
Abstract
We conducted a web-based survey targeting physicians in specialties of treating sexually transmitted infection (STI) and/or human immunodeficiency virus (HIV) patients to understand the current STI/HIV care practices and their acceptability of and barriers to the prescription of pre-exposure prophylaxis (PrEP) in Japan. A descriptive analysis was used to summarize survey responses. Univariate and multivariable logistic regression were performed to identify factors associated with willingness to prescribe PrEP. Of 316 survey respondents, 57 were specialized in HIV, 90 STI/Urology/Proctology, 55 Obstetrics/Gynecology, and 114 General Practice/Internal Medicine/Dermatology. Proportion of HIV-specialized physicians who interview the patients about risk behaviors tended to be higher than other physician groups (84.2% vs. 54.8%, 47.3%, and 50.9%, respectively), and 53 − 75% of non-HIV-specialized physicians reported that they were incapable of making decisions on HIV medications. Higher PrEP knowledge enhanced the willingness to recommend and prescribe PrEP drugs (odds ratio: 2.31, 95% confidence interval: 1.30–4.10, p = 0.0044), and 45.4% physicians with no PrEP knowledge raised the concern of incapability to respond and manage when an individual is infected with HIV. Educational opportunities on management and prevention measures for both STI and HIV may encourage non-HIV-specialized physicians to be involved in HIV care and to enhance initiation of HIV tests and adoption of PrEP.
Introduction
In 2020, there were 37.7 million people globally living with human immunodeficiency virus (HIV), of whom 1.5 million were newly infected and 680,000 died due to acquired immunodeficiency syndrome (AIDS)-related illnesses. 1 In Japan, over 30,000 people have been diagnosed with HIV, and according to the National AIDS Surveillance Committee's annual report, 1236 new HIV/AIDS cases were reported in 2019, of which 333 (26.9%) were those diagnosed after the onset of AIDS. 2 A study conducted to estimate the HIV care cascade in 2015 in Japan revealed that 85.6% of people living with HIV (PLWH) had received an HIV-positive diagnosis, indicating it had not achieved the first 90 of the “90–90–90 targets” set by the Joint United Nations Program on HIV/AIDS (UNAIDS) for the year 2020. 3,4 Early diagnosis and treatment result in better outcomes; however, these results indicate that a substantial number of PLWH remain undiagnosed and are unaware of their infection status. Therefore, Japan needs a strategy to promote HIV testing for early diagnosis.
In general, the majority of HIV tests in Japan are provided at public health centers and in clinics (facility-based testing). 5 Free, anonymous testing conducted in municipal health care centers identifies ∼45% of new HIV diagnoses. The remaining new HIV/AIDS cases are diagnosed and reported through paid voluntary testing or through usual medical practice in clinics and hospitals. 3 Newly identified HIV-positive individuals are referred to nearby “AIDS Core Hospitals,” which are hospitals with HIV-specialized physicians designated by the Ministry of Health, Labor and Welfare. As for individuals with symptoms of suspected sexually transmitted infections (STIs), consultation with specialists at nearby clinics according to their symptoms, such as dermatology for skin symptoms, urology for men and gynecology for women if their symptoms appear in the pubic area, and STI screening tests, are provided accordingly. Even when patients present to the hospital for an initial consultation related to STIs, clinicians may overlook the early signs of HIV infection.
High-risk sexual behaviors, such as anal, vaginal, and oral sex without a condom, multiple sex partners, anonymous sex partners, and sex under the influence of drugs and alcohol, can increase the risk of both STIs and HIV. 6 Machine learning models indicate that STI symptoms, past syphilis infection, age, and sexual behaviors associated with the risk of HIV infection are the most common predictors of STI/HIV diagnosis. 7 Further, a recent study showed a higher incidence of syphilis in HIV-infected men who have sex with men (MSM) in an urban HIV clinic in Tokyo. 8 In contrast, STI-infected individuals are at an increased risk of acquiring HIV. 9 Also, MSM with rectal STIs and men diagnosed with syphilis have a higher incidence of HIV. 10,11 In Japan, most patients with STIs are not being appropriately tested for HIV infection. 12,13 Therefore, there is an immediate need to promote HIV testing programs for high-risk groups—including MSM, sex workers, injection drug users, and STI-infected individuals.
The Centers for Disease Control and Prevention (CDC) guidelines recommend routine HIV testing for all people seeking STI evaluation, regardless of any specific patient-reported behavioral risks for HIV. Furthermore, people at higher risk for HIV infection, including sexually active gays, bisexuals, and other MSM, should be screened for HIV at least annually. 14,15 Yet, a database study conducted in Japan revealed that among 100 individuals diagnosed with syphilis before their HIV diagnosis, only 17% had received HIV testing suggesting that interventions to prevent missed opportunities for HIV screening are needed. 13,16,17
Early diagnosis, immediate treatment, and pre-exposure prophylaxis (PrEP) are a few important strategies to counter the HIV/AIDS epidemic. 18 Several studies have shown the effectiveness of PrEP in mitigating HIV transmission. 19 –22 In a multinational randomized placebo-controlled study, once-daily oral antiretroviral taken as PrEP resulted in a 44% reduction in HIV incidence compared with placebo. 23 In Australia, there has been a 25.1% decline in HIV diagnoses in MSM and a 35.1% decline in new HIV infections, indicating the effectiveness of PrEP at the population level in the real-world setting. 24 As such, implementation of PrEP is expected to play an important role in reducing the number of new HIV infections in Japan.
For the successful implementation of PrEP, the health care system must include trained PrEP prescribers as well as support services, such as facilities and physicians, who can provide follow-up exams with regular HIV testing for the monitoring and evaluation of PrEP users. Raising social awareness about HIV prevention may help to address differences in perceptions about PrEP among Japanese people, including medical professionals. 25,26
Since PrEP is assumed and expected to be prescribed at the clinics if approved in Japan, there is a need to understand health care professionals' (HCPs') familiarity with managing HIV infections, the depth of their PrEP knowledge, and their willingness to prescribe PrEP drugs.
