
Abstract
Personal and structural barriers to HIV pre-exposure prophylaxis (PrEP) care result in its underutilization and premature discontinuation. A home-based PrEP program comprised of telemedicine visits and/or self-administered lab testing may address some of these barriers. Our objective was to assess the acceptability and feasibility of a home-based PrEP program among stakeholders at an urban HIV and primary care clinic. We used the consolidated framework for implementation research to evaluate determinants of successful implementation of the program. We surveyed and interviewed PrEP patients and their health care team. In a baseline survey of PrEP users (n = 112) administered between May 2021 and August 2022, 65% expressed interest in switching to the home-based PrEP program. Seventeen patients over the course of follow-up through December 2023 started home-based PrEP, including 12 patients who completed both a telemedicine visit and a self-administered lab kit, and 5 patients who completed only a telemedicine visit. Of these, over 80% had positive feedback on the telemedicine visits. Survey results demonstrated excellent acceptability and feasibility of the lab kits. Patients indicated in interviews that the home-based PrEP program provided the strong advantage of convenience. Despite mixed feelings from PrEP providers on telemedicine visits (n = 5), most felt that the program made PrEP care delivery easier for patients and would encourage their patients to use the program if it were a good fit. Barriers to program success included shipping delays and staff turnover during program implementation. In conclusion, uptake of the home-based program was low but program participants expressed high acceptability.
Introduction
HIV remains a significant public health concern in the United States, with 1.2 million people currently living with HIV and approximately 31,800 new infections in 2022 alone, despite the existence of effective HIV pre-exposure prophylaxis (PrEP). 1 The Ending the HIV epidemic initiative was announced in 2019, with a goal of reducing new HIV infections in the United States by 90% by 2030. 2 One of the four main pillars of this initiative is the prevention of new HIV transmissions using PrEP and other effective HIV prevention modalities. Research to identify strategies to increase and maintain PrEP use in populations at risk of HIV acquisition is greatly needed.
PrEP is an evidence-based intervention that is highly effective at preventing HIV acquisition if taken as prescribed. 3 There are currently three PrEP medications in the United States approved by the Food and Drug Administration—oral tenofovir disoproxil fumarate/emtricitabine, oral tenofovir alafenamide/emtricitabine, and injectable cabotegravir. In 2023, about 1.2 million persons aged ≥16 years had indications for PrEP, but only 31.3% were prescribed PrEP. 4
There are many barriers to PrEP use that result in its underutilization. These include a lack of patient and provider awareness of PrEP, a low perception of one’s own HIV risk, 5 concerns about side effects, 6 competing priorities, the cost of PrEP care, 7,8 difficulty in accessing a clinic, 9 the burden of frequent clinic visits, the need for regular laboratory monitoring, fear of stigma, patient hesitancy to discuss their sexual history with medical providers, and structural and policy barriers that differ from region to region. The COVID-19 pandemic also presented a barrier, as many health care providers limited their practices and the public decreased their use of health services due in part to fear of COVID-19 exposure. A study found a 22% reduction in PrEP prescriptions and a 25% reduction in new PrEP users due to the COVID-19 pandemic. 10 Furthermore, PrEP discontinuation is common, as demonstrated in several studies reporting 37-62% discontinuation after 6 months. This is presumably due to a variety of reasons ranging from appropriate discontinuation in the setting of lowered HIV risk, to barriers that prevent those who remain at HIV risk from continuing on PrEP.
