
Abstract
Little is known about long-acting HIV treatment implementation with trans women. We piloted and evaluated the implementation of novel strategies to increase uptake and use of long-acting HIV treatment among trans women in San Francisco. In 2022, qualitative formative nominal groups (n = 8) and in-depth interviews with providers (n = 11) were conducted to elicit facilitators and barriers to long-acting HIV treatment delivery among trans women living with HIV and to inform a pilot delivery model. Between August 2023 and August 2024, participants were enrolled into the program. Sequential mixed methods were used to evaluate formative and implementation data to understand barriers to starting long-acting treatment. Barriers for trans women were concerns about side effects, fear of needles, and difficulty adhering to bi-monthly injections. They were also concerned about missed injections from lack of transportation and incarceration and medical mistrust. Providers were most concerned with participant adherence due to social determinants (e.g., housing) and behavioral health challenges (e.g., methamphetamine use, mental health disorders). Buttock fillers and implants, patient worries about interactions with hormones, clinical barriers (e.g., availability of genotyping data), insurance, and managing prescriptions were also potential barriers. A significant barrier to implementation was the burden on referring clinic providers for eligibility screening and many trans women who were referred declined participation or were not eligible due to contraindicated clinical histories. Our study identified barriers to implementing long-acting HIV treatment among trans women living with HIV and provides novel implementation insights for clinics and interventions serving this community.
Introduction
Trans women experience significant disparities across the HIV care continuum. In San Francisco, 42.3% of trans women 1 are living with HIV. While San Francisco meets recommendations for improving trans health through gender-affirming services, trans women have a lower proportion of linkage, retention in HIV care, and viral suppression than other groups. Only 76.5% of trans women achieved viral suppression in 2020, which is well below our 90% goal in San Francisco. 1,2 Cabotegravir/rilpivirine long-acting (CAB-RPV LA) as a monthly injectable could help address disparities in viral suppression among trans women.
Long-acting injectable treatment may be acceptable to trans women, given familiarity in the population with injectable hormones. 3 Yet uptake among trans women and other marginalized populations in San Francisco has been slow to date, which is consistent with data on long-acting HIV treatment uptake in the United States overall despite models predicting high uptake and significant impact on improving viral suppression. 4 Little data exist on implementation barriers to long-acting ART among trans women.
The slow uptake of long-acting HIV treatment is a roadblock to reducing disparities in viral suppression among trans women and other populations affected by HIV. Tailored clinics for delivery of specialty services have been used successfully within the San Francisco Department of Public health (SFDPH) (e.g., methadone clinic 5 ) and other health systems (e.g., PrEP clinic in Kaiser 6 ). Public health clinics that engage trans women are an important setting to evaluate delivery of long-acting HIV treatment. The SFDPH is a leader in HIV research, care, and gender-affirming services for trans women. 7 Our team was able to significantly improve PrEP uptake among trans women in San Francisco using a specialty clinic model tailored to addressing the PrEP needs of trans women through low threshold PrEP delivery and support outside primary care. 8,9
Our team implemented a similar low threshold delivery model tailored to increasing uptake of long-acting HIV treatment among trans women in San Francisco. Formative data were collected with trans women and providers to identify barriers to implementation and uptake of long-acting HIV treatment among trans women living with HIV and to refine our intervention. This study was conducted to assess anticipated and realized implementation barriers and successes to an intervention to promote long-acting HIV treatment uptake and enrollment among trans women living with HIV in San Francisco. The goal was to identify factors that may need to be addressed in future research and clinics seeking to offer long-acting injectable HIV treatment to trans women living with HIV in the United States.
