
Abstract
Adherence to antiretroviral therapy (ART) is essential in determining successful treatment of human immunodeficiency virus (HIV). The adoption of digital health is suggested to improve ART adherence among people living with HIV (PLHIV). This study aimed to systematically determine the effect of digital health in enhancing ART adherence among PLHIV from published studies. The systematic search was conducted on Scopus, Web of Science (WoS), PubMed, Ovid, EBSCOHost, and Google Scholar databases up to June 2022. Studies utilized any digital health as an intervention for ART adherence enhancement and ART adherence status as study's outcome was included. Digital health refers to the use of information and communication technologies to improve health. Quality assessment and data analysis were carried out using Review Manager (RevMan) version 5.4. A random-effects model computed the pooled odds ratio between intervention and control groups. The search produced a total of 1864 articles. Eleven articles were eligible for analysis. Digital health was used as follows: six studies used short message service or text message alone, three studies used mobile applications, and two studies used combination method. Four studies showed statistically significant impacts of digital health on ART adherence, while seven studies reported insignificant results. Results showed studies conducted using combination approach of digital health produced more promising outcome in ART adherence compared to single approach. New innovative in combination ways is required to address potential benefits of digital health in promoting ART adherence among PLHIV.
Introduction
Since the epidemic began in 1981, a total of 84.2 million individuals have been infected with human immunodeficiency virus (HIV), with ∼40.1 million deaths reported. 1 Recent statistics documented that about 38.4 million people across the globe are infected with HIV with 1.5 million new infections diagnosed in 2021. 2 In Malaysia, there are 77,903 people living with HIV (PLHIV), with 3564 newly infected cases in 2019. 3 With the increase in the number of PLHIV, the Joint United Nations Program on HIV and AIDS (UNAIDS) has proposed aggressive targets for the global response to HIV in 2020 by applying the 95-95-95 strategy.
This strategy sets a target in which 95% of PLHIV know their status, 95% of diagnosed PLHIV are on antiretroviral therapy (ART), and 95% of PLHIV on ART achieve an undetectable viral load by 2030. 4 To reach the third target, which specifically refers to PLHIV on ART that achieved undetectable viral loads, a good adherence to ART is the main key factor. 5
Antiretroviral drugs (ARV) act by interrupting viral replication processes and are classified based on how they inhibit the viral cycle. ART is a combination of at least three ARVs, which is used to prevent HIV replication and hence slow the disease progression. 6 Used as a long-term treatment, the success of ART is highly dependent on patients establishing and maintaining high levels of ART adherence. 7,8 ART is currently being advocated not only as a way to delay the onset of AIDS and improve the health of PLHIV but also as a public health tool to prevent HIV transmission. 9,10 ART effectiveness demands adherence of at least 95% to achieve viral load suppression. 7,11
Treatment adherence is associated with a multitude of benefits, including reduced transmission and lower expenditures. 12,13 Socioeconomic or environmental factors (such as income and access to ART medications), demographic factors (such as age, gender, and ethnic background), social elements (such as literacy level, use of alcohol/substance, and stigma), and emotional factors (such as anxiety, stress, tension, and fear) may also affect patients adherence to ART. 14 Nonadherence to HIV therapy may be linked to poor health and well-being, the development of drug-resistant HIV strains, treatment failure, a faster progression to AIDS, and death in PLHIV. 15,16
Digital health refers to the use of information and communication technologies to improve health. 17 The implementation of digital health has been classified into noninternet based [e.g., short message service (SMS) or text message and phone calls] and internet based (e.g., social media, e-mail, mobile application and website). 18
Most recently, digital health has been used to improve medication adherence. 19 Digital health is known as a cost-effective way to increase the efficiency of the health care system, such as improving medication adherence and health outcomes by utilizing technologies such as computers, internet, satellite communications, and mobile devices. 19 These technologies are also used as appointment reminders, mobile telehealth and patient monitoring, as well as for treatment adherence. 20 In earlier work, SMS or text message used as a reminder for 6 months has proven to be successful in enhancing ART adherence and treatment outcomes among PLHIV. 19
SMS or text message is particularly beneficial because of its simplicity, low cost, and flexibilty. 20 The rate of mobile phone subscribers in 2013 for developing countries was as high as 90%, 21 which is a key factor supporting the development of digital health as a means of improving adherence outcomes. The success of this particular type of digital health is further supplemented by declining costs of mobile devices and internet services. The average price of a smartphone in the Middle East and Africa has dropped 32.1% between 2013 and 2017 and steadily decreasing. 22 Mobile broadband subscriptions have surged by more than 20% globally since 2012, and by more than 30% in developing countries. 22
Previously, two systematic reviews indicate that weekly text messaging can improve adherence to ART when compared to standard care. 23,24 Another review showed the utilization of text message combined with phone calls from health care providers has demonstrated beneficial impacts on ART adherence outcomes. 25 A later review revealed inconclusive findings with wide variation regarding the efficiency of mobile phone interventions in enhancing adherence to ART. 26 A substantial number of recent articles utilizing randomized controlled trial (RCT) design, especially on the mobile applications, justify the demand of an extensive systematic review to collate and present the overall study designs and findings. Thus, the purpose of this review was to identify and systematically evaluate published research on the usefulness of digital health in enhancing ART adherence among PLHIV.
