
Abstract
Following the World Health Organization's guidelines for rapid antiretroviral therapy (ART) initiation [≤7 days after human immunodeficiency virus (HIV) diagnosis], China implemented Treat-All in 2016 and has made significant efforts to provide timely ART since 2017. This study included newly diagnosed HIV adults from Tianjin, China, between 2016 and 2022. Our primary outcome was loss to follow-up (LTFU) at 12 months after enrollment. The secondary outcome was 12-month virological failure. The association between rapid ART and LTFU, as well as virological failure, was assessed via Cox regression and logistic regression. A total of 896 (19.1%) of 4688 participants received ART ≤7 days postdiagnosis. The rate of rapid ART has increased from 7.5% in 2016 to 33.3% by 2022. The rapid ART group had an LTFU rate of 3.3%, as opposed to 5.0% in the delayed group. The rapid ART group had a much reduced virological failure rate (0.6% vs. 1.8%). Rapid ART individuals had a reduced likelihood of LTFU [adjusted hazard ratio: 0.65, 95% confidence intervals (CI): 0.44–0.96] and virological failure (adjusted odds ratio: 0.35, 95% CI: 0.12–0.80). The real-world data indicated that rapid ART is practicable and beneficial for Chinese people with HIV, providing evidence for its widespread implementation and scaling up.
Introduction
Since the development of antiretroviral therapy (ART), the worldwide pandemic of human immunodeficiency virus (HIV)/acquired immune deficiency syndrome (AIDS) has been under control. The World Health Organization's (WHO) 2015 treatment guideline advised starting ART for all people with HIV (PWH). 1,2 Further, because of the advancement of more efficient and secure ART, patients indicated virological suppression, increased immune recovery, reduced morbidity and mortality, improved overall quality of life, and reduced later HIV transmission. 3 –5
Nevertheless, new HIV infections continue to occur despite programs such as Treatment as Prevention, Preexposure Prophylaxis, and Ending the HIV Epidemic. This was particularly evident in certain populations at increased risk and geographical regions, such as in men who have sex with men (MSM). 6 HIV incidence may be decreased by initiating ART as soon as possible, ideally at the time of diagnosis. In 2017, WHO updated its guidelines based on the results of clinical trials on rapid initiation of ART, 7,8 which recommend initiating ART within 7 days after getting an HIV diagnosis, or on the same day for those who are ready. 9 However, If cryptococcal meningitis or tuberculosis is confirmed, ART should be postponed to prevent fatal infections from progressing. ART initiation should be delayed if cryptococcal meningitis or tuberculosis is suspected or proven to prevent deadly paradoxical infections from worsening. 9
In 2003, the Chinese government established the National Free Antiretroviral Therapy Programme (NFATP), which significantly enhanced the availability of ART to PWH. 10 By the end of 2020, 978,138 (92.9%) of 1053 million Chinese PWH were getting ART. 11 The NFATP initially advised ART initiation for PWH with <200 cells/μL CD4+ T cell count or stage 4 (AIDS). However, the CD4 count-based ART eligibility criteria incresed to 350 cells/μL in 2011, and 500 in 2015, and from June 2016, China has adopted a Treat-All policy that recommends immediate ART irrespective of CD4 level, following worldwide guidelines. 12
In addition, in China, many projects have encouraged early HIV diagnosis, more rapid treatment initiation, and extended support for patients by expanding testing and therapeutic options and streamlining the care process. The most recent guidelines (2021 edition) in China have recommended rapid initiation or same-day ART in PWH if possible. 13
The WHO rapid ART initiation recommendations were primarily based on the results of randomized trials; however, broad acceptance of rapid initiation has offered the possibility that enables observational studies to examine the real-life implications of this strategy. Numerous observational studies indicate a possible causal relationship between rapid ART initiation and dropout from care, which contradicts the findings of clinical trials; 14 –17 most of these studies were conducted in Africa. Further, between 2011 and 2015, two nationwide cohort studies in China revealed that immediate ART (within a month after HIV diagnosis) significantly reduced mortality, attrition from care, and virological failure in PWH. 18,19
Additional large-scale research on the impact of rapid ART is required to understand treatment outcomes, particularly under China's Treat-All policy. Therefore, this investigation sought to assess the relationship between rapid ART initiation, loss of follow-up, and virological failure within PWH in a large cohort from Tianjin, China.