Methods
We used an implementation science approach to both refine and evaluate a trans women-tailored injectable HIV treatment intervention to improve uptake and adherence to this relatively new treatment regimen. The intervention delivery model was tailored to offer education about a referral program for CAB-RPV long-acting injectable HIV treatment to providers of both gender-affirming and HIV care at collaborating public health and community clinics with transportation and peer navigation support. Core components of the delivery model included (1) delivery of injectable HIV treatment via a trans friendly injection clinic at an HIV research unit within SFDPH centrally located in San Francisco; (2) adherence support from a peer navigator at in-person visits and via text-messaging; (3) provider education about injectable CAB-RPV treatment and how to refer patients to the injection clinic; and 4) transportation support to the clinic ($50 for each injection visit). Participants had access to Weltel, a text messaging platform that previously was shown to be effective in increasing adherence to oral HIV treatment and virologic suppression. 10 In this study, Weltel was adapted to support long-acting injectable treatment, with weekly text messages about U = U (undetectable = untransmittable), check-ins about medication side effects, and facts on transgender history (to engage participants using content other than HIV). Participants continued receiving their primary care at their home clinic, and progress notes for injection visits were entered into the electronic medical record that could be viewed by the home clinic. The intervention delivery model was refined using formative qualitative data and sequential mixed methods were used to evaluate implementation.
Formative data collection and analysis
During the first 3 months of the study, our team conducted two pre-implementation nominal group technique (NGT) 11 discussions with trans women living with HIV (n = 8) and 11 in-depth interviews with providers who were known to serve trans women with HIV in clinics likely to refer to the program. NGT is a structured small-group method for qualitative data collection. The goal of NGT is to gain consensus on a topic, rather than probe for variation in perspectives. NGT was chosen so that the research team could identify priority targets for reducing barriers and improving access and utilization of this new treatment modality. For the NGT discussions, we purposively sampled trans women receiving HIV care within San Francisco Department of Health (SFDPH) clinics whose age, race/ethnicity, and length of time living with HIV would most closely resemble participants for the intervention. NGT discussions and in-depth interviews were used to determine the main barriers and potential facilitators to long-acting HIV treatment, and to seek feedback on our implementation strategies for an integrated delivery model.
HIV providers who cared for trans women within the SFDPH and other local gender-affirming care clinics (n = 11) participated in pre-implementation key informant semi-structured in-depth interviews to assess acceptability and feasibility of our intervention delivery model and long-acting HIV treatment among trans women patients. Known providers in San Francisco who were potential trans woman participant referral providers were directly outreached to via e-mail. We conducted semi-structured in-depth interviews with providers in referring clinics.
All groups and interviews were audio-recorded, and field notes were written up to provide brief synopses of findings captured by the qualitative field team. Nominal group rankings were scored to elucidate what concerns and benefits were the most important among participants. Qualitative data was coded and analyzed for content, focused on examining feasibility and acceptability of the implementation strategies and overall delivery model proposed for this project. Data were used to make refinements to the intervention delivery model.
Data-Informed implementation of delivery model
The intervention was implemented in August 2023. Participants were eligible for study participation if they were age 18 or older, male sex at birth and had a gender identity other than man, living with HIV, eligible to receive long-acting CAB-RPV per the FDA-approved label, virologically suppressed within the last 6 months, interested in initiating or continuing CAB-RPV LA for HIV treatment and willing to receive injections at Bridge HIV, currently receiving or willing to receive HIV care at one of the collaborating primary care clinics, had a cell phone and active service or another reliable method of contact, and were fluent in English or Spanish. Exclusion criteria included inability to receive gluteal injections, plans to move away from the site area within the next 9 months, and history of known or suspected drug resistance that would compromise the CAB-RPV regimen.
Participants were referred by gender-affirming care clinics within the SFDPH and a collaborating community-based clinic serving trans women for monthly or bi-monthly CAB/RPV injections delivered through a trans friendly injection clinic over a 9-month study period. Referrals for clinical care were combined with additional implementation strategies including peer navigation support. The study aimed to enroll 40 trans women into the pilot delivery model. An assessment of referrals for candidate patients to enrollment was conducted.
Exit interviews
Qualitative exit interviews were conducted with participants upon completion of the pilot study to further elicit feedback and suggested changes to the delivery model. Qualitative exit interview data provided information on motivations for taking long-acting HIV treatment, facilitators and barriers to participation in the study, experiences with accessing and using long-acting HIV treatment, and feedback on services received as part of the intervention delivery model.
