded based on the risk-of-bias assessment. Figures 2 and 3 show the risk of bias of the three RCTs. Tables 2 and 3 display the specifics of ROB for the cohort and pre–post studies, respectively.

Graphic representation of risk of bias of included RCT studies. RCT, randomized controlled trial.
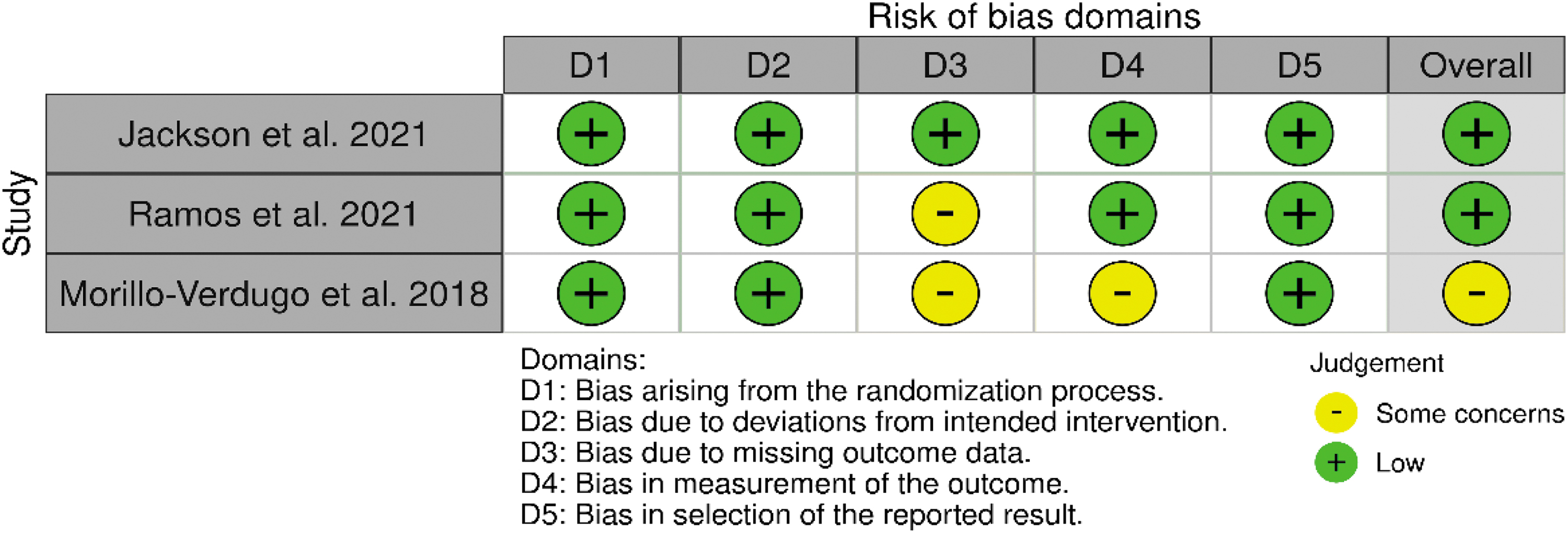
Assessment of the risk of bias of each RCT. RCT, randomized controlled trial.
Summary of Quality Assessment of Included Nonrandomized Intervention Studies (n = 3)
Quality Assessment for Pre–Post Studies Without a Control Group (n = 15)
Quality rating criteria: Poor: <4 points; Fair: ≥4–8 points; Good: >8 points.
Refer to the original tool cited in article.
If this question is NA, total score is out of 11, not 12.
CD, cannot determine; N, no; NA, not applicable; Y, yes.
Description of pharmacist's interventions
In all the studies, the pharmacists were trained in infectious diseases (IDs). The number of pharmacists involved in providing interventions ranged from 1 to 5. In 18 of the 21 studies, the pharmacist was the sole provider of intervention, 37,38,40 –42,44 –48,50 –57 while in the remaining 3 studies, the pharmacist delivered the intervention as part of an MDT. 39,43,49 In all studies, pharmacists have one-to-one contact with patients and access to their medical records. Pharmacists obtain the patients' information from the patient's medical records or through direct patient interviews. In general, pharmacists, in consultation with physicians, manage different aspects of medication-related problems such as medication review, medication reconciliation, dosage, incomplete regimen, management of ADRs/side effects, therapeutic drug monitoring, and identification and prevention of drug interactions. Pharmacists also provided lifestyle modifications to lower lipid levels, alcohol moderation, cardiovascular risk prevention, mental health interventions, laboratory data review (VL, CD-4 T lymphocytes), and OI prophylaxis. Adherence to ARVs is challenging and pharmacists use cognitive behavioral therapy to improve adherence in PLWHA. Cantillana-Suárez et al, for example, reported that over a 2-day session, pharmacists received initial training that covered the frameworks for changing patient behavior as well as educational skills to provide the intervention. 40 Similarly, Brizzi et al reported that before the study, pharmacists were trained in structured interview protocol as well as communication and motivational interviewing skills. 38 Cognitive behavior therapy was used to change the attitudes of PLWHA toward ARV adherence. Motivational interviewing and problem-solving treatment were used as counseling methods. Table 4 describes the details of pharmacist-delivered services in each study as described by DEPICT version 2. Further details of specific roles performed by the pharmacist in each study are detailed in Table 5.