Current standard PrEP prescribing practice includes a quarterly clinic visit for lab testing, evaluation of PrEP adherence using a combination of patient self-report and pharmacy refill patterns, and assessment of sexual and drug use practices. Lab testing involves checking for HIV and sexually transmitted infections (STIs) and monitoring renal function, which requires blood draws every 2 (for cabotegravir) or 3 (for oral PrEP) months and STI screening swabs/urine collection every 3–6 months. Home-based PrEP with telemedicine visits and self-administered HIV/STI testing has been studied as a possible method of improving PrEP delivery. One can hypothesize that it has the potential to reduce certain barriers to PrEP uptake and persistence, such as access to care, the burden of frequent clinic visits, fear of stigma, and the requirement of social distancing during a pandemic. A study of 1071 gay, bisexual, and other men who have sex with men in the United States showed that 72.3% were interested in home-based PrEP. 14 There are several commercial entities that now provide PrEP through an online platform, including NURX (nurx.com), PlushCare (plushcare.com), and MISTR (heymistr.com), which provide some combination of a video visit or text messaging with a health care provider with labs collected at a local lab or by a self-administered lab kit. There have been several pilot studies of other variations of telehealth PrEP programs, such as the Iowa TelePrEP program that targets rural populations and provides telehealth visits with a pharmacist and labs collected at a local outpatient lab. 15 This was found to be a feasible delivery model in their setting. Several other pilot studies have studied a self-administered lab kit for PrEP care, 16,17 or telehealth PrEP visits with an infectious disease physician in combination with laboratory visits, 18 and have found these to be acceptable and feasible from the perspective of patients. There have been few pragmatic studies of the implementation of a home-based PrEP program in a real-world clinic setting, and clinician feedback has thus far been limited. We used an implementation science framework to investigate the pragmatic roll-out of a home-based PrEP program at an urban community HIV and primary care clinic. Our objective was to examine the level of patient interest in a home-based PrEP program and the acceptability of the program from the perspective of different stakeholders, including both patients and members of their health care team.
Methods
Study design and participants
This is a pilot implementation of a home-based PrEP program at an urban community HIV and primary care clinic in Philadelphia, which has provided PrEP care to over 5000 patients since 2012 and currently provides care to 500 active PrEP users who have filled prescriptions in the previous 6 months. We used the consolidated framework for implementation research framework to plan and evaluate the implementation of the home-based PrEP program by considering intervention characteristics, stakeholder characteristics, the inner clinic setting, and the outer structural setting. 19 We obtained the perspectives of multiple stakeholders, including PrEP users ages 18 or older, PrEP providers, and PrEP retention coordinators (PRCs). At this clinic, each PrEP user is assigned a PRC as a part of their PrEP care and the PRC is responsible for providing PrEP education, securing medication coverage through insurance or patient assistance programs, ensuring patients are up to date on required laboratory testing, providing ongoing behavior and harm reduction counseling, providing tailored adherence assessment and support, reaching out to patients who miss their appointments, and working to reduce barriers to retention in care as needed.
Implementation strategy
The implementation strategy was a home-based PrEP care delivery model, which replaced in-person clinic visits with telemedicine visits provided by the patient’s existing PrEP provider, and replaced labs collected at a health care facility with a self-administered lab kit mailed to the patient’s home. The lab kits were assembled and processed by molecular testing labs (MTL) (Vancouver, WA). The lab kits could include the collection of dried blood spots (DBS) on Whatman DBS cards to run a fourth-generation HIV antigen/antibody test with confirmatory screening (GS HIV Combo Ag/Ab enzyme immunoassay [EIA] and Geenius HIV 1/2 Supplemental Assay [Bio-Rad Laboratories, Hercules, CA]), Treponema pallidum antibody (Diamedix Phoenix Bio-Tech Trep-Sure EIA Assay [Thermo Fisher Scientific, Waltham, MA]), hepatitis B virus surface antigen (GS HBsAg Confirmatory Assay 3.0 EIA [Bio-Rad Laboratories, Hercules, CA]), hepatitis C virus (HCV) antibody (ortho HCV Version 3.0 enzyme-linked immunosorbent assay [Bio-Rad Laboratories, Hercules, CA]), serum creatinine (MTL validated liquid chromatography-mass spectrometry platform), and tenofovir level by liquid chromatography-mass spectrometry, and the collection of urine specimens and oral and rectal swabs for Neisseria gonorrhoeae and Chlamydia trachomatis nucleic acid amplification testing (Cobas CT/NG 4800 Assay [Roche Diagnostics, Indianapolis, IN]), as well as additional testing options depending on the patient’s needs (https://moleculartestinglabscom/testing-menu/). Participants use prepaid shipping bags to mail completed lab kits back to MTL for processing. Labs results appear in an MTL electronic portal accessible by the clinical team.
