
Abstract
HIV-associated neurocognitive disorders (HAND) remain a major challenge for people with HIV in the antiretroviral therapy era. Cocaine use may trigger/exacerbate HAND among African American (AA) adults, especially women. Between 2018 and 2019, 922 adults, predominantly AAs, with/without HIV and with/without cocaine use in Baltimore, Maryland, were enrolled in a study investigating the association of HIV and cocaine use with neurocognitive impairment (NCI). Neurocognitive performance was assessed with the NIH Toolbox Cognition Battery (NIHTB-CB). NCI was considered to be present if the fully adjusted standard score for at least two cognitive domains was 1.0 standard deviation below the mean. Although the overall analysis showed HIV and female sex were associated with NCI, the associations were dependent on cocaine use. Neither HIV [adj prevalence ratio (PR): 1.12, confidence interval (95% CI): 0.77–1.64] nor female sex (adj PR: 1.07, 95% CI: 0.71–1.61) was associated with NCI among cocaine nonusers, while both HIV (adj PR: 1.39, 95% CI: 1.06–1.81) and female sex (adj PR: 1.53, 95% CI: 1.18–1.98) were associated with NCI in cocaine users. HIV was associated with two NIHTB-CB measures overall. In addition, HIV was associated with a lower dimensional change card sort score (an executive function measure) in cocaine users and not in nonusers. Cognitive performance was poorer in female than in male cocaine users. The adverse effect of HIV on cognitive performance predominantly affected cocaine users. However, cocaine use may moderate the impact of HIV and female sex on cognitive performance, highlighting the importance of reducing cocaine use in NCI prevention among the AA population.
Introduction
Although successful antiretroviral therapy (ART) has resulted in a significant reduction in HIV-associated dementia, the milder forms of HIV-associated neurocognitive disorders (HAND) remain an important HIV comorbidity, affecting ∼18 − 69% of people living with HIV (PLWH), despite viral suppression with ART. 1,2 Accelerated aging-related brain changes and neurocognitive decline have been observed in PLWH receiving ART and are a major source of concern among over 50% of PLWH in the United States today. 3 –5 Population-based studies of the effect of HIV on neurocognitive decline in the ART era among middle-aged adults, however, and especially among African Americans (AAs), were rarely performed. Abundant evidence suggests that neurocognitive performance is influenced not only by low education attainment and poverty 4,6 but also by substance use. 7 –9
Nevertheless, the findings on the associations between substance use and neurocognitive deficits are not consistent. For example, cocaine is one of the most widely used psychoactive substances. Although the predominant view supports the association between cocaine use and neurocognitive deficits, 10,11 recent evidence does not support the view that chronic cocaine use is associated with broad neurocognitive deficits. 12 Furthermore, whether, and, if so how, cocaine use influences the effect of HIV on neurocognitive performance among AA adults, especially women, is not well characterized.
Between January 2000 and August 2021, this research team recruited and followed ∼1500 adult men and women, most of whom (93%) are AAs from the inner city of Baltimore, thereby establishing the Heart Study in Baltimore. Of these participants, 950 were HIV infected. The purposes of these ongoing studies are to evaluate the effects of HIV, substance use, and other factors on the presence and development of HIV-associated cardiovascular and cognitive comorbidities. Cognitive performance has been evaluated with the NIH Toolbox cognition battery (NIHTB-CB). 13,14 As of December 2019, 922 adults, 42% of whom are women, HIV infected and uninfected, and with or without cocaine use, completed neurocognitive assessment with the NIHTB-CB.
The objectives of this study were (1) to estimate the prevalence of neurocognitive impairment (NCI), based on the NIHTB-CB, according to the revised research criteria for HAND, 15,16 (2) to examine whether and if so to what extent HIV itself is independently associated with cognitive performance deficits, and (3) to explore whether cocaine use modifies the association between HIV and NCI, and the association between female sex and NCI.
Methods
Participants
Between June 2018 and December 2019, 922 adult men and women, predominantly AAs, with and without HIV and with and without psychoactive substance use, from inner city Baltimore, Maryland, were consecutively enrolled in a population-based longitudinal study investigating the effects of HIV, exposure to ART, and cocaine use on HIV-associated cardiovascular and neurological comorbidities. This study is a continuation and an expansion of a 20-year investigation of the effects of HIV, exposure to ART, and cocaine and other psychoactive substances on subclinical coronary artery disease in inner city Baltimore, Maryland, supported by the National Institute on Drug Abuse. The 922 participants are a subset of the population originally recruited. In 2018, HIV-associated neurological comorbidity data collection was added to this study.