Ethical review
The University of California San Francisco Institutional Review Board performed an ethical review of this study. Participants provided written informed consent.
Results
Formative data on anticipated facilitators and Barriers-Trans women
Most trans women participants in the nominal groups were African American, lived in their own home or apartment, were unemployed, reported good or excellent HIV treatment adherence and were interested in switching to long-acting injectable HIV treatment.
Trans women participants' main anticipated barriers were related to the medication. The main barriers anticipated by trans women and providers were side effects, a fear of needles, and difficulty adhering to bi-monthly injections (Table 1). Some trans women were also concerned about possible interactions between recreational substances they use, interactions with fillers and surgeries they have in their buttocks, and possible interactions with other medications they take. Some trans women were also skeptical of being early adopters as they were worried about whether the medication was adequately tested with trans women for safety and efficacy. These concerns were also related to medical mistrust and misgivings about new therapies offered by pharmaceutical companies. Some trans women were worried that the clinical trials did not focus on trans women specifically so they felt that they could not know conclusively if the medication worked, was safe for their bodies, and did not have a negative interaction with substances they used recreationally, hormones, or other medications they were taking. Others wanted to know that the medication was safe for people ages 55 and older and people in African American communities. Some trans women mentioned being worried that the new regimen was not as high quality as their current regimen. Many trans women also questioned the reason for someone who is virally suppressed to switch to a new medication if their current regimen is working well. As one participant stated, “This medicine has kept me alive for yeeeeeears… Why would I switch to something else?”
Nominal Group Technique Barriers Identified
Implementation barriers were also expressed. Most trans women were worried about participants missing visits and developing drug resistance. Some trans women wanted to have their visits at their home clinic and they wanted to make sure there was transportation available so all participants would make it to their follow-up injection appointments. Participants also expressed concerns about getting injections if they were incarcerated during the study. They worried that their treatment would be interrupted if they were held in detention. Some participants preferred to have their injections at their home clinic due to concerns about quality of care and care management if they were to switch to a new care site and providers, even if temporarily.
For facilitators, many trans women were excited about having an option other than a daily pill for HIV treatment. Trans women expressed that managing oral medication posed logistical challenges in their lives and resulted in undue stress, including the stress of remembering doses, difficulties getting to pharmacies, and issues with refills and transportation. These factors often led to frustration and time constraints due to work schedules. Some trans women felt that having transportation and peer support could be helpful components of the long-acting HIV treatment intervention, and they had mixed feelings about text-messaging support as the way to communicate as some said they were not able to use their phones on a regular basis or did not regularly communicate via text. Many participants felt that other trans women living with HIV, particularly older trans women and those known in the local community, would be the best champions for promoting the intervention delivery model. Participants also thought that incentives are critical for promoting the intervention. Altogether, trans women wanted more options for HIV treatment. As one person expressed, “Everybody’s health is different. I think that a new breakthrough would be good for all of us. I just hope that it is effective.”
Formative data on anticipated facilitators and barriers-providers
Providers interviewed were medical doctors, nurse practitioners, and staff at SFDPH and other community clinics in San Francisco that provide gender-affirming care to trans women living with HIV. Like for trans women formative participants, providers' anticipated barriers primarily focused on the challenges with long-acting HIV treatment and fewer concerns were mentioned about the intervention delivery model. Most of the anticipated barriers expressed by providers were categorized as those related to social determinants (e.g., housing) and behavioral health issues (e.g., methamphetamine use, mental health disorders) that could affect visit attendance (Table 2). Providers’ main concerns were related to risks for developing resistance to a class of HIV treatment medications for those who missed injection appointments. Providers experienced in serving trans women mentioned that trans women face many challenges to HIV treatment and visit adherence with most stemming from social determinants like housing instability, immigration, and medication eligibility and access. Social determinants barriers in combination with underlying trauma resulted in having a detectable viral load and missing HIV care appointments. Providers were also concerned about the presence of buttock fillers used commonly by trans women. One provider said he would not give buttocks injections to trans women patients with fillers or silicone. Providers shared trans women participants' concerns that trans women would not use injectable HIV treatment for fear of interactions with hormones.