Procedure
We administered a baseline survey to patients receiving standard clinic-based PrEP care and collected data on demographics, HIV risk factors, barriers to PrEP use, and interest in a home-based PrEP program. Those patients who expressed interest in home-based PrEP in the survey were contacted by their assigned PRC and offered the opportunity to switch from the standard clinic-based PrEP care delivery model to the home-based model. For those who decided to switch to home-based PrEP, the PRC provided education on how to use the self-administered lab kit through in-person or virtual teaching. Instructions were also available through a pamphlet in the lab kit and online instructional videos. Through December 2023, patients who completed one telemedicine visit or self-administered lab kit were given a follow-up survey to evaluate their feedback on the program. We conducted semistructured interviews of patients who tried the home-based PrEP program. Clinicians who provided at least one home-based PrEP visit were surveyed to elicit feedback on the program. We also interviewed PRCs to collect their perspectives on barriers and facilitators of the home-based PrEP program.
The outcome variables of interest were acceptability and feasibility. We evaluated acceptability of the telemedicine visits and lab kit by asking questions around the domains of satisfaction, convenience, privacy, and preferences. Feasibility, defined as the extent to which the program can be successfully carried out in this setting, was evaluated by asking questions around the domains of patient access to technology and a stable mailing address, the usability of the lab kit, and the ease of incorporating the program into the providers’ clinical practices. A modified version of the system usability scale (SUS) was used to measure usability of the lab kits. This is a commonly used 10-item questionnaire with a Cronbach’s alpha of 0.92 and good convergent validity. 20 Study data were collected and managed using REDCap electronic data capture tools. 21,22
Analysis
Descriptive statistics were used to characterize the cohort. The SUS was scored according to guidelines, with a score of >71.4 indicating good usability. 23 Patient interviews were audio recorded and transcribed. Two researchers independently reviewed transcripts to create a list of codes, generated in an open-coding manner. Through discussion and consensus, a codebook was created. The transcripts were coded, with a kappa statistic of 0.73, indicating good interrater reliability. Final codes were analyzed using a grounded theory approach to produce a framework around patient perspectives of the home-based PrEP program.
Results
Baseline characteristics of pre-exposure prophylaxis users
The baseline survey was distributed to 214 patients and completed by 102 individuals (response rate of 47.7%) between May 2021 and August 2022. Baseline demographic characteristics of the PrEP users are shown in Table 1. The age of patients ranged from 18 to 71, with a median of 30. Most patients were male sex at birth (91%). About three-quarters of patients (76.2%) identified as male and 70.3% identified as gay or lesbian. The racial breakdown included 53.1% White patients, 30.2% Black patients, 9.4% Asian patients, 3.1% other, and 4.2% multi-racial patients. Eleven participants (11.7%) identified as Hispanic/Latinx. Most participants had greater than a high school education (86.1%).
Demographic Characteristics of Pre-Exposure Prophylaxis Users
Data are expressed as median (IQR) or n (%).
Cumulative exceeds 100% due to multiple selections.
PrEP, pre-exposure prophylaxis.
When asked to use a Likert scale to rate their level of interest in switching from a standard clinic-based PrEP program to a home-based PrEP program, 32.7% were very interested, 32.7% were somewhat interested, 16.8% were neutral, 12.9% were not very interested, and 5.0% were not at all interested. In evaluating the feasibility of the program, most patients reported having a device with the ability to perform video calls (98%) and a cell phone with texting capabilities (99%). Most patients had a stable mailing address (97%) to which a lab kit could be mailed and 86.1% endorsed feeling comfortable with having a lab kit mailed to the home.
Patients were also asked on the baseline survey to use a Likert scale to rate their perceptions of the acceptability of the home-based PrEP, prior to trying the program (Fig. 1). Fifty-eight percent felt to some degree that telemedicine would be more convenient than in-person visits and 54.5% felt home lab testing would be more convenient than in-clinic testing. Over half neither agreed nor disagreed that they would experience less stigma with a home-based PrEP program. Forty-five percent agreed that home-based PrEP would provide more privacy.
