
Abstract
HIV and other sexually transmitted infections (STIs) are on the rise nationally and internationally. The coronavirus 2019 (COVID-19) pandemic drove a shift toward telemedicine and prioritization of symptomatic treatment over asymptomatic screening. The impact in safety-net settings, which faced disproportionate baseline STI/HIV rates rooted in structural inequities, and where many patients lack telemedicine resources, is not yet known. This study describes the impact of COVID-19 on STI/HIV testing at an urban safety-net hospital. We used descriptive statistics to compare hospital-wide chlamydia, gonorrhea, syphilis, and HIV testing volume and positivity rates in the following periods: prepandemic (July 1, 2019–February 29, 2020), peak-pandemic (March 1, 2020–May 31, 2020), and postpeak (June 1, 2020–August 31, 2021). STI and HIV test volume dropped sharply in March 2020. STI testing during the peak-pandemic period was 42% of prepandemic baseline (mean 1145 vs. 2738 tests/month) and nadired in April 2020 (766 tests/month). Similarly, peak-pandemic HIV testing was 43% of prepandemic baseline (mean 711 vs. 1635 tests/month) and nadired in April 2020 with 438 tests/month, concentrated in emergency department and inpatient settings. STI and HIV testing rates did not return to baseline for a full year. STI and HIV test positivity rates were higher in the peak-pandemic period compared with the prepandemic baseline. Given the precipitous decline in STI and HIV testing during the pandemic, safety-net settings should develop low-barrier alternatives to traditional office-based testing to mitigate testing gaps, high positivity rates, and associated morbidity.
Introduction
Bacterial sexually transmitted infections (STIs), including chlamydia, gonorrhea, and syphilis, are on the rise in the United States, with record-high rates reported in 2019 for the sixth consecutive year. 1 In addition, HIV outbreaks, fueled by the opioid and polysubstance use epidemics, have occurred in people who inject drugs (PWIDs) and their sexual networks across the country. 2 Early diagnosis is critical in reducing the individual and community impacts of these infections and requires ready access to laboratory testing for symptomatic individuals and robust asymptomatic screening.
The coronavirus 2019 (COVID-19) pandemic demanded unprecedented changes in health care delivery to reduce SARS-CoV-2 transmission, including implementation of physical distancing and a transition to telemedicine. 3 In April 2020, the Centers for Disease Control and Prevention (CDC) recommended the use of telemedicine for STI-related visits and prioritizing symptomatic treatment while deferring routine asymptomatic screening when in-person evaluations were not possible. 4 Decreased access to preventive care visits also threatened services such as HIV pre-exposure prophylaxis (PrEP). 5,6 These changes prompted concern about a potential large-scale drop off in HIV and STI prevention and testing and downstream consequences.
Indeed, early data confirm substantial decreases in HIV and STI testing and case reporting. 7 –9 For example, the number of CDC-funded HIV tests distributed in 2020 were nearly half that of prepandemic levels, particularly affecting priority populations such as Black and Hispanic gay men, other men who have sex with men (MSM), and transgender individuals. 10 Similarly, data from a national reference laboratory demonstrated an April 2020 nadir in gonorrhea and chlamydia testing that was 59% below the prepandemic baseline in women and 63% below baseline in men. 11
It is estimated that >150,000 cases may have been missed nationally during the first 4 months of the pandemic. 11 Decreased testing was not limited to peak pandemic periods, however, and multiple states, including Massachusetts, California, and Oregon, have documented gaps in testing that persisted after the relaxation of the most stringent COVID-19 public health restrictions. 7 –9 Concerningly, decreases in testing coincided with an increase in test positivity rate, indicating the inadequacy of screening. 11
The consequences of inadequate STI and HIV screening may be more profound in already vulnerable communities due to the compounding effects of poverty, structural racism, and stigma. 12 Before the COVID-19 pandemic, Black and Hispanic populations experienced inequitable burdens of new STIs compared with non-Hispanic White peers driven by inequitable access to health care and sexual networks characteristics, and not by differences in sexual behavior. 13 Among Black MSM, decreased access to preventative services due to economic inequities, delayed screening, and higher prevalence sexual networks have been identified as drivers of the rise in syphilis incidence. 14 Further, individuals experiencing poverty and homelessness often lack the resources required to participate in telemedicine. The impact of COVID-19 on STI and HIV screening in safety-net settings remains uncertain.