Methods
Study setting and design
This is a retrospective observational study for adults who were newly diagnosed with HIV infection and received initial ART between June 2016 and December 2022 in Tianjin urban district, a Chinese municipality with >13 million people and a low HIV prevalence (PWH >7000). Exclusion criteria included individuals who (1) were <18 years, (2) had <1 year between enrollment and most recent visit, (3) had previous treatment experience, (4) never initiated ART, and (5) transferred to another health care facility. The study cohort eligibility criteria are shown in Fig. 1.
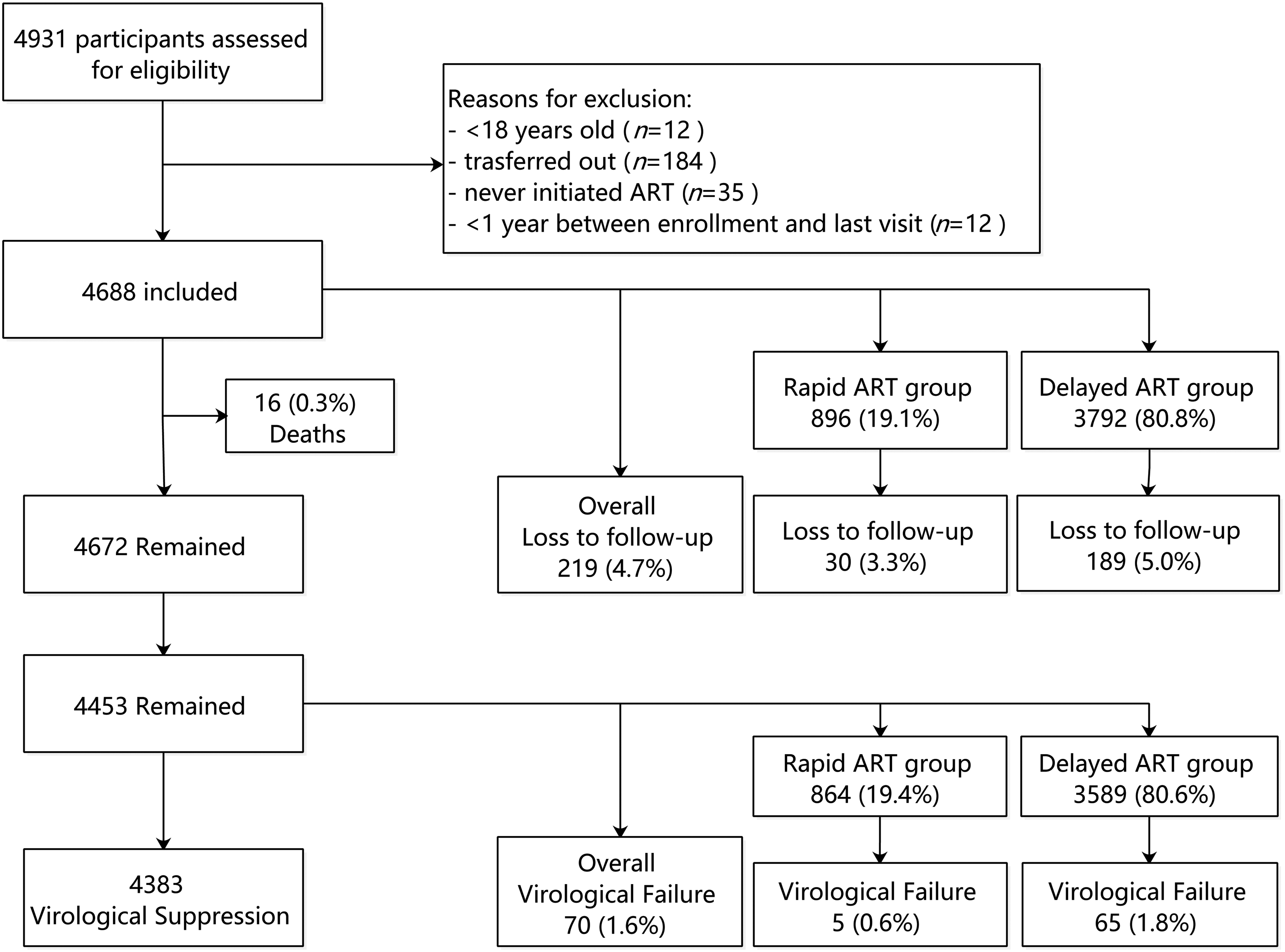
Flow chart of study cohort eligibility criteria. All newly diagnosed persons with HIV who started ART during June 2016 and December 2022 were screened. Participants were divided into the rapid ART (ART initiation ≤7 days of HIV diagnosis) and delayed ART (ART initiation >7 days postdiagnosis) groups. Treatment outcomes included loss to follow-up and virological failure (HIV RNA ≥200 copies/mL) at 12 months after enrollment. ART, antiretroviral therapy; HIV, human immunodeficiency virus.
