
Abstract
Side effects are a common concern of current and potential HIV pre-exposure prophylaxis (PrEP) users, potentially leading to missed doses. We examined the relationship between reported side effects and adherence in the Ontario PrEP Cohort Study (ON-PrEP). In total, 600 predominantly gay (87.3%), White (65.8%), and male (95.0%) participants completed questionnaires assessing the presence and severity of five side effect categories (nausea, diarrhea, headache, abdominal pain, and “other”) as well as their adherence to daily PrEP (any missed doses in the previous 4 days). In total, 175 participants (29%) ever reported experiencing side effects: most commonly diarrhea (7.5% of study visits), and most were of mild severity. Lower incomes (p = 0.01), identifying as bisexual (p = 0.04), and baseline concern about side effects (p < 0.001) were associated with ever reporting side effects. The odds of reporting any side effects decreased by a factor of 0.44 (95% confidence interval 0.25–0.80) with each additional year of PrEP use, however 1 in 10 participants still reported side effects after 1 year of use. The odds of reporting optimal adherence were 0.48 (0.28–0.83) times lower for participants reporting any side effects, 0.67 (0.51–0.89) times lower per additional side effect category reported, and 0.78 (0.65–0.97) times lower per incremental increase in side effect severity ratings. We found some evidence of interaction between side effect measures and duration of PrEP use, suggesting that these relationships were stronger for participants taking PrEP for longer. Clinicians should make efforts to ascertain patients’ experience of side effects and consider risk counseling and alternative PrEP regimens to promote adherence.
Introduction
Despite ongoing prevention efforts, HIV continues to pose a public health threat in Canada, with 4.7 in every 100,000 Canadians being newly diagnosed in 2022. 1 HIV pre-exposure prophylaxis (PrEP) remains an important part of HIV prevention strategies in Canada, with much attention going to facilitating engagement in the PrEP care continuum. 2 Previous research has focused on awareness and uptake of PrEP among Canadians at high risk of HIV, 3 –7 with cost and low perceived HIV risk identified as major barriers to uptake in Canada and internationally. 8,9 However, relatively less work has been done to study adherence and retention in Canadian PrEP users. 10 Adherence to a prescribed PrEP regimen is essential to maintain protection 11 and helps guard against the emergence of antiretroviral drug resistance.
Although PrEP is generally considered by clinicians and public health professionals to be highly tolerable and effective, it is known to cause several side effects including headache, nausea, and diarrhea. 12,13 These side effects are commonly understood to be due to a “start-up syndrome” that resolves within a short time of starting PrEP. 14 However, this is not always the case and many PrEP users continue to experience troublesome symptoms after initiating PrEP. 15
These symptoms may be side effects related to PrEP use, or could be due to other medications or lifestyle factors, but are nonetheless important to users’ decisions about their engagement in PrEP care. Side effects are a commonly-cited barrier to PrEP use, influencing both interest and uptake. 16 Previous work has also found associations between side effects and lower levels of dosing adherence among antiretroviral therapy users, 17 and among PrEP users in other jurisdictions. 15,18,19 These studies exclusively focused on presence or absence of any reported side effects as a binary variable, and questions remain about the relationship between reported side effect severity and medication adherence.
We used data from a cohort of Ontario PrEP users to characterize self-reported side effects and their impact on adherence. We examined participants’ likelihood of reporting side effects as a function of duration of PrEP use, anticipating a decline with longer duration. We then tested for a relationship between any reported side effects and reported adherence to daily PrEP, adjusting for potential confounders and interaction effects (objective 1). Finally, we estimated the dose–response relationships between two measures of overall side effect burden and reported adherence (objectives 2 and 3).
Methods
Study setting and design
We analyzed data from the Ontario PrEP Cohort Study (ON-PrEP), a prospective multicenter open cohort study of HIV-negative people using or initiating any form of HIV PrEP in Ontario. PrEP is not universally covered in Ontario, though several programs exist to partially or fully subsidize costs to many PrEP users. The overall goal of ON-PrEP was to gather real world data on key biological, behavioral, experiential, and engagement in care outcomes in Ontario PrEP users.