Boston Medical Center (BMC) is an urban safety-net hospital in Boston, Massachusetts. Suffolk County, where BMC is located, has the highest incidence of chlamydia and infectious syphilis of any county in Massachusetts, and the county incidence of chlamydia, gonorrhea, and infectious syphilis has increased for eight consecutive years. 15 In addition, Suffolk County is one of 57 jurisdictions identified by the CDC as having the highest rates of new HIV infection in the United States and BMC diagnoses more new HIV infections per year than any other health care system in Massachusetts (Johns, October 2, 2020, pers. comm.). 16
Further, Boston has had an ongoing HIV outbreak among PWIDs since late 2018 that has impacted patients with high rates of homelessness, poverty, and substance use disorders. 12,17 –19 Data from the first COVID-19 surge demonstrated an 86% drop in HIV testing in the first 45 days of modified COVID-19 operations at BMC overall and a 92% drop in HIV testing in ambulatory clinics compared with the prior 45-day period. 20
Given rising STI and HIV cases and the significant and inequitable impacts of the COVID-19 pandemic on already marginalized populations, it is critical to understand how the pandemic affected infection screening in safety-net settings. The goal of this study is to describe the impact of COVID-19 on STI and HIV testing and positivity rates at a large urban safety-net hospital in one of the federal Ending the HIV Epidemic priority counties.
Methods
This project took place at BMC, the largest safety-net hospital in New England, which is affiliated with Boston University Chobanian and Avedisian School of Medicine. Since 1988, BMC's Infectious Diseases Program and HIV Prevention Team have delivered comprehensive STD and HIV/AIDS prevention and treatment services to diverse patient populations, including PWID, MSM, people who engage in transactional sex, immigrants, and refugees.
BMC implemented modified COVID-19 operations on March 16, 2020. Operations changes included a significant shift to telemedicine for outpatient visits and limitations on in-person ambulatory visit volume. Based on institutional modified COVID-19 operations, we defined the following study periods: prepandemic (July 1, 2019–February 29, 2020), peak-pandemic (March 1, 2020–May 31, 2020), and postpeak (June 1, 2020–August 31, 2021).
We abstracted data on chlamydia, gonorrhea, syphilis, and HIV testing volume and positivity rates from an existing STI surveillance database, which aggregates hospital-wide test results across all ordering departments, including outpatient clinics, the emergency department, and the inpatient setting, for clinical quality assurance and the identification of candidates for HIV PrEP.
Descriptive statistics were used to characterize testing volume and positivity rates for STI and HIV during each of these periods. This study was undertaken as a quality improvement initiative and, therefore, was not supervised by the Boston University Medical Campus Institutional Review Board.
Results
Testing overall
Bacterial STI (i.e., chlamydia, gonorrhea, and syphilis) and HIV testing declined precipitously at the onset of the COVID-19 pandemic in March 2020 (Figs. 1 and 2).
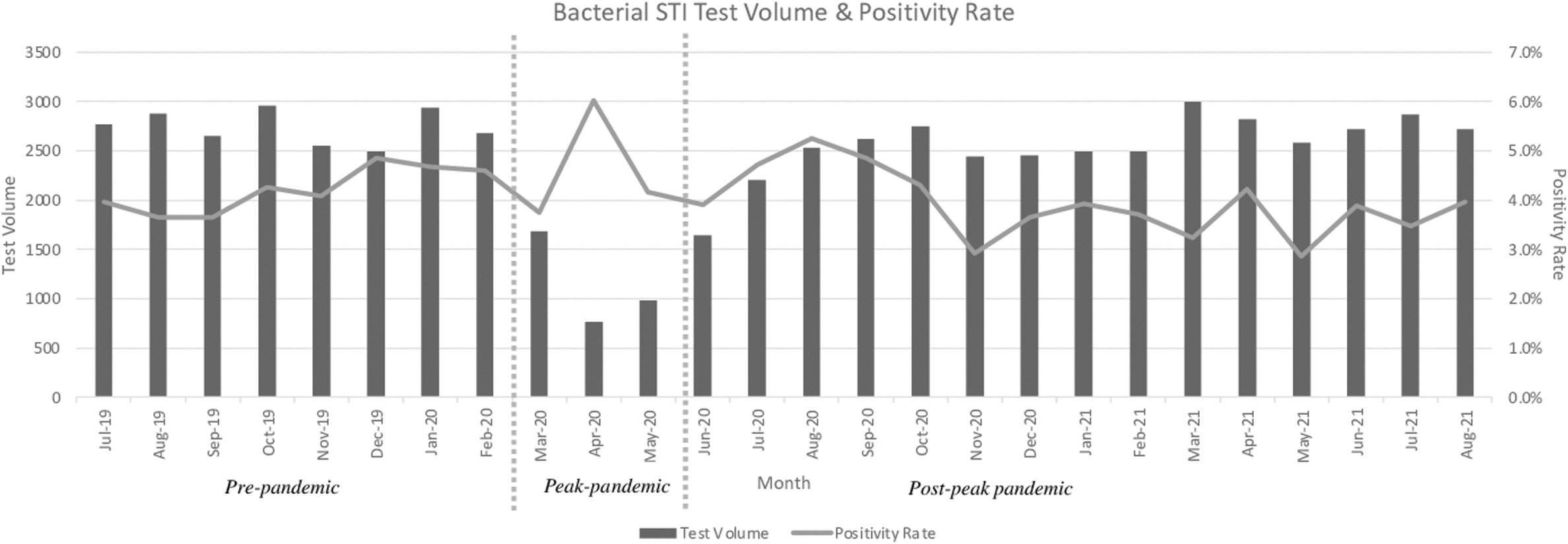
Bacterial STI (i.e., syphilis, gonorrhea, and chlamydia) testing volume and positivity rate at an urban safety-net hospital in Boston, Massachusetts, July 2019–August 2021. STI, sexually transmitted infection.