Anticipated Barriers from Provider Perspective
Providers also had logistical concerns like the absence of data on existing HIV treatment resistance in medical records, obtaining lab results for monitoring, securing insurance coverage, and management of prescriptions. Providers felt that there was not a strong rationale to change treatment regimens if existing oral treatment was already working well and trans women were not eager to try injectable treatment. Providers agreed that supports would be needed to ensure that trans women get their injections in a timely manner and thought that long-acting HIV treatment could be a beneficial treatment for a sub-group of trans women who were motivated by pill fatigue and who had fewer barriers to maintaining viral suppression.
Refinement of delivery model
Based on the formative data from trans women living with HIV and providers, along with our experience during implementation, we refined the delivery model (Table 3). The peer navigation manual was amended to include counseling points to address medical mistrust; provide information on the safety of CAB-RPV and CAB-RPV while using hormones, potential benefits of a monthly or bi-monthly HIV treatment (reduced stigma, peace of mind around dosing), and known side effects; and, strategies to support adherence to injection visits, including how to handle missed injections. The manual also included referrals for mental health and suicidality and other support services including behavioral health, case management, food assistance, housing and legal assistance, substance use treatment, and gender affirming care. Transportation was an added intervention component to facilitate visit attendance for injections. To address insurance coverage issues and concerns, an additional staff member was trained and dedicated to insurance navigation. To address concerns regarding fillers and implants, clinical staff performing injections were trained on assessing location of prior fillers/implants, and whether CAB/RPV injections could be safely administered in the ventrogluteal or dorsogluteal locations (i.e., buttocks). Referring providers were busy and so provider detailing materials were created to address key provider questions and education instead of delivering in-person didactic sessions. Additionally, referrals via telephone encounters in the electronic medical record were identified as a more efficient strategy than completing e-consults through the medical record to initiate referrals. Study clinicians also shared the responsibility of making clinical eligibility assessments, mostly by examining potential participants' medical records in depth and obtaining a detailed HIV medication treatment history to assess for medication resistance.
Characterization of Implementation Strategies and Refinements for CAB-RPV LA Delivery Model
CAB-RPV LV, Cabotegravir/rilpivirine long-acting; HER, electronic health record; SFDPH, San Francisco Department of Public health.
Intervention implementation-referral challenges
Once the intervention model was refined, the team conducted education with potential referral providers using the developed educational materials (Appendix), but referrals were slow. We asked one provider for detailed insights as to what are the barriers to referring potential participants. Half of potential referrals (N = 23) from this provider’s panel were not eligible due to potential drug resistance (see Table 4), while about 40% of potential referrals were not virally suppressed. Other referral challenges were potential participants with inconsistent HIV care visit attendance and social determinants barriers like competing mental health issues that made medication management difficult. Despite these challenges, some trans women were referred to the intervention. One of the challenges with moving from referral to enrollment was that some trans women were not reachable after being referred or did not show up for intervention enrollment visits.
Referrals Barriers from Gender Affirming Care Providers to Cheeky Study, N = 23 Potential Referrals
Figure 1 shows how referral challenges resulted in few completed enrollments to the project overall. Of the 21 referrals that occurred, 6 people were enrolled and initiated long-acting HIV treatment, 9 declined participation, 5 were ineligible (3 medically ineligible, 2 no longer at a partner clinic), and 1 had a scheduling conflict. Of the six, one discontinued CAB-RPV due to an unrelated medical condition, and another ceased using long-acting HIV treatment due to side effects.