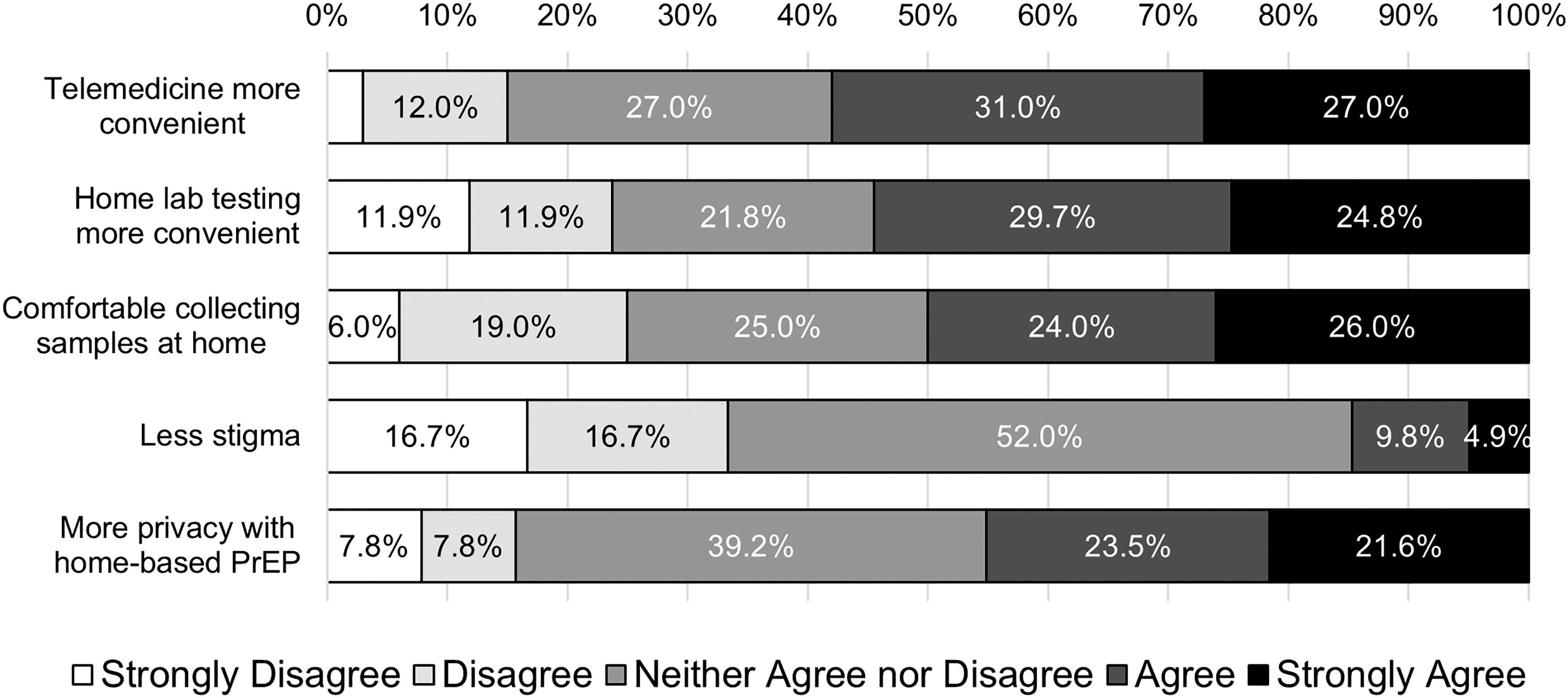
Baseline survey of standard clinic-based PrEP users rating their perceptions of the acceptability of a home-based PrEP program using a Likert scale (n = 102). PrEP, pre-exposure prophylaxis.
On the surveys, patients listed various reasons for not being interested in home-based PrEP, including the need to come to clinic in-person for other medical issues anyway, concerns about package deliveries getting stolen, doubts regarding the accuracy of a DBS test, concerns about the ability to collect one’s own lab samples, and the overall positive effect of seeing a provider in-person.
Patient survey feedback on home-based pre-exposure prophylaxis
Of 58 patients in the baseline survey who requested to be contacted by their PRC about switching to home-based PrEP, 17 (29%) tried the program. This included 12 patients who completed both a telemedicine visit and a self-administered lab kit and 5 patients who completed only a telemedicine visit. Per the PRC’s experiences in working with patients receiving PrEP, some commonly reported reasons that the other 41 patients did not make the switch include: the patient stopped taking PrEP, the patient changed their mind, the PRC was unable to reach the patient, or the patient’s PrEP provider preferred in-person care. Surveys were distributed to the 17 patients who completed at least one component of the home-based PrEP program, with a 100% survey response rate. Demographic characteristics are shown in Table 1. Patients who opted to switch to home-based PrEP tended to be younger, with a median age of 27 (interquartile range 23–36).