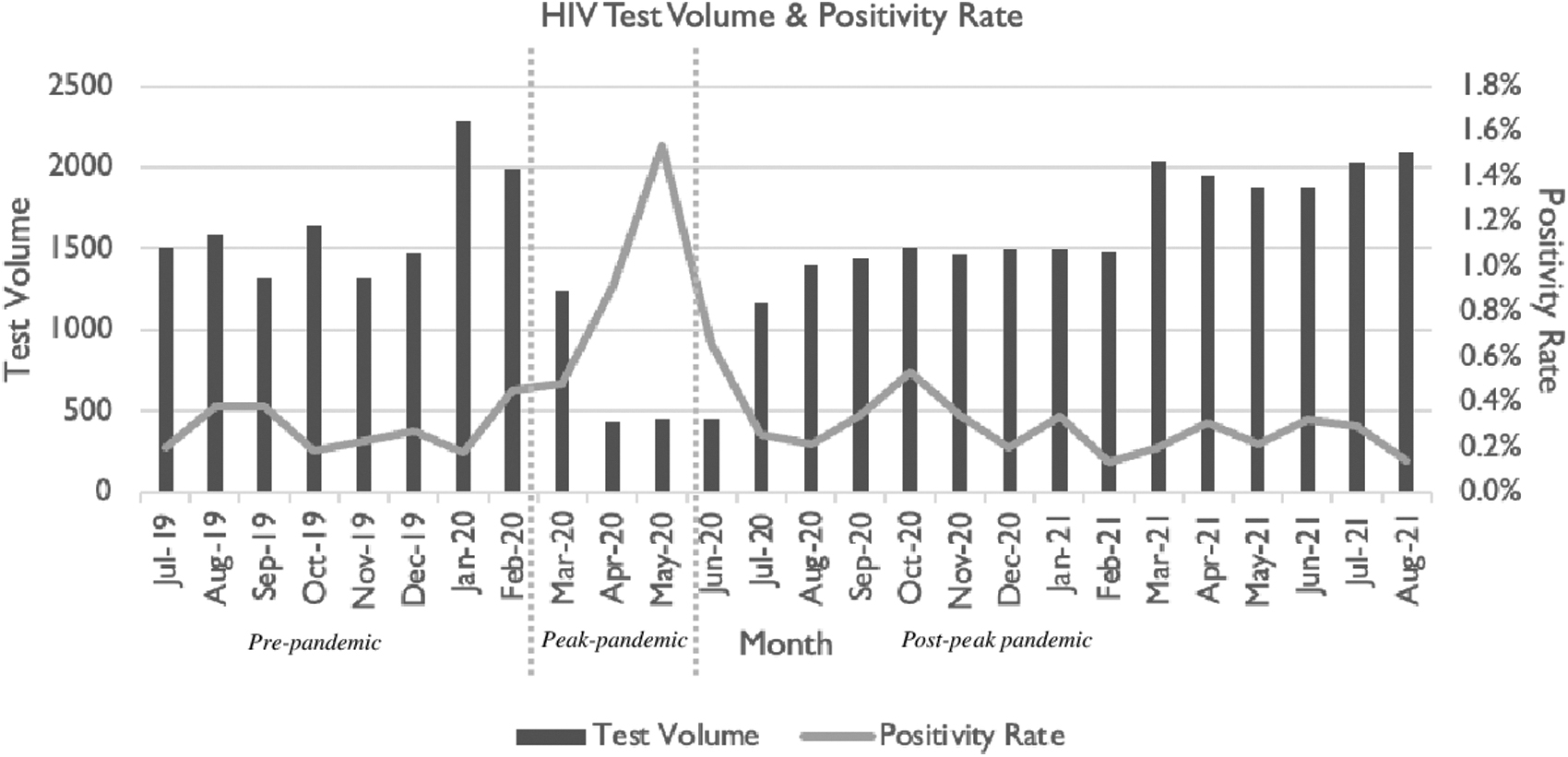
HIV testing volume and positivity rate at an urban safety-net hospital in Boston, Massachusetts, July 2019–August 2021.
