
Abstract
Pharmaceutical treatment for millions worldwide who have schizophrenia is limited to a handful of antipsychotics. Despite the proven efficacy of these drugs, the overall outcome for schizophrenia remains suboptimal. Thus, alternative treatment options are urgently needed. One possible approach may be antioxidant therapy. The extant evidence for the role of oxidative stress in the pathophysiology of schizophrenia offers a hypothesis-derived therapeutic approach in the form of antioxidants. Vitamins C and E, for example, are suitable for human clinical trials because they are readily available, inexpensive, and relatively safe. Research into the therapeutic use of antioxidants in schizophrenia can be grouped into two main clusters: for psychopathology and for side effects. Of these studies, some have been carefully conducted, but majority are open label. Use of antioxidants for treatment-related side effects has been more extensively investigated. The totality of the evidence to date suggests that specific antioxidants, such as N-acetyl cysteine, may offer tangible benefits for the clinical syndrome of schizophrenia, and vitamin E may offer salutary effects on glycemic effects of antipsychotics. However, a great deal of fundamental clinical research remains to be done before antioxidants can be routinely used therapeutically for schizophrenia and treatment-related complications. Antioxid. Redox Signal. 15, 2047—2055.
Introduction
Treatment of schizophrenia
Antioxidants as a therapeutic strategy
The discovery of impaired antioxidant defense system (AODS), lipid peroxidation, and other indices of oxidative stress in schizophrenia (56) offers an obvious therapeutic approach to countering the potential oxidative damage, and its clinical sequelae, in the form of antioxidants.
An antioxidant is a molecule capable of slowing or preventing the oxidation of other molecules. Oxidation reactions can produce free radicals, which start chain reactions that damage cells. Antioxidants terminate these chain reactions by removing free radical intermediates, and inhibit other oxidation reactions by being oxidized themselves.
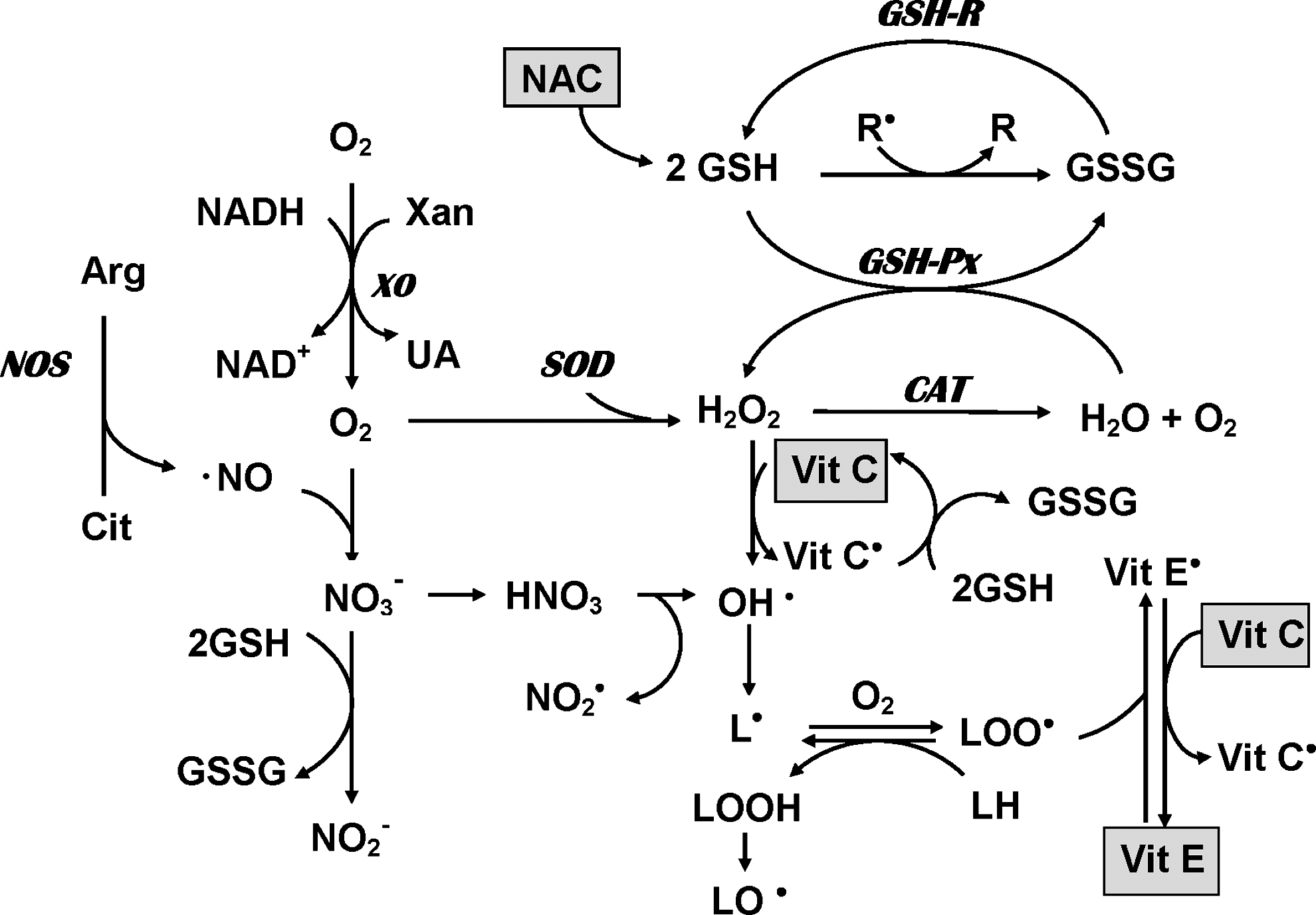
The mammalian antioxidant defense system (AODS) is an elaborate mechanism that comprises a large number of enzymatic and nonenzymatic processes (Fig. 1). The key antioxidant enzymes are superoxide dismutases (SODs), catalase (CAT), and glutathione peroxidase (GSHPOD). To date, no clinically useful means have been found to utilize exogenous antioxidant enzymes. SOD, in the polyethylene glycol–conjugated form (PEG-SOD), has been used in hypoxia–reperfusion models (54). However, exogenous SOD cannot cross the blood–brain barrier, a fact that has limited its utility as a practical free radical scavenger (24).