Recruitment began in February, 2018. Participants were followed at approximately 6-month intervals for up to 2 years. During each visit, participants completed a web-based, self-administered questionnaire which included questions on their experience of PrEP. Participants received $30 after their baseline visit and $20 after follow-up visits. Trained research staff also collected clinical data elicited via interview and/or chart review.
Participants
Participants in the study were 16 years of age or older, documented as HIV-negative within 3 months of enrollment, currently using or initiating HIV PrEP, and deemed to have sufficient English proficiency to complete study questionnaires by study personnel. We recruited participants at five study sites in Toronto, and one site each in Guelph, Sudbury, London, Hamilton, and Ottawa. We restricted the current analysis to participants after a daily dosing regimen (either tenofovir disoproxil fumarate/emtricitabine or tenofovir alafenamide/emtricitabine), first because our assessment of adherence is based on missed doses in the past 4 days, which is not applicable to on-demand users, and second because the number of participants using on-demand PrEP was minimal. Visits at which participants did not give responses to any of the side effects-related questions were excluded from our analysis, including baseline visits for participants who had not yet initiated PrEP.
Data collection
At each follow-up visit, we collected data regarding both providers and participants’ assessments of participants’ PrEP-related side effects. Providers’ assessments were recorded using a yes/no option for each of: nausea or vomiting, diarrhea, headache, rash, dizziness, and other toxicities. Participants were asked “have you experienced any of the following side effects while on PrEP?” for each of nausea, diarrhea, headache, abdominal pain, and other (open text) at their baseline visit, and further asked to rate the current severity for each side effect. At subsequent visits, participants were asked to rate the severity of those side effects in the previous 6 months. Severity ratings were ranked on a scale of none (0), mild (1), moderate (2), and severe (3). If participants answered only part of the side effects section, missing values were assumed to indicate no experience of side effects. We used participants’ self-reported side effect data to define the focal exposure variables corresponding to three multivariable models.
The primary outcome of interest was self-reported adherence to daily PrEP. At each visit, participants were asked “in the past four days, which days did you miss taking your medication?” Given the high levels of reported adherence observed in the cohort overall, we created a binary outcome variable, grouping participants as having either less-than-perfect self-reported adherence if they indicated missing at least one dose, or perfect self-reported adherence otherwise.
Several variables were created from questionnaire items for use as covariates in multivariable regression models to adjust for potential confounders or effect modifiers pre-identified in our conceptual model. Participants’ race was collected using 15 categories in which respondents could check all that applied. We transformed these into a single variable with 10 levels, grouping similar categories with small sample sizes, and assigning the applicable non-White category to individuals indicating both White and one other racial identity as we felt this would likely better reflect their social determinants of health and potential effects of structural racism. We used a validated seven-item scale as a measure of Discrimination in Medical Settings. 20 To capture common coexisting mental health conditions, we created a composite variable of self-reporting either or neither of “drug or alcohol dependence” and “mental illness.” We also computed the number of concomitant medications of each participant as the number of unique prescription drugs and supplements they were taking. We estimated participants’ duration of PrEP use by using self-reported responses on PrEP initiation dates, or provider estimates when this was not available. Finally, we computed a new variable representing the perceived efficacy of PrEP as the difference between participants’ estimated risk of contracting HIV in the next year (0–100 scale) if not using PrEP and risk of HIV in the next year if using PrEP.
Statistical analysis
All statistical analyses were conducted using R version 4.1.1. We first summarized characteristics of the study sample using descriptive statistics. At each time point, we quantified the proportion of participants reporting each of nausea, diarrhea, headache, abdominal pain, as well as “other” side effects, whose free-text descriptions were categorized into groups based on author (M.R., D.H.S.T.) consensus. We further compared demographic characteristics between subgroups of participants who reported ever versus never experiencing side effects using the Wilcoxon rank sum test and X2 test of independence, as appropriate. Participant-reported and provider-reported side effects were then compared using confusion matrices and sensitivity scores, treating participant-reported side effects as the gold standard. We similarly compared participant- and provider-reported adherence, though the measures of each were not directly comparable and provider-reported adherence was only assessed at baseline. Our last descriptive analysis of side effects was to estimate the crude trend in odds of reporting any side effects as a function of duration of PrEP use to test for a decline in reported side effects with longer duration of use. To capture within-participant correlation resulting from repeated measures, we used a binomial mixed-effects model with random intercept and slope terms. All random effects models in this analysis were estimated with the lme4 package version 1.1–32.