Description of Pharmacist Intervention in the Included Studies According to Descriptive Elements of Pharmacist Intervention Characterization Tool Version 2
ADR, adverse drug reaction; ARV, antiretroviral; DDI, drug–drug interaction; EMR, electronic medical record, HIV, human immunodeficiency virus; LOS, length of stay; NR, not reported; TDM, therapeutic drug monitoring; VL, viral load.
Description of Pharmacist's Specific Interventions
Foot/dental care, alcohol moderation.
Cardiovascular risk prevention.
Quality of life.
Economic role.
Creatinine clearance.
Mental health, laboratory data review.
Hepatic tests.
OI prophylaxis.
ADR, adverse drug reaction; OI, opportunistic infection; TDM, therapeutic drug monitoring.
Description of MDTs
In three of the 21 studies, the pharmacists worked in an ARV stewardship team (AST) comprising other HCPs such as ID physicians, 39,49,57 clinical microbiologists, 39 and infection prevention nurses 39 to manage ARV therapy. In an AST, pharmacists provided PC activities such as interviewing patients, assessing patients' medical history (drug allergies, history of drug abuse, potential for hepatic or renal toxicity, and potential for adverse effects), reviewing patients' medications, optimizing medication therapy (medication recommendations, dose conversions, and adjustments through patient rounds and consultation), identifying drug-related problems, monitoring ADRs, and providing educational services to the PLWHA.
In one study, the AST designed a questionnaire to help them identify medication errors. 57 Errors were noted in the i-vent online system to record and communicate recommendations and interventions within patient records. The resident pharmacist handled the interventions, while the physician and HIV pharmacist guided the patients. 57 In another study, the AST led by an ID pharmacist, developed a pocket guide regarding the therapeutic management of HIV. 39 All hospital pharmacists were provided with training to use the guide, and proficiency with its use was added as an annual competency requirement. The AST included the pocket guide at order verification of ARVs to identify inappropriate regimens or nonformulary substitutions. 39 Interdisciplinary approaches led to a significant decrease in medication errors 39,49,57 and time to rectify these errors. 57
Tools used to measure relevant outcomes
The included studies used varying but standard methods for detecting medication-related problems, such as chart review, computerized monitoring, administrative databases, claims data, direct observation, incident reporting, and patient monitoring. Guzmán Ramos et al used the medication regimen complexity index (MRCI) to quantify the complexity of the medication regimens. 44 Medication adherence was measured by the proportion of days covered, 40,44 Adherence to Refills and Medications Scale (ARMS), 45 Morisky Green Levine questionnaire, 40 and the Simplified Medication Adherence Questionnaire (SMAQ). 40,48 To assess actual or potential DDIs, studies used online University of Liverpool HIV drug interaction charts, Lexicomp®, Micromedex®, and the Department of Health and Human Services (DHHS) guidelines for assessing drug interactions. 49,54,56 Further, Morillo-Verdugo et al used the Framingham score for coronary artery disease assessment. 48
Effect of pharmacist's interventions on medication-related problems
The details of PIs in managing the primary outcomes are provided in Table 6. ARV-related drug interactions are very common in PLWHA. Fourteen studies 37 –39,41 –43,46,47,49 –52,54,57 reported the involvement of pharmacists in managing drug interactions, out of which nine recorded a significant reduction in drug interactions compared with the control group. 39,41,43,46,47,51,52,54,57 The most common drug interactions reported involved integrase inhibitors and polyvalent cations. 39,46,47,51,52,54,57 Studies reported that ARV agents interacted with concomitant medications through CYP450 induction or inhibition or QT-interval prolongation as the primary mechanisms. 39,41,46,47,51,54,57
Primary Outcomes of Pharmacist's Interventions (Medication-Related Problems)
✓, Data reported; +, outcome with statistically significant effect in favor of the intervention.