The HIV-infected participants were recruited from the Johns Hopkins Bartlett Clinic. The HIV-uninfected participants were recruited from the local community, where most HIV-infected participants reside.
Inclusion criteria were as follows: (1) age ≥18 years; (2) HIV infected and HIV uninfected, which was determined by ELISA and confirmed by Western blot test; and (3) self-reported estimates of duration and frequency of use of psychoactive substances, including cocaine, heroin, tobacco, marijuana, and alcohol.
Use of cocaine was defined as use by any route and duration (year) of >0, while never use of cocaine was defined as duration of cocaine use = 0, and (4) all races, which were self-designated. Exclusion criteria were as follows: (1) clinical evidence of or any history of or current symptoms believed to be related to coronary artery disease; (2) history of or current chronic obstructive pulmonary disease, seizures, traumatic brain injury, delirium, or dementias; (3) pregnancy, (4) child-bearing potential and not using effective birth control measures or the intent to become pregnant during the follow-up period; (5) chronic kidney disease with an estimated glomerular filtration rate of <60 mL/min/1.73 m2; and (6) limitations in activities of daily living.
The Investigational Review Boards at the Johns Hopkins School of Medicine and the University of Maryland School of Medicine approved the study protocol, and all study participants provided written informed consent. All procedures used in this study were in accordance with institutional guidelines, HIPAA, local and federal regulations, and the Declaration of Helsinki.
Interview, medical chart review, physical, and laboratory examination
Study participants underwent a detailed interview to obtain sociodemographic characteristics, medical history, alcohol consumption, psychoactive substance use, cigarette smoking, and prescribed psychotropic medications use. The Zung self-rating depression scale (Zung depression scale) was also obtained. 17,18 Ranges of Zung depression scale for mild, moderate, and severe depressive symptoms are 50–59, 60–69, and 70 and above, respectively. 17 For HIV-infected participants, detailed information about HIV-related risk factors, duration of known HIV, and medications, including ART use, was also collected. A medical chart review was used to confirm the medical history and prescribed medications provided by the study participants. Physical examination was performed and the results, including vital signs, were recorded. Routine clinical laboratory blood chemistry tests were conducted. The following laboratory tests were performed at baseline: total cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), very low-density lipoprotein (VLDL), triglycerides, and fasting glucose.
Neuropsychological performance tests
Neurocognitive performance was assessed with the use of the NIHTB-CB, iOS (iPad) version 1.20.2456 (
In addition to unadjusted and age-adjusted, standard scores, the NIHTB-CB results also provide a fully corrected standard score [with a mean of 50 and standard deviation (SD) of 10], which compares the score of the test-taker to those in the nationally representative normative sample after adjusting for key demographic variables, including age, sex, race, ethnicity, and educational attainment, collected during the NIHTB-CB norming study. 21
Definition of NCI
Fully adjusted T scores (adjusting for age, gender, race, ethnicity, and educational attainment) were used to assess neurocognitive performance. According to the revised research criteria for HAND, 15,16 NCI was considered to be present if the fully adjusted standard score for at least two cognitive domains among language, working memory, executive function, episodic memory, and speed of information processing was 1.0 SD below the mean for the fully adjusted standard test scores. 15,16
Statistical analysis
Statistical analysis was performed with SAS (SAS 9.4; SAS Institute, Cary, NC). All categorical parameters were summarized as proportions and continuous variables as means with SDs. The chi-square test was used to compare the differences for the categorical and dichotomized variables. The t-test was used to compare differences on continuous measures between those with and without CI, as defined using the NIHTB-CB measures. The overall and group-specific prevalence of NCI and corresponding confidence intervals (95% CIs) were calculated.