Nonenzymatic antioxidant mechanisms include scavenging and quenching. Scavenging is the interaction of free radicals with expendable, but replaceable, substrates, such as glutathione, uric acid, and bilirubin. Quenching is the absorption of electrons or energy and is performed very effectively by β-carotenoids and tocopherols.
Antioxidant molecules in the human AODS can broadly be divided into two classes based on solubility: water-soluble (hydrophilic) and fat-soluble (hydrophobic) (Table 1). Hydrophilic antioxidants, such as vitamin C, neutralize free radicals in the cytosol; hydrophobic antioxidants, such as vitamin E, scavenge radicals to protect cell membranes to limit lipid peroxidation. Thus, nonenzymatic antioxidants are highly suitable for human clinical trials also because they are readily available, generally inexpensive, and relatively safe (although exceptions exist).
α-Lipoic acid is both hydrophilic and hydrophobic.
An enormous interest has arisen in the dietary antioxidants since the discovery more than 5 decades ago that antioxidants could extend the life span (25). Today a large number of putative antioxidant molecules, including those derived primarily from plant sources, are widely consumed (phytochemicals, nutraceuticals), although their clinical efficacy remains to be firmly established (12, 28, 36). However, ongoing intense research is occurring into several promising antioxidant molecules (9, 16). One among these is Gingko biloba, which has a long history of use in traditional healing (49).
Antioxidant Use in Schizophrenia
No antioxidant monotherapy treatment trials are in progress for treatment of schizophrenia. Such a trial is unlikely to be conducted in the absence of demonstrable primary antipsychotic activity of an antioxidant molecule. Although some second-generation antipsychotic agents show antioxidant activity (3, 40, 41), it is not known whether these antioxidant effects contribute to the antipsychotic efficacy of these agents. It is possible that the antioxidant actions may be mediating other neuroprotective effects that have implications for treatment outcome (33).
Increasing interest exists in using antioxidants as adjunctives or supplements to the primary (antipsychotic) treatment of schizophrenia because of the premise that oxidative damage is associated with poorer outcome (34, 45) and treatment-emergent adverse effects, such as tardive dyskinesia (11).