The primary objectives of this study were to understand current STI and HIV practices for the early diagnosis of HIV in Japan, and to understand physician awareness, willingness, and barriers to implementing PrEP in Japan. The results will enable health care providers and other stakeholders to identify strategies for the successful implementation of PrEP and the effective prevention of further STI/HIV infections.
Methods
Study design
This is a noninterventional, cross-sectional study that involved the collection of data through a web-based survey (Nikkei BP panel, NBP) conducted in February 2021. The survey questionnaire was created based on the key areas of uncertainty, and consisted of 6 sections with 8 screening questions and 33 main survey questions covering details related to HIV/STI screening and diagnosis, HIV treatment, care, and management, perceptions, and knowledge of PrEP in addition to participant attributes. The survey consisted of questions in Japanese, and the outcomes from the main survey questions were analyzed based on the physician background information obtained from the screening questions on clinical practice and attribution questions.
Study population
The target population included physicians selected through the NBP panel, which is used for online marketing purposes and has been widely used for market research and other survey activities among physicians. The survey was sent to ∼6000 targeted physicians in specialties that have the possibility of treating patients with STI/HIV. Informed consent was obtained electronically from 888 physicians; a written consent form was shown online, and those who read and agreed to the consent statement were able to start the screening questionnaire by clicking “Yes, I agree” button and downloading the informed consent form. Those who satisfied the inclusion/exclusion criteria determined from the screening questionnaire were recruited, were able to move on to the main survey, and grouped based on their practice for the study as follows:
Group A, either infectious disease/hematology physicians or board-certified physicians of the Japanese Society of AIDS Research treating 10 or more PLWH within the past year at AIDS core hospitals with 20 beds or more; Group B, physicians working at STI/urology/proctology; Group C, physicians working at obstetrics and gynecology; Group D, physicians working at dermatology/internal medicine clinics.
The survey responses were compared and analyzed across these four groups of physicians.
Statistical methods
A convenient and adequate physician sample size was included to generate descriptive data. However, the study did not intend to test any statistical hypothesis. Hence, no power calculations were required. As of September 2019, there were 219 physicians registered as board-certified fellows and 113 physicians registered as trainers by the Japanese Society for AIDS Research. 27,28 Also, as of October 2020, 1554 physicians were registered as specialists in infectious diseases by the Japanese Association for Infectious Diseases. 29 Considering these numbers, we estimated that around 300 physicians would be a sufficient sample size to capture Japanese physicians' perceptions regarding STI and HIV treatment.
A descriptive analysis was carried out for all physicians included in the study. Physician characteristics and perceptions/management/challenges related to STI/HIV, including PrEP, were stratified by four groups (A–D) spanning the four working medical departments described above. Categorical variables were summarized as frequencies and percentages of the study population, and continuous variables were reported by mean and standard deviation. Wherever justified, nonparametric data were summarized as median and 25% and 75% quartile range.
Knowledge of PrEP was measured from the YES or NO responses to the following three survey questions: (A) Did you know PrEP is a preventive measure that reduces the risk of HIV infection in people at high risk by taking anti-HIV drugs before they are likely to be exposed to HIV? (B) Did you know the US CDC guidelines recommend PrEP use in sexually active MSM who are at high risk for HIV infection? and (C) Did you know that the US CDC guidelines recommend regular HIV tests due to the concern of drug resistance in people infected with HIV while taking PrEP? Based on the responses to the above questions, physicians were segregated into three PrEP knowledge groups for further analysis: “High,” physicians who answered “yes” to all three questions, “Partial,” physicians who answered “yes” to one to two questions, and “No,” physicians who answered “no” to all three questions.
Logistic analysis was conducted to assess the association between willingness toward recommending and prescribing PrEP and physician characteristics, such as gender, age, practice location, specialty, and professional experience as well as knowledge of PrEP, which was defined as physicians who knew the first question (A) regarding PrEP indicated above. For multivariable analysis, all covariates were simultaneously assessed, as done in an earlier Canadian study where a multivariable logistic regression model was used to identify associations between responding physician characteristics and willingness to prescribe PrEP. 30
Results
Demographic characteristics of survey respondents
A total of 316 survey responses from 4 groups (A through D) of physicians, as described in Materials and Methods section, were collected, consisting of 57 physicians in Group A, 90 in Group B, 55 in Group C, and 114 in Group D. Table 1 summarizes the demographic and clinical attributes of the respondents. Among the respondents, 88.3% (279/316) were men, and 63% (199/316) were over 50 years of age. Regarding age distribution among four physician groups, 77.2% of Group A physicians were in their 40s and younger, whereas the other groups tended to be older, with 75.6% in Group B, 76.4% in Group C, and 66.7% in Group D in their 50s and above. Regarding practice location, 44.6% (141/316) of physicians worked in rural areas, whereas 28.2% (89/316) worked in metropolitan cities. Group A included more physicians who practiced in large cities with populations of >2 million compared with the other groups. Only 13.9% (44/316) of the responding physicians, all from Group A, were certified physicians and supervising physicians of the Japanese Society for AIDS Research.
Demographics and Clinical Attributes of Survey Respondents
Metropolitan city (Tokyo, Osaka, Yokohama, Nagoya) with population of ≥2 million inhabitants.
Ordinance-designated city with a population of >0.5 million to 2 million inhabitants.
Rural areas.
AIDS, acquired immunodeficiency syndrome; ART, antiretroviral therapy; DERM, dermatology; GIM, general internal medicine; GP, general practitioner; GYN, gynecology; HIV, human immunodeficiency virus; MSM, men who have sex with men; OB, obstetrics; STI, sexually transmitted infection.