Since odds ratios may considerably overestimate the strength of associations in cross-sectional studies, prevalence ratios (PRs) derived from Poisson regression models were used to examine the associations between HIV and NCI. 22
To examine whether HIV was independently associated with the presence of NCI, univariate Poisson regression analyses were performed to explore crude associations between NCI and each independent variable and to obtain crude PRs and corresponding 95% CIs and p-values. We also performed multivariate Poisson regression analyses to adjust for potential confounding factors. Continuous confounding factors were first dichotomized using the median split method to prevent residual confounding. 23
The following potential confounding factors were included in multivariate Poisson regression analyses: age, sex, education attainment (<high school vs. otherwise), annual family income (<$20,000 vs. otherwise), marital status (married vs. otherwise), current employment, cigarette smoking (>30 years, the median years vs. otherwise), cocaine use (>7 years, the median, vs. otherwise), alcohol use (>15 years, the median, vs. otherwise), marijuana use (>6 years, the median, vs. otherwise), heroin use (>2 years, the median, vs. otherwise), systolic blood pressure (>130 mmHg), diastolic blood pressure (>75 mmHg), total cholesterol (>180 mg/dL), fasting glucose (>90 mg/dL), VLDL (>20 mg/dL), HDL (>50 mg/dL), triglycerides (>100 mg/dL), and the Zung depression scale (>40, the median, vs. otherwise).
To examine whether cocaine use modified the association between HIV and NCI and the association between female sex and NCI, a stratified Poisson regression analysis was performed according to cocaine use vs. nonuse. A general linear model was used to examine the impact of HIV on NIHTB-CB scores and whether cocaine use influenced the association between HIV and NIHTB-CB scores. The p-values reported are two sided. A p value <0.05 indicated statistical significance.
Results
General characteristics
The demographic, behavioral, clinical, and cognitive characteristics of 922 participants by the presence of NCI are presented in Table 1.
Characteristics of 922 Adult Study Participants in Baltimore, Maryland, by the Presence of Neurocognitive Impairment
NCI was defined according to the Frascati Conference criteria for HIV-associated neurocognitive disorders. 15,16 Data are n (%) or mean (SD).
Age, age at interview (years); Glucose, fasting glucose; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; NCI, neurocognitive impairment; SD, standard deviation; VLDL, very low-density lipoprotein; Zung depression scale, Zung self-rating depression scale.
NCI was significantly more prevalent in women than men (p < 0.0001), in those with < a high school education than otherwise (p < 0.0001), in those with annual household income <$20,000 than otherwise (p = 0.0008), in those who were currently unemployed than otherwise (p = <0.0001), in those with a higher Zung depression score than otherwise (p < 0.0001), and in those with HIV than otherwise (p = 0.02) (Table 1).
Prevalence of NCI
The overall prevalence of NCI was 28.5% (95% CI: 25.6 − 31.6). The prevalence of NCI in females (36.7%, 95% CI: 31.9 − 41.7) was significantly higher than that in males (22.6%, 95% CI: 19.1 − 26.4) (p < 0.0001), in those with < a high school education (41.3%, 95% CI: 36.2 − 46.5) was significantly higher than that in those with ≥ a high school education (20.1%, 95% CI: 16.9 − 23.7) (p < 0.0001), in those with annual household income <$20,000 (31.9%, 95% CI: 28.3 − 35.6) was significantly higher than that in those with annual household income ≥$20,000 (20.7%, 95% CI: 16.0 − 25.9) (p = 0.0005), in those who were unemployed (31.6%, 95% CI: 28.3 − 35.1) was significantly higher than that in those were employed (15.7%, 95% CI: 10.7 − 21.9) (p < 0.0001), in those with a Zung depression scale >40 (the median) (39.3%, 95% CI: 34.2–44.6) was significantly higher than that in those with a Zung depression scale ≤40 (21.3%, 95% CI: 18.4 − 25.4) (p < 0.0001), and in HIV infected (31.4%, 95% CI: 27.5 − 35.5) was significantly higher than that among the HIV uninfected (24.4%, 95% CI: 20.2 − 29.1) (p = 0.02) (Fig. 1).
