
Abstract
Despite the availability of pre-exposure prophylaxis (PrEP), Latino sexual minority men (LSMM) continue to experience disparities in PrEP uptake and subsequently, HIV vulnerability. Social network norms are an underutilized solution to increase PrEP uptake. We used a peer influence model (network autocorrelation model) to examine the role of social network descriptive norms (i.e., actual behaviors) surrounding PrEP use. A total of 11 sociocentric networks of 13 friends (n = 143 LSMM) were recruited into our study from 2018 to 2019 in South Florida. Most participants were in PrEP pre-contemplation (n = 44), and almost one-third of our sample were using PrEP (n = 38). Three network autocorrelation models were estimated using an empirically informed Bayesian analysis. We found a positive association between participants’ Motivational PrEP Cascade (MPC) position and their network members’ (friends’) cascade position based on three different measures of connection even when accounting for PrEP knowledge: friendship (ρ = 0.22; 95% CIa = 0.01–0.42), emotional closeness (ρ = 0.24; 95% CI = 0.03–0.44), and frequency of interaction (ρ = 0.22; CI = 0.03–0.42). Our findings highlight that an individual’s progress in the MPC may be influenced by their network members’ progress in the MPC, suggesting that LSMM using PrEP may serve as role models to their peers for PrEP use due to descriptive norms. Our findings further suggest that PrEP interventions for LSMM along the MPC can be implemented at the social network level.
Introduction
In 2021, approximately 1.1 million individuals in the United States were living with HIV. 1 ,Of particular concern is the disproportionate burden of HIV-related morbidity and mortality among racial, ethnic, sexual, and gender minority subpopulations. In 2021, Latino individuals and men who have sex with men accounted for 29% and 67%, respectively, of the nearly 36,000 new HIV infections in the United States. 2 If current rates persist, one in five Latino sexual minority men (LSMM) will be diagnosed with HIV by age 49 years. 3 In Miami-Dade County, Florida, a domestic epicenter of the HIV epidemic, the HIV incidence rate was 37.3 per 100,000 in 2019 and 30.3 per 100,000 in 2021 among persons aged ≥13 years. 4 Latino individuals represented 60.4% and sexual minority men (SMM) represented 69.8% of new diagnoses in MDC in 2021. 4
Pre-exposure prophylaxis (PrEP) is an effective biomedical preventive tool that reduces the risk of infection by over 99% when adherence is followed. 5 –7 However, LSMM have low PrEP uptake despite having high PrEP awareness and acceptability. 8 Despite many Latino men qualifying for PrEP, there continues to be a large discrepancy in the percentage of these men who actually receive a PrEP prescription compared to White men. 9 The Motivational PrEP Cascade (MPC) 10 can be used to understand this discrepancy between awareness and uptake. This framework, informed by the Transtheoretical Model of Change and the Theory of Planned Behavior, 11,12 includes five stages to describe an individual’s willingness and intentions for PrEP uptake, engagement, and persistence. The precursory phase for entry into the cascade is objective identification, which is a combination of an individual’s awareness and perception of HIV risk, knowledge of HIV status, and clinical indication for PrEP based on current Centers for Disease Control and Prevention (CDC) PrEP guidelines. Individuals eligible for PrEP may then move forward or backward through the following stages: PrEP precontemplation (unwilling to take PrEP or do not perceive themselves to be an appropriate candidate for PrEP), PrEP contemplation (willing to take PrEP but no means or plans to do so), PrEParation (have plans and means to obtain PrEP but have not yet received PrEP prescription), PrEP action (have spoken to doctor and obtained PrEP prescription), and PrEP maintenance (adhering to PrEP and following PrEP care guidelines). 10
Recent studies have utilized the MPC to characterize PrEP outcomes among SMM to identify where along the cascade individuals may be lost to care or stop progressing. 10,13 –16 Together, these studies consistently suggest that most PrEP-eligible individuals do not progress past the early stages of the MPC. This may be a limitation of the MPC as it gives little attention to the social context and subjective norms (i.e., beliefs of others and the desire to comply with others) that may impact an individual’s willingness and intentions to engage in PrEP care. 17 Thus, we sought to fill this gap by using social network methods to examine the importance of social norms and peer influence on LSMM progression within the MPC.