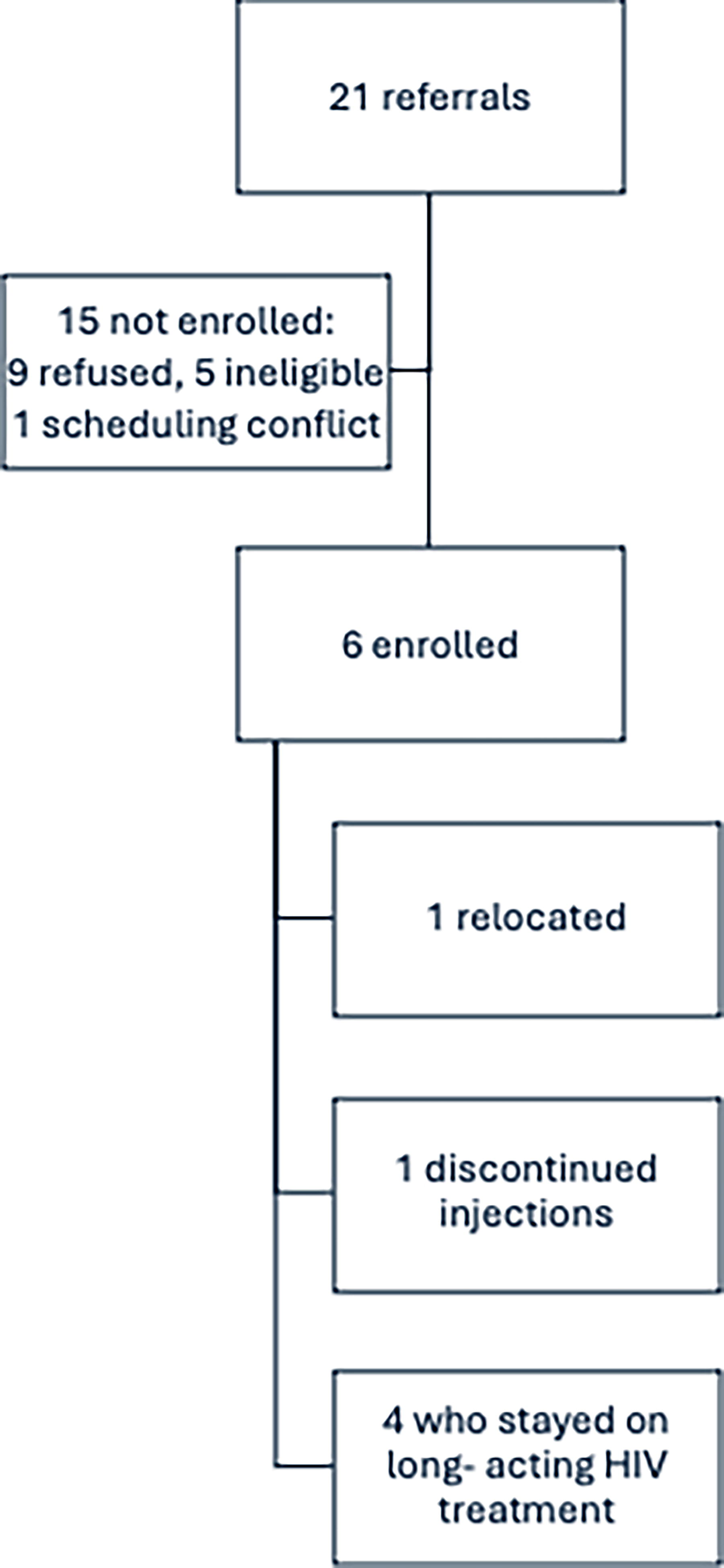
Referrals to enrollment and study completion.
Qualitative exit interview data highlight some of the challenges trans women faced with long-acting injectable HIV treatment, most of which included physical pain from injections. Specifically, participants reported pain at the injection site. Pain experienced after the injection was reported by all trans women at least once, and other side effects reported were stiff muscles, sleeplessness, the inability to sit on one side, and trouble walking and putting weight on the side where the injection was given. One trans woman reported mood swings from the injections. One woman dropped out because of the pain she experienced.