Because of the lack of available procedures for rapid ART initiation under China's Treat-All policy, their physician initiated ART when the patient felt ready, after assessing their psychological and clinical preparation and taking other clinical factors into account. The China Centers for Disease Control and Prevention (CDC) handles HIV/AIDS surveillance along with diagnosis, whereas health care facilities offer ART and follow-up. 12 Therefore, same-day ART (on the same day of HIV diagnosis) was not accessible to PWH who came to the CDC, as ART was provided by health care facilities.
Thus, here, the association between rapid ART initiation (defined as starting ART within 7 days after diagnosis) and treatment outcomes was assessed rather than same-day initiation. Delayed ART initiation was defined as starting ART >7 days after diagnosis. Routine follow-up visits were arranged at 1, 2, and 3 months after the start of ART, and every 3 months afterward. Further, free CD4 count screening was carried out at the start of treatment and subsequently every 6 months, whereas free HIV viral load measurement was performed annually after starting ART.
The study was approved by the Human Medical Ethics Committee of Tianjin Second People's Hospital and followed the Helsinki Declaration. At the time of diagnosis, informed consent was acquired from all PWH, allowing the use of their clinical records.
Data collection
Data were obtained from the China CDC's HIV/AIDS information management system and the hospital's computerized medical records. Variables acquired included gender, age, marital status, HIV diagnosis dates, transmission routes, viral load, baseline CD4 count, tuberculosis treatment status (ever) during follow-up, entry into HIV care, ART prescription date, initial ART regimen, date of transfer to other health care facilities, and deaths. The initial ART regimen is defined as the antiretroviral medications given at the onset of ART. In addition, baseline CD4 count was assessed using test data from 3 months before ART initiation.
Outcome measures
The primary treatment outcome was loss to follow-up (LTFU), defined as the patient's (who had not died or been transferred) absence to contact the health center after 90 days from the last drug pick-up or clinical visit in the 12 months after enrollment. 16,20 The virological failure at 12 months post-ART initiation (≥200 copies/mL) was also evaluated.
Statistical analysis
For continuous variables, pre-ART characteristics were reported with medians and interquartile ranges (IQRs), whereas for categorical variables, frequencies and proportions were used. Differences in continuous variables were evaluated using Kruskal–Wallis tests, and those in categorical variables were evaluated by chi-square tests. Further, Kaplan–Meier estimators were employed to determine the LTFU time and compare the timing of ART initiation (rapid vs. delayed ART). Using univariate and multivariate Cox regression models, the determinants of LTFU at 12 months after enrollment were evaluated.
Moreover, the hazard ratio (HR) and adjusted hazard ratio (aHR) were reported with 95% confidence intervals (CIs). In addition, univariate and multivariate logistic regression models were employed to investigate factors associated with rapid ART initiation and virological failure, yielding odds ratio and 95% CI. All p values are two sided, where p < 0.05 was considered statistically significant. All analyses were performed using SPSS software version 26.0 (SPSS, Chicago, IL).
Results
Characteristics of the participants
In total, 4688 participants who underwent HIV screening were enrolled. Table 1 represents the detailed characteristics of the enrolled participants. A total of 94.9% of participants were male (4449/4688), and the median age was 37 years (IQR: 31–48), where 57.6% of participants were aged 30 to 49 years. At enrollment, the median CD4 count was 292 cells/μL (IQR: 157–431), with 31.9% of participants indicating <200 cells/μL. About two-thirds (67.2%) of individuals acquired HIV through MSM, and nearly half (55.8%) were single. Of all, 2.1% of patients were diagnosed with tuberculosis during follow-up, and 67.6% received free government-sponsored drugs. A total of 896 (19.1%) patients started ART within 7 days after diagnosis (rapid ART group), whereas 3792 (80.9%) started later (delayed ART group).
Demographic Details and Other Characteristics of Participants
ART, antiretroviral therapy; IQR, interquartile ranges; MSM, men who have sex with men; TB, tuberculosis.