Individuals can be considered within their social context. Social network support and social network connectedness have been shown to reduce barriers to engaging with PrEP and other HIV prevention services. 18 –21 For example, LSMM may be more likely to engage in PrEP care if they hear about PrEP from a social network member (i.e., a friend or another LSMM). 22 Qualitative research suggests that LSMM’s PrEP use is also swayed by social norms, including descriptive norms or observed behaviors within a social network. 17 Greater social network connectedness to the SMM community and Latino group social network membership endorsement are also associated with PrEP initiation. 23 Furthermore, SMM with more social network connections are more likely to engage in PrEP services, necessitating the importance of considering individuals within their social context. 21 Thus, to examine the influence of the social context, or peer influence, social network analyses such as the autocorrelation model can be used. 24 To our knowledge, the present article is one of the first to explore peer influences of an individual’s MPC position, focusing on a population at high vulnerability to HIV (LSMM) and using a Bayesian sociocentric network approach. The overall aim of the present analysis is to characterize LSMM’s stage in the MPC and describe how their stage relates to the stages of those in their friendship network using the peer influence/network autocorrelation model. The underlying mechanism of social influence in the context of this study is hypothesized to be communication. Previous studies have explored discussions and encouragement surrounding PrEP among networks of friends and sexual partners and the relationship of these discussions with various dyadic characteristics (i.e., closeness, frequency of contact). 25 –28 This work highlights the need for additional analyses to further investigate PrEP communication within social networks as a mechanism for social influence in increasing uptake, adherence, and persistence in biomedical HIV prevention services.
Methods
Participants, setting, and recruitment
Data for this study were collected from August 2018 to January 2020. A total of 11 networks composed of 13 individuals (n = 143 LSMM) were recruited into our cross-sectional social network study. We partnered with a South Florida community-based organization (CBO) that prioritizes LSMM sexual health to recruit participants using a respondent-driven sampling (RDS) approach. A detailed description of our RDS recruitment approach can be found elsewhere. 25 –27,29 –31 To summarize the RDS approach, 11 participants were recruited as seed individuals, and each seed referred their friends to the study, who in turn referred their friends to the study. Participants met the following inclusion criteria: identifying as Latino, self-reporting HIV-negative status, and having recommended indications for PrEP use based on the CDC guidelines. 32 Study staff obtained informed consent from participants and then conducted a 2-hour long assessment in English or Spanish using tablets and paper-based sociocentric surveys.
Measures
Sociodemographic measures included age (in years), race (White, Black, Multi-racial, Another race), marital status (single, married), education (high school degree or less, some college, college degree, or more), and county of residency (Miami-Dade County, Broward County). Knowledge of PrEP effectiveness was measured with the question, “How effective is PrEP when taken as prescribed in preventing HIV?” with options, “I don’t know,” “Less than 50% effective,” “Less than 75% effective,” “Less than 90% effective,” and “90% or more effective.” Participants who selected the option “90% or more effective” were scored “1,” while all other responses were scored “0.”
Stage on the MPC was calculated using Parson’s MPC approach, 10 with participants placed based on their current PrEP use at six stages. In order, the stages were: objective identification (this included all participants within our sample as they were identified as being at high vulnerability to HIV in accordance with CDC guidelines), 33 PrEP precontemplation (unwilling to take PrEP), PrEP contemplation (willing to take PrEP but no means or plans to do so), PrEParation (have plans and means to obtain PrEP but have not yet received PrEP prescription), PrEP action (have been prescribed PrEP), and PrEP maintenance (adherence to PrEP in the past 3 months).
Network-level measures included declared friendship with another participant in their recruited network (a binary indicator), their emotional closeness to the declared friends (a 5-point scale from 0 = “Not at all close” to 5=“Extremely close”), and their frequency of interaction with the declared friends (a 4-point scale from 0=“Never” to 4=“Almost every day”).
