
Abstract
Exogenous antioxidants may influence endogenous antioxidant enzyme activity. We observed in healthy women (n = 95) that higher plasma α-carotene, β-carotene, β-cryptoxanthin, sum of plasma carotenoids, and fruit and vegetable intake were associated with lower plasma extracellular-superoxide dismutase activity. In women with a history of cardiovascular disease, diabetes, or cancer (n = 62), we observed no associations. Our observation that plasma extracellular-superoxide dismutase activity was inversely associated with plasma carotenoids and fruit and vegetable intake in healthy women, but not in women with a history of cardiovascular disease, diabetes, or cancer, suggests that the associations between exogenous and endogenous antioxidants may differ in health and disease. Antioxid. Redox Signal. 14, 9–14.
Oxidative Stress, Exogenous Antioxidants, and Superoxide Dismutase
Superoxide dismutase (SOD) is an enzymatic endogenous antioxidant that scavenges superoxide radicals (O2 •−) (9). In humans, three types of SOD have been identified: the cytosolic Cu/Zn SOD (SOD1), the mitochondrial Mn-SOD (SOD2), and the extracellular Cu/Zn SOD (SOD3/EC-SOD) (13). EC-SOD is found in extracellular fluids, such as plasma, lymph, and synovial fluid (7). Main functions of plasma EC-SOD are to catalyze dismutation of superoxide radicals and thereby preserve nitric oxide involved in vascular tone regulation (7). EC-SOD gene expression may be regulated by a variety of molecules, such as different cytokines (25). Studies have shown altered EC-SOD activity among people with chronic diseases (11, 16, 18).
Exogenous and endogenous antioxidants may cooperate to exert protective effects against ROS and other reactive molecules (23). Animal and in vitro studies suggest that carotenoids may be involved in different transcription systems and affect expression of other antioxidants (24). However, it is unclear how high dietary antioxidant intake from fruit and vegetables and circulating carotenoids may be associated with endogenous antioxidants, such as EC-SOD, in humans. Since increased oxidative stress has been associated with chronic diseases, antioxidants may be regulated and cooperate differently in healthy individuals compared to individuals with chronic diseases. How associations between high fruit and vegetable intake, plasma carotenoids, and EC-SOD activity may differ in health and disease has not been investigated previously.
Different Associations Between Plasma Carotenoids, Fruit and Vegetable Intake, and EC-SOD Activity in Health and Disease
The aim of this study was to assess the associations between the exogenous antioxidants plasma lycopene, lutein/zeaxanthin, α-carotene, β-carotene, and β-cryptoxanthin concentrations, as well as fruit and vegetable intake and the endogenous antioxidant plasma EC-SOD activity in women with and without a history of CVD, diabetes, or cancer. The women in this study were 55–74 years old and randomly selected from the Swedish Mammography Cohort (SMC) (Note 1). Healthy women (n = 95) were defined as women without a history of CVD, diabetes, or cancer and nonhealthy women (n = 62) were defined as those with a history of CVD, diabetes, or cancer. Fruit and vegetable intake was assessed by food frequency questionnaire, and plasma EC-SOD activity and carotenoid concentrations were measured (Notes 2 –5). Among nonhealthy women, 44 women (71.0%) had a history of CVD, 1 woman (1.6%) had a history of diabetes, and 2 women (3.2%) had a history of cancer. There were 15 women (24.2%) who had two or more of the diseases. The mean (±standard deviation [SD]) age of the 95 healthy women was 63.5 ± 5.2 years, and that of the 62 nonhealthy women was 67.4 ± 4.7 years (p < 0.0001). Mean (±SD) body mass index (BMI) in healthy women was 26.0 ± 3.7 kg/m2 and in nonhealthy women 26.7 ± 4.5 kg/m2 (p = 0.26). Mean (±SD) plasma EC-SOD activity was 6.3 ± 1.5 U/ml in healthy women and 6.7 ± 1.6 U/ml in nonhealthy women (p = 0.15). We observed no difference in plasma EC-SOD activity among users of dietary supplements compared to nonusers neither in healthy nor in nonhealthy women.