In the rapid ART group, the median time from diagnosis and ART initiation was 4 days (IQR: 2–6), whereas for the delayed ART group, it was 22 days (IQR: 14–56, data not shown). Rapid ART group showed lower baseline CD4 counts [269, IQR (124–401) cells/μL] than delayed ART initiators [299, IQR (165–436) cells/μL]. Low CD4 counts were more prevalent in the rapid ART group (<200 cells/μL: 36.7% vs. 30.7%). Further, in the rapid ART group, more individuals indicated MSM as their transmission route (71.7% vs. 66.1%), whereas most delayed ART group participants reported an unknown route (11.4% vs. 7.5%). In the rapid ART group, there were fewer tuberculosis cases (1.2% vs. 2.3%) and a few participants received free government-sponsored HIV medications (48.2% vs. 72.7%).
Trends in rapid ART initiation and time from HIV diagnosis to treatment initiation
As Fig. 2A shows, in 2016, 7.5% of participants in Tianjin began ART within 7 days after diagnosis. The percentage of rapid ART individuals exhibited a consistent upward trend, peaking at 34.6% in 2021, before declining marginally to 33.3% in 2022. The median time from diagnosis to treatment initiation declined from 26 days (IQR: 15–132) in 2016 to 11 days (IQR: 6–23) in 2021, before mildly increasing to 12 days (IQR: 6–28) in 2022 (Fig. 2B).
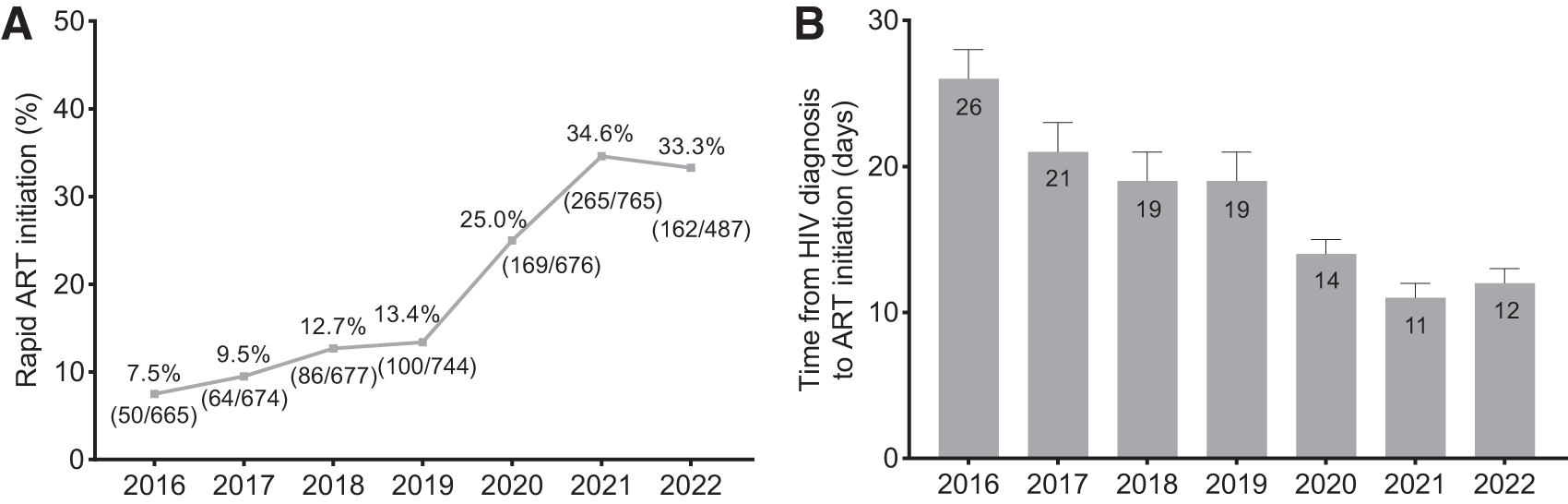
Trends in rapid ART initiation
Factors associated with rapid ART initiation
The results of logistic regression analyses carried out to identify the risk variables associated with rapid ART are presented in Fig. 3. Rapid ART was not as frequently reported in PWH with baseline CD4 counts of 350–499 [adjusted odds ratio (aOR): 0.75, 95% CI: 0.60–0.93, p = 0.009] and ≥500 (aOR: 0.74, 95% CI: 0.58–0.94, p = 0.013) than those with <200 CD4 counts. Further, it was also less common in individuals with an unknown route of infection than those with heterosexual contact (aOR: 0.69, 95% CI: 0.50–0.95, p = 0.024) and tuberculosis (aOR: 0.40, 95% CI: 0.20–0.73, p = 0.005). In addition, rapid ART was more frequent in patients who took Medicare/self-paid medications (aOR: 2.78, 95% CI: 2.40–3.23, p < 0.001) than those who chose free government-sponsored drugs.
