
Abstract
A diet enriched in lupin kernel flour can lower blood pressure, but mechanisms responsible are unclear. Lupin is a source of polyphenols, protein, and L-arginine, factors that may influence blood pressure via effects on oxidative stress and vascular function. Therefore, we aimed to determine the effects of a lupin-enriched diet on oxidative stress and factors influencing vascular function as potential mechanisms for demonstrated benefits on blood pressure. Overweight men and women (n = 88) were recruited to a 16-week parallel-design study. Participants were randomly assigned to replace 15%–20% of their usual daily energy intake with white bread (control) or lupin kernel flour-enriched bread (lupin). All measurements were taken at baseline and 16 weeks. At baseline, plasma F2-isoprostanes and 20-hydroxyeicosatetraenoic acid (20-HETE) were positively associated with blood pressure, and plasma nitrite was negatively associated with blood pressure (p < 0.05). For lupin relative to control, the estimated differences in plasma F2-isoprostanes (45 pmol/L; 95%CI: − 68, 158), urinary F2-isoprostanes (17 pmol/mmol creatinine; 95%CI: − 43, 76), plasma 20-HETE (75 pmol/L; 95%CI: − 91, 241), and plasma nitrite (-0.3 μmol/L; 95%CI: − 1.1, 0.4) were not significant. Although regular consumption of lupin-enriched bread can lower blood pressure, these results do not support for the hypothesis that this is via effects on oxidative stress or vascular function. Antioxid. Redox Signal. 13, 1517–1524.
Introduction
We have previously shown that regular consumption of lupin-enriched bread when compared to white bread results in lower blood pressure (21). The net effect on systolic blood pressure was 3 mm Hg (21). Pilvi et al. (30) found that lupin protein can attenuate the development of hypertension, and improve nitric oxide (NO)-dependent vasorelaxation in a salt-sensitive rat model of hypertension. The mechanisms are uncertain, but may be linked to components in lupin such as the polyphenols, protein, and/or L-arginine.
Foods and beverages rich in polyphenols have been reported to lower blood pressure (39). Possible mechanisms for this include effects on oxidative stress and NO metabolism. Oxidative stress has been linked to high blood pressure (33, 34); polyphenols are potent antioxidants in vitro (12); and lupin extracts have been shown to have antioxidant activity in vitro (16, 24, 28). Polyphenols have also been linked to inhibition of certain cytochrome P450 enzymes such as 3A4 (29, 32). Furthermore, it is possible that specific polyphenols may inhibit cytochrome P450 enzymes (4A and 4F) responsible for the production of 20-hydroxyeicosatetraenoic acid (20-HETE), a potent vasoconstrictor (18, 25). We have previously shown that urinary 20-HETE is associated with lower NO-dependent vasodilation (41) and higher blood pressure (42). Dietary polyphenols can also acutely increase markers of nitric oxide (NO) status including plasma nitrite and urinary nitrate concentrations (23), and improve endothelial function in humans (13).
Increasing protein at the expense of refined carbohydrate in the diet can lower blood pressure. Lower blood pressure with higher protein intake has been a consistent finding in both population studies (1) and randomized controlled trials (3, 10). This effect may be due to a higher amino acid load resulting in a dose-dependent diuretic effect (4). Alternatively, an increase in intake of the amino acid L-arginine, a precursor for NO synthesis, may be responsible. Lupin protein is rich in L-arginine, containing approximately 10% by weight (6, 19, 30). Increased L-arginine intake can augment NO status and thus contribute to lower blood pressure (35). Thus, lupin protein may benefit blood pressure via effects on NO metabolism.
We have investigated the effect of regular consumption of a lupin-enriched diet on plasma and urinary F2-isoprostanes as reliable markers of in vivo oxidative stress, as well as plasma 20-HETE and plasma nitrite because of their potential influence on vascular function. We have also investigated the cross-sectional associations of these factors at baseline with blood pressure and fasting blood lipids, glucose, and insulin concentrations. The population recruited to this study were overweight and obese men and women. This population are known to have increased risk of hypertension (8) and oxidative stress (17).
Materials and Methods
Participants
Overweight and obese men and women aged between 20 to 70 years with a body mass index between 25 and 35 kg/m2 were recruited from the general population. Exclusion criteria included current and recent smoking, history of cardiovascular or peripheral vascular disease, diabetes, fasting plasma glucose concentrations ≥5.6 mmol/L, history of asthma, renal disease, liver disease or gout, psychiatric illness, history of major gastrointestinal problems, other major illnesses such as cancer, uncontrolled hypertension (systolic blood pressure >150 mmHg or diastolic >95 mmHg), use of >2 antihypertensive agents, a change in antihypertensive, lipid-lowering or other medication within the previous 3 months, women who were pregnant or intended to become pregnant, history of food allergies, current weight loss, and alcohol intake >200 g/week for women and >300 g/week for men. All procedures followed were in accordance with institutional guidelines, and the study was approved by the University of Western Australia Human Ethics Committee. All participants provided written informed consent. This trial was registered at the Australian New Zealand Clinical Trials Registry as ACTRN12606000034538 on January 25th 2006.
Study design
A total of 88 participants were recruited. Participants entered a 16-week randomized, controlled parallel-design trial, where they were randomly assigned to one of two groups: control or lupin. Randomization was performed using computer-generated random numbers concealed in opaque envelopes. Both groups were required to replace approximately 15%–20% of their usual daily energy intake with bread, approximately 4 × 40 g slices of bread per day. Apart from this small shift in dietary intake, participants maintained their usual diet, physical activity, and medication regimen throughout the trial.
The bread formulation has been described in detail previously (22). Briefly, a standard white bread, with small modifications to the recipe, was used as the control. The lupin bread was formulated by substituting 40% of the wheat flour usually present in the white bread with lupin kernel flour. Compared to the control bread, the lupin bread was higher in protein and fiber derived from lupin kernel flour, and lower in wheat-derived carbohydrate. The wheat-derived protein (gluten) content of the two breads was matched. A dietician counselled the participants at baseline on how to incorporate the bread into their usual diet and then every 2 weeks throughout the intervention to ensure achievement of the bread incorporation and maintenance of usual lifestyle. All measurements were performed at baseline and at completion of the 16-week intervention.
Dietary assessment
Dietary intake was assessed using a modified diet history questionnaire (2) at week 0 and at the end of 16 weeks. The data collected from the questionnaire was analysed using FoodWorks Professional 2007 (Xyris, Australia) to determine average daily energy and macronutrient intake. Compliance with the bread intake was assessed using a daily bread intake record where participants recorded the number of slices consumed each day throughout the study.
Blood pressure assessment
Twenty-four hour ambulatory blood pressure was measured at baseline and at the end of 16 weeks. Measurements were performed using Spacelab monitors (Spacelabs 90207, Australia), programmed to take a reading every 20 minutes while the individual was awake and every 30 minutes while they were asleep (21). Mean blood pressure values were calculated for 24 hours, day time (awake) and night time (asleep).
Biochemistry
At baseline and at 16 weeks, blood samples were taken after a 12-h fast from the antecubital fossa vein and a 24-h urine collection was performed. All routine biochemical analyses, including blood lipids and glucose and insulin concentrations, were performed by PathWest at Royal Perth Hospital, Western Australia. Blood samples were centrifuged at 3000 rpm at 4°C for 10 minutes and stored at −80°C until analysis. Aliquots of urine were also stored at −80°C until analysis. All samples were run in a single batch to reduce variability.
Plasma total F2-isoprostanes and urinary free F2-isoprostanes were measured by gas chromatography-mass spectrometry (GCMS) couple to electron capture negative chemical ionization using a modification of our previously reported method (26). Briefly, F2-isoprostanes in plasma (0.25 ml) were hydrolyzed under nitrogen with 1 M KOH in methanol for 40 min at 40°C. The sample was acidified to pH 4.0 before solid-phase chromatography on a prewashed 200-mg Certify II column (Varian, Belmont, Australia). After eluting with methanol/water (v/v, 50/50) and hexane/ethyl acetate (v/v, 75/25) the F2- isoprostanes were eluted with 2 ml of ethyl acetate/methanol 90%/10%, dried, and derivatized. Urinary F2- isoprostanes were measured in the same manner but without base hydrolysis. F2-isoprostanes were detected by selected ion monitoring using m/z 569 and m/z 573 for endogenous and tetra-deuterated internal standard, respectively.