We computed three measures of side effects to use as focal exposure variables: a binary variable of whether or not participants reported any side effects (for objective 1), the number of side effects as a count of side effect categories for which participants indicated a severity greater than none (objective 2), and the sum of participants’ severity ratings across the five categories (objective 3). We estimated the change in odds of reporting perfect adherence for each of our focal exposure measures using random intercept-only models. Selection of covariates in these models was conducted after the causal model selection framework of Kleinbaum, Kupper, and Morgenstern. 21 We preidentified candidate covariates for inclusion in the analysis through consultation with members of the study team, which includes clinicians, academic researchers, and community partners. Two-way interactions between five potential effect modifiers (duration of PrEP use, baseline concern about side effects, concern with current risk of HIV, perceived PrEP efficacy, and number of male sex partners in the past 6 months) and focal exposures were tested using backwards selection with a significance threshold of p < 0.1. We then evaluated potential confounders for inclusion in the multivariable model based on a leave-one-out backwards selection procedure. A change in primary odds ratio of greater than 10% with removal of each potential confounder was considered sufficient evidence of confounding for inclusion in the model. If interactions were present in a model, we evaluated estimated focal odds ratios at various levels of interaction variables (5th, 25th, 50th, 75th, and 95th percentiles) and considered a >10% change at any level to be evidence of confounding. The variable with the lowest magnitude of change was eliminated and the process repeated until no potential confounders had a change in association measure lower than 10%. Variables with nearly significant (p < 0.1) interaction terms or which were significant (p < 0.05) predictors of adherence were ineligible for removal regardless of evidence of confounding according to the hierarchical modeling principle. 22
Ethics approval
Ethical approval was obtained from the Research Ethics Board of the primary study site (St. Michael’s Hospital: REB#17–281), as well as relevant Boards for Hamilton Integrated, Ottawa Health Science Network, Public Health Ontario, University Health Network, and University of Toronto. All participants provided informed consent before participating in study activities.
Results
Participants
Of the 3435 total possible study visits from the 712 participants enrolled in ON-PrEP as of May 18, 2023, 990 (29%) were absent in our data due to missed visits, loss to follow-up, and/or study withdrawal. In post hoc analyses, we observed that participants reporting suboptimal adherence had half the odds of attending their next study visit, but no significant association between side effects and attendance at subsequent visits. We also found that 42% of missed visits occurred in the 365 days after March 17, 2020, and odds of missing a visit in this time period were 90% higher, adjusting for study visit and participant ID. These findings suggest that disruptions related to the COVID-19 pandemic were at least partially responsible for these high levels of missingness. A full description of our missing data analysis can be found in Appendix 1. An additional 628 visits were excluded due to participants not answering questions about dosing regimen (n = 482, 14%) or indicating they were using an on-demand regimen (n = 146, 4%). Finally, 37 remaining visits (1%) were excluded because participants did not answer any questions about side effects, leaving 600 participants with at least one and an average of 3.0 eligible visits each in the analysis (Table 1). At their first eligible visit, the average participant was 38.6 (11.4) years old and had been using PrEP for 12.8 months. The majority of participants identified as gay (87.3%), White (65.8%), and males (95.0%).
Characteristics of HIV PrEP Users Stratified by Self-Reported Side Effects
“White—North American” and “White—European” were grouped as “White,” “Black—African,” “Black—Caribbean,” and “Black—North American” as Black, “First Nations,” “Inuit,” “Metis,” and “Indigenous/Aboriginal” as “Indigenous.” People indicating “Indian—Caribbean,” “Other,” or nothing were grouped as “Other.”