Characteristics of the women in the highest and lowest quartiles of the sum of plasma carotenoids are presented in Table 1. Healthy women in the highest quartile of the sum of plasma carotenoids were statistically significantly younger and had higher education, higher use of dietary supplements, and higher fruit and vegetable intake than women in the lowest quartile. Nonhealthy women in the highest quartile of the sum of plasma carotenoids were younger and had lower BMI, higher education, higher serum total cholesterol concentration, and higher fruit and vegetable intake than the lowest quartile. In healthy women, plasma EC-SOD activity was statistically significantly lower in the highest quartile of the sum of carotenoids compared to the lowest quartile (−1 U/ml, p = 0.02). In nonhealthy women there was no difference in plasma EC-SOD activity comparing the highest quartile to the lowest.
Women without a history of cardiovascular disease, diabetes, or cancer.
Women with a history of cardiovascular disease, diabetes, or cancer.
Mean ± standard deviation (all such values).
Significantly different from quartile 1, p < 0.05 (analysis of variance).
Sum of plasma lycopene, lutein/zeaxanthin, α-carotene, β-carotene, and β-cryptoxanthin concentrations.
EC-SOD, extracellular superoxide dismutase.
Pearson correlation coefficients between plasma EC-SOD activity and plasma carotenoids, as well as fruit and vegetable intake in healthy and nonhealthy women, are shown in Table 2. In healthy women, plasma EC-SOD activity was statistically significantly inversely correlated with plasma α-carotene, β-carotene, β-cryptoxanthin, sum of carotenoids, and fruit and vegetable intake. Pearson partial correlation coefficients ranged from −0.22 to −0.38. Plasma lycopene (r = −0.20) and lutein/zeaxanthin (r = −0.18) were inversely, nonsignificantly correlated with plasma EC-SOD activity. In nonhealthy women, no statistically significant Pearson correlation coefficients were observed.
Women without a history of cardiovascular disease, diabetes, or cancer.
Women with a history of cardiovascular disease, diabetes, or cancer.
Adjusted for age (years, continuous), body mass index (kg/m2, continuous), smoking (never or ever), education (≤12 or >12 years), supplement use (no or yes), and serum total cholesterol concentrations (mM, continuous).
Sum of plasma lycopene, lutein/zeaxanthin, α-carotene, β-carotene, and β-cryptoxanthin concentrations.
On the basis of a multivariable regression model (Note 6), we plotted adjusted mean plasma EC-SOD activity across quartiles of sum of plasma carotenoids to examine the associations in healthy and nonhealthy women separately (Fig. 1). Healthy women in the highest quartile of the sum of plasma carotenoids had 1.2 U/ml lower mean plasma EC-SOD activity compared to women in the lowest quartile (p = 0.01). Among nonhealthy women, there were no significant differences of EC-SOD activity across quartiles of the sum of plasma carotenoids. We further examined the association between multivariable-adjusted mean plasma EC-SOD activity across quartiles of fruit and vegetable intake (Fig. 2). Healthy women in the highest quartile of fruit and vegetable intake had 1.8 U/ml lower mean plasma EC-SOD activity than those in the lowest quartile (p < 0.0001). Among nonhealthy women, we observed no significant differences in EC-SOD activity across the quartiles of fruit and vegetable intake.