Plasma free 20-HETE was measured by GCMS using electron capture negative chemical ionization using a modification of the method previously described by Tsai et al. (40). Nitrite and nitrate concentrations in plasma and urine were determined using a previously published GCMS method (23). The total polyphenol content of the two breads (control and lupin-enriched) was determined using a modification of the Folin-Ciocalteu assay (38). Extracts were assayed at 750 nm with gallic acid serving as the standard.
Statistical analysis
Statistical analyses were performed using SPSS 15.0 software (SPSS Chicago, IL). For descriptive data, including baseline and 16-week measurements, results are presented as mean ± SD. Based on 40 participants per group, the study was powered at 80% to detect a 25% difference in plasma and urinary F2- isoprostanes and a 40% difference in plasma nitrite concentrations. At baseline, the characteristics of the participants in the two groups were compared with the independent-samples t test and the chi-squared test for categorical variables. Pearson's correlation coefficient (r) was used to determine the degree and directions of association between variables at baseline. The baseline and end of intervention values for biochemical indices of oxidative stress and vascular function are presented as mean ± SEM in Figure 1. The baseline-adjusted end of intervention values and between-group differences are presented as mean (95% CI). p < 0.05 was the level of significance in two-tailed testing. General linear models (analysis of covariance) were used to assess baseline-adjusted end of intervention between-group differences. Between-group differences were also adjusted for potential confounding factors, including age, gender, body mass index, and changes in energy and nutrient intakes.
Results
Baseline characteristics
A total of 88 participants were randomized to the trial. Eight participants withdrew because they were unable to consume the required quantity of bread; 4 withdrew due to an inability to commit to time requirements; 1 withdrew due to moving interstate; and 1 withdrew due to an unrelated medical problem requiring a change in medication. There were no reported adverse effects of eating either the white bread or the lupin bread during the 16-week study. A total of 74 participants completed the trial, 37 in each group. There were no significant differences in characteristics of the participants at baseline (Table 1). The mean (±SD) energy intakes from bread at baseline was 1182 ± 675 kJ/d and 1251 ± 925 kJ, for the control and lupin groups, respectively, which equates to approximately 12% of total energy intake. Thus, the change in diet to incorporate 15%–20% of usual daily energy intake with bread was generally minimal.
p-value for between-group difference analysed using the independent samples t test and the chi-squared test for categorical variables.
Values are presented as mean ± SD.
Geometric mean (95% CI).
Estimated polyphenol, protein and L-arginine intakes
Total polyphenol intakes in the lupin and control groups were estimated from polyphenol measurements performed in the control and lupin-enriched breads. Relative to control, consumption of lupin-enriched bread resulted in a significantly higher total polyphenol intake (173 mg/d; 95% CI: 157, 188).
Total protein intakes were estimated from the diet history questionnaire. Relative to control, consumption of lupin-enriched bread resulted in a significantly higher total protein intake (13.7 g/d; 95%CI: 2.3, 25). Approximately 10% by weight of the lupin protein is L-arginine. Therefore the L-arginine intake was higher in the lupin compared to control by approximately 1.4 g/d.