Descriptive analysis
We assessed associations between sociodemographic characteristics and MPC stages using chi-squared tests, one-sample t-tests, and analysis of variance tests. We constructed three adjacency matrices of the connections between respondents and friends based on friendship, emotional closeness, and interaction frequency. We used each of these in a network autocorrelation model to assess the relationship between a respondent’s stage on the MPC and the positions of the respondent’s friends on the cascade. Each model was estimated with Bayesian methods specifying an informed prior distribution for the autocorrelation coefficient
Three models explore variations in measures of contact with associates. Model A examines an individual’s cascade position and the weighted average of their friends’ cascade positions, where each friend has the same weight. Model B weighs the positions of associates by the level of emotional attachment, so the positions of associates to whom the individual has close emotional attachment have greater weight. Model C weighs the positions of associates by the frequency of interaction; the positions of associates to whom the individual has frequent interaction have greater weight. In each model, the individual’s PrEP knowledge score is included as a covariate. The assumed prior distribution of the autocorrelation coefficient is based on Dittrich, Leenders, and Mulder’s work, in which they explored peer influence in more than 50 published studies, finding a mean for the distribution of 0.36, with a standard deviation of 0.19. 38
The network effects autocorrelation model is expressed by the equation:
In this equation,
Ethical approval
Each participant received a $50 gift card as compensation for their time during interviews and a $10 gift card for each friend referral who enrolled in the study. Study staff obtained written informed consent from participants. Ethical approval was obtained from the University of Miami Institutional Review Board. We used the STROBE guidelines to report our study findings. 42
Results
Among seeds, five were current PrEP users and six were not using PrEP at the time of data collection. Most participants were aged between 25 and 29 years, White (71%), and single (87%). Additional descriptive statistics of participants can be found in Table 1 and elsewhere. 25 –27,29 –31 Most participants were in the PrEP pre-contemplation stage (n = 44), and almost one-third of our sample were using PrEP (n = 38). The MPC visualized as a stacked bar plot can be found in Figure 1.
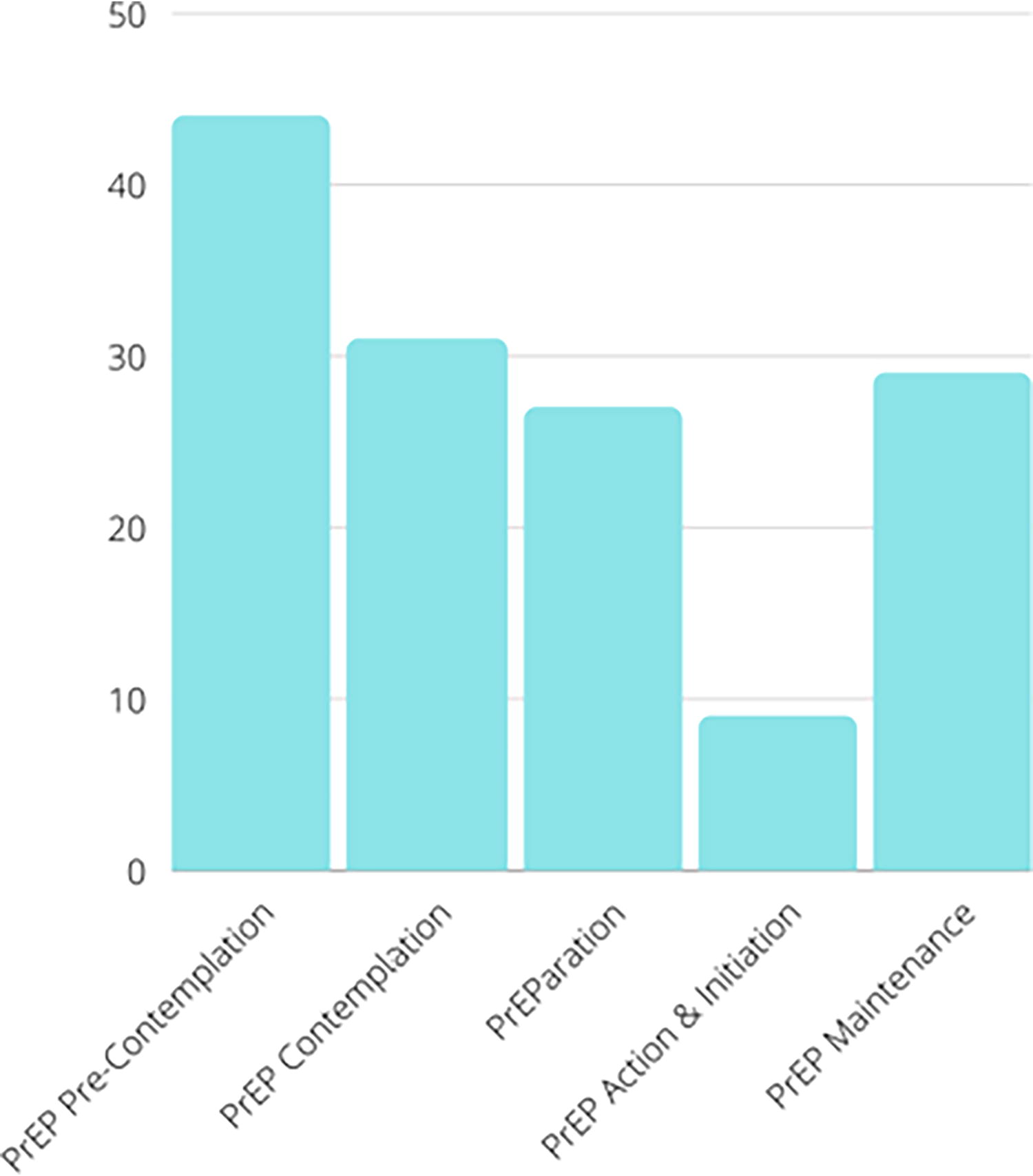
Bar plot of Motivational PrEP Cascade stage of Latino sexual minority men in South Florida, n = 140. PrEP, pre-exposure prophylaxis.
Sociodemographic Information of Latino Sexual Minority Men at Risk of HIV in South Florida, Stratified by Motivational PrEP Cascade Stage
p < 0.05.
PrEP, pre-exposure prophylaxis.
A visualization of the LSMM social networks and their stage along the MPC can be found in Figure 2. The color of the node denotes the participants’ stage in the MPC, with darker colors indicating further progression. The shape of the node denotes the seed of the network (i.e., the first person recruited for that network) and is visualized as a square with a dark border, and participants who are not seeds are visualized as a circle with a light gray outline. A line between nodes indicates a declared friendship. As depicted in Figure 2, all networks contain individuals at different stages in the MPC. However, the density varies across the networks, with some networks having ties among every friend and others with only a few friends who know one another.
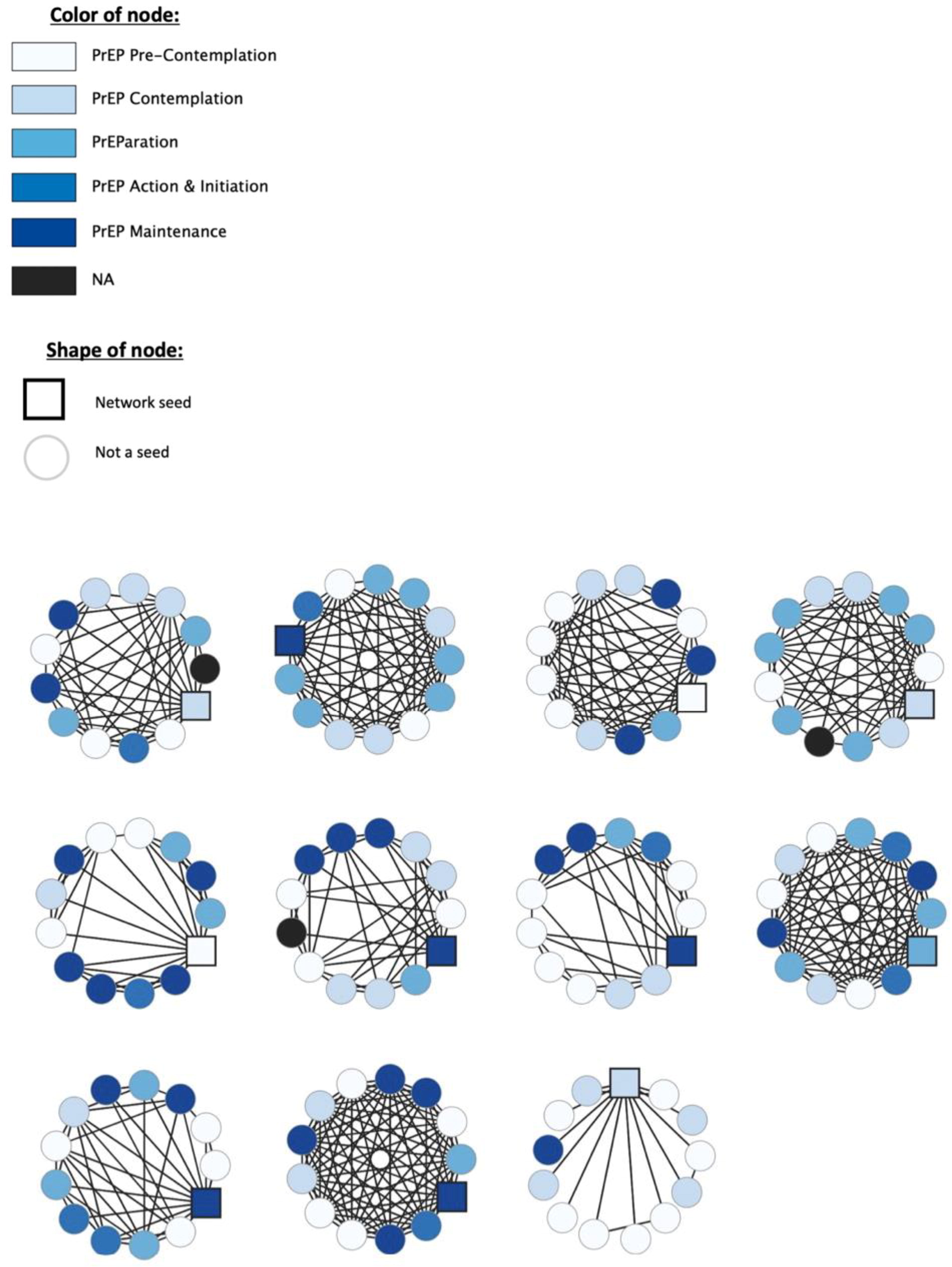
Sociometric visualization of Latino sexual minority men networks and their stage in the Motivational PrEP Cascade, n = 143. PrEP, pre-exposure prophylaxis.
Correlates of MPC stage
PrEP knowledge was significantly associated with an individual’s position on the MPC (χ2 = 9.48; Fisher’s p = 0.028), and participants who had correct knowledge of PrEP effectiveness were more likely to be further advanced in the MPC. For participants who had correct information about PrEP effectiveness, 29% were in the pre-contemplation stage, 22% in the contemplation stage, 16% in the preparation stage, 5% in the action and initiation stage, and 28% in the maintenance stage. For participants who had incorrect information about PrEP effectiveness, 36% were in the pre-contemplation stage, 23% in the contemplation stage, 25% in the preparation stage, 9% in the action and initiation stage, and 6% in the maintenance stage. The association between participant age and the MPC position trended toward significance (χ2 = 20.75; Fisher’s p = 0.052).
Correlation of MPC position relative to friends’ positions
All correlations between participants’ MPC position and the average of their friends’ positions were positive and provided strong evidence of peer influence (Table 2). The first model (Model A) explored the relationship between the average position of the respondents’ friends and their MPC position with PrEP knowledge as a covariate (βPrEPKnowledge = 0.537, CI = 0.04–0.99), yielding a positive autocorrelation coefficient (
Findings from the Bayesian Analysis of the Network Effects Autocorrelation Model
The intervals presented in parentheses refer to the credible interval.
Weighted average of network members.
H1: rho > 0; H2: complement.
PrEP, pre-exposure prophylaxis.
Finally, the Bayesian approach allowed us to calculate the posterior probability of a specific hypothesis, like
Discussion
Our study used a sociocentric network approach to investigate how descriptive norms within social networks can influence LSMM’s progression in the MPC. We found that although around 25% of our sample were using PrEP, generally progression along the MPC was not as advanced as that seen in other studies. Importantly, we found that LSMM’s PrEP use was influenced by their friends’ PrEP use. More specifically, LSMM’s stage in the MPC was associated with the average stage of the participants’ friends’ position in the cascade. We also found that LSMM’s progress along the MPC was associated with correct PrEP knowledge. Furthermore, we found that emotional attachment and interaction frequency may influence progression along the MPC, with stronger emotional attachment and more frequent interactions positively weighing the strength of the autocorrelation. Altogether, the models were very similar statistically in terms of size of effects. Substantively, we might expect the model based on interaction frequency (Model C) to display the strongest effect since direct contact with an associate is intuitively a prerequisite for influence. On the other hand, frequent contact with someone to whom one does not feel especially close may not lead to more influence than less frequent contact but with someone to whom one feels especially close, an argument that weighs in favor of emotional closeness as a preferred indicator of adjacency.
A key finding of this study was the positive association between an individual’s stage on the MPC and the mean stage of their friends—an association influenced by emotional attachment and frequency of interaction. We found that a person’s cascade position was more closely associated with the cascade position of those with whom the individual perceived themselves to be closer or with whom they interacted more frequently. Our findings support previous studies that found that individual health behaviors and motivations, such as those related to the use of and adherence to PrEP among LSMM, do not occur in isolation from one’s social and structural environments. Instead, these behaviors are influenced by an individual’s relationships with others and the values or behavioral norms of such behaviors within their social networks. 43 –47 Our findings also support previous research that found that exposure to a behavior within a network is associated with the adoption of that behavior and that tie strength is associated with peer influence. 48 –50 This also aligns with previous research that while weaker ties are important for the dissemination of information, tie strength is more important to “transmit” more complex behaviors, such as PrEP use. 48,51,52
We found that around 25% of our sample was either taking PrEP or adherent to PrEP; other studies have found PrEP use to be higher with 28–42% of LSMM using PrEP, 13,23,53 with one study reporting PrEP use to be lower among LSMM with only 15–19% of the LSMM sample reporting PrEP use. 54,55 Because our study was recruited through a CBO in South Florida that prioritizes LSMM health, this could suggest that the high awareness and use of PrEP in this sample could be in part due to the efforts of this CBO. However, in the circumstance that participants of this study were not seeking services at our partner CBO, this suggests that social networks could serve as a bridge to PrEP information and access. Our findings support the original construction of the MPC, which found that once participants reached PrEP action and initiation, more participants reached PrEP maintenance. 10 Future interventions can leverage the current clientele of CBOs and focus on peer navigation or influence interventions to reach their social networks.
A review by Zhang and Centola (2019) also highlighted the complexity of the spread of health-related information, beliefs, and behaviors through social networks and the importance of understanding the general mechanisms for the diffusion of these health-related contagions (e.g., pathogenic diffusion, diffusion of information and beliefs, diffusion of positive and negative health behaviors). 44 Peer influence may operate to change health outcomes through several processes such as social norm adoption, social learning, social pressure, and peer imitation. 44 Furthermore, peer influence within the MPC may have significant implications for both the stage of LSMM along the cascade and why LSMM may fall out of care. Although the specific mechanisms of peer influence for PrEP uptake, adherence, and maintenance were not assessed in this study, future studies may expand upon these findings by incorporating questions as to whether participants know the MPC stage of their friends to better understand the underlying processes of peer influence on PrEP uptake, adherence, and maintenance among LSMM and their social networks.
While this is one of the first studies to demonstrate peer influence as it relates to the MPC within friendship networks of LSMM, the MPC has been criticized previously for the lack of attention given to the social context, which may impact an individual’s willingness and intentions to engage in PrEP care. 17 The findings from this study indicate that when used in conjunction with social network approaches, the MPC can be a useful tool to describe engagement with PrEP services among friendship networks of LSMM. Engagement in preventive behaviors, such as HIV testing and condom use, may, at least in part, be influenced by the consistency of such behaviors with the descriptive norms and values of one’s social network. 56 The focus of this study was on interpersonal behaviors and dynamics within LSMM friendship networks. However, progression along the PrEP cascade is heavily influenced by factors at each level of the socioecological model. In particular, structural and systemic barriers impede access and engagement in PrEP services among Latinx populations, such as competing needs (i.e., housing, food, employment), 57 costs, distance to clinics, 31 shortage of Spanish-speaking health care providers and availability of Spanish-language informational materials, 31,57,58 immigration status and concerns, 57 –59 medical mistrust, 55 and negative PrEP messaging. 60 Because LSMM may not access sexual health services at the same rate as White SMM, often due to immigration and discrimination-related barriers and stressors, 31 social networks have utility in reinforcing PrEP use norms and serving as a bridge to PrEP services. Future studies may build up on these findings to further explore the importance of social norms and networks as tools for increasing access to information about biomedical HIV prevention services. Network interventions along with other community-based programming (i.e., CBO-delivered PrEP telehealth 61 ) may serve to further increase access to and engagement in PrEP services among priority populations.