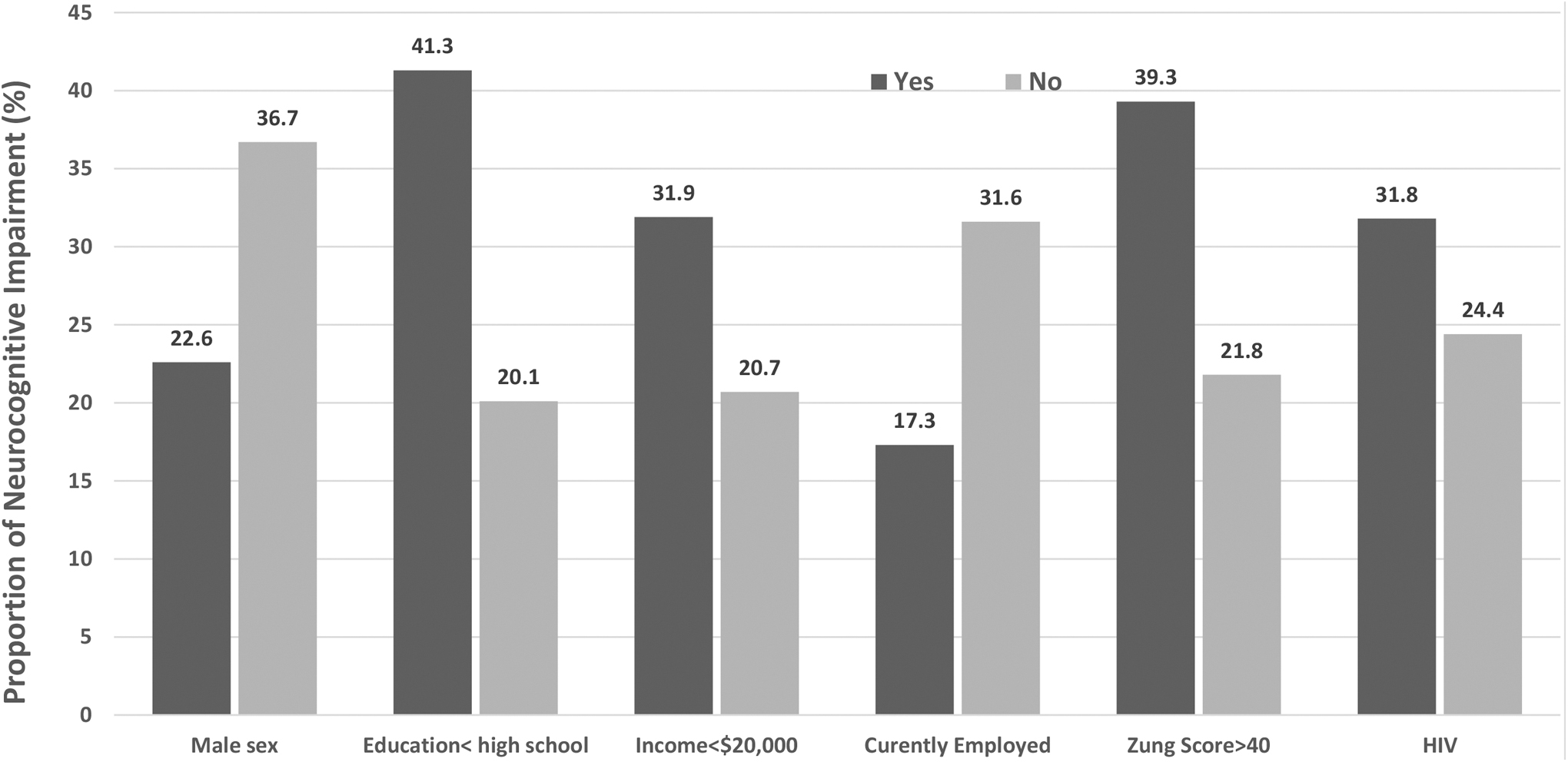
Prevalence of NCI by Associated Factors. The prevalence of NCI in women (36.7%, 95% CI: 31.9 − 41.7) was significantly higher than that in men (22.6%, 95% CI: 19.1 − 26.4) (p < 0.0001), in those with < a high school education (41.3%, 95% CI: 36.2 − 46.5) was significantly higher than that in those with ≥ a high school education (20.1%, 95% CI: 16.9 − 23.7) (p < 0.0001), in those with annual household income <$20,000 (31.9%, 95% CI: 28.3 − 35.6) was significantly higher than that in those with annual household income ≥$20,000 (20.7%, 95% CI: 16.0 − 25.9) (p = 0.0005), in those who were unemployed (31.6%, 95% CI: 28.3 − 35.1) was significantly higher than that in those were employed (15.7%, 95% CI: 10.7 − 21.9) (p < 0.0001), in those with a higher Zung depression scale >40 (the median) (39.3%, 95% CI: 34.2–44.6) was significantly higher than that in those with a Zung depression scale ≤40 (21.3%, 95% CI: 18.4 − 25.4) (p < 0.0001), and in HIV infected (31.4%, 95% CI: 27.5 − 35.5) was significantly higher than that among the HIV uninfected (24.4%, 95% CI: 20.2 − 29.1) (p = 0.02). CI, confidence interval; NCI, neurocognitive impairment.
The prevalence of NCI in those ≤55 years of age (the median) (28.0%, 95% CI: 23.8 − 32.5) was not significantly different from that in those >55 years of age (29.1%, 95% CI: 25.0 − 32.3) (p = 0.73).
Factors associated with the presence of NCI
Multivariate Poisson regression analysis indicated that female sex (adj PR: 1.39, 95% CI: 1.12–1.72, p < 0.0001), less than a high school education (adj PR: 1.78, 95% CI: 1.42–2.23, p < 0.0001), current employment (adj PR: 0.58, 95% CI: 0.39–0.87, p = 0.008), Zung depression scale >40 (adj PR: 1.39, 95% CI: 1.14–1.70, p = 0.001), and HIV (adj PR: 1.31, 95% CI: 1.06–1.62, p = 0.01) were independently associated with a higher prevalence of NCI, while current employment (adj PR: 0.58, 95% CI: 0.39–0.87, p = 0.008) was associated with a lower prevalence of NCI. Cigarette smoking, alcohol use, cocaine use, heroin use and marijuana use were not associated with NCI (Table 2).
Factors Associated with the Presence of Neurocognitive Impairment
NCI was defined according to the Frascati Conference criteria for HIV-associated neurocognitive disorders. 15,16
Age, age at interview (years); BP, blood pressure; Glucose, fasting glucose; HDL-C, high-density lipoprotein cholesterol; NCI, neurocognitive impairment; PR, prevalence ratio; VLDL, very low-density lipoprotein; Zung depression scale, Zung self-rating depression scale.
The associations between HIV and NCI by cocaine use
Among cocaine nonusers, multivariate Poisson regression analysis indicated that HIV was not independently associated with NCI (adj PR: 1.07, 95% CI: 0.73–1.57, p = 0.71). However, among cocaine users, multivariate Poisson regression analysis indicated that HIV was independently associated with NCI (adj PR: 1.39, 95% CI: 1.06–1.81, p = 0.015) (Table 3).
Factors Associated with the Presence of Neurocognitive Impairment by Cocaine Use Versus Nonuse
NCI was defined according to the Frascati Conference criteria for HIV-associated neurocognitive disorders. 15,16
Age, age at interview (years); BP, blood pressure; Glucose, fasting glucose; HDL-C, high-density lipoprotein cholesterol; NCI, neurocognitive impairment; PR, prevalence ratio; VLDL, very low-density lipoprotein; Zung depression scale, Zung self-rating depression scale.
The associations between female sex and NCI by cocaine use
Among cocaine nonusers, multivariate Poisson regression analysis indicated that female sex was not independently associated with NCI (adj PR: 1.07, 95% CI: 0.71–1.51, p = 0.76). However, among cocaine users, multivariate Poisson regression analysis indicated that female sex was independently associated with NCI (adj PR: 1.53, 95% CI: 1.18–1.98, p = 0.001) (Table 3).
The adjusted associations of HIV with the NIHTB-CB, overall and by cocaine use
Based on the overall regression analysis, HIV was significantly associated with worse measures in the domains of language, information processing speed, episodic memory, and executive function. Among cocaine nonusers, HIV was associated with a worse oral reading recognition speed score in the domain of language, and a worse picture sequence memory score in the domain of episodic memory. Among cocaine users, HIV was associated with a worse oral reading recognition score in the domain of language, a worse picture sequence memory score in the domain of episodic memory, and a worse dimensional change cart sort score in the domain of executive function (Table 4).
Adjusted Associations Between the NIH Toolbox Cognition Battery and HIV, Overall and by Cocaine Use Status
Adjusted for age, sex, low education attainment (<high school), Annual family annual income <$20,000, being married, cigarette smoking >30 years, alcohol use >15 years, marijuana use >6 years, heroin use >2 years, systolic blood pressure >30 mmHg, diastolic blood pressure >75 mmHg, cholesterol >180 mg/dL, glucose >90 mg/dL, very low-density lipoprotein >20 mg/dL, high-density lipoprotein >50 mg/dL, and Zung depression score >40.