Cross-sectional associations at baseline
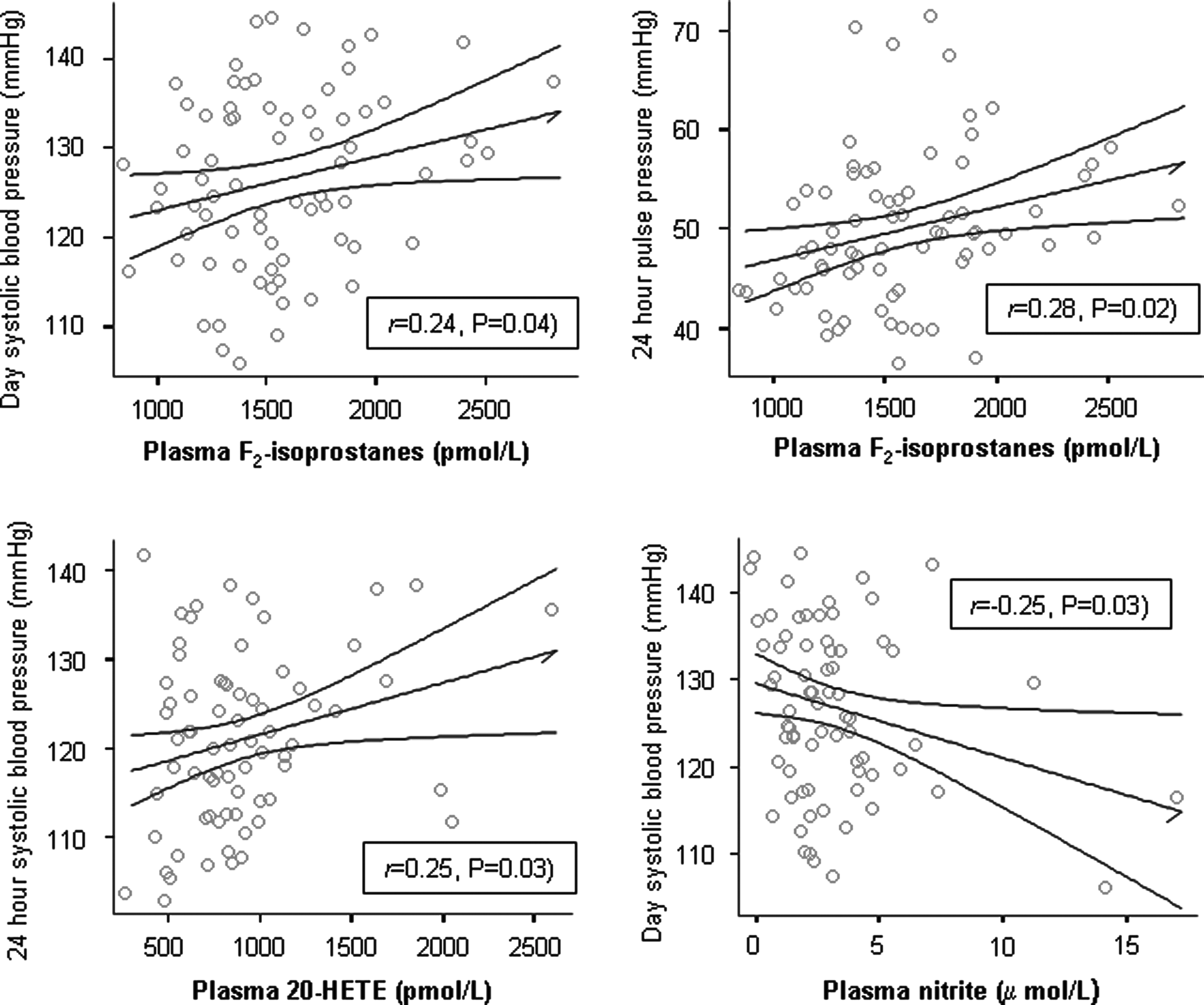
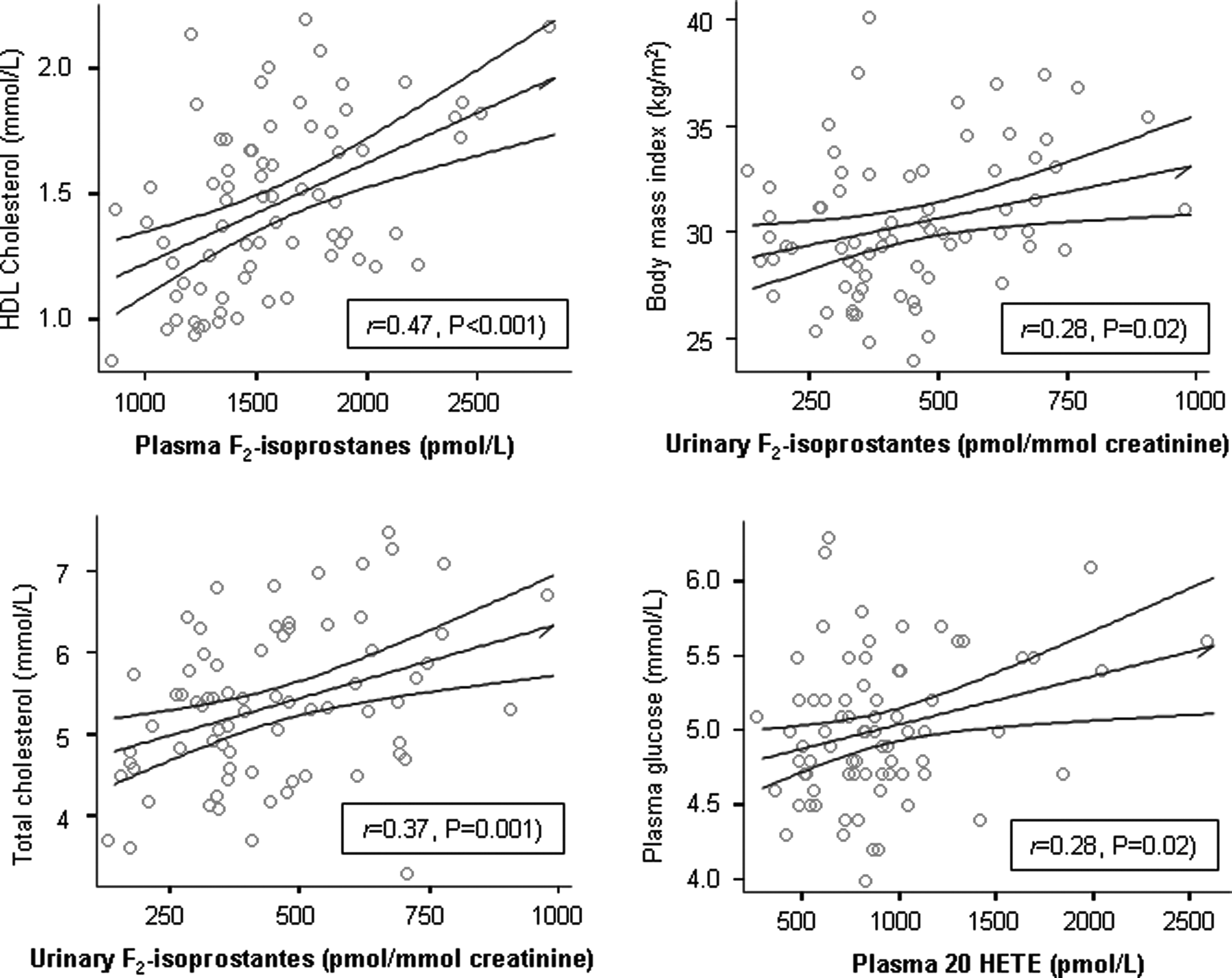
At baseline, a number of significant cross-sectional associations were observed. Plasma F2-isoprostanes were positively associated with 24-h pulse pressure (r = 0.28, p = 0.02), daytime systolic blood pressure (r = 0.24, p = 0.04), and HDL cholesterol (r = 0.47, p < 0.001). Urinary F2-isoprostanes were positively associated with body mass index (r = 0.28, p = 0.02), total cholesterol (r = 0.37, p = 0.001), and LDL cholesterol (r = 0.35, p = 0.003). Plasma 20-HETE was positively associated with 24-h systolic blood pressure (r = 0.25, p = 0.03), night time systolic blood pressure (r = 0.29, p = 0.01), and fasting glucose (r = 0.28, p = 0.02). Plasma nitrite was negatively associated with 24-h systolic blood pressure (r = −0.24, p = 0.04), and daytime systolic blood pressure (r = −0.25, p = 0.03). Urinary nitrate was positively associated with HDL cholesterol (r = 0.26, p = 0.03), and negatively associated with fasting glucose (r = −0.26, p = 0.03). Associations between blood pressure and indices of oxidative stress and vascular function are summarized in Figure 1, and associations between cardiovascular disease risk markers and indices of oxidative stress and vascular function are summarized in Figure 2.