Participant-reported side effects and adherence
Participants indicated no experience of side effects for a large majority of study visits (Fig. 1) with 71% of participants never reporting any side effects. Participants indicated a severity of none at 95.1% of study visits, averaged across all categories. When side effects were reported, they tended to be mild (3.4%), followed by moderate (1.3%) in severity; severe side effects were rare (0.2%). “Other” side effects were reported at a total of 73 study visits, with the most common categories being sleep issues (n = 8), reduced kidney function (n = 8), fatigue (n = 7), soreness (n = 7), and dizziness (n = 6).

Self-reported side effect severities by category. “Other” author-categorized reported side effects included change in appetite/weight (n = 9), sleep issues (n = 8), fatigue (n = 7), GI disturbance (n = 7), nephrotoxicity (n = 7), soreness (n = 7), dizziness (n = 6), skin/hair issues (n = 6), increased heart rate (n = 4), sensory disturbance (n = 3), change in sexual function (n = 3), mood disturbance (n = 2), gynecomastia (n = 1), hiccups (n = 1), dry mouth/lips (n = 1), and cytopenias (n = 1).
Participants who ever reported experiencing side effects were more likely to report being in the lowest income category (20% vs. 13% with annual income <$30,000, p < 0.01), identify as bisexual as opposed to gay (15% vs. 7%, p = 0.04), and indicate that they were concerned about experiencing side effects at baseline (69% vs. 46%, p < 0.001) compared to participants who never reported side effects (Table 1). Participants ever reporting side effects also appeared to report fewer average years of PrEP use (0.9 vs. 1.1, p = 0.05), take more concomitant medications (2.1 vs. 1.7, p = 0.07), and have a greater frequency of mental illness or substance dependence (23% vs. 16%, p = 0.05) than people who did not, albeit with borderline statistical significance.
At visits where participants indicated experiencing nausea, headache, and diarrhea, providers tended to underestimate the presence of these side effects (Fig. 2). We computed sensitivities of 17%, 5%, and 9% for providers’ detection of each side effect, respectively. Conversely, providers tended to overestimate participants’ adherence to their daily PrEP regimens: among participants who reported missing at least one dose in the 4 days preceding their baseline visit (n = 77), providers reported 96.1% (n = 74) were dosing 7 days per week.
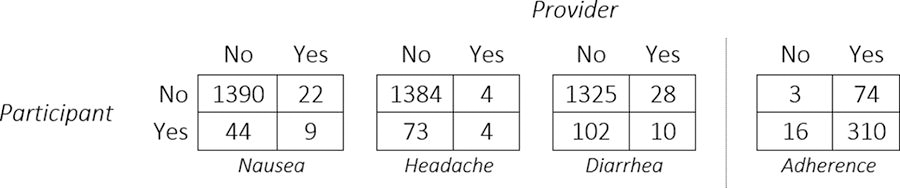
Comparison of participant- and provider-reported side effects and adherence.
A nonparametric estimate of the fraction of participants reporting any side effects as a function of years on PrEP is presented in Figure 3. Consistent with our hypothesis of decreasing side effects over time, the odds of reporting any side effects decreased by a factor of 0.44 [95% confidence interval (CI) = 0.25 to 0.80] for each additional year of PrEP use. Interestingly, after approximately 1 year of PrEP use, we noted a plateau in the proportion of participants experiencing side effects, which stabilized at approximately 11%. Coincident with this plateau in reported side effects, we observed a marked divergence in reported adherence after 1 year, with adherence rates remaining stable among participants reporting no side effects, but declining among those reporting side effects (Fig. 3).

Fraction of visits reporting any side effects by duration of PrEP use (left) and fraction reporting optimal adherence by reported side effects and duration of use (right). PrEP, pre-exposure prophylaxis.
Regression analyses
Backwards selection procedures to assess for interactions in all three regressions found that duration of PrEP use was significant or nearly significant, and we therefore included it in all of our multivariable models. All three models found significant negative relationships between their respective measures of side effects and adherence. Table 2 reports estimated coefficients for each association of interest and relevant covariates. Because these relationships change as a function of duration of PrEP use, we report estimated adjusted odds ratios for a participant with a PrEP duration of 1.8 years (the cohort mean over all eligible study visits). Adjusted odds ratios and CIs as a function of duration of PrEP use are plotted in Figure 4.