Methods
Search strategy
A systematic review and meta-analysis of published literature were conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for the classification of quality assessment and data extraction. 27 Systematic search of literature was performed from the date of inception until June 30, 2022, on various databases namely Scopus, Web of Science (WoS), PubMed, Ovid, EBSCOHost, and Google Scholar.
The screening search was focused on identifying studies that evaluate the effectiveness of digital health in enhancing ART adherence among PLHIV. Digital health was included as any digital technology that was used to enhance medication adherence, which includes SMS, mobile applications, e-mail, reminder, and text message. Search keywords were selected based on Population, Intervention, Comparison, and Outcome Model. The population was set as PLHIV on ART. The intervention was any use of digital health. The comparison was a formal control group such as standard management. The outcome was ART adherence measurement as primary or secondary outcomes.
Medical Subject Heading (MeSH) and terms that were used to search for relevant publications include “antiretroviral therapy,” “highly active antiretroviral therapy,” “human immunodeficiency virus,” “HIV,” “acquired immunodeficiency syndrome,” “disruptive technolog*,” “digital technolog*,” “mobile app*,” “digital app*,” “mobile healthcare,” “mhealth,” “digital health,” “adherence,” “compliance,” and “medication adherence” Boolean's operators such as OR and AND were utilized to narrow the search. No limitation was applied with regard to the year of publication during searching. Articles published in English language were only included. Abstracts and conference proceedings, editorials, and expert opinion articles were excluded.
Study selection and eligibility criteria
Initial screening was performed, and the title and abstract of each study were reviewed. Based on the inclusion and exclusion criteria, the full eligibility of screened abstracts was assessed. Two reviewers (M.F.C.P. and FI) performed the screening and all disagreements were resolved by moderation with a third researcher (MMB). Only RCT and randomized factorial trial (RFT)-designed studies that utilized digital health to enhance ART adherence compared to a control were included. Studies were included based on the following criteria: ART adherence as a primary or secondary outcome. ART adherence using specific method of adherence tool. Reports on adherence level. Adult patients older than 18 years. English articles.
The search retrieved 1864 articles. After screening process, 24 abstracts were excluded. A full-text review of the remaining 35 potentially eligible articles was conducted. A total of 11 articles were included in the analysis. The most common reason for exclusion was labeled under others category (n = 12). These include articles that involved patients younger than 18 years (n = 2), PLHIV with mental illnesses (n = 2), articles available in abstract only (n = 4), and studies with viral suppression or viral load level only as an outcome (n = 4). Other studies were excluded due to qualitative studies (n = 1), feasibility and acceptability studies (n = 1), no adherence method was available (n = 3), and non-RCT studies (n = 7).
Extraction and analysis of the data
Data extraction included study design, aim of study, reminder method, population, inclusion and exclusion criteria, type of adherence measure, type of digital health, duration of study, and study outcomes. A p values <0.05 was considered significant.
A meta-analysis was performed to synthesize the results of two or more studies that used comparable outcome measures. The Mantel-Haenszel fixed-effect model was used to generate odds ratios and 95% confidence intervals for Forest plots. The chi-square and I 2 tests were used to determine heterogeneity. Data retrieval using the Web Plot Digitizer version 4.6 web tool 28 was utilized for one of the studies, which describes the results in a graphical form. 29 Review Manager (RevMan) version 5.4 was used to conduct all statistical analyses (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen).