Blood pressure
A detailed analysis of the effects of lupin-enriched bread on blood pressure has been presented previously (21). In summary, the regular consumption of lupin-enriched bread in comparison to control bread resulted in significantly lower 24-h ambulatory systolic blood pressure (-3 mm Hg; 95%CI: − 5.6, − 0.3) and pulse pressure (-3.5 mm Hg; 95%CI: −5.3, −1.8). Similar effects on daytime and night-time systolic and pulse pressures were observed. Diastolic blood pressure was not significantly altered (21). Compared to control, consumption of the lupin-enriched bread did not significantly alter sodium and potassium intake estimated using 24-h urinary sodium and potassium excretion (0.4 mmol/mmol creatinine; 95% CI: −1.6, 2.4, and 0.6 mmol/mmol creatinine; 95% CI: −0.2, 1.4, respectively).
Oxidative stress and biochemical indices of vascular function
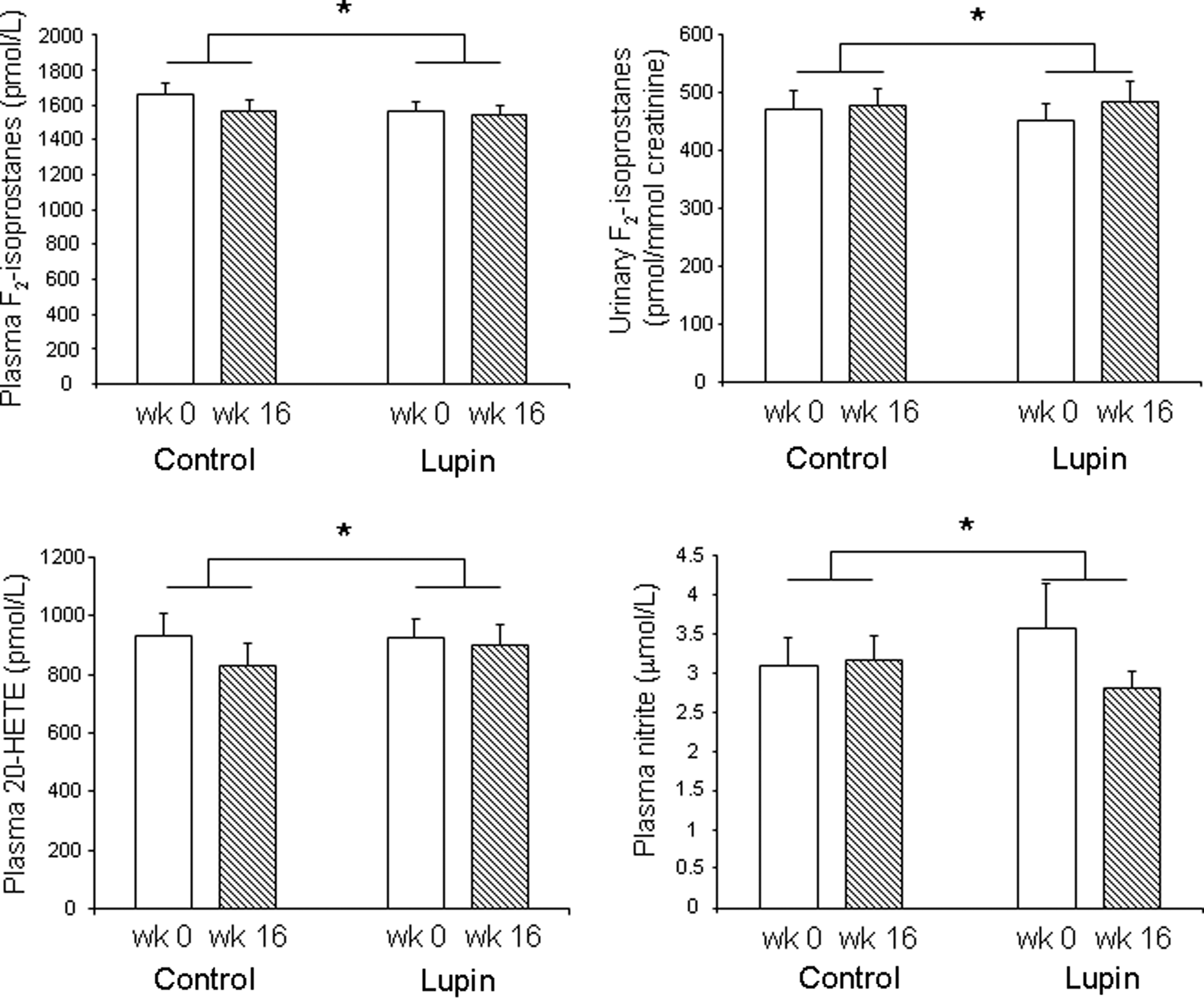
At baseline there was no significant difference between the control and lupin groups in plasma and urinary F2-isoprostanes, plasma 20-HETE, and plasma and urinary nitrite and nitrate concentrations (p > 0.30). The baseline and end intervention values for plasma and urinary F2-isoprostanes, plasma 20-HETE, and plasma nitrite are presented in Figure 3.There were no significant changes from 0 to 16 weeks, and there were no significant between-group differences at 16 weeks in any of the outcome measurements. For lupin relative to control, differences in plasma F2-isoprostanes (45 pmol/L; 95%CI: −68, 158), urinary F2-isoprostanes (17 pmol/mmol creatinine; 95%CI: − 43, 76), plasma 20-HETE (75 pmol/L; 95%CI: −91, 241), plasma nitrite (-0.3 μmol/L; 95%CI:-1.1, 0.4), urinary nitrite (-0.7 μmol/mmol creatinine; 95%CI: −3.0, 1.7), plasma nitrate (-0.6 μmol/L; 95% CI: −9.0, 7.7), and urinary nitrate (8 μmol/mmol creatinine; 95%CI: −24, 40) were not significant. Adjustment for potential confounding factors did not influence interpretation of the findings.
Discussion