The logistical improvements associated with long-acting antiretroviral therapy made a significant positive difference in participants’ lives, regardless of the high bar to receiving the intervention. The proximity to the intervention injection clinic made accessing injections easier, as both the clinic and lab were conveniently located close to home. Scheduling follow-up appointments for injections was straightforward, alleviating worries about timely access to treatment. The care provided by knowledgeable staff and navigators also contributed to a positive experience. Participants reported that information about the intervention and treatment was clearly explained, and injections were administered with minimal pain. The support from a navigator was invaluable, offering reminders and connecting individuals to resources like support groups, substance use assistance, social work, and housing resources when needed. The proactive approach of staff, who consistently provided information on upcoming events and outreach efforts for trans women of color, fostered a sense of community. Overall, the gender-affirming and respectful environment, coupled with effective peer navigation, significantly enhanced engagement with the study and supported adherence to follow-up visits.
Discussion
Trans women and providers shared expected and novel insights for long-acting HIV treatment implementation with trans women. The main provider concern for implementation of long-acting HIV treatment among trans women was drug resistance from lack of adherence to injection visits. Providers were concerned that housing, immigration, health insurance and other social determinants challenges faced by many trans women might affect engagement in HIV care, along with trauma, mental health and substance use impacting visit attendance. Trans women wanted to make sure injectable HIV treatment was offered with the necessary supports to ensure adherence, like transportation assistance, to ensure visit attendance was as feasible as possible. Prior literature on injectable PrEP and HIV treatment 3,12 cited concerns trans women have about injectables in their buttocks, which was also expressed by trans women in our study. Trans women were also concerned about CAB/RPV interactions with hormones, recreational substances used, and other medications taken. Fear of and experiences of injection site pain occurred among trans women, which may present an important barrier. Providers have expressed injection site pain as a concern for their patients as well. 13 Many trans women also had a fear of needles, which may have to be explicitly addressed in implementation.
Trans women also brought up concerns for missed injections among those who become incarcerated while on long-acting HIV treatment. The lifetime prevalence of incarceration among trans women in San Francisco is 67% and is associated with living with HIV. 14 Incarceration could result in treatment interruption if CAB/RPV is not available in the detention facility and resistance to this class of drugs can occur for those who do not get their injections on time. Clinics who serve highly justice system involved participants may need to coordinate with carceral systems to provide long-acting HIV treatment and/or systems for ensuring people receiving CAB/RPV are identified upon entry.
Various responses related to mistrust were also expressed by participants in our study. Trans women were skeptical about trying a new medication when their existing one is already working, and were not sure about safety or efficacy at many axes of identity, including for trans women, African Americans, older people and people from marginalized populations. Trans women also expressed mistrust of the government, the Food and Drug Administration and pharmaceutical companies. Medical mistrust is a known barrier to health care engagement among trans women, 15 and was recently found to reduce intentions of using long-acting PrEP in a study of trans women. 16 Mistrust in medicine and structures that create and regulate medication may also be higher in the Covid-19 era because of widespread misinformation during the pandemic. 17,18 The high mistrust may also reflect the experiences of people in our sample, which was comprised mostly of African American trans women, given the mistreatment of African Americans in medical research and services. 19,20 Mistrust could be an important barrier to uptake of this new HIV treatment and all future HIV prevention and treatment modalities that are currently being implemented and tested. For example, participants expressed wanting to see if the medication is effective and safe in other communities before endorsing use for trans women. At the same time, some trans women expressed having high trust with their existing primary care providers and wanting to get the injection with those individuals. Interventions to implement new HIV treatment medications may need to lean on the trust built between those providers and trans women to promote uptake for those who could most benefit.
The most significant barrier to implementation of our intervention for improving long-acting injectable HIV treatment uptake and adherence among trans women was the limited candidacy for referrals. Few trans women were candidates for the intervention due to not meeting eligibility criteria for viral suppression, medication resistance, or existing HIV treatment visit adherence challenges. Barriers identified in the formative phase did bear out to some degree, but many of the concerns expressed by providers and trans women did not come to fruition. Resistance to prior medications emerged as the biggest issue for referrals to the intervention and long-acting HIV injectable treatment eligibility, compounded by other factors that may impact the ability to adhere to more frequent clinic visits, such as mental health challenges, substance use, housing instability, and other challenging social determinants. The burden on providers to identify suitable candidates for long-acting injectable HIV treatment was also notably high, as it required detailed chart reviews and medical histories, assessment of resistance and psychosocial factors, which are all time-intensive tasks. Strategies to limit provider labor and streamline referrals to this new treatment modality may increase utilization. Additionally, the need for more frequent clinic visits further increased the burden on both providers and clinics, which has been found to be a barrier in other research in the United States. 21 Efforts to increase long-acting HIV treatment in clinics will have to assess capacity for doing so.