Risk of bias assessment
The quality assessment was conducted based on the recommendation by the Cochrane Handbook of Systematic Reviews, particularly emphasizing on allocation concealment, sequence generation, outcome assessment, blinding, and selective reporting. 30 The bias risk for each domain was rated as low, unclear, or high risk. The total bias risk was labeled as high if at least one area was at high risk of bias.
Results
A total of 1864 articles were identified. Based on the study criteria, only 11 articles were included (Fig. 1). Six studies used SMS or text message alone for reminders, three studies used mobile applications, and two studies used a combination method of SMS with phone call or interactive voice response (IVR; Table 1). Five studies were conducted in the United States of America 31 –35 and one each from Malaysia, 19 Singapore, 36 China, 37 Cameroon, 38 India, 29 and Uganda. 39
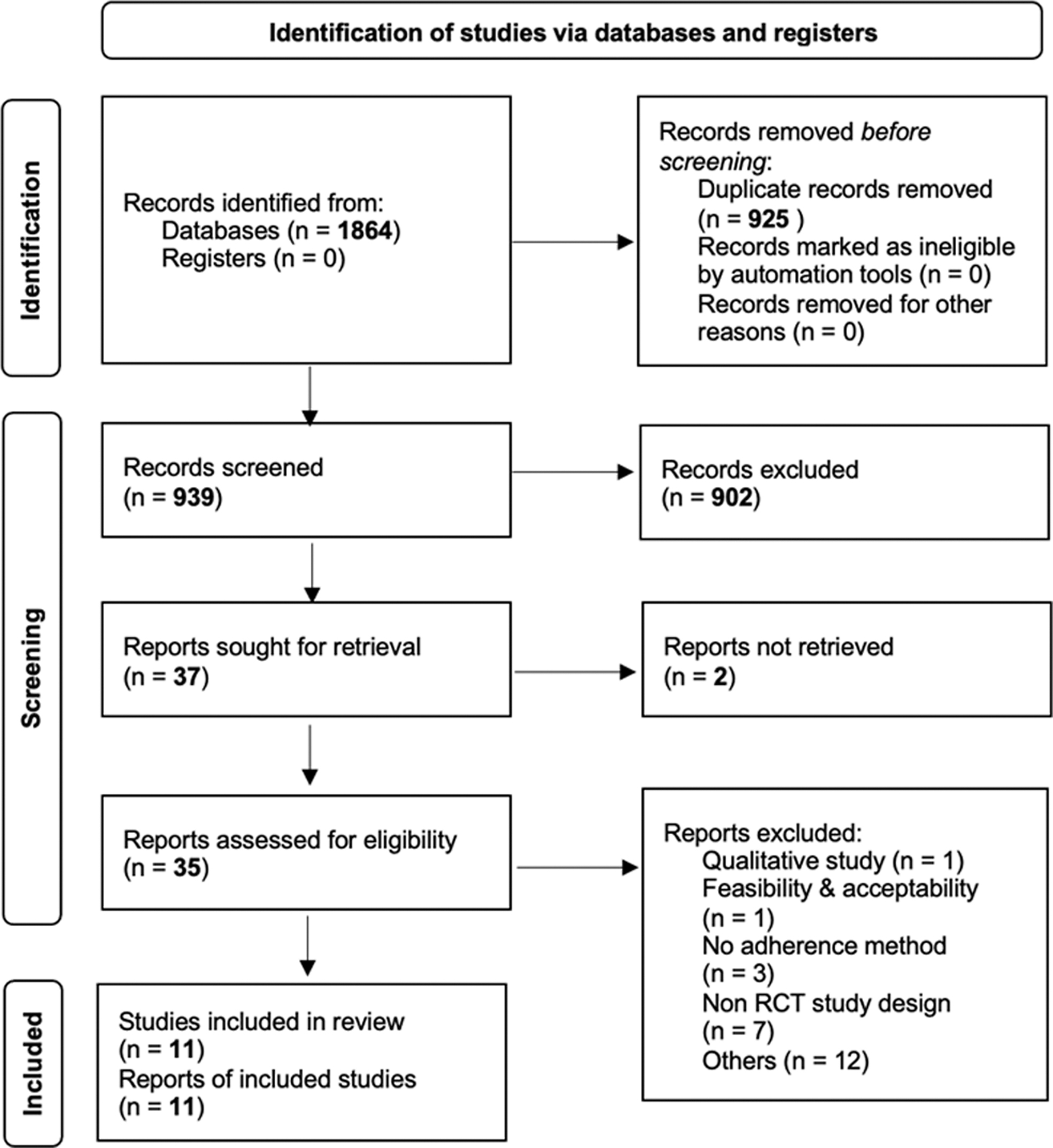
PRISMA flow chart of study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Details of Included Studies
AACTG, adult AIDS clinical trial group; ACTG, AIDS clinical trial group; ART, antiretroviral therapy; CPCRA, community programs for clinical research on AIDS; iTAB, individualized texting for adherence building; IVR, interactive voice response; MEMS, medication event monitoring system; MIST, mobile interactive supervised therapy; MSM, men sex with men; N/A, not available; N/R, not reported; PLHIV, people living with human immunodeficiency virus; RCT, randomized controlled trial; RFT, randomized factorial trial; SMS, short message service; UPC, unannounced pill count; VAS, visual analogue scale.