Our primary aim was to determine the effects of a lupin-enriched diet on markers of oxidative stress and factors that can influence vascular function. We have previously published data from this study showing that a diet enriched in lupin kernel flour can lower blood pressure (21). Lupin is a source of polyphenols, protein, and L-arginine (7, 28), and there is evidence that these dietary factors could influence blood pressure via effects on oxidative stress and vascular function (12, 16, 24, 30, 35, 39). Therefore, the rationale for the current investigation was to explore potential mechanisms for benefit on blood pressure. We also investigated the associations at baseline of F2-isoprostanes, 20-HETE, and nitrite and nitrate with blood pressure and other risk markers for cardiovascular disease. The observed cross-sectional associations at baseline were generally consistent with previously reported associations. However, the lupin-enriched diet did not significantly alter F2-isoprostanes, 20-HETE, or nitrite and nitrate concentrations.
Significant associations were observed for both indices of oxidative stress and factors influencing vascular function with blood pressure and other cardiovascular disease risk factors. Plasma F2-isoprostanes were positively associated with blood pressure. Studies have linked markers of oxidative stress with higher blood pressure (42). However, studies using more specific markers of oxidative damage in vivo, such as isoprostanes, have produced inconsistent findings (5, 34, 41). The observed positive relationship of 20-HETE with blood pressure is consistent with several studies showing associations between increased urinary 20-HETE excretion and higher blood pressure (41, 42). This is the first report of a positive association between plasma levels of 20-HETE and blood pressure. Recent in vivo studies have reported that plasma nitrite reflects endothelial-dependent NO synthesis in humans (20). The observed relationship of plasma nitrite with blood pressure is consistent with increased NO synthesis being related to lower blood pressure. A similar positive association was found between urinary F2-isoprostanes and body mass index in the Framingham population (17). A strong positive association was found between HDL cholesterol and plasma F2-isoprostanes in the current analysis. This is counterintuitive because HDL cholesterol is associated with reduced risk of cardiovascular disease. However, we have recently demonstrated that HDL is the major lipoprotein carrier of F2-isoprostanes in the circulation (31), suggesting that HDL may be responsible for removal of oxidised species.
