
Abstract

To the Editor:
The introduction of cabotegravir and rilpivirine long-acting (CAB + RPV LA) for HIV treatment in 2021 marked a groundbreaking change for people with HIV (PWH). For the first time in the history of HIV, it became possible to be treated without daily medication, instead utilizing bimonthly intramuscular injections.
Nevertheless, in the face of this revolution, HIV RNA monitoring remains anchored in excessive caution, so much so that there is currently no consensus on the optimal timing of HIV RNA evaluation in people receiving LA therapy. While some guidelines provide no specific recommendations, 1 the British HIV Association guidelines, 2 based on the design of registration trials, advise HIV RNA assessment every 2 months. Furthermore, the implementation of bimonthly monitoring has the potential to address any concerns that may arise, such as a possible reduction in plasma concentrations of RPV and CAB, in addition to limiting the risk of emerging resistance. 3 In this regard, it is important to note that health care providers worldwide have expressed concerns about missed appointments and treatment adherence. A recent study conducted in Spain, which surveyed 154 physicians, found that nearly half of them were concerned about the introduction of LA therapy, particularly in terms of adherence. 4
However, such an intensive approach may represent over-supervision for most PWH on CAB + RPV LA, identified based on the eligibility criteria specified in the international guidelines, 1 and may instead be reserved for selected populations. Indeed, bimonthly HIV RNA evaluation risks restoring PWH to a pre-Highly active antiretroviral therapy era: in fact, such close monitoring has never been indicated for any of the currently available regimens, nor for earlier, even less effective combinations or low-barrier agents, except in high-risk settings. 5 This can potentially increase stigma due to frequent required visits and procedures, discourage individuals from accessing this innovative treatment option, arising fears about its actual efficacy and increase both time and financial costs associated with frequent hospital appointments and blood testing.