Ten studies followed an RCT design (six RCT 19,31,32,37 –39 and four pilot RCT 29,33,34,36 ) and one study utilized RFT design. 35 The studies were conducted between 2011 and 2018 and published from 2016 to 2020. The total number of participants in the included studies was 1785, and the study sample size varied from 30 to 600 participants per study. The primary outcomes addressed in the studies included ART adherence, HIV viral suppression, and usability and feasibility of the technology.
The risk of bias in RCTs was assessed using domains suggested by the Cochrane Handbook of Systematic Reviews. All studies reviewed fell under the low-risk category of bias, as shown in Fig. 2. Four studies 31,33,37,38 did not report allocation sequence concealment. One study 34 contained a possible contamination bias between control and intervention participants.
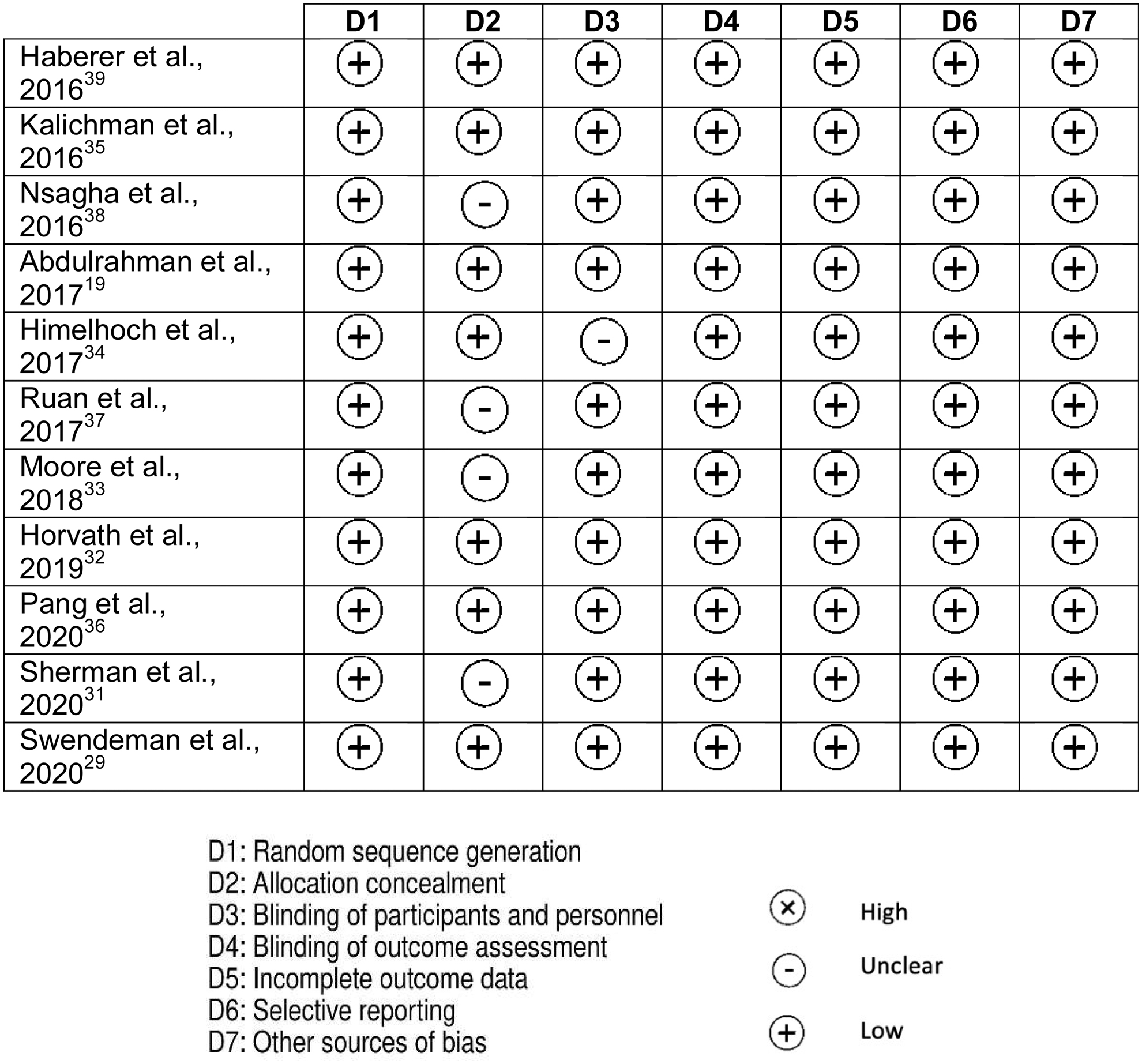
Risk of bias summary of individual study.
The majority of studies involved male and female participants, except for one study that only included MSM individuals. 32 Four studies recruited participants who have less than 95% adherence at baseline. 