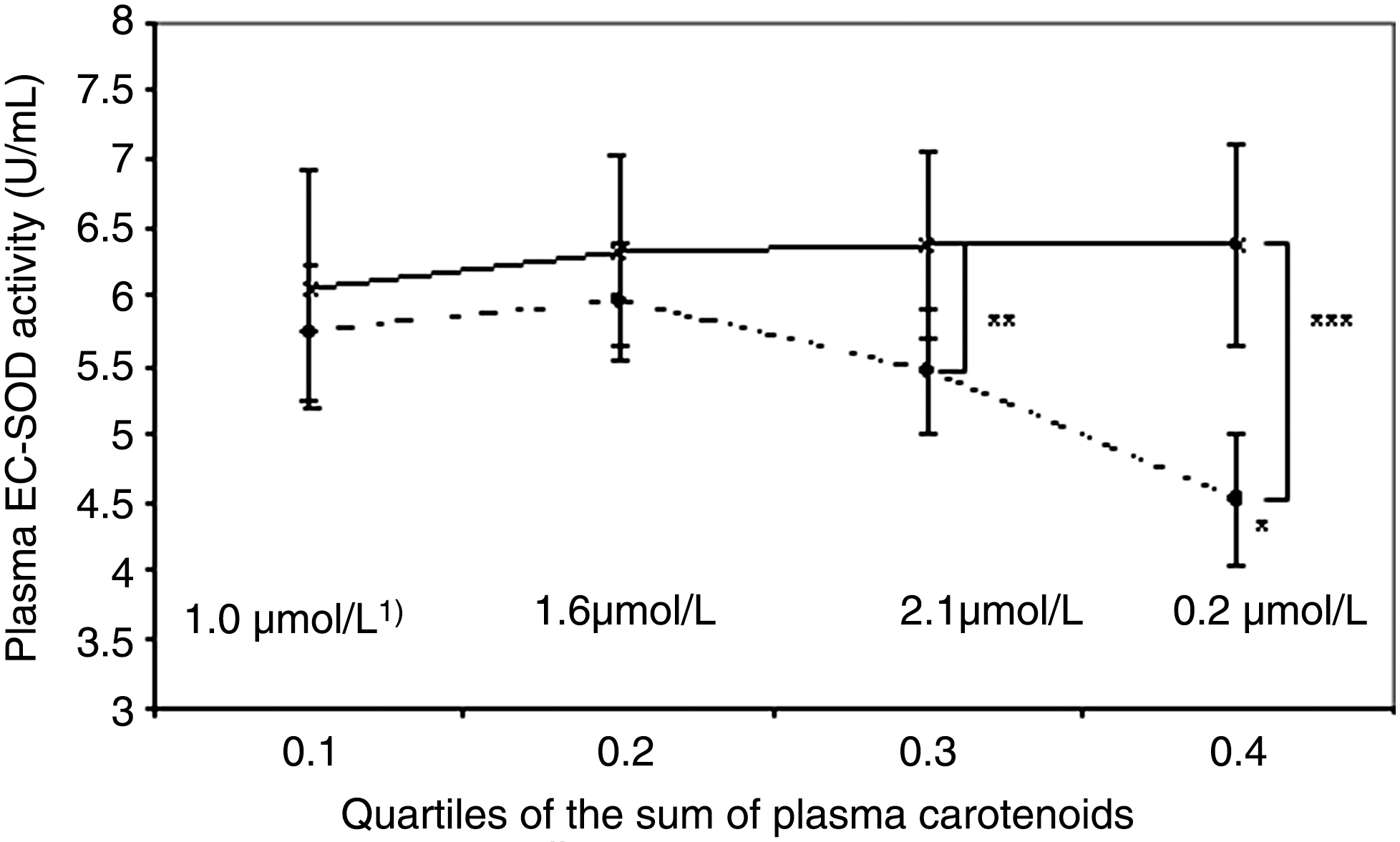

Further, in healthy women, multivariable-adjusted mean plasma EC-SOD activities were 0.9 U/ml (p < 0.05) and 1.9 U/ml (p < 0.001) lower, respectively, compared to nonhealthy women in the two highest quartiles of the sum of plasma carotenoids (Fig. 1). Similar result was observed for healthy women in the highest quartile of fruit and vegetable intake; they had 2.0 U/ml (p < 0.001) lower multivariable-adjusted mean EC-SOD activity than nonhealthy women in the highest quartile (Fig. 2).
Our study is the first to investigate the associations between exogenous dietary antioxidants represented by plasma carotenoids and by fruit and vegetable intake and endogenous antioxidant enzyme EC-SOD activity separately in women with and without a history of CVD, diabetes or cancer. Two previous studies have examined the associations between blood carotenoids and EC-SOD activity in healthy populations only. One study observed no statistically significant inverse associations between plasma EC-SOD activity and serum concentrations of lycopene and β-carotene (17). Another study found a weak positive correlation (r = 0.12, p = 0.02) between the sum of serum lutein/zeaxanthin, α-carotene, β-carotene, and β-cryptoxanthin at baseline and EC-SOD activity measured 15 years after baseline (12). To our knowledge, no previous studies have examined the associations between fruit and vegetable intake, the major source of dietary antioxidants, and plasma EC-SOD activity.