The adjusted associations of female sex with the NIHTB-CB, overall and by cocaine use
Based on the overall regression analysis, females had significantly worse measures in the domains of language, working memory, and executive function compared to males. Among cocaine nonusers, females had significantly better list sorting working memory score in the domain of working memory than males. Among cocaine users, females had significantly worse picture vocabulary score in the language domain, and a worse Flanker inhibitory control and attention score in the domain of executive function than males (Table 5).
Adjusted Associations Between the NIH Toolbox Cognition Battery and Female Sex, Overall and by Cocaine Use Status
Adjusted for age, HIV, low education attainment (<high school), Annual family annual income <$20,000, being married, cigarette smoking >30 years, alcohol use >15 years, marijuana use >6 years, heroin use >2 years, systolic blood pressure >130 mmHg, diastolic blood pressure >75 mmHg, cholesterol >180 mg/dL, glucose >90 mg/dL, very low-density lipoprotein >20 mg/dL, high-density lipoprotein >50 mg/dL, and Zung depression score >40.
Discussion
The findings of this study demonstrated that in the ART era among a predominantly AA population, (1) HIV and female sex were independently associated with the presence of cognitive impairment overall; however, the associations were dependent on cocaine use, (2) cocaine use modified the association between HIV and NCI, (3) female sex was independently associated with the presence of cognitive impairment overall, (4) cocaine use modified the association between female sex and NCI, (5) HIV negatively affected cognitive scores in the domains of language, information processing speed, episodic memory and executive function overall; however, HIV was independently associated with worse executive function in cocaine users, but not in cocaine nonusers, and (6) poorer cognitive performance in the domains of language and executive function was identified in female cocaine users than their male counterparts.
This study was performed in a predominantly AA population living in inner city Baltimore and disproportionately impacted by HIV and cocaine use. The overall prevalence of NCI in this population was 28.5% (95% CI: 25.6 − 31.6). To our best knowledge, the prevalence of NCI in a similar AA population has not been reported. The Baltimore Study of Black Aging recruited participants living in senior housing facilities in Baltimore and reported that the prevalence of minor cognitive impairment based on the Mini-Mental State Examination in this population was 22% among urban-dwelling AAs between 55 and 90 years years of age. 24 However, these two study populations are quite different with an expected significantly lower prevalence of HIV and cocaine use and an older age in the latter cohort.
The overall analysis shows that HIV was independently associated with the presence of NCI. This finding is consistent with other published data. 1,2 The overall analysis also shows that female sex was independently associated with the presence of NCI. Sex differences in cognitive abilities have been investigated and suggest that men perform better on spatial memory, while women perform better on verbal memory testing. 25
However, our data suggest that the association of HIV with NCI is largely dependent on cocaine use. According to the stratified analyses shown in Table 3, the association between HIV and NCI was most apparent among cocaine users. For cocaine never users, the adverse impact of HIV on cognitive performance was not observed in this study. This finding suggests that cocaine use may exacerbate the effect of HIV on cognitive performance among a predominantly AA population disproportionately impacted by HIV and cocaine use. The effect of cocaine on HIV-associated neurocognitive comorbidities has not been thoroughly investigated since most research to date has focused on the impacts of viral and antiviral actors. 6
We previously reported that cocaine use may modify the associations between duration of ART and subclinical coronary atherosclerosis, 26 between HIV/ART and myocardial and hepatic steatosis, 27 and between HIV and telomere shortening. 28 The mechanisms by which cocaine use modifies the association between HIV and NCI are not completely known. Cocaine intake is consistently associated with an increase in the number and upregulation of several neuroinflammatory markers in both human and animal studies. 28,29 Neuroinflammation is a common feature of virtually every central nervous system disease and is increasingly recognized as a potential mediator of NCIs. 30
The data in Table 3 also indicate that the association between female sex and NCI was less among cocaine nonusers. It has been reported that females may be more likely to develop cocaine use disorder compared to males, 31 and progress from reactional use to pathological use faster than do males. 32
Although several studies examined whether women were more vulnerable to HIV-related cognitive dysfunction than were men, they reported inconsistent findings regarding the existence, magnitude, and pattern of sex differences, largely due to small sample sizes. Recently, two large investigations have been conducted to examine sex differences in HAND. The first study performed longitudinal analyses on data combined from two large prospective studies of The Women's Interagency HIV Study and Multicenter AIDS Cohort Study.