Clinical practice characteristics of survey respondents
Physicians' characteristics, as well as the volume of patient visits, varied substantially from Group A to D (Table 1). Physicians in Group A had a fewer median patient visits per month [200, interquartile range (IQR): 100–400], but saw a greater median number of MSM patients each month (20, IQR: 10–48.8) compared with Groups B, C, and D physicians (Table 1). Overall, physicians across all cohorts screened the median of 30 patients for STIs (IQR: 5–100) and 5 patients for HIV (IQR: 0–30) within the last year, with the highest median number of STI and HIV screening tests given by OB/GYN physicians in Group C (100, IQR: 45.5–375) and Group A physicians (35, IQR: 10–90), respectively. Furthermore, the median number of individuals whose HIV screening tests came back positive was the highest for Group A physicians (5, IQR: 2–15). Across all groups, the number of screening tests for STIs other than HIV provided in the past year included genital chlamydia infections (median: 12, IQR: 1–50), syphilis (median: 10, IQR: 2–30), and gonorrhea (median: 10, IQR: 0–39.5) (Table 1).
Current practices and challenges in STI/HIV care
Examination of patients with STI/HIV
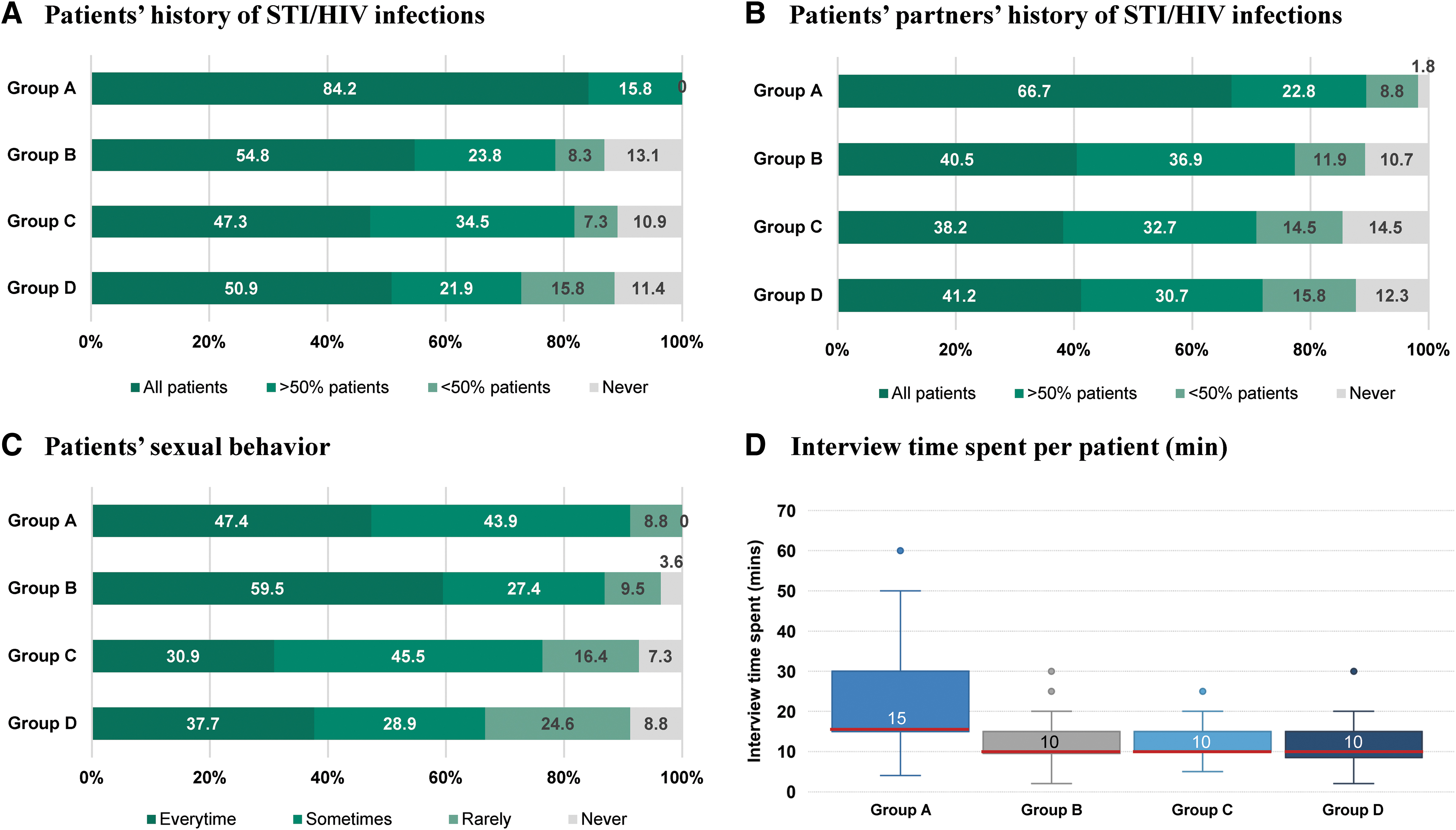
Proportions of physicians who check with all patients on the history of STI and/or HIV infection of the patients and their partners were 84.2% and 66.7%, respectively, in Group A; 54.8% and 40.5% in Group B; 47.3% and 38.2% in Group C; and 50.9% and 41.2% in Group D (Fig. 1A, B). In addition, a majority of physicians interviewed patients about their sexual behavior either at every visit or sometimes, while the proportion of physicians who never sought this information ranged from 0% in Group A to 8.8% in Group D (Fig. 1C). Distribution of physicians in interviewing other risk behaviors of STI/HIV is shown in Fig. 2. Group A physicians spent more time consulting with each patient (median: 15 min, IQR: 15–30) compared with Group B (median: 10 min, IQR: 9.5–15), Group C (median: 10 min, IQR: 10–15), and Group D physicians (median: 10 min, IQR: 8.5–15) (Fig. 1D).