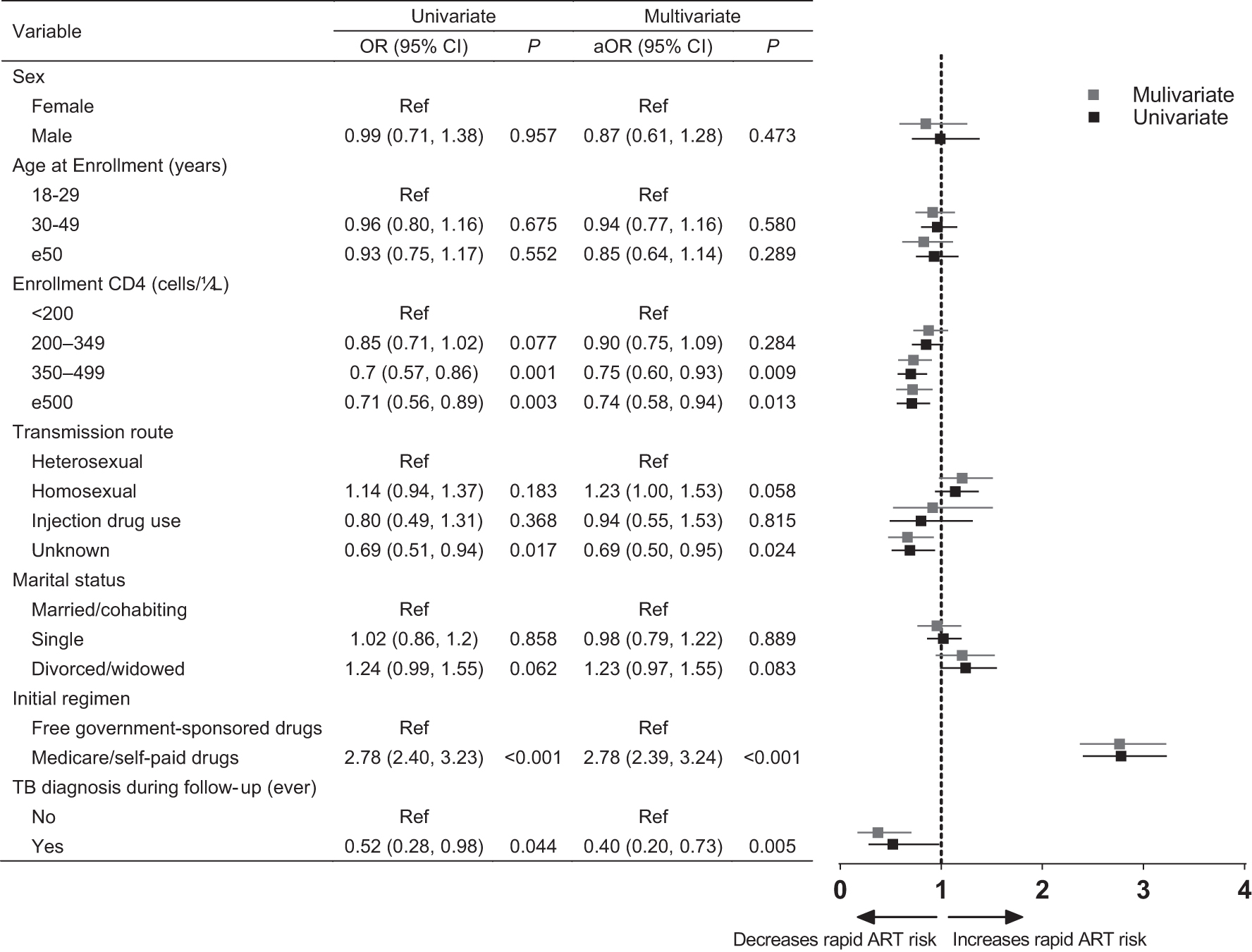
Factors associated with rapid ART initiation according to logistic regression model. aOR, adjusted odds ratio; ART, antiretroviral therapy; CI, confidence interval; MSM, men who have sex with men; OR, odds ratio; TB, tuberculosis.