Compared with the prepandemic period (mean 2738 total tests ordered/month, inclusive of chlamydia, gonorrhea, syphilis, and HIV), testing decreased by 58% during the peak-pandemic period (mean 1593 tests ordered/month). Testing reached its nadir in April 2020 with 766 tests ordered. Total testing levels did not return to the prepandemic baseline until March 2021.
Ordered tests were also less likely to be completed, which occurs when patients are unable to make it to the laboratory, after the onset of the COVID-19 pandemic. For example, the rate of ordered gonorrhea and chlamydia tests that were not completed increased from a prepandemic baseline of 6.8–10.8% peak-pandemic, a rate that persisted in the postpeak period (10.8%; Supplementary Table S1).
Gonorrhea and chlamydia
The number of gonorrhea (GC) and chlamydia (CT) tests ordered dropped dramatically from a prepandemic mean of 2263 tests/month to a peak-pandemic mean of 913 tests/month, with a nadir of 614 tests in April 2020, representing a 73% decline from baseline (Supplementary Table S1). In the postpeak period overall, GC/CT testing (mean 2017 tests/month) remained 11% below baseline. March 2021 was the first postpeak month where testing volume met or exceeded the prepandemic baseline.
The positivity rate for completed GC/CT tests increased from a prepandemic mean of 5.3–6.3% in the peak-pandemic period. April 2020 had the highest single month positivity rate at 8.2% (Supplementary Table S1).
The drop in GC/CT testing from the prepandemic to the peak-pandemic period was more pronounced for rectal (29.4% baseline), urinary (37.3% baseline), and pharyngeal (37.5% baseline) than vaginal/endocervical sites (42.9% baseline; Supplementary Table S2).
Syphilis
Similar to GC/CT testing, syphilis testing dropped precipitously at the onset of the pandemic from a baseline prepandemic mean of 1186 tests/month to a peak-pandemic mean of 314 tests/month, with a nadir 314 tests in April 2020, representing a 74% decline (Supplementary Table S3). There was no significant difference between the prepandemic and postpeak periods in syphilis testing.
Unlike GC/CT, the syphilis test positivity rate did not increase after the onset of the COVID-19 pandemic. The monthly positivity rate for the prepandemic period was 6.33% compared with 4.91% in the peak-pandemic period and 4.10% in the postpeak period. The proportion of infectious syphilis cases slightly increased during our study period, from 0.21% prepandemic to 0.30% peak-pandemic and 0.34% postpandemic.
Time to treatment
Among all cases of GC, CT, and infectious syphilis, mean time to treatment was similar across the prepandemic (3.98 days), peak-pandemic (4.14 days), and postpeak (3.83 days) periods.
HIV
HIV testing volume, which had a mean of 1641 tests/month prepandemic, dropped to 711 tests/month in the peak-pandemic period with a nadir 438 tests ordered in April 2020, representing a 73% decrease (Fig. 2). In the postpeak period overall, average HIV testing volume was 1585 tests/month, 97% of baseline. However, volume did not consistently return to baseline until March 2021 (Table 1).
HIV Testing Volume, Positivity Rate, and Incidence at an Urban Safety-Net Hospital in Boston, Massachusetts, July 2019–August 2021
HIV incidence (i.e., new diagnoses of HIV) is lower than the test positivity rate due to inadvertent screening in patients with pre-existing HIV infection.
The HIV test positivity rate increased from a prepandemic mean of 1.30–1.76% during the peak-pandemic period, peaking at 2.64% in May 2020 (Table 1).
Discussion
Before the COVID-19 pandemic, CT/GC and syphilis rates were on the rise and many regions of the United States, including Boston, Massachusetts, faced HIV outbreaks. This retrospective study demonstrates that STI and HIV testing volume at an urban safety-net medical center declined precipitously at the onset of the COVID-19 pandemic and did not return to baseline levels for a full calendar year. Increased GC/CT and HIV test positivity rates during the peak-pandemic period further supports the inadequacy of infection screening during this time.