Adjunctive use of antioxidants for schizophrenia psychopathology
Ironically, the use of antioxidants for treating the key clinical aspects of schizophrenia (such as positive and negative symptoms and cognitive deficits) has lagged far behind the treatment of adverse effects of conventional treatments of schizophrenia. Although there is a paucity of adequate-sized controlled trials, findings from studies to date (Table 2) offer encouraging preliminary results.
AIMS, Abnormal Involuntary Movements Scale; BAS, Barnes Akathisia Scale; BPRS, Brief Psychiatric Rating Scale; CGI, Clinical Global Impression; GAF, Global Assessment of Functioning; GPx, glutathione peroxidase; MDA, malondialdehyde; PANNS, Positive and Negative Symptoms Scale; RBC, red blood cell; SANS, Scale for Assessment of Negative Symptoms; SAS, Simpson-Angus Scale; SOD, superoxide dismutase; TBARS, thiobarbituric acid reactive substances.
Dakhale and colleagues (15) conducted a controlled trial of vitamin C supplementation in patients with schizophrenia. Forty patients were randomly assigned to either placebo or 500-mg/day vitamin C for 8 weeks. A significant reduction in total score on the Brief Psychiatric Rating Scale (BPRS), the primary outcome measure, was found from baseline (36.7 ± 5.8) to 8 weeks' supplementation (19.3 ± 5.5), relative to the placebo group. Notably, an inverse correlation was detected between plasma ascorbic acid level and BPRS total score, but not between plasma level of malondialdehyde (MDA), an index of lipid peroxidation, and plasma ascorbic acid level.
Berk and colleagues (7) examined the efficacy of N-acetyl cysteine (NAC), precursor of the antioxidant glutathione, in patients with chronic schizophrenia. There is evidence of glutathione deficit in schizophrenia (17, 55), providing a theoretical rationale for the treatment trial. In this study, 69 subjects were randomly assigned to NAC group and 71 subjects to the placebo group. NAC was administered in divided doses totaling 2 g/day for 24 weeks. All subjects were being treated with antipsychotic agents (45% with clozapine). The primary outcome measure was the total score on the Positive and Negative Symptoms Scale (PANSS) and a variety of standard secondary measures, including assessment of motor symptoms. A significant reduction in scores of PANSS total, negative symptoms and general symptoms in the NAC group was found relative to placebo group. Further, a reduction occurred in akathisia severity in the NAC group. No difference was seen between the clozapine and other antipsychotics. Although the study outcome indicates a moderate effect, it is notable that it was observed in a group of patients with an average of 12 years of illness duration, and with almost half the cohort taking clozapine. Berk and colleagues (8) used a qualitative data-analysis method in this trial. They replicated the principal findings from the quantitative study. Additionally, they found that NAC supplementation was associated with improvement in positive and mood symptoms.
In a recent meta-analysis of adjunctive use of Ginkgo biloba extract (EGb) in patients with chronic schizophrenia, a moderate effect size was detected for improvement in total and negative symptoms, as assessed by the Scale for Assessment of Positive Symptoms (SAPS), Scale for Assessment of Negative Symptoms (SANS), and Brief Psychiatric Rating Scale (BPRS) (46). Six studies (three double-blind) were included for pooled analyses. In total, 466 subjects were taking EGb and 362 subjects were taking placebo. EGb dose ranged from 120 mg/day to 360 mg/day, with a minimum treatment duration of 8 weeks. Average duration of illness was 11 years. Ninety percent of the study population was Chinese, and the remainder was Turkish. The results from these studies suggest, as the authors conclude, that larger controlled trials are required to replicate the findings (49).
A small number of open-label studies using combination supplementation (omega-3 fatty acids, vitamins C and E) have been conducted that show that these combinations may offer clinical benefit (5, 50) (Table 2).
Antioxidants for emergent adverse effects in the treatment of schizophrenia (other than TD)
An emerging trend in the use of antioxidants in patients with schizophrenia is either to treat emergent adverse events or to prevent such from occurring (Table 3). Three relevant preliminary investigations are reviewed.