Patients found the telemedicine visits highly acceptable (n = 17). Over 80% had positive feedback about their telemedicine visits, agreeing that it was as good as an in-person visit, telemedicine made it easier to see a health care provider, they were satisfied with their visit, and would use telemedicine services again for PrEP (Fig. 2).
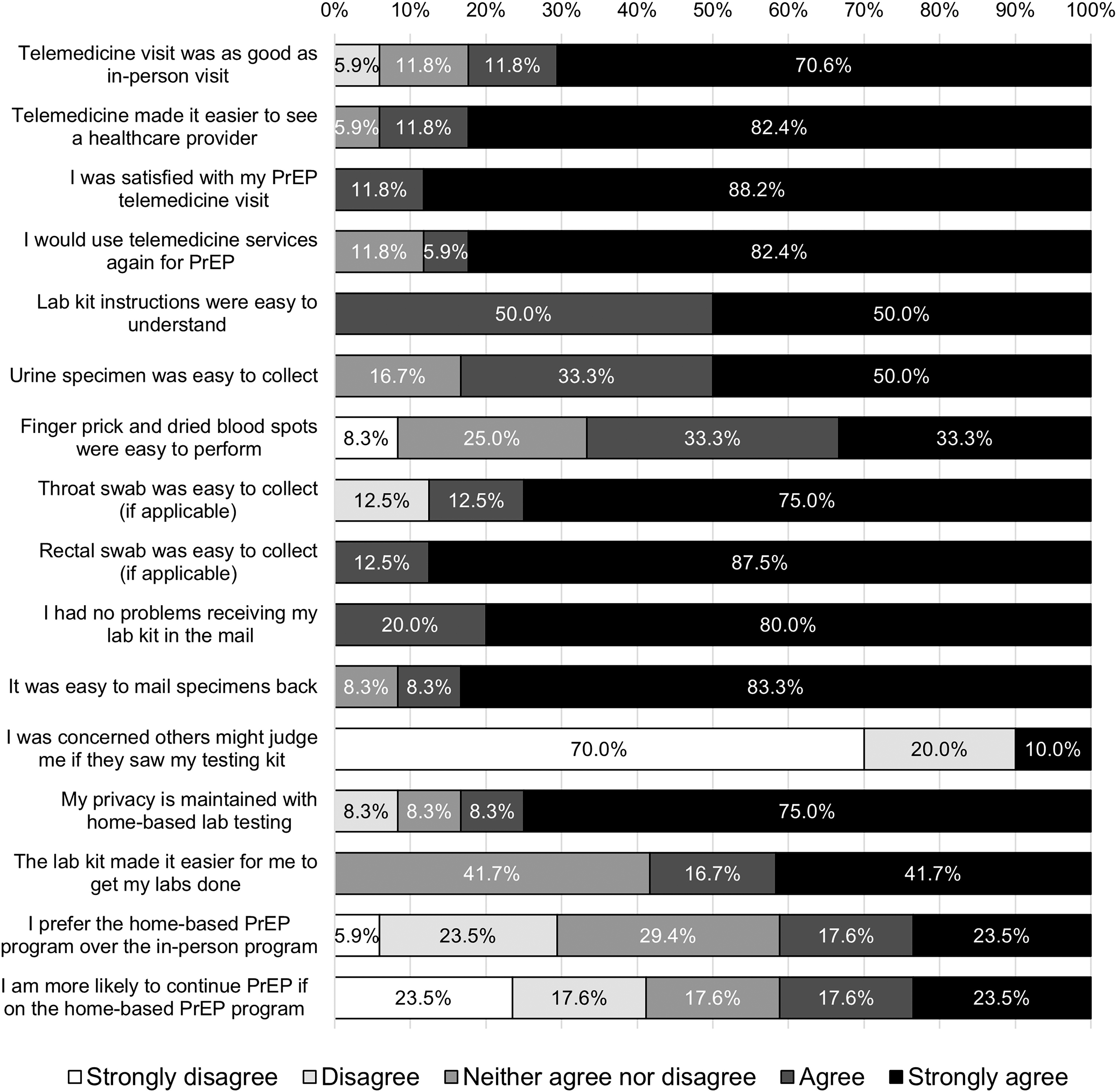
Survey of home-based PrEP users on the acceptability of telemedicine visits (n = 17), ease of use of lab kits (n = 12), and preferences on the mode of PrEP care delivery (n = 17), using a Likert scale. PrEP, pre-exposure prophylaxis.