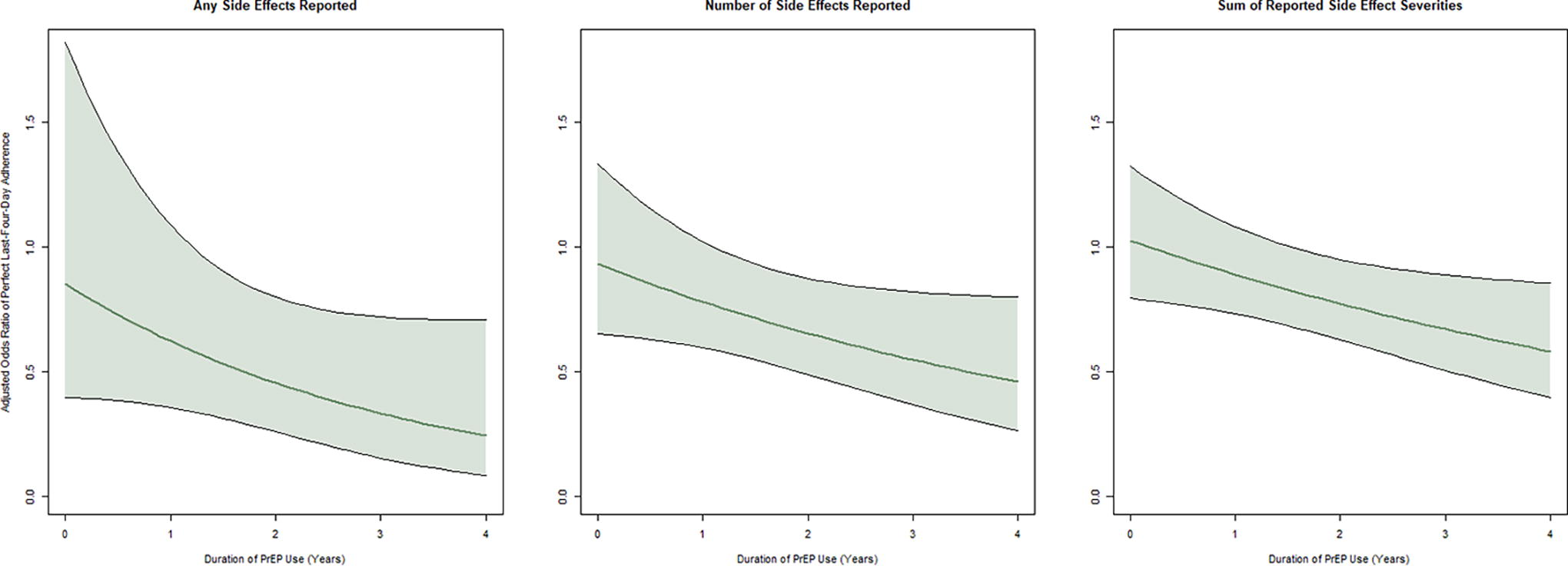
Estimated odds ratio (95% CI) of reporting optimal adherence for any reported side effects vs. none (left), for each additional side effect category (middle), and incremental increase of one severity level (right), as a function of duration of PrEP use (years). CI, confidence interval; PrEP, pre-exposure prophylaxis.
Multivariable Regression Models for Self-Reported Optimal Adherence as a Function of Three Side Effect Measures
Multivariable regression models for self-reported optimal adherence as a function of any side effects (regression 1), number of side effect categories (regression 2), and sum of side effect severity ratings (regression 3). Baselines concern about side effects, perceived risk of HIV infection, perceived PrEP efficacy (difference in risk if not using PrEP and if using PrEP), and number of male sex partners in the past 6 months were considered as potential interaction terms but had estimated p-values above 0.1. Gender, preferred language of communication, baseline concern with health, chronic illness, mental illness/substance abuse, number of concomitant medications, and method of paying for PrEP were considered as potential confounders but excluded by the model selection process. PrEP, pre-exposure prophylaxis; CI, confidence interval.
At average PrEP duration, participants reporting side effects had 0.48 (95% CI = 0.28–0.83) times lower odds of reporting perfect adherence compared to those using PrEP for the same time who did not report side effects. The interaction between PrEP duration and any side effects suggested that participants who have been using PrEP longer had lower adjusted odds ratios, although this relationship was not statistically significant in the final model (p = 0.10).