29,32,34,35 Seven studies acknowledged recruiting treatment-experienced patients, 29,32 –36,38 while another four studies enrolled newly initiated ART patients. 19,31,37,39 Three studies recruited PLHIV with a history of drug use. 32 –34
Four studies found that adherence to ART had a statistically significant and beneficial effect on groups of PLHIV who were allocated digital health 17,29 –31 (Table 2). The remaining seven studies failed to find a significant difference between the intervention and control groups. 21,23 –28
Summary of Duration of Study and Adherence Measures
Seven studies were included in the meta-analysis. 19,29,31,32,35,37,38 One study was excluded from meta-analysis due to non-numerical data reported and data could not be estimated using a graph digitizer. 34 Two studies reported data as percentage of adherence without the exact number of patients. 33,39 Another one study was excluded as the odds ratio was not estimable as all recruited PLHIV in both intervention and control group achieved 100% good adherence at baseline and at the end of the study. 36
A meta-analysis was performed on the remaining seven studies. An odds ratio was used to compare the outcome of intervention between studies. The odds ratio estimated odds of poor adherence between control and intervention groups. The pooled odds ratio was found to be 0.05 (p = 0.08; Fig. 3) with statistical heterogeneity (I 2 = 82%). Subanalysis was carried out to compare the outcome of intervention between studies that involved single and combination approach of digital health with statistical heterogeneity, I 2 = 50% and I 2 = 86%, respectively (Fig. 3). One study that was conducted among new PLHIV, who initiated ART, showed improvement in adherence status compared to stable PLHIV. 19
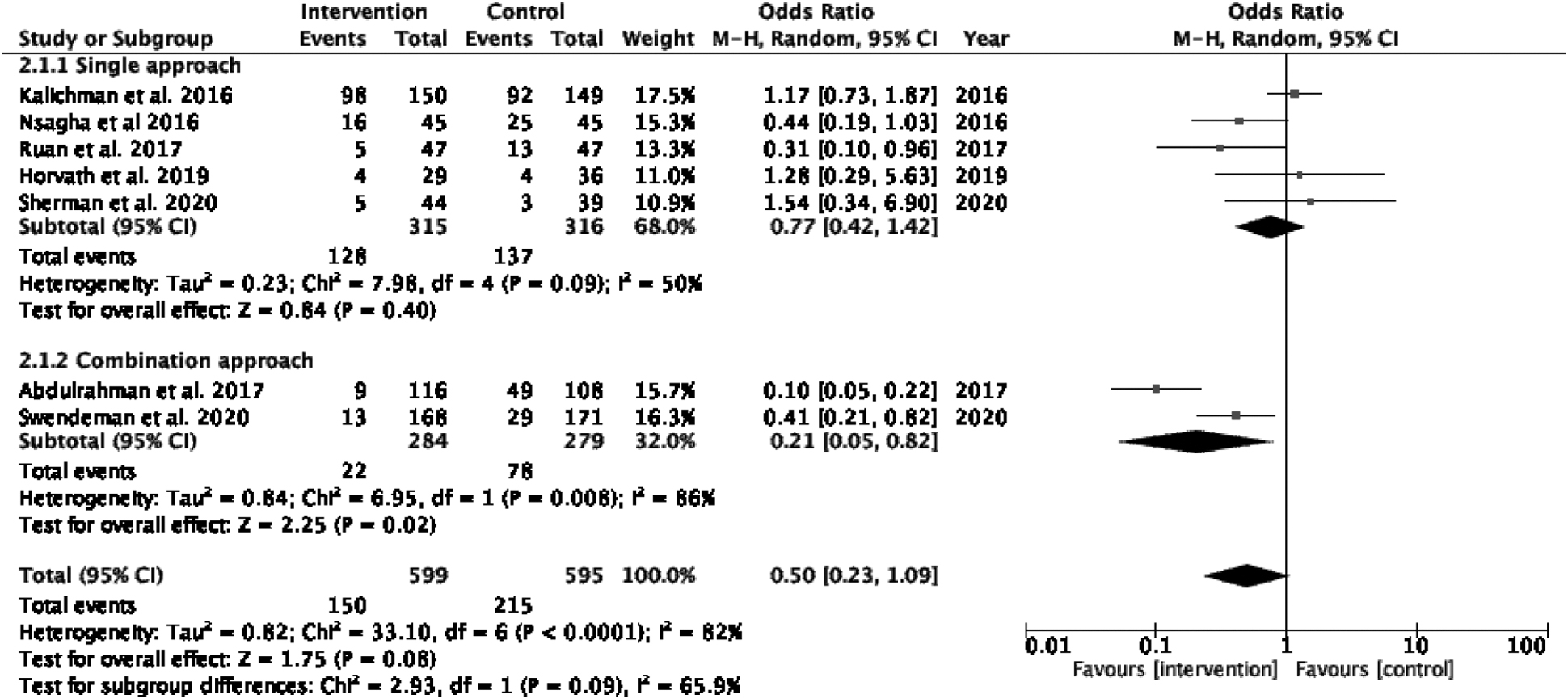
Forest plot result showing ART adherence with digital health intervention. ART, antiretroviral therapy.
Discussion
Along with the industrial revolution, health care technology continues to evolve exponentially. 40 However, not all interventions showed positive outcomes on medication adherence. Only 36% (n = 4) of included studies concluded that digital health significantly enhanced PLHIV adherence to ART. These data are lower than previously reported at 56%, specifically in low- and middle-income countries. 26 The higher percentage of other work could be due to the inclusion of 8 non-RCT studies from a total of 27 studies.