Loss to follow-up
A total of 219 participants (4.7%) indicated LTFU, with a median duration of 181 days (IQR: 121–253). Further, 3.3% (n = 30) of rapid ART individuals were identified to be LTFU after a median of 215 days (IQR: 180–266). Among delayed ART initiators, LTFU was observed in 189 (5.0%) cases, with a median duration of 121 days (IQR: 96–246) (Fig. 1). The incidence rate for LTFU was notably lower in the Kaplan–Meier plots for the rapid ART cohort than in the delayed ART cohort (Fig. 4, Log-rank p = 0.035). Moreover, the rapid ART group showed a decreased risk of LTFU compared with the delayed ART group (HR: 0.66, 95% CI: 0.45–0.97, p = 0.037), also confirmed in the multivariable model (aHR: 0.65, 95% CI: 0.44–0.96, p = 0.029) that controlled for age, gender, enrolment CD4 count, transmission route, marital status, initial regimen, and tuberculosis diagnosis during follow-up (Table 2).
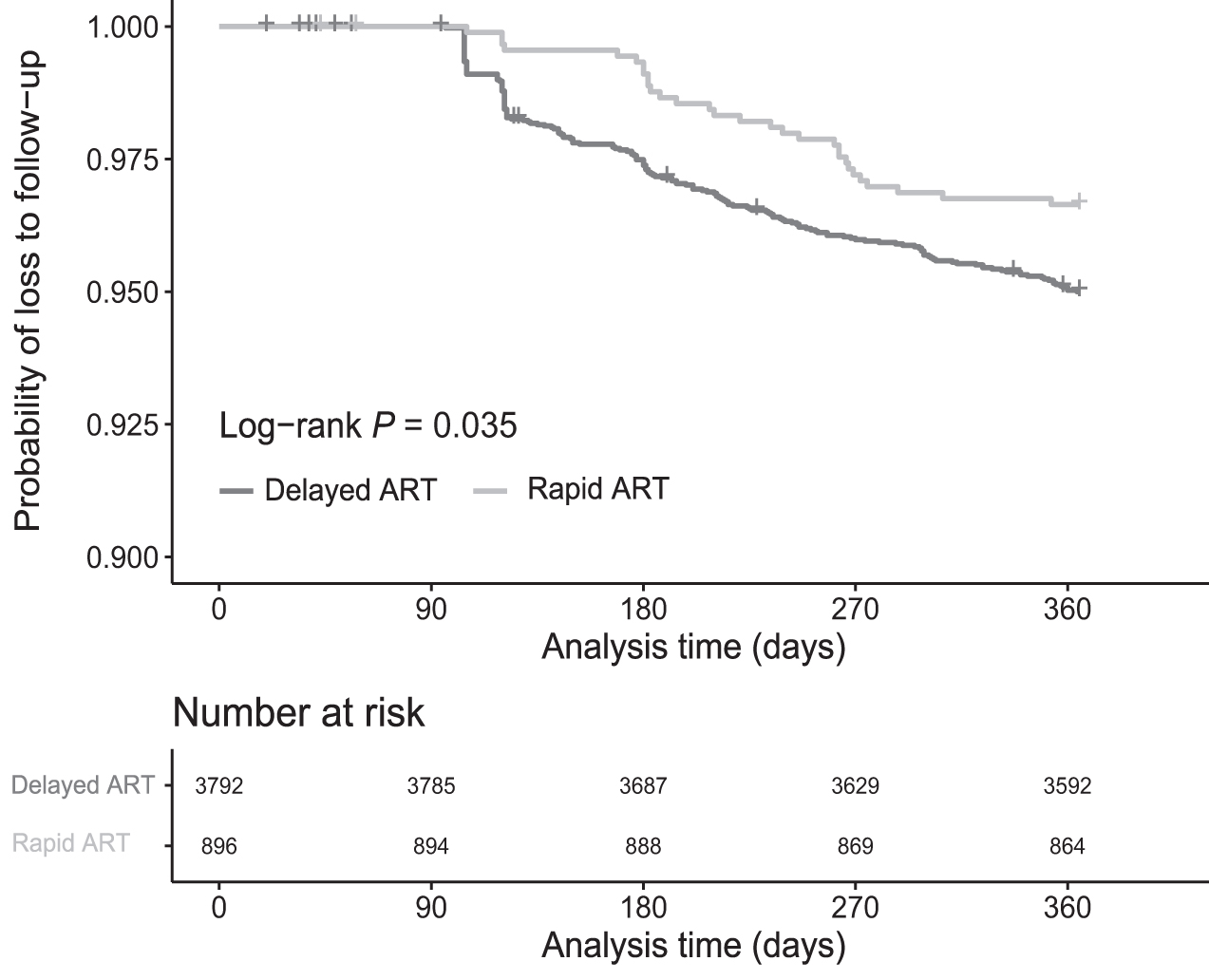
Kaplan–Meier survival curve of loss to follow-up in ART initiation group. (Rapid ART, ART initiation ≤7 days postdiagnosis; delayed ART, ART initiation >7 days postdiagnosis). ART, antiretroviral therapy.