Implications for public health interventions
Our findings support the utility of network interventions, defined as “purposeful efforts to use social networks or social network data to generate social influence, accelerate behavior change, improve performance, and/or achieve desirable outcomes among individuals, communities, organizations, or populations,” to increase PrEP use among LSMM. 62 More specifically, our findings suggest that social network-based PrEP interventions can leverage emotional attachment and interaction frequency—relational attributes that bear weight on the peer influence of PrEP—relative to just having a friend in the network who uses PrEP. There are four types of social network-based interventions: identification, segmentation, induction, and alteration. 62 Of these, HIV prevention interventions have predominantly and successfully used identification, segmentation, and induction strategies. 62,63 Research suggests that individuals who are more central within sociocentric networks and in the network core are more likely to practice HIV preventive behaviors such as HIV testing. Thus, a potential future intervention could consider altering network structures to increase social proximity of LSMM to other LSMM who have progressed along the MPC. Alternatively, efforts can be focused on supporting and providing resources to peers and trusted community leaders (i.e., individuals that are already within LSMM friendship networks) so that they can serve as sources of PrEP information, reduce stigma, and increase trust in communities that have experienced historical and systemic distrust in the health care system. 28 Key network members may also be instrumental in increasing PrEP use self-efficacy, frequency of PrEP-related conversations, and improving willingness to use PrEP and PrEP-related descriptive and subjective peer norms among sociocentric networks of key populations. 29,47
Limitations
This study is not without limitations. First, our findings may not be generalizable to the broader US LSMM population for several reasons: (1) Miami is heterogenous for Latino nationalities, which is not often seen throughout the rest of the nation; and (2) the study sample was identified using RDS, a nonrandom type of sampling method. However, as we have 13 networks of LSMM, there is some generalizability of our findings outside this study.
Regarding the network structure of those included in the sample, one of the networks had all friends stemming unidirectionally from the seed—an abnormal structure that was outside of the RDS recruitment approach that was used in this study. Given the cross-sectional nature of the study, causality cannot be determined. In addition, we were unable to test for changes in PrEP use or observe the directionality of peer influence; thus, our study does not ascertain whether LSMM use PrEP because their network members are using PrEP or if they are actively seeking out other PrEP users to include them in their network (i.e., differential attribution). Furthermore, as a cross-sectional study, we were unable to determine the driving force behind progression in the PrEP cascade. Our ability to understand the role of PrEP knowledge as a measure of intrinsic opinion that either influences or is influenced by progression along the cascade is also limited. In future longitudinal studies, we will examine changes in network dynamics and their association with progression in the cascade.
Conclusions
Despite the US Food and Drug Administration approving the use of oral PrEP in 2012 and injectable PrEP in 2021, 64 LSMM continue to experience HIV and PrEP-related disparities. We found that by increasing one person’s PrEP use, a program may also increase their network’s positive descriptive norms surrounding PrEP, as we found that exposure to PrEP use within a network is associated with the adoption of PrEP use. The widening gap between PrEP awareness and use in this population may be due to multi-faceted structural and individual-level barriers that prevent access to HIV prevention services. This study found that social network factors affect individual health outcomes and can be used to develop health behavior interventions. Our findings suggest that the MPC can be a useful tool to describe engagement with PrEP services among friendship networks of LSMM.
Footnotes
Acknowledgments
The authors would like to acknowledge our community partner, Latino Salud, for their continued support. The authors would also like to thank our participants without whom this work would not be possible.
Authors’ Contributions
C.H.S.: Conceptualization, methodology, investigation, data curation, writing—original draft, writing—review and editing, visualization, and project administration. L.C.: Writing—original draft and writing—review and editing. E.R.: Writing—original draft and writing—review and editing. A.J.: Writing—original draft and writing—review and editing. J.S.: Formal analysis and writing—reviewing and editing. K.S.: Writing—original draft and writing—review and editing. M.K.: Conceptualization, methodology, investigation, writing—review and editing, supervision, and funding acquisition.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the National Institute on Drug Abuse (#K99DA041494 and #R00DA041494; PI: M.K.), the