Similarly, for each additional side effect reported, participants had 0.67 (95% CI = 0.51–0.89) times reduced odds of reporting perfect adherence. The interaction term also suggested this relationship deepens as PrEP duration increases, albeit with borderline statistical significance (p = 0.057).
Finally, for each incremental increase in side effect severity, participants had 0.79 (95% CI = 0.65–0.97) times reduced odds of reporting perfect adherence. The interaction between side effect burden and PrEP duration was significant in this model (p = 0.028), again suggesting that adherence among participants who had been using PrEP longer was more strongly affected by side effects.
Discussion
Among people reporting taking daily PrEP in Ontario, Canada between 2018 and 2023, we found that side effects were associated with decreased adherence, and nonadherence worsened with the number and severity of side effects reported. Although self-reported side effects declined with duration of use, participants still reported side effects at 11% of study visits after 1 year of use. These same participants reported progressively lower levels of adherence as their time on PrEP lengthened. Finally, we found that providers tended to under-report side effects when reported by participants, and over-report adherence when participants indicated missing doses.
The relationship between medication side effects and adherence is not new: it has been observed in other contexts, 23,24 among antiretroviral therapy users, 17,25 and in correlational studies of PrEP users. 15,18,19 Our analysis extends these findings by demonstrating a dose–response relationship, where the odds of reporting optimal adherence worsened with the number of side effect categories reported, and with the sum of side effect severity ratings. This suggests that decreasing the severity and quantity of side effects, as opposed to eliminating them entirely, may be a worthwhile goal. The most commonly reported side effect was diarrhea, which can be troubling because of the lost sense of personal control, embarrassment/stigma, and physical discomfort it sometimes causes, among other reasons. To optimize long-term PrEP adherence, clinicians may thus consider searching for alternative causes for symptoms that patients perceive to be side effects of PrEP, and/or recommending over-the-counter therapies to manage troubling symptoms. Additionally, qualitative studies of current and prospective users of long-acting injectable PrEP suggest perceived ease of adherence compared to daily oral PrEP, 26,27 despite similar frequencies of headache and gastrointestinal side effects and a high frequency of injection site reactions in clinical trials. 28,29
The finding of persistent participant-reported side effects after 1 year of use challenges the common narrative that PrEP users experience a “start-up syndrome” which goes away with time. Considering that clinical trials have mostly found rates of reported side effects do not differ between PrEP and placebo users, 30 it is possible that symptoms reported as side effects are actually due to other factors. However, the exact cause of these side effects is immaterial when considering users’ reasons for nonadherence.
This is particularly true for patients reporting side effects long after initiation of PrEP, where reported side effects were found to increasingly indicate risk of suboptimal adherence. New PrEP users may be more likely to tolerate side effects, but gradually become more likely to miss doses as their initial enthusiasm for PrEP fades. This effect may be under-estimated in our analysis due to survivorship bias. Participants in whom side effects and adherence are worst may be more likely to fall out of care and be under-represented in the ON-PrEP data.
These findings all underscore the need for clinicians to broker conversations with patients about experienced side effects. As in our study, research on antiretroviral therapy users has found that clinicians tend to underestimate the frequency of patient-reported side effects. 31 –33 Possible reasons may include social desirability bias, if patients are unwilling to raise concerns about side effects, and also be because providers are not initiating or documenting these conversations. These are missed opportunities to enhance patient quality of life and improve adherence, and can undermine the therapeutic alliance between patient and provider. Related work has found that the use of self-administered modules for measurement of side effects can improve detection sensitivity which might be a valuable tool to promote consistent clinical evaluation of patient symptoms. 34,35
This analysis has limitations that must be considered when interpreting our results. First, loss to follow-up in the ON-PrEP cohort was significant, with 29% of all possible study visits missing and an additional 15% excluded due to missing dosing or side effect data. Some missed visits were due to challenges of follow-up during the COVID pandemic and were unrelated to the study variables. We hypothesize that if any nonignorable missing data mechanism is present, it is more likely that participants experiencing side effects or with suboptimal adherence missed study visits. Under this assumption, we would expect the direction of any bias to be towards the null. A second limitation of this analysis is the use of optimal reported adherence as the primary outcome, due to high levels of self-reported adherence in the cohort overall. Most suboptimal responses involved only one missed pill in the previous 4 days, a level of adherence corresponding to a 96% risk reduction in HIV incidence among GBM. 11 However, it is known that self-reported adherence often over-estimates adherence as assessed by biomarkers, 36 and the associations found in this analysis may still help identify those at increased risk of PrEP failure. Finally, data on some potential confounders such as education level were not assessed in the ON-PrEP study, although we used alternative markers of socioeconomic status such as annual income instead.