These concerns regarding its actual efficacy are, in fact, not substantiated by real-world data, which, similarly to registrational studies, demonstrate very low virological failure (VF) rate, ranging from 0.4% to 4.1% in published studies. 6 In addition, it is important to note that the most recent data from the follow-up of clinical trials 7,8 have shown that increasing the frequency of HIV RNA monitoring led to the detection of more blips, both in CAB + RPV LA and those on oral bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF). In none of these cases blips were associated with subsequent VF, demonstrating no real clinical advantage from such close monitoring.
In order to mitigate the aforementioned risks while allowing early identification of potential VFs during CAB + RPV LA therapy, one potential solution would be the implementation of a risk stratification system, which could personalize and stratify HIV RNA monitoring intervals (Fig. 1). Treatment is offered to eligible PWH based on the criteria of the international guidelines, 1 namely: (1) HIV viral load suppressed for at least 6 months, (2) HBsAg negativity, and (3) no resistance-associated mutations (RAMs) to RPV or CAB. The presence of RAMs is assessed by evaluating a previous genotypic resistance test on HIV RNA [genotypic resistance test (GRT)] and eventually performing a baseline next-generation sequencing (NGS) test on HIV DNA if a GRT is not available. Although proviral DNA genotyping is not the preferred tool to verify the presence of archived RAMs, the European guidelines suggest that it may be considered in PWH with multiple VFs, unavailable resistance history, or too low viremia to allow for RNA sequencing at the time of switch. 1,9
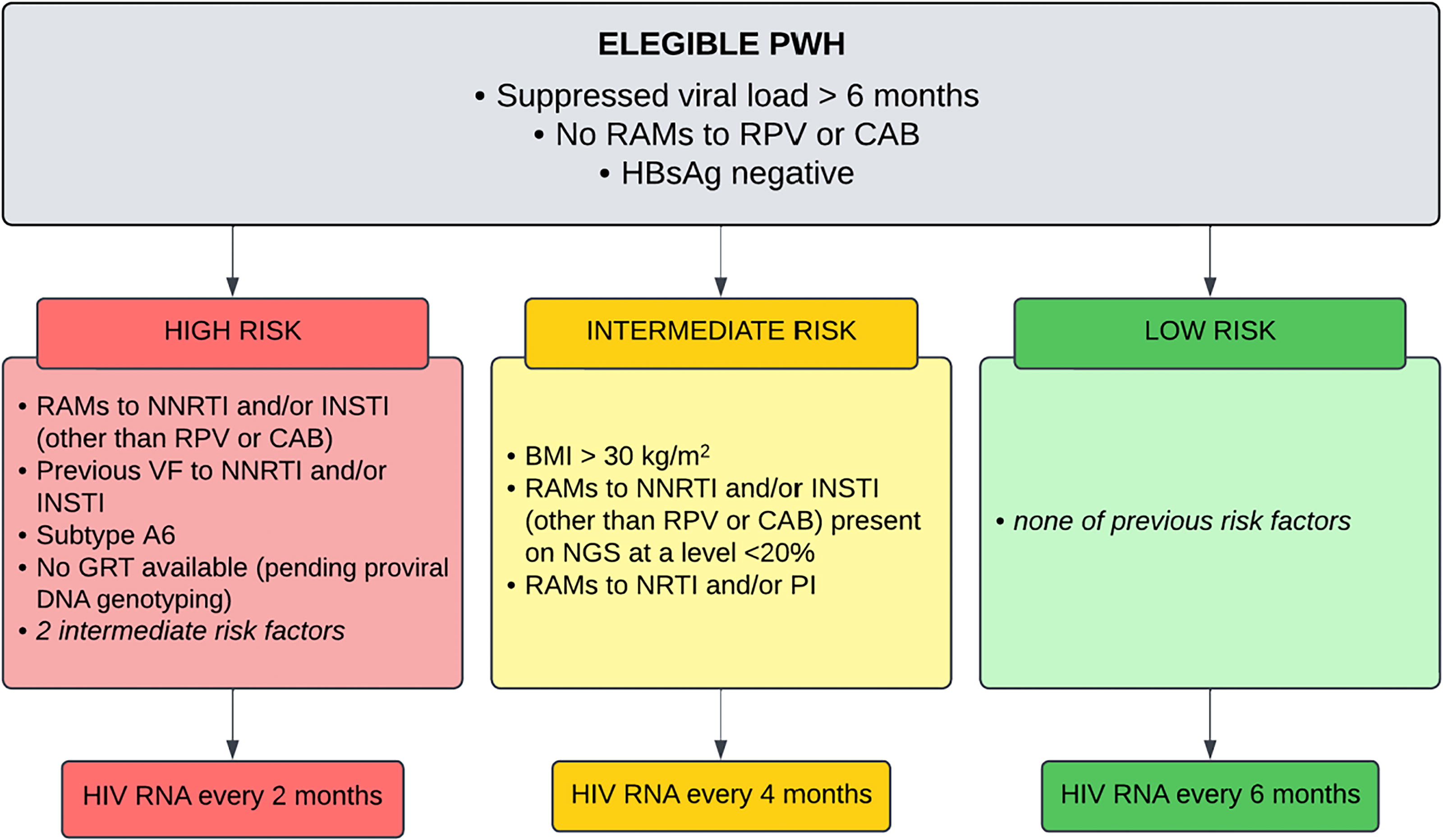
Risk stratification of viral failure for PWH on long-acting RPV and CAB treatment. BMI, body mass index; CAB, cabotegravir; GRT, genotypic resistance test; HBsAg, hepatitis B surface antigen; INSTI, integrase strand transfer inhibitors; NGS, next-generation sequencing; NNRTI, nonnucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; PWH, people with HIV; RAMs, resistance-associated mutations; RPV, rilpivirine; VF, virological failure.