The biological mechanism behind the inverse association observed between plasma carotenoids, fruit and vegetable intake, and plasma EC-SOD activity in healthy women is unknown. We can only speculate that this inverse association may be explained by a compensatory downregulation of EC-SOD activity by exogenous antioxidants. High serum lycopene and β-carotene concentrations have been inversely related to oxidative damage, measured by the lipid peroxidation product malondialdehyde (17). In addition, animal and in vitro studies have shown that plasma carotenoids may be involved in different transcription systems, such as the retinoid receptors, peroxisome proliferator receptors, and the antioxidant response element (3, 24). However, mechanisms of how plasma carotenoids may potentially influence EC-SOD activity and whether the findings from animal studies can be directly related to humans need further investigation.
We did not observe an inverse association between plasma carotenoids or fruit and vegetable intake and plasma EC-SOD activity in nonhealthy women, suggesting that plasma EC-SOD activity may not be downregulated with increasing plasma carotenoids or fruit and vegetable intake in the presence of disease, potentially due to higher oxidative stress and inflammatory burden. Moreover, we observed that mean plasma EC-SOD activity in the highest quartiles of sum of plasma carotenoids and fruit and vegetable intake was statistically significantly higher in nonhealthy women than in healthy women. This suggests a potential upregulation of the enzyme in nonhealthy women (10). We have recently observed similar differences in results between women with and without a history of CVD, where multivitamin use was inversely associated with myocardial infarction among women with no history of CVD, but no association was observed in women with a history of CVD at baseline (21). Previous animal studies have shown the importance of EC-SOD in protection against vascular function and blood pressure (6, 14, 26). In vasculature regions of disturbed blood flow, EC-SOD expression has been shown to be upregulated (20). Transgenic mice with EC-SOD overexpression in the heart showed significantly improved myocardial function after ischemia and reperfusion injury (4). Upregulation of EC-SOD activity in angiotensin II-induced hypertensive rats has also been reported (8). Studies of EC-SOD activity in association with CVD in humans have been inconsistent. Upregulation of vascular EC-SOD expression was observed in patients with acute myocardial infarction, suggesting an upregulation of the enzyme as a compensatory mechanism to protect against oxidative stress (11). Other studies, however, have reported no difference in EC-SOD concentrations (1) and activity (18) in patients with coronary artery disease (CAD) compared to controls, but a slight increase in EC-SOD activity in association with the number of arteries involved (18). In another study, decreased EC-SOD activity has been reported in patients with CAD (16). In patients with type 2 diabetes mellitus, significantly higher serum EC-SOD concentrations have been observed compared to healthy controls (1, 2, 15).
Our observations that high plasma carotenoid concentrations and fruit and vegetable intake downregulated EC-SOD activity in healthy women, but not in nonhealthy women, probably due to higher oxidative stress and inflammation levels, suggest that the associations between exogenous and endogenous antioxidants may differ in health and disease. Therefore, we believe that it is important in future studies to examine the associations between antioxidants separately in healthy and nonhealthy participants to better understand their interplay. Since many randomized controlled trials are conducted among participants with already existing diseases and observational studies are mainly based on healthy participants, this may also provide a possible explanation of the contradictory results between randomized controlled trials and prospective cohort studies regarding the beneficial (or lack of/detrimental) effects of antioxidants (5).
Conclusion
In the present study, higher plasma α-carotene, β-carotene, β-cryptoxanthin, sum of plasma carotenoids, and high fruit and vegetable intake were associated with lower plasma EC-SOD activity in middle-aged and elderly women without a history of CVD, diabetes, and cancer. This inverse association was, however, not observed in women with a history of CVD, diabetes, or cancer. Further elucidation of the associations between exogenous and endogenous antioxidants, separately in healthy and nonhealthy individuals, is needed.
Notes
1. Study population
The SMC was established in 1987–1990. All women born between 1914 and 1948, residing in Uppsala and Västmanland Counties, received a mailed questionnaire regarding diet and lifestyle factors, including questions on age, smoking status, education, and use of dietary supplements; 74% responded. In 1997, a second follow-up questionnaire was sent to the women who were alive and still living in the study area; 70% returned the second questionnaire. In 2003–2005, a subcohort of 5022 women from the SMC living in Uppsala County donated blood and completed a third questionnaire about diet and other lifestyle factors. