
Abstract

To the Editor:
A crucial goal in HIV prevention is to increase individuals’ awareness of their HIV status. Globally, the Joint United Nations Program on HIV/AIDS 95-95-95 target is to have 95% of People Living With HIV (PLWH) know their HIV status, 95% of people who know their status to receive treatment, and 95% of people on treatment to have a suppressed viral load. 1 Achieving this goal necessitates a substantial scale-up of HIV testing. Emergency Departments (EDs) are increasingly recognized as primary sites for HIV screening due to the higher likelihood of PLWH visiting EDs compared with non-HIV counterparts. 2,3 Opt-out HIV testing, which involves testing patients unless they explicitly decline, has emerged as an effective strategy to encourage widespread HIV screening, removing the stigma associated with testing and facilitating earlier diagnosis and treatment.
Several studies have successfully implemented opt-out testing (reviewed in Tan et al., 2018, Soh et al., 2022), though it is not yet the standard of care. 1,4 For example, Lin et al. employed routine opt-out HIV and hepatitis C virus (HCV) screening in the ED of the University of Illinois Hospital and Health Sciences System, yielding 0.4% HIV-positive results, with 75% newly diagnosed and 66.7% linked to care. 5 Similarly, Eckardt et al., used ED opt-out HIV testing in the Memorial Healthcare System (Hollywood, FL), detecting 0.5% HIV seropositivity, with 26.2% newly diagnosed patients and 73.8% known HIV patients. 6 A meta-analysis by Henriquez-Camacho found a significantly higher (44%) prevalence of HIV infection detected by opt-out testing compared with opt-in strategies (19%). 7 Similar opt-out approaches have also been established in some pediatric EDs (reviewed in Bi et al., 2022), recognizing that approximately 21% of new US HIV diagnoses are in the 13 to 24 year old age range. 8
Building on the success of these initiatives, we established opt-out testing in Miami, a city with a heightened prevalence of HIV. The FOCUS program was developed and implemented in the University of Miami Health Tower (UHT) Emergency Department to integrate routine opt-out HIV screening into the existing electronic medical record (EMR) workflow. Our primary outcomes included determining the HIV screening rate, number of new HIV cases discovered, and percentage linked to care. Our work reflects a retrospective analysis of ED data collected before (October 2018–Sept 2019) and after (October 9th 2019–October 8th 2022) the implementation of the FOCUS program. Inclusion criteria was limited to patients 18 years old or greater who presented to the ED and received blood tests during the study period. Excluded from the study were those who declined HIV screening, had a documented HIV infection in their EMR or an HIV test within six months of presenting to the ED, or any patients who did not have the capacity to verbally opt-out of screening.
Opt-out HIV screening was incorporated into the ED workflow using the EMR system, EPIC (Cerner Corporation, Kansas City, Missouri), with automated eligibility screening and ordering of HIV lab work. Patients were first asked about their self-reported past testing history. Subsequently, trained nurses and triage staff informed eligible patients about screening benefits and risks, providing clear explanations and the ability to opt out if they chose. This was further reinforced with signage in the ED, which stated that anyone treated in the ED would be tested for HIV unless they opted out. HIV screening was conducted using antigen and antibody immunoassays, with positive results further confirmed and categorized into newly diagnosed or established HIV infection based on data reconciliation with the Department of Health (DOH)-Miami Dade, chart review, or patient self-report after disclosing results. Positive patients were reported to the DOH-Miami-Dade and were linked to care within 3 months.
Pre-implementation data revealed minimal HIV screening based on risk factors. From October 2018–September 2019, 42,170 patients presented to an ED affiliated with UHT, of which only 38 (0.09%) patients were screened for HIV based on risk factors. Of the 38 patients screened, one (2.63%) patient tested positive for HIV. After implementing FOCUS, HIV screening increased significantly, resulting in an 86-fold increase in screening and a corresponding increase in positive cases. A 3-year analysis showed consistent increases in HIV testing rates, with notable increases in positive cases among younger populations. Study characteristics of HIV-tested subjects are described in Table 1. Between October 2019 and December 2022, a total of 126,558 patients presented to an ED affiliated with UHT, of which 57,675 (45.57%) were eligible for testing per the automated EMR tool (Fig. 1). Of those eligible, 34,314 (59.50%) had labs ordered. From this population, 17,850 (52.02%) HIV tests were ordered, with a 47.98% opt-out rate. Of those receiving HIV testing, 17,622 (98.72%) tested negative for HIV, and 228 (1.28%) tested positive, with 37 (16.23%) newly diagnosed cases of HIV, per data reconciliation with DOH-Miami-Dade.
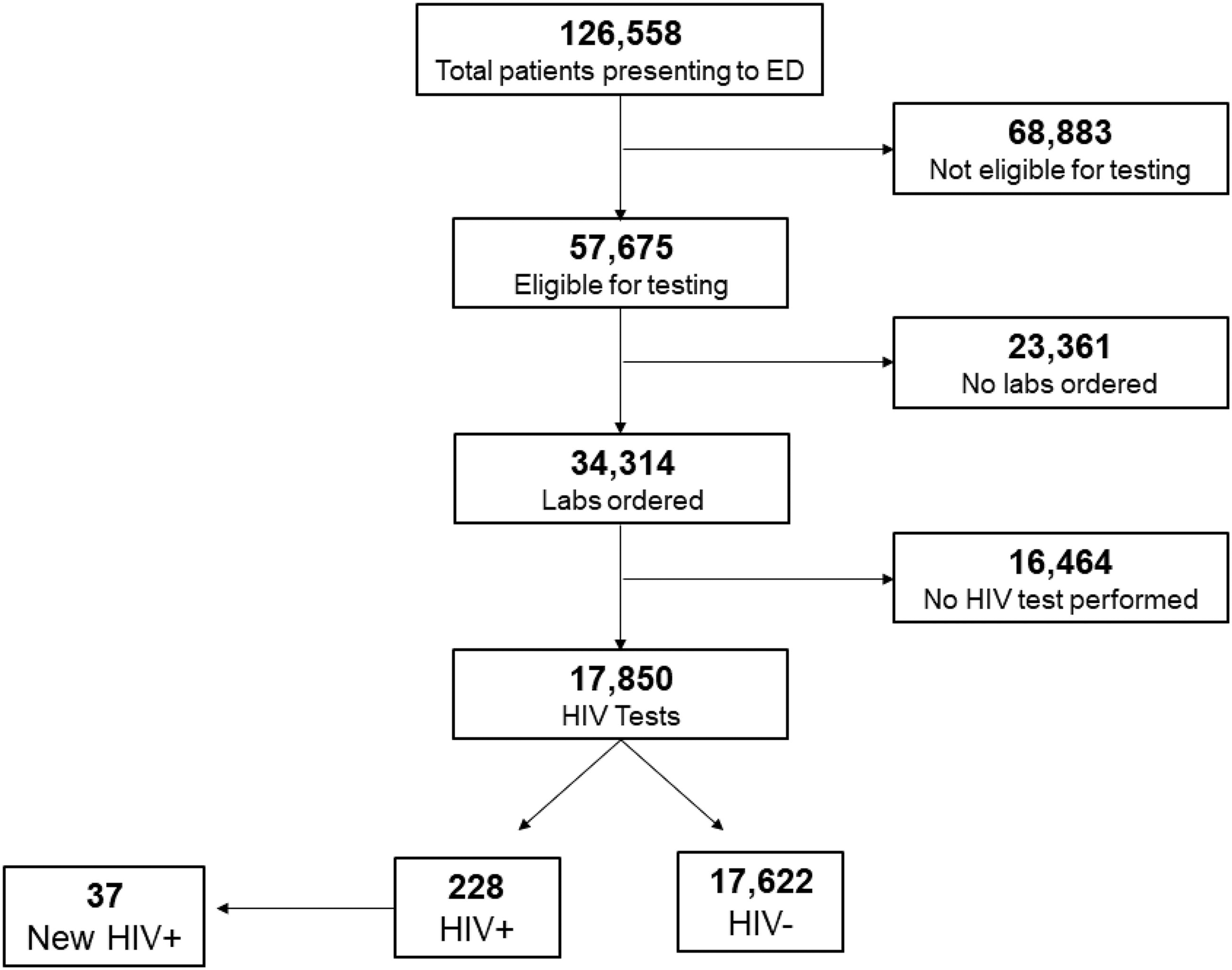
Workflow for FOCUS opt-out HIV testing. Of all patients presenting to the UHT ED, initial eligibility for FOCUS included patients 18 years old or greater who did not meet exclusion criteria: HIV infection documented in EMR, HIV test within 6 months of presenting to the ED, or any patients who did not have the capacity to verbally opt-out of screening. Subsequent eligibility for inclusion in FOCUS included patients already receiving blood tests. From this pool of eligible participants receiving blood work, patients who did not opt-out progressed to HIV testing, and the number of positive and negative cases were documented. Positive cases were further subdivided into newly diagnosed HIV infection versus established HIV infection via data reconciliation with the Department of Health (DOH)-Miami Dade, chart review, or patient self-report.