Proportion of physicians among four physician groups who check
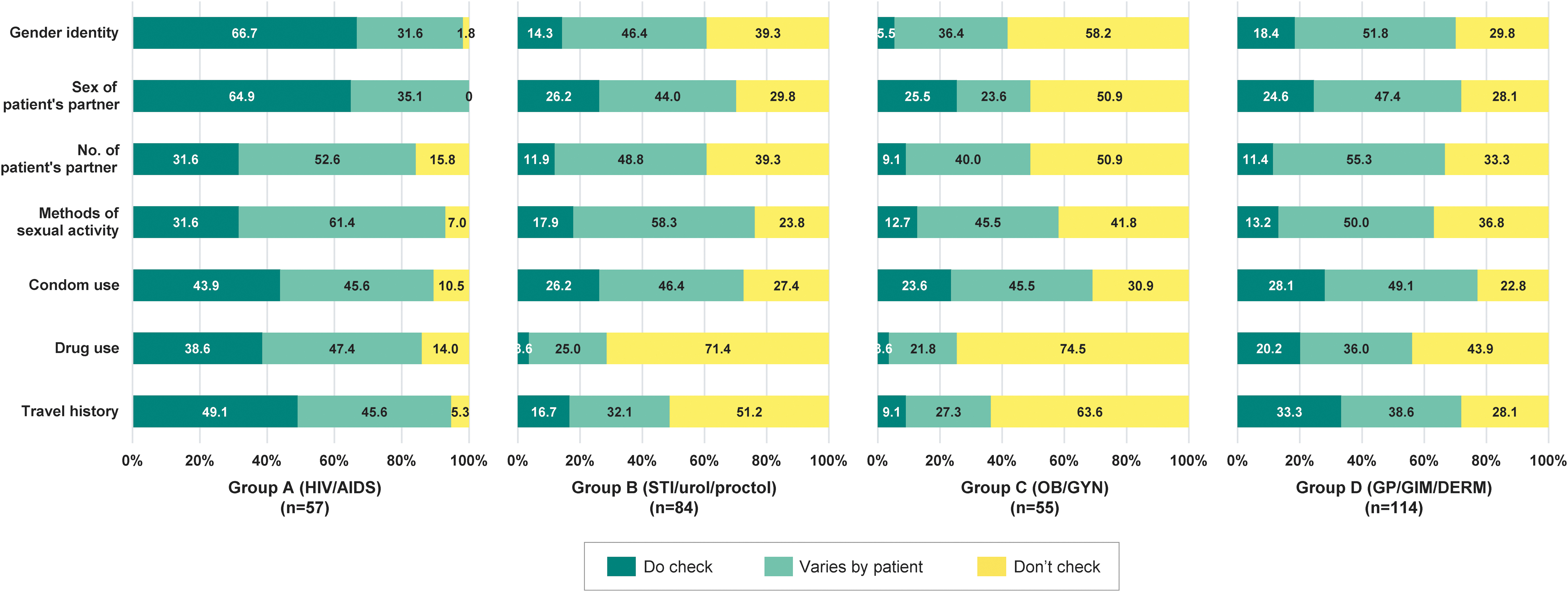
Interview on patients' risk behaviors. Distribution of physicians in Groups A to D by frequency of obtaining STI/HIV risk behaviors from their patients. AIDS, acquired immunodeficiency syndrome; DERM, dermatology; GIM, general internal medicine; GP, general practitioner; Gr, group; GYN, gynecology; HIV, human immunodeficiency virus; OB, obstetrics; proctol, proctology; STI, sexually transmitted infection; urol, urology.
To learn more about consultation practices, 274 and 220 physicians who provided screening tests for STI and HIV, respectively, in the past year were asked about the reasons for performing screening tests. When initiated by patients, the most frequent reasons for STI screening tests (excluding HIV) were: (1) patients had related symptoms (76.6%, 210/274); followed by (2) patients engaged in risky behavior (68.2%, 187/274); and (3) patients' partner/s had STI/HIV (58.8%, 161/274) (Table 2). When physicians recommended STI screening, the main triggers were: (1) suspected of having STI/HIV (56.9%, 156/274), followed by (2) engaged in behavior that poses a risk of infection (43.1%, 118/274), and (3) because partner has STI/HIV (35.4%, 97/274) (Table 2).
Reasons for STI and HIV Screening Tests
AIDS, acquired immunodeficiency syndrome; CSW, commercial sex worker; DERM, dermatology; GIM, general internal medicine; GP, general practitioner; GYN, gynecology; HIV, human immunodeficiency virus; MSM, men who have sex with men; OB, obstetrics; STI, sexually transmitted infection.
Similarly, the main reasons for HIV screening tests when initiated by patients were: (1) patients engaged in risky behavior (56.4%, 124/220); followed by (2) patients' partner/s had STI/HIV (26.8%, 59/220); and (3) patients had related symptoms (20.9%, 46/220) (Table 2). When physicians recommended HIV screening, the most common reasons were: (1) suspicion of having STI/HIV (38.6%, 85/220); (2) engaging in risky behavior (30%, 66/220); and (3) having a partner with STI/HIV (17.3%, 38/220) (Table 2).