Eligible PWH are stratified in three risk classes: high-risk individuals are PWH with one of the following factors: (1) RAMs for nonnucleoside reverse transcriptase inhibitors (NNRTIs) and/or integrase strand transfer inhibitors (INSTIs), other than those to RPV or CAB, detected both with conventional techniques or with NGS above the 20% threshold; (2) previous VFs to NNRTIs and/or INSTIs; (3) subtype A6 1 ; (4) individuals without available GRT, pending proviral DNA genotyping (subsequently reclassified based on DNA results); (5) two intermediate-risk factors. PWH at intermediate-risk are those with one of the following: (1) BMI >30 kg/m2; (2) RAMs for NNRTIs and/or INSTI on NGS, only if detected under the 20% threshold 10 ; (3) RAMs for NRTIs and/or PIs, not because of the increased risk of VF, but rather because of the limited future options in case of VF. All other PWH are considered at low-risk. HIV RNA is then performed 1 month after the first injection; then, we propose an HIV RNA monitoring every 6, 4, and 2 months for the low-risk, intermediate-risk, and high-risk group, respectively.
In our center, 58 PWH have completed at least 6 months of follow-up after initiation of CAB + RPV LA (Table 1). All PWH started CAB + RPV LA without the oral lead induction phase. Fifty PWH are still on CAB + RPV at the time of writing, with persistently HIV RNA <50 copies/mL. Eight individuals discontinued the treatment: four due to adverse events (Table 1), one due to personal choice, one for pregnancy, one for retrospective viewing of the documentation of an E138Q mutation in the historical GRT, and one due to a virological blip (HIV RNA 236 copies/mL) detected after sixth dose. At baseline, this individual was classified as low-risk: both RNA and DNA GRT were available, and injections were consistently administered as scheduled (within a ±7-day window of the previous administration). Although the subsequent virological evaluation showed an undetectable viral load while still on CAB and RPV, we decided to switch back to oral antiretroviral therapy (B/F/TAF), obtaining persistently HIV RNA <50 copies/mL over the following 6 months of follow-up.
Main Characteristics of People with HIV on Long-Acting Treatment
Three individuals are currently awaiting their results and, in the meantime, are undergoing viral load monitoring every 2 months.
All reporting pain at the injection site, one also hyperpyrexia.
BMI, body mass index; GRT, genotypic resistance test; HBsAg, hepatitis B surface antigen; INSTI, integrase strand transfer inhibitors; NGS, next-generation sequencing; NNRTI, nonnucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor; PWH, people with HIV; RAMs, resistance-associated mutations; VF, virological failure.
The significant change brought about by LA regimens requires a rethink of the overall management of PWH undergoing this treatment.
A tailored, risk-based strategy could be a possible option rather than a one-size-fits-all approach.
A subpopulation that was not considered in our study includes individuals experiencing challenging social determinants of health, who could also benefit from an individualized follow-up that takes these factors into account, ensuring that their comprehensive needs are fully addressed. 11
Therapeutic drug monitoring (TDM) was not available at our center and, considering its unavailability in many other centers, was excluded from the criteria, as its inclusion could limit the broader applicability of the scoring system. Further, recent data suggest that the likelihood of failure is independent of pharmacodynamic parameters. 12,13
Moreover, baseline HIV RNA levels and lack of virological control during oral therapy may also play a role in increasing the risk of VF. Although these factors were not included in the criteria we described, considering them–when available–may be useful in light of recent studies, particularly if the loss of virological control was recent. 13
In conclusion, we propose a comprehensive and easily applicable risk stratification in order to avoid excessive monitoring during LA treatment. This strategy, based on our experience, albeit limited, has been shown to be safe and effective, with a low rate of VF, comparable with that observed in real-world studies. 6 By ensuring rigorous follow-up for individuals with risk factors for VF and reducing unnecessary evaluations in others, this approach enhances the feasibility and acceptability of long-acting therapy.
Footnotes
Author Disclosure Statement
Outside the submitted work, L.T. attended advisory boards, served as consultant, or received grants for conference participations from Gilead Sciences and ViiV Healthcare. Outside the submitted work, A.D.B. has received funding for scientific advisory boards, travel, and speaker honoraria from ViiV Healthcare and Gilead. Outside the submitted work, M.B. reports research grants and/or personal fees for adviser/consultant and/or speaker/chairman from BioMérieux, Cidara, Gilead, Menarini, MSD, Pfizer, and Shionogi. All other authors: none to declare.
Funding Information
This study was conducted as part of the authors’ routine work.