Identifying barriers to engagement in the PrEP care continuum is an important part of scaling up HIV prevention efforts in Ontario and globally. Overall, our findings highlight the importance of having ongoing conversations with patients about their experience of side effects and PrEP adherence over the long term, and of developing strategies to improve tolerability. Other PrEP modalities such as on-demand dosing or long-acting injectable cabotegravir may be suitable alternatives that support users in adhering to their regimen.
Footnotes
Acknowledgments
The ON-PrEP Cohort study is administered at 10 study sites spanning much of what is now called Ontario, the traditional territories of more Indigenous peoples than can adequately be acknowledged. We are grateful for the opportunity to live and work on this land, and reaffirm our commitment to seeking redress for the historical and ongoing dispossession faced by these communities. We would like to thank the research participants for making this work possible. Additional thanks to Janet Raboud for her advice on the supplemental analysis of missing data.
Authors’ Contributions
M.R.: Conceptualization, data curation, formal analysis, methodology, software, visualization, writing—original draft, writing—reviewing and editing. M.M.: Methodology, writing—reviewing and editing. R.L.: Funding acquisition, project administration, supervision, writing—reviewing and editing. P.M.: Funding acquisition, investigation, resources, writing—reviewing and editing. D.K.: Funding acquisition, investigation, resources, writing—reviewing and editing. K.W.: Funding acquisition, investigation, resources, writing—reviewing and editing. J.R.: Funding acquisition, investigation, resources, writing—reviewing and editing. J.M.: Investigation, resources, writing—reviewing and editing. I.I.B.: Funding acquisition, investigation, resources, writing—reviewing and editing. D.C.: Investigation, resources, writing—reviewing and editing. M.J.B.: Investigation, resources, writing—reviewing and editing. S.S.: Investigation, resources, writing—reviewing and editing. A.L.: Funding acquisition, writing—reviewing and editing. G.D.: Writing—reviewing and editing. A.S.: Writing—reviewing and editing. F.O.: Writing—reviewing and editing. A.N.B.: Funding acquisition, writing—reviewing and editing. D.H.S.T.: Conceptualization, funding acquisition, investigation, methodology, project administration, resources, supervision, writing—reviewing and editing.
Author Disclosure Statement
P.M. has received speaker honoraria from Merck and Gilead. I.I.B. has consulted to Intercept: Global Public Health & Health Security. M.J.B. has received speaker honoraria from Gilead. D.H.S.T.’s institution has received support from Abbott and Gilead for investigator-initiated research grants and from Glaxo Smith Kline for industry-sponsored clinical trials. The other authors have no conflicts of interest to declare.
Funding Information
ON-PrEP is funded by the Canadian Institutes of Health Research (CIHR),
Appendix 1—Analysis of Missing Data
Due to higher-than-expected rates of missing data in our analysis of side effects and adherence in the ON-PrEP cohort study, we performed several supplemental analyses to assess the potential for bias in our main results.
We created a dataset of all potential study visits prior to May 18, 2023, classifying each potential visit into four categories reflecting reasons for inclusion/exclusion into our main analysis: Not Present: Potential visits for which we had no record of study attendance. Present—on-demand dosing: participant attended study visit but indicated they were following an on-demand PrEP regimen. Present—missing fields: participant attended study visit but did not answer required fields (dosing regimen, experience of side effects) and was excluded from analysis. Present—eligible: participant attended study visit and met all eligibility criteria for inclusion in our analysis.