Polypharmacy.
ADR, adverse drug reaction; OI, opportunistic infection.
Incorrect combinations significantly affect the health of PLWHA. Three RCTs 44,45,48 and 10 pre–post studies 37 –39,42,46,50 –52,54,55 reported PIs in the management of incorrect combination regimens, of which 4 studies 39,50,52,54 reported a significant impact of the pharmacist's activities. Preintervention, protease inhibitor-based regimens were more commonly used, whereas postintervention, NNRTI and integrase strand transfer inhibitors (INSTI)-based regimens were more commonly used. 39,50,51,54 Around 42% and 33% reduction in protease inhibitors and booster prescribing was observed during a review of individual agents by class, respectively, between the pre- and postintervention periods. 39 INSTI prescribing, on the contrary, increased by 28%. 39
Incorrect dosing is commonly reported in PLWHA. One RCT 45 and 10 of the pre–post studies reported PIs in dosage adjustments. 37 –39,42,46,50 –52,54,57 Four studies reported the significant impact of PIs in reducing low- or high-dose-related errors in patients on either lifelong ARV therapy or those receiving prophylactic ARV therapy. 39,46,52,54 The pharmacist was actively involved in dosage adjustments in renal impairment PLWHA in five pre–post studies, 46,50,52,54,57 from which PIs significantly reduced ARV dosing errors in two studies. 50,54
ARV administration error poses a significant threat to patients. One RCT 45 and eight pre–post studies 37 –39,46,51,52,54,57 reported that PIs resolved administration errors such as crushing medicines that were not recommended to be crushed 57 and lack of coadministration with meals. 39,45,51,52 One RCT 48 and five pre–post studies 37,38,50,51,57 reported PI in the detection and resolution of problems such as therapeutic duplication during medication reconciliation and patient education. Likewise, Cantillana-Suárez et al reported the effect of PIs in reducing polypharmacy with consequent improvement of adherence. 40
Omissions or forgetfulness, such as failure to take one of the ARV drugs, can lead to an uncontrolled VL and may result in the development of drug resistance. Six pre–post studies documented PI in reducing ARV omission-related errors. 37 –39,52,56,57 In one RCT 45 and four pre–post studies, 37,38,50,51 PIs resulted in avoiding missing medication-related issues in inpatients. Further, two pre–post studies reported pharmacist involvement in changing ARV formulations, such as switching from oral to intravenous formulation based on the patient's health status. 50,52
Antiretroviral therapy (ART) has potential adverse effects and can result in nonadherence to therapy, thereby negatively impacting health outcomes. Four studies reported that PIs effectively identified and resolved the adverse effects of ARVs. 39,43,44,54 In six studies where PLWHA were admitted to the hospital, pharmacists proactively monitored the safety of ARVs. 37,41,42,49 –51 Pharmacists ensured that clinicians prescribe, dispense, and administer appropriate medicines safely and monitor medication use. 37,42,49,51 The interventions also ensured that consumers were well-informed about medicines and were aware of their medication requirements and risks. 37,49,51
Finally, in three studies, pharmacists were involved in the provision of PC for PLWHA experiencing OIs. 42,53,56 Pharmacist's interventions significantly decreased the dose- and omission-related errors. 42 The timely resolution of medication-related problems is critical, and five studies reported that the presence of a pharmacist had corrected or informed the physician on time and saved the occurrence of medication errors. 37,42,50,51,56
Effect of pharmacist's interventions on secondary outcomes
The details of PIs in managing the secondary outcomes are summarized in Table 7. PIs played an important role in promoting adherence to ART, which is critical for achieving desired health outcomes. 40,44,45,48,49,51,55 Pharmacists typically used cognitive behavioral therapy, directly observed treatment, peer support, and other effective strategies to improve the adherence to ARVs. 40,44,45,48,51,55 Specifically, improvement of adherence by PIs led to viral suppression 40,44,45,47,55 and increased CD4 T lymphocytes. 40,44,47 Three studies reported the effect of PIs in removing barriers to care that were linked to poor virologic and immunologic outcomes and the emergence of ARV drug resistance. 38,41,43 Pharmacists accomplished this through improving PLWHA's access to medications and linkage to care by removing mental health barriers and indirectly saving the cost of hospital readmission. 38,41,43
Secondary Outcomes of Pharmacist's Interventions
✓, Data reported; +, outcome with statistically significant effect in favor of the intervention.
BMI, body mass index; BP, blood pressure; VL, viral load.