The 12 individuals who completed a lab kit were surveyed on the ease of use of the lab kits using the SUS, which showed an average score of 80 (standard deviation 16.7) indicating excellent usability and feasibility. As shown in Figure 2, all patients agreed that the lab kit instructions were easy to understand. Most agreed that the urine, blood, throat, and rectal samples were easy to collect. They had no problems with receiving the lab kit in the mail, and most (87.5%) felt it was easy to mail the lab kit back. As for privacy of the lab kits, 90% of patients did not feel concerned about judgment from others if they were seen with the lab kit and 83.3% felt their privacy was maintained with self-testing. Over half of patients felt the lab kit made it easier to get labs done as compared to clinic-based lab testing.
Patients were asked about their preferences for the method of PrEP care delivery. When presented with the statement “I prefer the home-based PrEP program over the in-person PrEP program,” 23.5% strongly agreed, 17.6% agreed, 29.4% felt neutral, 23.5% disagreed, and 5.9% strongly disagreed (Fig. 2). When asked whether they would be more likely to continue PrEP if they were on the home-based PrEP program as compared to the in-person program, 41.1% agreed, 17.6% felt neutral, and 41.1% disagreed.
Major themes from qualitative patient interviews
Six patients on home-based PrEP were interviewed about their experience with the program, and thematic saturation was achieved. Convenience was the most common reason as to why patients liked the program. Patients expressed that it was easier to fit visits into their work schedule, there was less clinic wait time, no commute, no parking difficulties, and improved efficiency and flexibility. No one expressed concerns about telemedicine visits impairing the patient-provider relationship. In reference to the self-administered lab kits, several patients voiced the advantages of having their labs drawn by a trained professional, as this addresses the anxiety and pain of pricking one’s own finger and offloads the responsibility of following instructions on sample collection and shipping. Overall, however, these drawbacks with the self-collected lab kit did not outweigh the advantage of convenience provided by the home-based PrEP program.
Medical provider survey feedback
The five clinicians who provide PrEP care were surveyed on their experience with the home-based PrEP program, with responses ranked on a Likert scale (Fig. 3). Providers had mixed opinions regarding the acceptability of telemedicine visits, although over half disagreed that telemedicine-impaired the patient–clinician relationship or hindered clinical care. As for feasibility of the program, 40% felt that incorporating the program into clinic practices had become fairly seamless. Suggested areas of improvement were to include RPR testing, improve lab result turnaround time, reduce patient technical difficulties with sample collection, and integrate lab ordering and results into the existing electronic medical record. Overall, the program appeared acceptable to providers as 80% agreed that it made PrEP care delivery easier for patients, and 80% agreed that they would encourage their patients to use the program if it were a good fit.