The differences in the PLHIV population between studies were observed. Three of four studies conducted among new PLHIV patients who had only been on ART for less than 3 months found that digital health effectively enhanced ART adherence. 19,37,39 Only one of the seven trials enrolling PLHIV who were already on ART demonstrated a significant usage of digital health in improving ART adherence. 38 This finding emphasized the crucial function of commencing intervention earlier before PLHIV developed ART taking habits. 36
Two studies showed no benefit of digital health among the subpopulation of PLHIV with a history of stimulant used. 32,33 These results may suggest that certain components of an individual's lifestyle may be more difficult to adjust depending on their PLHIV background. Digital health may need to be accompanied with additional components to enhance positive behavioral changes, such as direct communication with a physician other than just reminders from text messages and mobile applications. 22
The efficiency of using mobile applications as reminders is currently unclear, and more research is needed. Definite conclusion cannot be drawn as the available studies that used mobile application as a reminder recruited a small sample size. 32,34,36 In one study, both intervention and control groups demonstrated 100% adherence to ART at baseline, which left no possibility for additional improvement. 36 Despite this challenge, the potential use of mobile applications should be explored as one of the effective ways in enhancing medication adherence. Quintiles IMS institute for health care informatics reported 23,682 iOS mobile applications substantially relevant to health were established. In 2015, the number of iPhone operating system (iOS) mobile applications related to health surged by more than 100%. 22 About 65% of these mobile applications include medication reminders and health information. 22
The latest innovation in HIV treatment is long-acting ART. The majority of PLHIV expressed a high level of interest in long-acting ART, despite its administration through injection form, and requires monthly visit to hospital. This novel innovation is a future improvement to ART regarding adherence challenges, but it may be associated with other issues among PLHIV. 41
This meta-analysis, however, showed no significant difference in the odds ratio for ART nonadherence between intervention and control groups. A study conducted among adolescents living with HIV similarly showed no difference in ART adherence and clinical outcomes. 42 Nevertheless, subanalysis of digital health in combination approach produced significant result compared to single approach. Both studies combined a telephone call or voice message with SMS or text messages as part of the approach. 19,29 According to a previous meta-analysis and systematic review, a combination of reminder methods was found to be much more effective than a single reminder method in improving ART adherence. 43,44 Although a combination approach can enhance adherence, their efficacy is limited, diminishes over time, and varies across countries. 26
In comparison to the previous work, a Cochrane review only included two RCTs from Kenya, and concluded text messages at a weekly interval are effective in enhancing adherence to ART. 23 Another review incorporated three RCTs and used SMS or text message intervention only. 24 Both reviews represented results from Africa and may not be applicable to other settings. Further, a vast majority of these reviews only evaluated a single digital health as an intervention, which is SMS or text messages. 23,24 A review by Shah et al., which involved various types of digital health interventions, including SMS or text messages, voice calls, mobile applications, and mixed methods, found the effect of daily SMS or text messages on ART adherence when measured as standard mean difference. 25
The review findings resulted from a meta-analysis on two studies utilizing similar measure of adherence [Medication Event Monitoring System (MEMS)]. Due to the various interventions included, the review highlighted the importance of combination approaches in improving ART adherence. This finding is consistent with the conclusions of Quintana et al.'s 44 and Amankwaa et al.'s 45 systematic reviews, which explored the benefits of multiple approaches. Yet, both reviews covered a wide range of study designs. 44,45 A recent review found the effect of digital health on ART adherence was inconclusive and restricted in low- and middle-income countries. 26 This review offers a valuable contribution by involvement of the new PLHIV and MSM key population in the included studies. In addition, it encompasses evidence from both existing reviews and newly published studies that were not included in earlier systematic reviews.
This systematic evaluation utilized different approaches compared to previously published works. 25,26,44,45 First, ART adherence was the main focus. Thus, the included studies should document the type of adherence used and the outcome of ART adherence assessment. Second, this review may represent a more comprehensive global perspective ranging from developed to low-income countries. Third, this review concentrated only on RCTs that represented high-quality studies. Finally, this review included studies utilizing the mobile application as digital health, in addition to SMS or text messages and IVR-based interventions, which were reported previously.
Although this study has highlighted several important findings, a few limitations may have influenced the overall conclusion. These limitations include only English articles were evaluated, which limit the comparison to other studies in different languages and populations. In addition, variation of adherence measures was used such as pill count, visual analog scale (VAS), MEMS caps, and real-time adherence monitoring. Moreover, two studies used self-reported data, which are considered a less sensitive measure of adherence than MEMS and can lead to overestimation of adherence.
Overall, these available data did not demonstrate any benefit of digital health as a sole intervention in enhancing ART adherence among PLHIV. However, combination approaches showed significant benefits in improving adherence. New innovative approach in adopting digital health using combination method is needed to prove its effectiveness. This review highlighted the lack of studies using mobile applications and some key populations, such as MSM, substance abuse, or chemsex. Future studies evaluating the combination of mobile applications with other technologies are needed to be explored in larger studies with extended follow-up.
Footnotes
Authors' Contributions
M.F.C.P.: Writing—original draft (lead); formal analysis (lead); and writing—review and editing (equal). M.M.B.: Conceptualization (supporting); methodology (supporting); and writing—review and editing (equal). F.I.: Conceptualization (lead); methodology (lead); original draft (supporting); and writing—review and editing (equal).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.