Study Demographics of the HIV Tested UHealth Tower Emergency Department Adult Population
Significant demographic disparities were observed. For instance, though the majority of patients tested for HIV were Caucasian (65.83%), African Americans were over-represented (54.67%) in the number of patients returning a positive HIV test. However, they only accounted for 27.78% of patients being tested at UHT, which supports other findings on health disparities in HIV diagnoses. 9,10 Of those testing positive for HIV, the median age was 57 years old (IQR, 47.15–63.51), whereas it was 56.5 years (IQR, 40.5–66.2) for patients testing negative for HIV. Patients testing positive for HIV were linked to care through our collaboration with the DOH-Miami-Dade. With FOCUS, 70.27% of patients newly diagnosed with HIV and 83.51% of those with established HIV diagnoses were successfully linked to care. In both groups, failure to link to care was most commonly associated with patients moving, unlocatable, refusing care, or expiring before linkage could be provided. In parallel, other programs have shown that urban ED patients identified with HCV infection can progress to treatment and cure from an ED diagnosis, with rates comparable to those found after diagnosis in ambulatory care settings. 11
We urge all Emergency Departments to consider implementing opt-out HIV testing as part of their standard protocols. Opt-out testing aims to facilitate earlier HIV diagnoses, reduce the stigma associated with risk-based testing, facilitate linkage to care and re-engagement with treatment, and reduce high-risk behaviors and HIV transmission by patients unaware of their HIV status. In our study, 191 of the 228 subjects (83.77%) were found to already have a diagnosis of HIV, highlighting the challenging issue of stigma related to disclosing an HIV diagnosis, even with health care providers. Furthermore, studies have demonstrated that risk-based HIV testing may fail to detect the majority of PLWH in medical care settings. 12 Together, this has prompted recommendations from influential organizations such as the CDC and WHO for provider-initiated opt-out HIV testing for all patients in health facilities, regardless of epidemic setting, with specific emphasis on high HIV prevalence settings. By integrating HIV testing into routine ED workflows, we have the opportunity to reach individuals who may not access traditional testing services and ensure that more people know their HIV status. Additionally, the laboratory results obtained from opt-out HIV screening can further be utilized to identify patients who are candidates for pre-exposure prophylaxis (PrEP). 13 This method enables the detection of individuals at high risk for HIV acquisition despite negative test results, thereby providing an opportunity for targeted education and immediate initiation of PrEP. 13 Collaborating with public health agencies, streamlining testing procedures, and providing staff training are key steps in successfully integrating opt-out testing into ED workflows. By doing so, we can make significant strides towards ending the HIV epidemic by ensuring that more individuals are aware of their HIV status. However, the feasibility and cost-effectiveness of non-targeted opt-out screening may vary depending on the local HIV prevalence and resource availability. In settings with limited resources, such as those with low HIV prevalence or budgetary constraints, HIV screening may be limited to diagnostic and targeted testing. At the root, screening protocols should be tailored to the characteristics of the health care facility and patient population to optimize effectiveness.