BAS, Barnes Akathisia Scale; BMI, body mass index; BPRS, Brief Psychiatric Rating Scale; CK, creatine kinase; FBG, fasting blood glucose; HOMA-IR, Homeostasis Assessment Model of Insulin Resistance, SGOT, serum glutamate oxaloacetic transaminase; WBC, white blood cell count.
Antipsychotic treatment increases the risk of developing the metabolic syndrome, particularly the second generation (atypical) antipsychotic agents, likely by inducing weight gain (36). The diabetogenic effects of these treatments are a serious limitation in the management of patients with schizophrenia. Kim and colleagues (27) examined the effect of α-lipoic acid (ALA) for treating the metabolic syndrome in patients with schizophrenia who had a weight gain of 10% or more from baseline. ALA has been used in diabetic neuropathy and several neurodegenerative disorders (27). In this open-label study, seven patients (five of whom were taking clozapine) were administered 1,200 mg/day of ALA for 12 weeks. A significant weight loss occurred of more than 3 kg, associated with reports of reduced appetite. A trend was observed toward reduction in fasting blood glucose (FBG), fasting insulin, and insulin-resistance index. Among serum lipid indices, cholesterol levels were reduced significantly. No changes in psychiatric status were seen. Although these findings are intriguing, the open-label design and very small sample size severely limit the interpretation of the findings.
Salmasi and colleagues (47) also examined the effect of an antioxidant on the diabetogenic aspects of olanzapine, a second-generation antipsychotic agent. They examined the effects of vitamin E on a variety of end points associated with diabetes, by using a double-blind placebo-controlled design. Thirty-six patients with schizophrenia were randomized to either 1,200 IU/day vitamin E or placebo. At the end of the 8-week trial, vitamin E treatment was associated with significant reductions in FBG; the placebo group experienced increased FBG. No significant reductions were noted in fasting insulin levels or HbA1c levels in the vitamin E–treatment group. By contrast, fasting insulin levels significantly increased in the placebo group.
Another way of looking at the data is to compare the vitamin E and placebo groups. In this case, FBG, HbA1c, fasting insulin levels, and HOMA-IR index were significantly different between the groups, favoring the vitamin E–treatment group. Although not stated by the authors, the findings suggest that vitamin E may provide an antidiabetogenic effect (47).
Vitamin E has been studied extensively in the treatment of TD (reviewed later). However, no studies have examined the potential role vitamin E in the prevention of acutely emergent extrapyramidal symptoms. Dorfman-Etrog and colleagues (19) prospectively examined whether vitamin E would prevent acute neuroleptic-induced extrapyramidal symptoms in patients being treated for an exacerbation of psychosis with first-generation antipsychotic agents. Thirty-nine patients were randomly assigned to antipsychotic agent only or antipsychotic agent and 600 IU/day vitamin E in this 2-week open-label study. The short duration of the study is commensurate with the greatest likelihood of acute neuroleptic-induced extrapyramidal symptoms during the first few days to weeks of treatment. The vitamin E treatment had no effect on psychiatric status, but showed a trend toward reducing the severity of extrapyramidal symptoms.
The earliest trial of vitamin E in the treatment of TD was more than 2 decades ago (31), and in the subsequent 10 years, numerous trials examined both treatment and prevention of TD (1, 2, 14, 18, 20, 21, 29, 30, 32, 42, 48).
Taken together, the controlled trials do not unequivocally show that vitamin E treatment reduces TD severity, in part because of small sample sizes and relatively short duration of the trials (48), although the largest prospective, randomized, placebo-controlled multisite trial with vitamin E (1,600 IU/day) for up to 2 years of treatment showed no efficacy in reducing TD severity (1). Careful examination of the data suggests that in those studies in which vitamin E was found to be beneficial, a shorter duration of TD was associated with better therapeutic response. Because of a lack of robust efficacy of vitamin E, and decreased concern about emergence of TD with atypical antipsychotics, clinical and research interest in using vitamin E for TD has been waning.
Future Directions
Although the findings reviewed here are intriguing, the multiple antioxidant molecules tested for different aspects of schizophrenia leave a puzzling picture, largely because no replication studies have been performed, with the exception of vitamin E treatment for TD. With the exception of Berk and colleagues (7,8), other controlled trials have had small sample sizes. No dose-finding studies have been conducted. Thus, deriving any general treatment principles is currently not possible. Nonetheless, the available evidence from antioxidant supplementation studies in schizophrenia suggests that this approach is promising; however, a great deal of systematic research is required before antioxidant therapeutics can be incorporated into routine clinical practice. For this to happen in the future, important questions first must be answered.