At their nadir in April 2020, GC/CT, syphilis, and HIV testing volume were 73–74% below baseline levels. This drop in HIV testing exceeds the March 2020 HIV testing decline of >50% reported by the CDC in two national commercial laboratories. 10 Further, the overall peak-pandemic drops in STI and HIV testing, which declined by 58% and 56%, respectively, concords with or exceeds decreases in testing reported in other settings. Prior work from the Oregon State Public Health Laboratory demonstrated a 58% reduction in STI testing and a 50% decrease in HIV testing from March to May 2020. 7
The decline in testing observed in our setting was likely driven by public health recommendations designed to reduce COVID-19 transmission, including limitations on in-person visit volume. The height of the pandemic was associated with a decrease in routine visits where asymptomatic screening is often completed, including preventive care visits, elective appointments, and visits for other chronic conditions. 21 Testing of symptomatic patients and, in many cases, presumptive treatment without testing, were prioritized over routine screening. Expedited partner therapy (EPT) may also have been provided more readily than at baseline, although this study was not designed to evaluate trends in EPT prescribing.
Further, the outpatient visits that continued shifted largely to telemedicine. As a safety-net institution serving patients with high social and economic vulnerability, our population likely experienced outsized barriers to engaging in telemedicine, including lack of concrete resources (e.g., telephones and internet) or privacy to engage in these visits. Routine laboratory testing was often deferred to minimize health care contact. When laboratories were ordered during telemedicine visits, the need for a trip to the medical center—separated in space and time form the visit—presented another barrier to STI screening. In our experience, patient fears about coming to the medical center due to the possible risk of COVID-19 exposure played a role in increased noncompletion of ordered tests.
Our findings provide important context for physicians and other clinicians in safety-net and resource rich settings across the globe, who should both anticipate increased STI transmission and maintain a high index of suspicion for complications of untreated STI, including pelvic inflammatory disease, infertility, ectopic pregnancy, and disseminated GC. 22 Decreased testing associated with the COVID-19 pandemic also demands innovation in STI and HIV screening to support systems in “catching up.” For example, electronic medical record templates can be created to help integrate risk assessment and testing systematically into office visits and screening frequency can be adopted to the local context. 20
Community-based outreach can increase access for populations facing specific barriers to engagement, including homelessness, poverty, and criminal legal system involvement, and can help facilitate telemedicine visits. 23 Alternatives to phlebotomy-based HIV testing, including rapid HIV testing, can be provided for patients unwilling or unable to present to a laboratory. 24 Finally, systems can decouple STI and HIV screening from scheduled outpatient medical appointments through routine testing in emergency department (ED) and inpatient settings as well as community-based testing and drop in services that utilize standing orders and incorporate interdisciplinary teams.
Our study has several limitations. First, our retrospective analysis does not permit us to draw causal conclusions explaining the decrease in STI and HIV testing and increase in positivity rates at the onset of the pandemic. We offer the aforementioned possible explanations from our own clinical experience and available literature. Further, we evaluated system-level data on STI and HIV testing volume that was not linked to demographic or clinical variables. We are, therefore, unable to comment on whether certain patient characteristics, including race, ethnicity, gender, sexual orientation, and substance use disorder history, were associated with differential impacts of the COVID-19 pandemic on screening.
Overall, our study reveals a drastic reduction in STI and HIV testing and an increase in test positivity rates at the onset of the pandemic in an urban safety-net hospital and adds to the growing body of data demonstrating diverse and outsized health harms experienced by vulnerable populations during the COVID-19 pandemic. High STI transmission rates portend future infectious disease crises; indeed, the monkeypox virus outbreak of 2022, which occurred subsequent to our study period, further emphasized the vulnerability of current sexual and public health infrastructure, with consequences concentrated in marginalized communities. 25 Results should serve as a call to action for safety-net medical providers to innovate in the delivery of low-barrier STI and HIV screening and for the reinvestment in public health infrastructure.
Footnotes
Authors' Contributions
J.S., G.R.M., and J.L.T. led conceptualization. J.S. led data curation. H.S. led methodology and formal analyses. T.N.L. led writing (original draft) and project administration. J.L.T. provided supervision. All authors contributed to writing (review and editing) and approved the final article.
Author Disclosure Statement
H.S. and G.R.M. are partially funded by a Frontlines of Communities in the United States (FOCUS) grant from Gilead Sciences that supports HIV, hepatitis C virus, and hepatitis B virus screening and linkage to care. Gilead Sciences had no role in the development of this study. Other authors have no conflicts of interest to disclose.
Funding Information
This study was supported by a grant from the Massachusetts Department of Public Health Bureau of Infectious Disease and Laboratory Sciences, Office of HIV/AIDS [INTF4944MM3181926007] (J.S., H.S., G.R.M., and J.L.T.).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.