Further, the pharmacists distributed information leaflets, conducted individual motivational interviews, and communicated with PLWHA regularly face to face, phone calls, or through text messages about cardiovascular diseases or blood pressure, 44,45,48 body weight, 43,48 health economic benefits of adherence, 38,41,43 healthy living habits, 53 smoking cessation, 43,44,48 and health promotion. 53,57
Discussion
To the authors' knowledge, this is the first systematic review summarizing the pharmacist's role in managing the ARV-related problems in PLWHA. Pharmacists play a vital role in the care of PLWHA and ensure the quality use of medicines, thereby improving medication safety across the continuum of care. A meta-analysis was not performed due to the methodological heterogeneity related to varying study designs, PIs, medication-related problems reported, and follow-up durations. Overall, PIs contributed to reducing the incidence of medication-related problems by decreasing ADRs, drug interactions, dosing problems, administration errors, safety-related errors, hospital readmission, and by improving adherence, CD-4 lymphocytes, VL suppression, smoking cession, and outcomes of comorbid conditions in hospitalized PLWHA.
The most frequently reported interventions included the following: (1) medication reviews, (2) incorrect regimen adjustments, (3) management of ADRs/side effects, (4) therapeutic dosage adjustment, (5) prevention of drug interactions, (6) provision of drug information to patients and HCPs, and (7) lifestyle modification, either exclusively delivered by pharmacists or implemented in collaboration with other HCPs.
Medication review was the most commonly reported intervention, effectively reducing actual and potential ARV-related ADRs, drug interactions, and dosage errors. Medication reviews include dosage adjustments (increase or decrease) for patients with hepatic impairment and chronic kidney disease (CKD), change of medications from oral to intravenous dosage form, starting a first-line or second line ART, and identifying and resolving medication-related problems. 58 Physicians make dose adjustments based on the pharmacist's recommendations, 40,45,47,51 or by the pharmacists based on approved protocols, 52,53,56 or by the pharmacist as a member of the MDT. 39,43,49 Pharmacists decided whether it was necessary to recommend ART adjustments based on the degree of patient's VL, the occurrence of ADRs, liver and kidney function, or the risk of potential DDIs. 59 Hence, medication review should be considered a significant component of pharmacist involvement in managing PLWHA. The studies have shown that medication reviews might not be performed in hospital settings as there is a lack of clinical pharmacists or limited pharmacist roles, especially in resource-constrained settings. 60 –62 Such countries should consider the feasibility of building capacity and employment of pharmacists in ID or HIV/AIDS specialization. 63 –65 Pharmacists are essential members of the MDT managing PLWHA due to their expertise in medication management, background in pharmacology, and contribution to antimicrobial stewardship program implementation. 39,49,57
This review shows that pharmacists can improve HIV/AIDS management and prevent viral resistance to ARVs through patient education, counseling, and consultation. This is especially important when PLWHA need information regarding their disease, management of disease symptoms, diagnosis, treatment, follow-up, and medication side effects. 66 –68 There is sufficient evidence that educational interventions by the pharmacist are beneficial for HIV patients. 27 Another important consideration is that patients with HIV/AIDS frequently require combination therapies for managing comorbidities that could result in more DDIs and toxicities. 69,70 Similarly, evidence showed that pharmacist consultation or patient education reduced DDIs in patients with HIV/AIDS. 26,51,56
There is also an increasing trend toward using complementary and alternative medicine (CAM) therapies along with standard ARVs among PLWHA. 71 Any combination of CAM therapy ARVs and food can cause pharmacokinetic or pharmacodynamic interactions. There is also a scarcity of evidence about the efficacy and safety of CAM therapies. 72 Pharmacists' participation in the CAM consultation should be encouraged because they may play a key role in ensuring the effective use of CAM in patients with HIV/AIDS. 73,74 Therefore, integrating pharmacists as a part of MDT can foster better collaborative care with other HCPs to better manage patients with HIV/AIDS.
PLWHA usually encounter mild-to-severe ADRs, particularly at the onset of therapy, mainly nucleoside reverse transcriptase inhibitor (NRTI), such as zidovudine-induced nausea, constipation, dizziness, vomiting, sleepiness, pruritus, anorexia, and heartburn that are commonly seen after administration. In a cohort study by Khan et al, 42.5% of PLWHA reported ADRs 75 ; lipodystrophy was recorded in 35.5%, followed by skin rashes in 18.8%, anemia in 17.4%, and peripheral neuropathy in 6.3% patients. 75 ADRs can burden patients and the health care system. 76,77 Pharmacists' integration in the MDT can positively impact lowering ADR incidence in PLWHA. 28,78 The usual practice by pharmacists is to identify ADRs during ward rounds and report to the physicians or other concerned stakeholders.