The findings of this study showed that women with HIV had a higher probability of NCI compared to men with HIV, and that sex differences were constant over time. The investigators concluded that cognitive disadvantages were more pronounced in HIV-infected women than in HIV-infected men However, this finding is based on a secondary data analysis, and sex differences in verbal learning and memory were not compared. 33 The second investigation studied 1361 HIV-infected participants, including 294 women. HAND was more prevalent in women (52%) than in men (41%); however, the difference was eliminated after adjustment for reading level. The study concluded that women, particularly AA women, were most at-risk for HAND, and that the higher rates of HIV-associated NCI in women than in men may reflect differences in educational quality. 34
A recently published large study reported that HIV-related internalized stigma may be negatively associated with neurocognitive functioning for women with HIV, and significant negative associations between internalized stigma and specific neurocognitive domains such as executive functioning, psychomotor speed, attention, learning, memory, motor, and verbal skills. 35 Since brain MRI may detect signs of cognitive decline earlier than symptoms appear, 36 –39 MRI assessments may provide further insights into the pathways explaining the relationship between internalized stigma and neurocognition.
Further studies are needed to clarify the responsible mechanism.
Depression, as screened for by the Zung rating scale, was increased in this HIV population as has been shown in other studies in populations with HIV. 40 There are numerous studies suggesting that depression is linked to increased inflammation in many disease states. 41 The presence of depression has been shown to impair cognition and exacerbate cognitive impairment, and thus depression likely furthers the cognitive deficit burden in our study population. It is also worth noting that depression is a risk factor for cocaine use and that depression is worsened by cocaine use, amplifying the effects of depression in this population.
Furthermore, the study results revealed that low educational attainment was independently associated with NCI in this population. Nearly 40% of study participants had less than a high-school education. Educational attainment is often regarded as a proxy for cognitive reserve in older adults. 42 Cognitive reserve refers to the brain's ability to make flexible and efficient use of cognitive networks (networks of neuron-to-neuron connections), which enable a person to continue to conduct cognitive tasks, despite brain changes. 43 –47 The concept that additional years of education builds more cognitive reserve is also supported by reports that those with more years of formal education are at lower risk for Alzheimer's disease and other dementias than are those with fewer years of formal education.44.45–47
This study also has several important limitations: (1) this investigation is a cross-sectional study and although we explored whether HIV was associated with the presence of NCI, we had no knowledge as to whether or not NCI was present before HIV. Longitudinal studies are needed to address this important issue, (2) our study was conducted in an inner-city AA population and substance use is highly prevalent in this AA population. The results derived from this sample, therefore, may not be generalizable to other populations, (3) fully adjusted T scores (adjusting for age, gender, race, ethnicity, and educational attainment) were used to assess neurocognitive performance.
Thus, the association of age with NCI may not be assessed from this study, and (4) NCI was considered to be present if the fully adjusted standard score for at least two cognitive domains among language, working memory, executive function, episodic memory, and speed of information processing was 1.0 SD below the means for the fully adjusted standard test score. Although this definition is well accepted, it may not be used to detect early cognitive decline for the purpose of early prevention and intervention among AA population.
Conclusions
Despite the limitations of this investigation, our findings have important implications for the prevention of HIV-associated neurocognitive comorbidities, especially among AAs. This study indicated that cocaine use, as an effect modifier, may trigger and/or exacerbate NCI among adults with HIV and/or women. Specifically, the findings of this study reveal that (1) although HIV was significantly associated with NCI overall in this low socioeconomic predominantly AA population, there was little appreciable association between HIV and NCI among those with only limited exposure to cocaine, and (2) although female sex was significantly associated with NCI among this population, females with limited or no exposure to cocaine were also not observed to be more vulnerable to NCI than were males. Longitudinal studies are needed to verify these findings.
Footnotes
Acknowledgments
We thank all the participants for their participation and contribution.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Research reported in this publication was supported by grants from the US National Institute on Drug Abuse, National Institutes of Health (NIH R01DA12777, R01DA15020, R01DA25524, R01DA035632, R21DA048780, and U01DA040325).