Factors Associated with Loss to Follow-Up Within 12 Months After Enrollment
aHR, adjusted hazard ratio; ART, antiretroviral therapy; CI, confidence intervals; HR, hazard ratio; MSM, men who have sex with men; TB, tuberculosis.
In addition, it was observed that LTFU was greater among injection drug users (aHR: 2.40, 95% CI: 1.37–4.18, p = 0.002; injection drug use vs. heterosexual), single individuals (aHR: 1.50, 95% CI: 1.01–2.22, p = 0.044; single vs married/cohabiting), and those who take Medicare/self-paid medications (aOR: 1.37, 95% CI: 1.03–1.82, p = 0.030) compared with those who chose free government-sponsored drugs.
Virological failure
Among the 4453 people who remained alive, eliminating individuals who died or were LTFU, 70 had viral load ≥200 copies/mL. The total rate of virological failure was 1.6%. About 0.6% (5/864) of rapid ART participants were not virally suppressed compared with 1.8% (65/3589) participants who initiated treatment >7 days after diagnosis (Fig. 1, p = 0.010). Further, rapid ART individuals had a reduced probability of virological failure than delayed ART initiators (aOR: 0.35, 95% CI: 0.12–0.80, p = 0.026) (Table 3).
Factors Associated with Virological Failure at 12 Months Postantiretroviral Therapy Initiation
aOR, adjusted odds ratio; ART, antiretroviral therapy; CI, confidence intervals; MSM, men who have sex with men; OR, odds ratio; TB, tuberculosis.
Discussion
This research indicated that after China implemented the Treat-All policy, there was a notable and sustained decline in ART initiation time in Tianjin. Between 2016 and 2022, the median duration from an HIV diagnosis to treatment initiation dropped from 26 to 12 days. When PWH who received delayed ART were compared with those who received rapid ART, the latter had a lower likelihood of LTFU and virological failure at 12 months afterenrollment.
Here, 19% of PWH initiated treatment within 7 days of diagnosis, whereas 81% initiated ART after 7 days had passed. There are several complex reasons for these unexpected delays.
In 2016, China removed CD4+ count-guided ART eligibility and established the notion of “rapid initiation” in its HIV/AIDS guidelines in 2021. In China, HIV diagnosis/testing and treatment are conducted by the CDC and medical facilities independently, which is a structural obstacle to integrating care. The former standard-of-care pathway for initiating ART encompasses several clinic visits, separate blood tests, and long waiting periods. In certain regions, confirmatory testing is only provided to people who test HIV positive in hospital settings (43%). 21 Moreover, a recent study found that ∼30% of gay, bisexual, and other MSM in China did not test for HIV during the coronavirus disease 2019 (COVID-19) pandemic. 22
Consequently, there is increased loss of follow-up, diagnostic delays, incomplete clinical evaluation, and delayed treatment initiation. 23 The Chinese government has undertaken various attempts to simplify the HIV care cascade, offer timely ART, and avoid excessively high mortality. 23,24 Further, experts suggested implementing an integrated care cascade by combining diagnostic services, treatment, and management in HIV health care facilities to provide comprehensive care. 12 The streamlining and avoidance of unnecessary clinic visits might assist PWH in overcoming financial and logistical obstacles to treatment.
However, regional inequalities in the HIV epidemic, economic growth, and medical services could impede the acceptance and implementation of rapid ART policy. Based on the regional implementation of the integrated care cascade in Tianjin, it is evident that more work is required to enhance the linkage of care.
Our analysis revealed that PWH with high CD4 counts (≥500 cells/μL) were less likely to get (rapid) ART, which is in line with a recent study from Guangdong. 25 PWH with a delayed diagnosis had a higher probability of presenting with advanced disease or receiving greater encouragement from health care providers to start ART. However, due to the retrospective nature of this study, many factors such as educational level, income, and active HIV testing that might influence ART initiation were not included.