PLWHA are at increased risk of developing acute and CKDs due to a combination of traditional risk factors such as diabetes and hypertension, as well as HIV-related factors such as HIV-associated nephropathy and increased susceptibility to infections and exposure to nephrotoxic medications. 79 Pharmacists with expertise in recognizing potential DDIs, laboratory monitoring, determining drug dosage adjustment, developing monitoring plans, avoiding nephrotoxic drugs, managing kidney disease complications, and establishing effective medication management programs can help PLWHA in their kidney health.
Apart from these interventions, a pharmacist has a potential role that can directly or indirectly help in better management of PLWHA, which includes providing written information, manuals, or booklets to the patients, and providing drug information and education to both patients and HCPs. 80 Providing written information, manuals, or brochures boosts patients' confidence, which may increase their likelihood of complying with treatment, adhering to medications, or seeking appropriate follow-up care, participating in the medical decision-making process, and reducing uncertainty, stress, and anxiety. 81,82 Several ARVs or new ARV drugs are on the market. 83 Emerging long-acting ARVs may have more dosing convenience, tolerability, and cost effectiveness compared with current daily-based oral therapy. 84,85
However, in Massaroni et al's study, 83.7% of PLWHA reported concerns about the possible lower efficacy of the long-acting ARVs. 86 Pharmacists can address PLWHA's concerns about efficacy through education and follow-up. 27 Long-acting ARVs can also lessen the psychological and social burden of daily anti-HIV pill intake for PLWHA, thereby improving adherence and clinical outcomes. Therefore, there is a need for patient-specific information regarding ADRs and several aspects of drug use. This creates a demand for drug information for the HCPs for better prescribing. 87 –89 Considering the positive impact of pharmacist involvement in HIV care based on this review findings, we recommend the policymakers around the globe to include clinical pharmacists in their HIV/AIDS treatment teams for better ARV stewardship.
This study has potential limitations. First, meta-analysis was not conducted due to the methodological heterogeneity related to study designs, PIs, and follow-up durations. Second, included studies were generally of low-to-moderate quality and susceptible to the risk of bias, which means that the positive outcomes reported in this review should be interpreted cautiously. Third, the comparison group, that is, usual medical care mentioned in the included studies, did not define whether pharmacists were involved or not. Therefore, it is difficult to tell whether the pharmacist was involved in usual medical care or not. This is further exacerbated by gaps in reporting for some studies. Lastly, although an exhaustive literature search was performed, there might be unpublished studies that the authors were unaware of.
This review highlights essential directions for future research. First, more studies are needed to understand the nature, type, and mode of pharmacists' intervention to benefit PLWHA. Second, future studies should describe PIs in sufficient detail so that they can be reproduced, and outcomes such as patient satisfaction, medication-related problems, and medication adherence should be measured using validated instruments. Third, more prominent, multi-center RCTs are needed to establish pharmacists' economic, clinical, and humanistic outcomes in HIV/AIDS management. Fourth, most of the studies were from high-income countries, and future research must explore the potential role of pharmacists in HIV/AIDS management in low-middle-income countries. Fifth, more longitudinal studies should be conducted to check the long-term impact of PIs on the QoL and mortality rate of PLWHA.
Finally, no study was conducted at community pharmacies; therefore, future research should explore the community pharmacist role in managing medication-related problems in PLWHA as they are readily available in the community.
The findings of this systematic review demonstrated that pharmacists' involvement in HIV/AIDS management has overall positive effects in reducing ARV-associated medication-related problems, and improving adherence and comorbid conditions. This study provides evidence that dedicated clinical pharmacists with ID experience participating as an MDT member in HIV/AIDS management can improve PLWHA desired health outcomes. More research with better study designs is needed to assess the long-term outcomes of PI in HIV/AIDS management, such as QoL, morbidity, and mortality rate of PLWHA.
Data Availability
The article contains all the important data sets used in this study. If you require additional information, do not hesitate to contact the corresponding author.
Footnotes
Authors' Contributions
Ali Ahmed (A.A.1): Conceptualization, methodology, software, validation, analysis, investigation, resources, data curation, writing —original draft, editing, visualization, and project administration. Maria Tanveer (M.T.): Methodology, data curation, and validation. Juman Abdulelah Dujaili (J.D.): Supervision, methodology, validation, and data curation. Lay Hong Chuah (L.H.C.): Supervision, data curation, and resources. Furqan Khurshid Hashmi (F.K.H.): Supervision and validation. Ahmed Awaisu (A.A.2): Supervision, review, and validation. All authors approved the final version of the article for submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.