Among those referred, enrollment into the intervention was often hampered by missed enrollment visits, and some trans women expressed reluctance to try long-acting injectable HIV treatment or were difficult to reach for enrollment purposes, as indicated by instances of both active and passive refusals. Providers from a large community-clinic in New York City similarly found barriers to long-acting HIV treatment that included client readiness and concerns about injection-site reactions. 12 There were also hard refusals, with no reasons documented. Some individuals did not follow up to enroll, which may be partly due to the lag time between discussions about long-acting HIV treatment and delays in obtaining the medication due to insurance coverage issues. Systems issues were also a pre-implementation concern of providers who worried about logistics like obtaining the medication via insurance and more frequent appointment management burden for the clinic and patients. Similar concerns were related to providers’ lower perceived need of long-acting injectable HIV treatment. 21
Long-acting HIV treatment is an important new choice for people living with HIV; however, implementation challenges may be high, especially for populations that are treatment experienced and face challenges to HIV care engagement. Implementation of our intervention was modified to address fears and concerns of trans women and providers, like medical mistrust, and we modified education and referrals processes and offered transportation to ensure trans women could make it to scheduled visits. Some individuals struggled with the enrollment process, highlighting broader difficulties in maintaining contact and avoiding missed visits for injections. Various other barriers were identified pre implementation, including mistrust of the medical system, concerns about injections affecting cosmetic fillers, and the general skepticism towards government and pharmaceutical companies. The enrollment of trans women in long-acting HIV treatment was affected by several factors, including hesitation to change treatment regimens, fearing potential loss of viral suppression. This may have been compounded by the fact that many trans women in San Francisco have been living with HIV for a long time and may have developed resistance to other medications. The requirement for viral suppression as an eligibility criterion further limited enrollment. Additionally, the process was labor-intensive for health care providers, who needed to thoroughly review patient information, consult with their teams, and make referrals. Mental health issues and challenges with maintaining appointment attendance also played a significant role in the low referral rates. While not all trans women were suitable candidates for this intervention—including those who were already virally suppressed—there is research suggesting the need for expansion of this novel HIV treatment regimen among people living with HIV. Researchers in San Francisco who piloted this new HIV treatment regimen with people who were not virally suppressed demonstrated high rates of virologic suppression after initiating CAB-RPV. These researchers caution against limiting availability of CAB-RPV to only those who are virally suppressed and adherent for fear of reinstating barriers to HIV treatment progress with assumptions about resistance and adherence. 22 Our study provides novel implementation insights for clinics and interventions that offer long-acting HIV treatment to trans women living with HIV. Our study also provides data to suggest the expansion of long-acting HIV treatment to trans women who are struggling with viral suppression along with the need for building trust in the medical system so they can benefit from additional choices in HIV care.
Footnotes
Authors’ Contributions
E.C.W. designed the study, conceptualized the research question, and drafted the article. J.M., S.S., A.L., and G.M.A. worked with E.C.W. in the developing the research question. E.C.W., S.S., G.M.A., and E.S. conducted data analysis. E.S., C.-D.A., N.W., J.V., H.S., and A.L. oversaw study implementation, data collection, and study coordination. G.M.A. and A.D. led study implementation. S.B., A.L., J.M., and G.M.A. assisted with article development. All the authors reviewed the article and approved the submitted version.
Author Disclosure Statement
The authors have no competing interests to declare.
Funding Information
The funding was provided by ViiV Healthcare grant# 214124 with award to A.L.