Results of several studies show that lupin extracts and lupin products possess antioxidant activity in vitro (16, 24, 28). This is suggested to be due to polyphenols. Although there is evidence that polyphenols may reduce vascular oxidative damage in animal models of atherosclerosis (27, 36), there is limited data demonstrating reduced plasma or urinary F2-isoprostane concentrations with an increase in flavonoid intake (11, 14, 15). More sensitive and specific markers of vascular oxidative damage may be needed to detect effects within the arterial wall.
Effects of the polyphenols present in lupin on NO metabolism and endothelial function is another possible mechanism for benefit of lupin on blood pressure. We observed no significant effect on plasma nitrite and urinary nitrate, or on plasma 20-HETE concentrations. We have previously shown that supplementation in humans with isolated polyphenolic compounds (flavonoids) can augment NO status acutely, including an increase in plasma nitrite and urinary nitrate concentrations (23). The estimated increase in total polyphenol intake in the present study of 173 mg/d is similar to the dose of polyphenols shown to augment NO status (200 mg). However, we have demonstrated that the structure of the polyphenolic compounds is likely to strongly influence bioactivity (23). The structures of the polyphenols present in lupin kernel flour have yet to be fully elucidated. Isolated polyphenols and polyphenol-rich foods and beverages have been shown to improve endothelial function and reduce blood pressure (9, 27). However, these effects are not consistent and may depend on the structure and dose. Thus, the lack of observed effect on plasma nitrite, urinary nitrate and 20-HETE may relate to the structure of the polyphenols as well as to the dose provided.
An increase in protein intake at the expense of carbohydrate is consistently shown to result in lower blood pressure (3, 10). The mechanisms responsible are not clear but may be related to higher total amino acid load (4) and/or an increase in L-arginine, a precursor of NO (35). Supplementation with pure L-arginine—between 3 and 10 g/d—can augment markers of NO status and lower blood pressure (35, 37). The estimated increase in arginine intake with lupin-enriched bread in the present study was 1.4 g/d. This could contribute to effects on blood pressure, but may be insufficient to alter markers of NO status.
We have attempted to establish the effects of a lupin-enriched diet on oxidative stress and factors influencing vascular function as potential mechanisms for demonstrated benefits on blood pressure. The markers of oxidative stress and NO status measured were not significantly altered by a lupin-enriched diet. It is possible that plasma and urinary F2-isoprostanes and plasma nitrite and urinary nitrate may not be sensitive enough to identify small changes in oxidative stress and NO status. Furthermore, ambulatory blood pressure was measured over 24 hours, during which participants were consuming the lupin or control breads. Therefore, acute and short-term effects of a higher L-arginine intake or a higher polyphenol intake could have contributed to the benefits of lupin on blood pressure. Measurements performed in 24-h urine samples may provide an integrated measure, but measurements in fasting plasma samples, such as nitrite and F2-isoprostanes, may fail to identify any acute or short-term effects.
In conclusion, we have shown cross-sectional associations of markers of oxidative stress and factors that can influence vascular function with blood pressure and risk factors for cardiovascular disease. These associations are largely consistent with previously reported relationships. However, a lupin-enriched diet did not significantly alter any of the outcome measures. Therefore, although regular consumption of lupin-enriched bread can lower blood pressure, these results do not provide support for the suggestion that lupin can reduce blood pressure via effects on oxidative stress and vascular function.
Footnotes
Acknowledgments
This study was funded by the Western Australian Government, Department of Industry and Resources, and conducted under the Centre for Food and Genomic Medicine. Xingbin Yang was supported by the State Scholarship Fund (No.2008106628) of the China Scholarship Council, and the Overseas Scholarship Program of Shaanxi Normal University (No.2008861024). We acknowledge Mrs. Noelene Atkins for nursing assistance, Ms. Clare Jurcyzk for dietetic assistance, Mr. John Noonan and Bodhis Bakery for help with development of bread formulations, and Mr. Ken Dods and Mr Liquin Liu for their assistance in measuring the polyphenol content of the bread.
Author Disclosure Statement
No competing financial interests exist.