Which antioxidants should be used?
The AODS is an enormously complex network of antioxidant metabolites and enzymes that work together to prevent oxidative damage. Organ-specific vulnerabilities to oxidative damage exist. For example, the brain is uniquely vulnerable to oxidative stress because of its high metabolic rate and high concentrations of lipids (45). Because the brain is the presumed target in the case of schizophrenia, exogenous antioxidant molecules that are likely to cross the blood–brain barrier should be the focus of future investigation.
What is an effective dose?
Because treatment trials of antioxidants use supraphysiologic doses, effective dosing ranges must be established in conjunction with safety considerations. Previous studies of vitamin E for TD used doses ranging from 800 IU/day to 1,600 IU/day. It has subsequently been discovered that a daily dose of vitamin E greater than 400 IU may increase the risk of all-cause mortality (38). Similarly, the controversy continues with the recent findings that beta carotene, vitamin A, and vitamin E, singly or combined, increased mortality, but not vitamin C and selenium (10). Thus, increasing awareness suggests that antioxidants in supraphysiologic doses are not necessarily benign.
Should supplementation trials be monotherapy or combination antioxidants?
For example, previous TD studies used vitamin E as monotherapy. It is well known that vitamin C is used to regenerate vitamin E from its peroxyl state. In the absence of vitamin C, vitamin E radical can potentially be a prooxidant (see Fig. 1). This figure shows only a small portion of the numerous chemical interactions required for effective antioxidant activity.
What should be the minimal duration of treatment?
For example, Berk and colleagues (7) found that the effect of NAC on negative symptoms was not evident till 8 weeks of treatment and continued to accumulate for 24 weeks, whereas general improvement was noted as early as 2 weeks. Whenever feasible, studies should be conducted with the longest duration reasonably possible to determine the time course of treatment response, and posttreatment follow-up should be included to determine the durability of treatment effects. These data also will be valuable in understanding theoretic underpinnings of antioxidant therapies.
When should treatment be initiated?
Clearly, preventing treatment-emergent adverse effects requires that antioxidant supplementation be started at the onset of treatment of schizophrenia, as was done by Dorfman-Etrog and colleagues (19). It is possible that antioxidant supplementation may be most beneficial as a nonspecific modifier of the clinical course of the illness, in which case, supplementation should also be initiated early in the course of illness.
Should antioxidant treatment be combined with omega-3 fatty acid supplementation?
Burgeoning evidence exists for O3FA deficits in schizophrenia (35, 46), and evidence suggests that O3FA supplementation improves the clinical state in schizophrenia (22, 43). Further, O3FAs appear to have antioxidative properties (52). This has notably been demonstrated by Berger and colleagues (6), who showed that ethyl-eicosapentaenoic acid, an O3FA, administered for 12 weeks to patients at first episode was associated with increased brain glutathione, and the glutathione levels were inversely correlated with negative symptoms. Because oxidative stress leads to membrane O3FA deficits, the “bonus” antioxidant effect of O3FA supplementation suggests that benefit may accrue with combining antioxidants and O3FA supplementation (35). Lending support to this notion are findings of decreased levels of GSH in postmortem prefrontal cortex from patients with schizophrenia (23), an inverse relation between brain GSH levels and negative symptoms in patients with schizophrenia (37), and improvement of mismatch negativity (a measure of auditory sensory processing) with NAC, a GSH precursor (30). Observations from two open-label studies indicate that administering a combination of O3FA with vitamins E and C was tolerated by patients with schizophrenia and that a reduction in general psychopathology occurred (5, 50). Rigorous controlled trials will be required to assess the utility of combination supplementation, a daunting task, given the complexity of the underlying biochemical systems.
In summary, it is apparent that the effort to develop rational and evidence-based antioxidant therapeutics has merit, but it will require systematic investigation and multidisciplinary collaborative effort. The primary objective of this research is to improve the outcome of patients with schizophrenia, and even a modest gain in clinical outcomes is a worthwhile endeavor and a public good.