Challenges in STI and HIV care
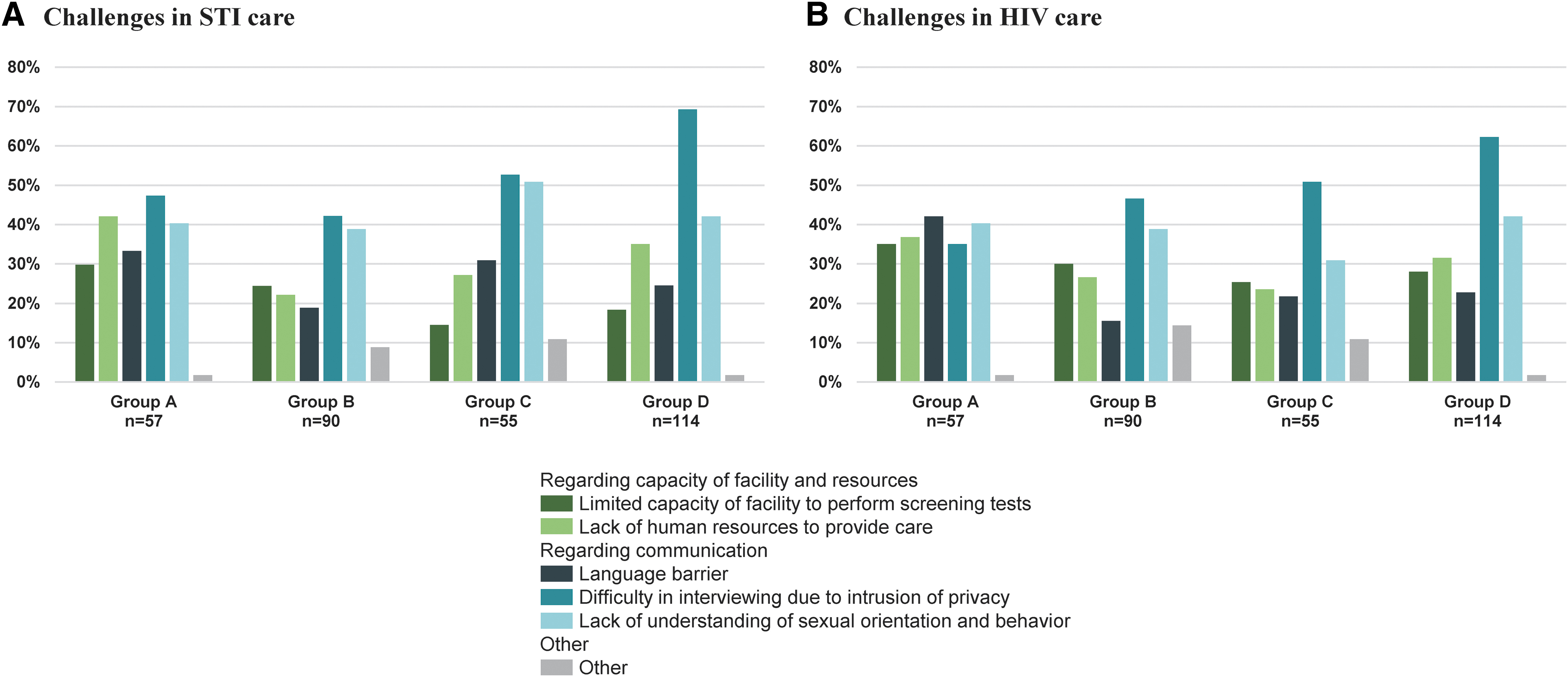
Physicians across Groups A to D were probed about the challenges in STI/HIV care associated with patient communication, as well as resource and capacity limitations. Difficulty in interviewing due to intrusion of privacy was the most frequently raised challenge in both STI and HIV care across all groups, with it being highest for Group D (69.3% for STI care and 62.3% for HIV care) (Fig. 3A, B, respectively). Insufficient knowledge about the sexual orientation and behavior of sexual minorities emerged as another major communication barrier (Fig. 3A, B).
Challenges in
Familiarity with HIV care
Physicians from Groups A to D were probed regarding their awareness of recommended antiretroviral drugs in HIV treatment guidelines and their ability to provide treatment for PLWH. All of the HIV-specialized physicians in Group A were familiar with all the recommended combinations as per the latest guidelines or knew the combination, although this may not be the latest information (Fig. 4A). More than half of the physicians in Group B (58.9%, 53/90), Group C (58.2%, 32/55), and Group D (44.7%, 51/114) were not aware of any recommended combinations regardless of whether the guidelines were the latest or not (Fig. 4A). Most physicians in Group A (86%, 49/57) declared that they could treat and manage PLWH, including making decisions on antiretroviral regimens, whereas the proportions of physicians in Groups B to D who declared that they could treat and manage HIV patients either with or without support for treatment decisions were 25.6% (23/90), 25.5% (14/55), and 47.4% (54/114), respectively (Fig. 4B).

Familiarity with HIV care among four physician groups.