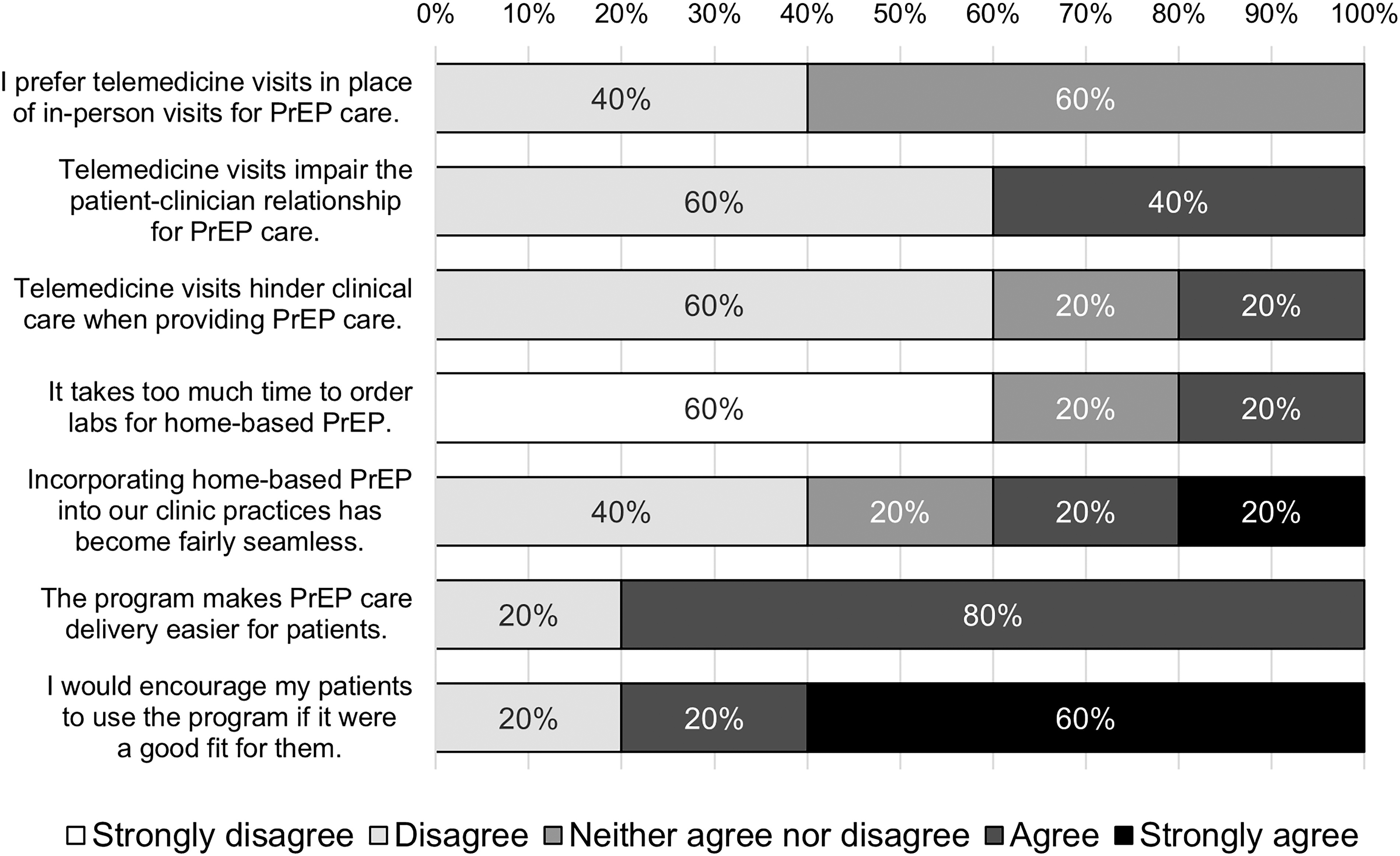
Clinician feedback on home-based PrEP using a Likert scale (n = 5). PrEP, pre-exposure prophylaxis.
Pre-exposure prophylaxis retention coordinator perspectives
The two PRCs were interviewed about barriers and facilitators to implementation of the home-based PrEP program. Barriers included delays in lab kit shipping, inability to track the shipment, and staff turnover. In addition, because of the good rapport between patients and their health care team, some patients preferred in-person appointments, especially older patients. Some individuals may also benefit from in-person visits over telemedicine visits, as they need more intensive counseling. It was observed that for patients who already struggle with adherence to PrEP and in-person quarterly visits, many will still struggle with completing the regular self-administered lab kits.
As for facilitators of implementation, the PRCs felt the program tended to be successful in patients who needed it for convenience due to living further away, traveling frequently, or having busy schedules. The program also tended to work well for patients who had historically been adherent to PrEP and clinic visits in the past, and patients who had experience with telemedicine PrEP through other commercial platforms. An initial video visit for the PRC to walk the patient through the steps of the lab kit helped with successful sample collection. Further, the program was free to patients, which encouraged its use.