Consistent with findings from randomized trials, 26,27 thisstudy indicated that newly diagnosed HIV individuals who were offered rapid ART initiation had substantially lower LTFU and achieved increased HIV suppression within the first year when compared with delayed ART patients. A recent meta-analysis indicated that rapid ART was better than delayed therapy in continuing care for at least 8 months. 28 Several observational studies conducted in South Africa, however, indicated that rapid-start ART was linked to poorer rates of retention in care. 14,20,29 This might be because of factors such as the individual's socioeconomic status, level of literacy, and concurrent mental, physical, and social health conditions. 30
This study indicates the advantages of rapid ART over delayed care in terms of viral suppression at 12 months. Although rapid ART has been indicated to not achieve long-term HIV suppression, it is contributing to the UNAIDS 95-95-95 targets in low-/middle-income countries. Therefore, the timing of ART initiation should not be the only focus as it might be because of the result of inadequate care provision, relatively ineffective antiretroviral drugs, poor retention/linkage of care, and restrictive access to viral load monitoring. 30 Overall, the real-world data in this study prove that rapid initiation of ART is practically pertinent and beneficial for Chinese PWH.
It is noteworthy that rapid ART initiation was more prevalent among Medicare/self-paid medication users; however, their LTFU risk was also higher than those who used free government-sponsored medications. During this study, the standard first-line regimen administered by the NFATP was tenofovir+lamivudine+efavirenz. 31 Free second-line treatment substitutes efavirenz with lopinavir/ritonavir. In 2009, raltegravir became the first HIV/AIDS integrase strand transfer inhibitor in China, followed by dolutegravir, elvitegravir, and bictegravir in 2015, 2018, and 2019, respectively. 32 Further, China introduced new non-nucleoside reverse-transcriptase (rilpivirine and doravirine) and protease (darunavir/cobicistat) inhibitors in 2019 and 2021.
However, the high cost and the specifications of local government reimbursement limited the use of these new antiretroviral drugs in most regions. Therefore, >90% of PWH in China get free medications supported by the government. Many PWHs buy cheaper generic versions of their physicians' prescriptions from generic manufacturers or specific channels. However, since 2020, Chinese medical insurance has covered the new antiretroviral medications at lower prices, whereas Tianjin municipal health insurance covers 45–90% of the cost, allowing more PWH to acquire Medicare-brand drugs. Individuals who paid for brand or generic drugs themselves may not visit medical facilities as often as those who get free government-sponsored medications for a 3-month drug pick-up. Therefore, there was a higher risk of LTFU among Medicare/self-paid drug users than free drug users.
This study has several limitations. (1) There is a selection bias as those PWH who never began ART were not included in our study. (2) Certain factors were not examined in this study such as societal, cultural, financial, and personal factors, such as acceptability and willingness to get ART, as well as the health care system and provider factors that may affect the practicality and acceptance of rapid ART initiation (e.g., levels of staffing, skills, facilities, and equipment), which vary across settings. Moreover, the emergence of the COVID-19 epidemic might have affected the compliance of HIV individuals receiving ART, especially in 2022. Lastly, the generalizability of these results in different settings might be limited due to factors such as the vastness of China, the unequal distribution of health care resources, and the HIV pandemic.
In summary, a substantial increase was observed in the rapid ART initiation of newly diagnosed PWH under the national Treat-All policy in Tianjin, China, indicating that the WHO's guidelines for rapid ART after HIV diagnosis have been progressively implemented and scaled up. Further, rapid ART patients indicated a reduced LTFU risk and virological failure, which demonstrated the acceptability, viability, and efficacy of rapid ART strategy in a routine clinical setting. Further surveillance of outcomes in routine settings is necessary to precisely assess the programmatic effects of rapid ART initiation.
Footnotes
Acknowledgments
The authors thank the clinicians and data staff from the Tianjin Second People's Hospital who made this analysis possible.
Ethical Approval and Informed Consent
The study was approved by the Human Medical Ethics Committee of Tianjin Second People's Hospital and followed the Helsinki Declaration.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Authors' Contributions
Conceptualization: H.X. and P.M. Investigation: H.X., Y.W., D.Z., and L.L. Data acquisition and curation: H.X., L.L., D.Z., L.G., and Y.W. Writing—original draft: H.X. Writing—review, editing, and revision: H.X. and P.M.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Natural Science Foundation of China (82002136). the Health Science and Technology Project of Tianjin Health Commission (TJWJ2021MS033), and the Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-059B). The funders had no role in the study design, collection, analysis, and interpretation of the data; in article preparation; or the decision to publish.