Knowledge and willingness of recommending PrEP
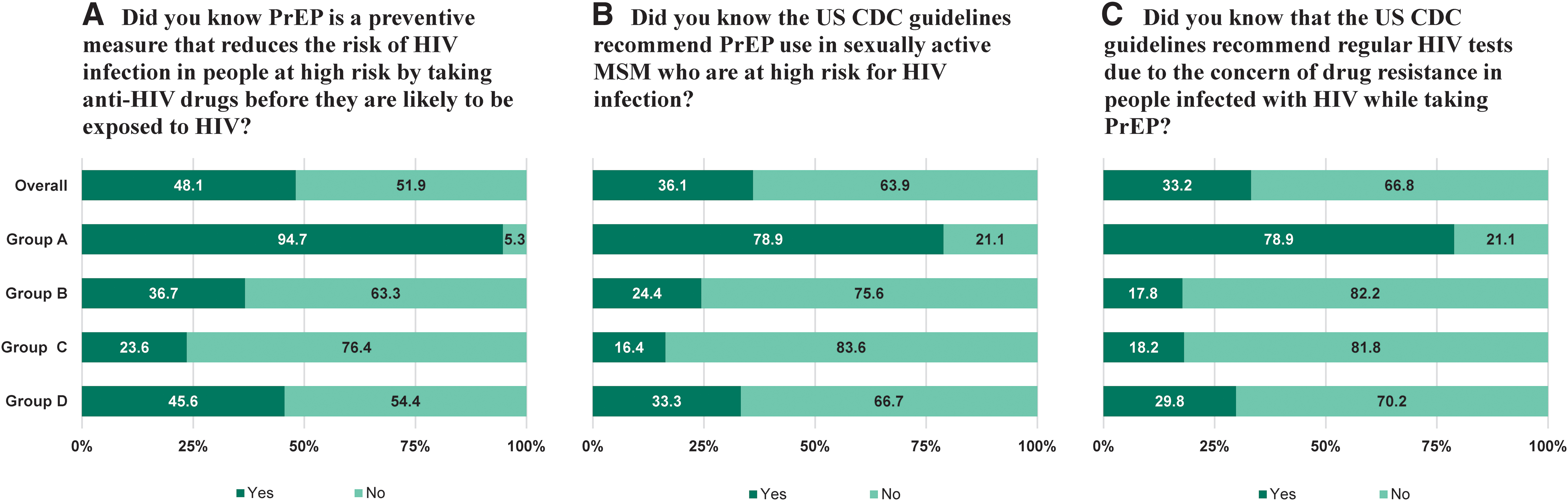
Physicians across Groups A to D were probed regarding their depth of knowledge of PrEP as an HIV prevention method. Overall, 48.1% (152/316) knew that PrEP is a method of prevention in which people with a high risk of contracting HIV are given antiretrovirals before they are likely to be exposed to HIV, thereby reducing the risk of HIV infection (Fig. 5A). Overall, the proportion of physicians with knowledge of other PrEP concepts was low, with 36.1% (114/316) knowing that CDC guidelines recommended the use of PrEP for sexually active MSM who are at risk of HIV infection and 33.2% (105/316) knowing that CDC guidelines recommended routine HIV testing to confirm HIV-negative status (Fig. 5B, C, respectively). The proportion of physicians with PrEP knowledge differed greatly across the four groups. Regarding the first question on PrEP, for instance, 94.7% (54/57) of the physicians in Group A were aware, whereas the proportions in Groups B, C, and D were 36.7% (33/90), 23.6% (13/55), and 45.6% (52/114), respectively (Fig. 5A).
Differences in PrEP awareness among four physician groups.
Likewise, 78.9% (45/57) of the physicians in Group A knew that CDC guidelines recommended the use of PrEP for sexually active MSM who are at risk of HIV infection. On the other hand, the majority of the physicians in Group B (75.6%, 68/90), Group C (83.6%, 46/55), and Group D (66.7%, 76/114) were unaware of this CDC guideline (Fig. 5B). Unlike those in Group A, the majority of physicians in the other groups did not know that individuals who take HIV PrEP should be regularly tested for HIV due to concerns about drug resistance (Fig. 5C). Clearly, a higher proportion of HIV-specialized physicians in Group A were aware of PrEP guidelines.
The level of attitude toward recommending and prescribing PrEP to their patients varied among the four physician groups. The proportion of physicians who would proactively recommend PrEP to their patients was the highest for Group A at 49.1% (28/57), whereas the proportion was lower at 10% (9/90) in Group B, 14.5% (8/55) in Group C, and 14.9% (17/114) in Group D. In contrast, physicians who would prescribe PrEP only when the patient requested it were more common in Groups B, C, and D, at 64.4% (58/90), 72.7% (40/55), and 77.2% (88/114), respectively. A logistic analysis was carried out to identify physician-related factors associated with a willingness toward recommending and prescribing PrEP. Univariate analysis showed several factors to be significantly associated. In the multivariable analysis, having knowledge of PrEP was identified as a factor associated with willingness to recommending and prescribing PrEP (odds ratio: 2.31, 95% confidence interval: 1.30–4.10, p = 0.0044) (Table 3).
Factors Associated with Willingness to Prescribe PrEP
City; ordinance-designated cities.
Rural; any other areas.
Statistically significant, p < 0.05.
CI, confidence interval; CSW, commercial sex worker; DERM, dermatology; GIM, general internal medicine; GP, general practitioner; GYN, gynecology; HIV, human immunodeficiency virus; OB, obstetrics; OR, odds ratio; PrEP, pre-exposure prophylaxis; STI, sexually transmitted infection.
Perception toward PrEP approval and concerns
Knowledge of PrEP was identified as an independent factor associated with the willingness to prescribe PrEP, as shown in Table 3. For subsequent analyses, physicians were regrouped into one of the three PrEP knowledge groups based on the awareness of PrEP (Fig. 6A). This regrouping enabled us to determine physician responses based on their knowledge of PrEP independently of the nature of their clinical practice.
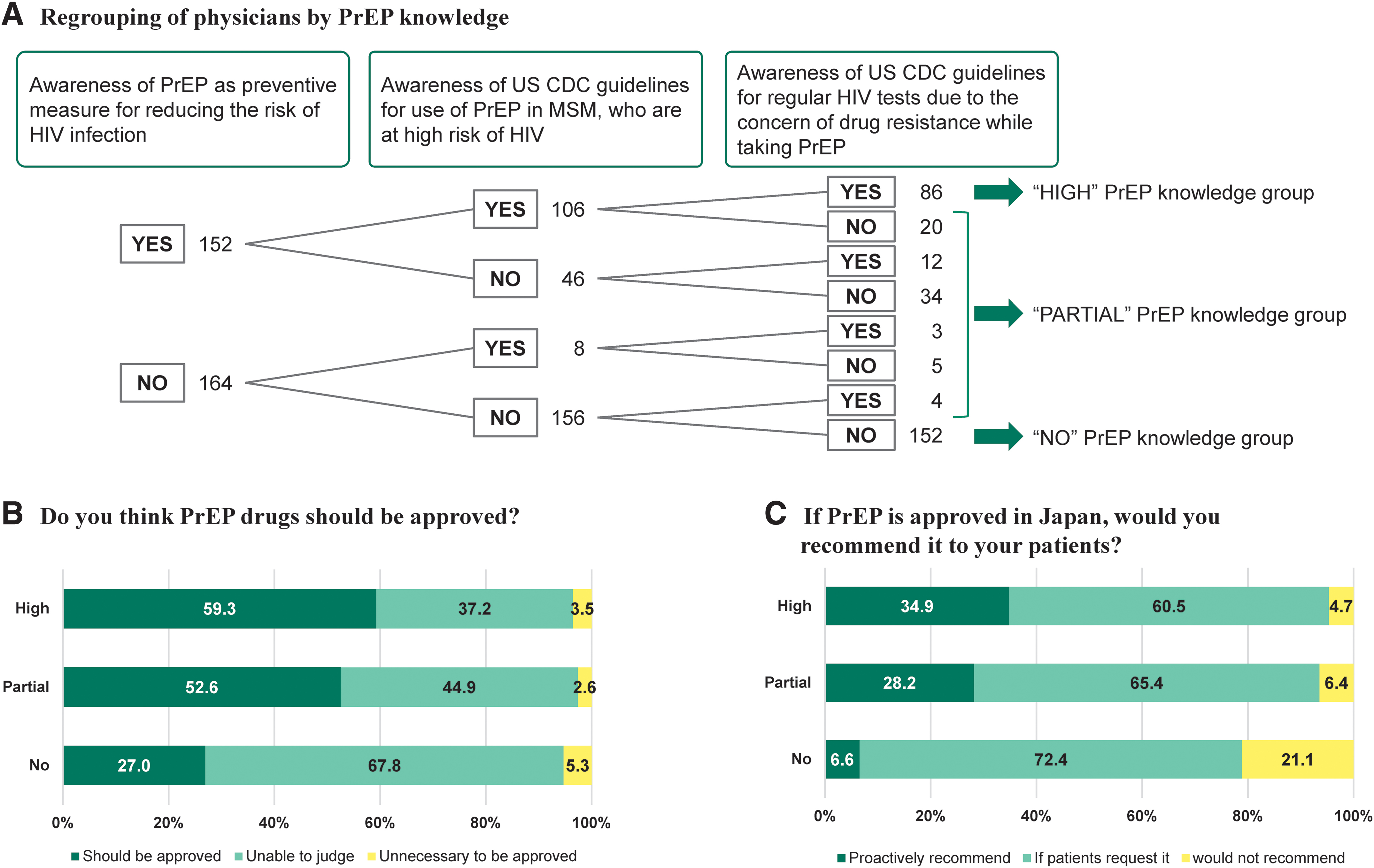
Regrouping of physician, PrEP approval, and recommendation by PrEP knowledge groups.
PrEP approval and recommendations
Regarding the opinions on the approval of PrEP drugs in Japan and their willingness to recommend them to their patients, physicians in the “High” knowledge group (59.3%, 51/86) were supportive of the approval of PrEP drugs in Japan, whereas the majority of physicians in the “No” knowledge group were unable to decide (67.8%, 103/152) (Fig. 6B). The proportion of physicians who would proactively recommend PrEP to their patients after its approval in the High, Partial, and No knowledge groups was 34.9%, 28.2%, and 6.6%, respectively. Together with the physicians who would prescribe PrEP upon patient request, 95.3%, 93.6%, and 78.9% of physicians were willing to prescribe PrEP in the High, Partial, and No knowledge groups, respectively (Fig. 6C). Physicians who knew about PrEP tended to be supportive of its approval and were willing to recommend it to patients.
Concerns about PrEP use
Physicians were asked about the concerns they would have in prescribing PrEP drugs if approved in Japan. Among the High PrEP knowledge group, an increase in unsafe sexual practices without condom use, the consequent increase in STIs (61.6%, 53/86), and the economic burden on PrEP users (55.8%, 48/86) were the key concerns, whereas in the Partial PrEP knowledge group, the major concerns were side effects (57.7%, 45/78), drug resistance (53.8%, 42/78), and an increase in STIs (53.8%, 42/78) (Fig. 7). The key concerns for the No PrEP knowledge group were side effects (52.0%, 79/152), increase in STIs (48.7%, 74/152), economic burden (46.7%, 71/152), and response to HIV infections (45.4%, 69/152) (Fig. 7).

Concerns about prescribing PrEP raised by “High,” “Partial,” and “No” PrEP knowledge levels.
Discussion
The present study explored the current practices of STI/HIV care, including initiation of STI/HIV screening tests, the challenge of managing patients with STI/HIV, and the knowledge, willingness, and key concerns of PrEP among the four physician groups (A to D) who would encounter and provide health care for individuals with STI and/or HIV, and we observed differences among the four Groups, especially between Group A (HIV specialized physicians) and other Groups B–D (non-HIV specialized physicians). There was a small proportion (3.6–8.8%) of non-HIV specialists, Group B to D, who never interviewed patients with STI/HIV about their sexual behaviors. On the contrary, a large proportion of HIV specialists, Group A, always interviewed the patient's and/or patient's partner's history of STI/HIV (84.2% and 66.7%, respectively) (Fig. 1), as well as other possible risk behaviors (Fig. 2). They were also found to spend approximately twice as much time interviewing compared with non-HIV specialists, suggesting that these patients' background information is valued by HIV specialists in providing STI/HIV care.
Concerns about intrusion into patient privacy were the key challenge for non-HIV specialists seeking information from patients about their history and risk behavior, and this may have resulted in the lower proportion of provider-initiated STI/HIV screening tests (Table 2). As early symptoms of HIV infection are usually not apparent, it is important for physicians to recommend HIV testing based on the patient's risk behavior and subtle symptoms for early detection and treatment. Low numbers of HIV screening tests as opposed to the number of STI patients suggested that recommending and performing HIV screening test at the time of STI diagnosis would lead to early detection of HIV. Furthermore, the average number of STI and HIV tests was the highest in Group C (Table 1), and this may be because tests for syphilis and HIV are included as part of prenatal care exams. Although the rate of HIV positives is low at 0.7%, incorporating STI/HIV screening tests into routine physical exams may be another way to increase early testing and diagnosis.
Approximately 53% to 75% of non-HIV-specialized physicians declared that they were incapable of making decisions related to HIV medication or manage treatment, whereas the majority of HIV-specialized physicians (86%) were capable of HIV treatment decision making and management. The competence gap between HIV and non-HIV specialists in this regard can be bridged because 16.4% to 38.6% of the non-HIV-specialized physicians revealed that they could manage PLWH after an antiretroviral therapy regimen is selected. This suggests that enabling cooperation and support among HIV and non-HIV specialists can motivate non-HIV specialists to consider treatment for PLWH and manage HIV care thereafter. Such collaborative support of HIV specialists will reduce the hesitancy in diagnosing and providing HIV care, and enhance concurrent STI/HIV testing opportunities by non-HIV physicians.
With regard to PrEP, differences in knowledge and awareness were observed between HIV-specialized physicians (Group A) and the groups of other physicians (Groups B to D) (Fig. 5). Physicians who knew all three basic concepts of PrEP (“High” PrEP knowledge group) were more supportive of PrEP approval and showed a willingness to proactively recommend PrEP to their patients than those with less knowledge (Fig. 6 and Table 3). This is in line with previous studies that reported the higher willingness of specialist physicians to prescribe PrEP compared with primary care providers. 31,32 This suggests that measures to raise awareness and provide training on PrEP for physicians who may encounter STI patients and potential undiagnosed PLWH are needed for the successful implementation of PrEP. 33,34
Concerns about the possibility of an increase in STIs due to an increase in unsafe sexual practices without the use of condoms while on PrEP was raised regardless of the PrEP knowledge level. Recent studies on the PrEP users' sexual behavior found the increased proportion of the condomless anal sex after PrEP initiation, and the authors discussed the need for client-centered approaches to encourage condom use while on PrEP. 35,36 As many physicians in this study were already concerned that PrEP initiation might lead to unprotected sex, it is desirable to take more time to interview deeper about each patient's risk behaviors (Fig. 2 and Table 1) and discuss about the health protection strategies with the PrEP users.
The inability to respond and manage when an individual is infected with HIV while on PrEP was the concern raised more frequently by physicians in the “No” PrEP knowledge group compared with those in the other groups. A study by Operario et al. showed that training physicians on STI and HIV knowledge, diagnosis, treatment, and counseling results in a reduced incidence of STI reinfection. 37 Such training on HIV and STIs for physicians regardless of their specialty is needed in Japan to address these concerns and to promote STI/HIV preventive measures. Non-HIV-specialized care providers have greater access to patients who are undiagnosed with HIV compared with HIV specialists. Disseminating knowledge to non-HIV specialist providers, such as primary care providers and OB/GYNs, is important, as such providers can act as key sources of information on PrEP, especially for women. 38,39
Altogether, collaborative efforts by both HIV specialists and non-HIV-specialized physicians, as well as educational programs on STI and HIV, will promote provider-initiated STI/HIV screening tests for early diagnoses, enhance preventive measures for STI and HIV, and create linkages to HIV care. Furthermore, providing knowledge and tools (information, guidance, etc.) will allow physicians with limited experience in HIV care to prescribe and use PrEP, thereby improving patient access in a sustainable manner. 40
Limitations
The study participants were selected by a single panel, which may have resulted in sample selection bias. Also, the sample drawn from a single panel might not be representative of the physician population in Japan. There is a possibility of inaccuracy in the recollection of events and experiences reported by the participating physicians, which may have led to information bias. Nevertheless, within the panel, the physicians were selected randomly by a third party, which may have minimized the possible bias. Furthermore, all the data collected were anonymized, which contributed to a reduction in observer bias. There may also have been a bias stemming from the heterogeneity of patients interviewed by Group A physicians, as opposed to those interviewed by physicians in Groups B to D. Group A physicians mostly saw PLWH who visited hospitals routinely and could be interviewed thoroughly, whereas physicians in Groups B to D often had outpatients who visited the clinic only once for a certain symptom.
Footnotes
Acknowledgments
The authors would like to acknowledge Hiromi Kato from IQVIA Solutions Japan K.K. for data collection, Lakshman Puli for medical writing and editing support, and Sven Demiya for project administration. The authors are grateful to Takanori Aikawa from MSD K.K. for project administration support.
Authors' Contributions
M.K.: Conceptualization, Methodology, Validation, Writing—Review and Editing, and Visualization. D.F.: Validation and Writing—Review and Editing. N.K.: Conceptualization, Methodology, Validation, and Writing—Review and Editing. D.A.: Methodology and Project administration. J.H.: Conceptualization, Methodology, Validation, Writing—Review and Editing, and Visualization.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. This study is based on the web-based survey. For the purpose of the study, data of respondents' attributes collected were limited to the age group, gender department of specialty, location of medical practice, and type of institute, with which the survey respondents, or their patients could not be identified. For the reason, this study does not meet the definition of human subject and we did not seek for the approval of an Ethics Committee. Informed consent was obtained from all individual participants before participating in the survey.
Author Disclosure Statement
M.K., D.F., N.K., and J.H. are employees of MSD K.K., Tokyo, Japan.
Funding Information
The study was sponsored by MSD K.K., Tokyo, Japan (VEAP ID 9163).