Discussion
We evaluated the implementation of a home-based PrEP program that incorporated telemedicine visits and self-administered lab kits. We found high levels of interest in the program in our baseline population of PrEP users (65%). About 29% of those who expressed interest in being contacted about changing from standard clinic-based PrEP to home-based PrEP ultimately made the switch during our period of follow-up. These patients found the home-based PrEP program to be acceptable and feasible. PrEP providers had mixed opinions about the acceptability of telemedicine, but most felt that the program made PrEP care delivery easier for patients and would encourage the use of the program in patients for whom it is a good fit. Interviews with patients and PRCs suggested that the home-based PrEP program provided the strong advantage of convenience. Although many patients may benefit from in-person visits with their medical provider or PRC, a subset of patients may find home-based care to be a good fit. In addition, patients can transition between the in-person and home-based PrEP programs as needed depending on circumstances. It is unclear whether the home-based PrEP program may be helpful in re-engaging patients who are lost to care, but this would be an interesting area for further study. Barriers to success of the implementation of the program included lab kit shipping and turnaround times, staff turnover, and difficulties with collecting blood for DBS tests.
These results fit with other pilot studies in the existing literature demonstrating feasibility and acceptability of telehealth-based PrEP programs. Prior studies have shown that such programs are viewed favorably by patients and, as seen in our study, have cited accessibility, convenience, privacy, ease of use, and low stigma. 18,24,25 In one study, 87.5% of clients reported high satisfaction with the program, similar to the over 80% of patients in our study who had positive feedback about telemedicine visits. 26 One study found a similar SUS score of 76.91 for a self-administered PrEP lab kit in which participants collected finger prick whole blood in a gravity-fed microtube, urine specimen, and rectal and pharyngeal swabs. 16 This study had a different home PrEP program that did not offer telemedicine visits, but instead reduced quarterly visits to one annual in-person clinic visit, with additional visits as needed based on laboratory results and a behavioral survey. That study found that 40% of participants in their home PrEP program felt they would be more likely to persist in care if the program was available. We found a similar response in our study group, with 41% of users reporting that they were more likely to continue PrEP if they were on our variation of a home-based PrEP program as compared with the clinic-based program. Another study examined the feasibility and acceptability of self-collected lab samples for PrEP and SARS-CoV-2, and found that participants had positive feedback on the lab kit and a mean SUS score of 69.9. 17 Our interviews with patients and PRCs revealed that some patients found it difficult to collect their own blood samples. This coincides with several other studies that have demonstrated patient difficulties with blood sample collection. 17,25,27
Our study has various limitations. Our numbers were low, with only 17 of the 102 PrEP patients opting to try home-based PrEP; therefore, it is difficult to generalize our findings. Many patients who expressed initial interest in home-based PrEP ultimately did not enter the program, and the reasons for this should be explored in a future study in order to assess the barriers to uptake of the program and how they should be addressed. Despite the low numbers, our findings are consistent with other existing studies. Because of the pragmatic nature of our study, the participants in home-based PrEP were self-selecting, which likely resulted in overall positive feedback. However, this pragmatic study is likely an accurate representation of what would be experienced in a real-world clinical setting, with patients deciding whether they want to receive their care in-person or remotely. Because our pilot study focused on studying the implementation of a home-based PrEP program among existing PrEP users, we cannot make conclusions about whether this program will increase PrEP uptake and retention. However, this would be an interesting area for future study. Further, costs were not a consideration in this study because any individual who did not have insurance or was underinsured was able to have the costs of the telemedicine visit and lab kit covered by the clinic’s funding. This is unlikely to be the case in other clinical settings.
Overall, we received positive feedback on a home-based PrEP care delivery model, which included telemedicine visits and self-administered lab kits mailed to the patient’s home. PrEP care delivery is not one-size-fits-all and a home-based program is an excellent tool in our toolkit that can be used by patients for whom it is a good fit.
Footnotes
Acknowledgments
The authors want to thank all participating patients for sharing their experiences with us, and the authors thank the providers for their contributions to this work.
Ethical Approval
The study protocol was approved by the Institutional Review Board (IRB) of the University of Pennsylvania.
Consent
Informed consent was obtained from all participants.
Authors’ Contributions
T.Y., H.K., and F.M. helped conceptualize the study. H.S., T.S., and D.S. assisted with study implementation. T.Y., L.L.C., HK, and F.M. contributed to instrument development. T.Y., D.Z., and H.S. performed data collection. L.L.C. led data curation. T.Y. performed data analysis. T.Y. led the article writing and all authors contributed to article development and review. All authors have read and approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the US Department of Health and Human Services (HHS) Agency for Healthcare Research and Quality (AHRQ) under a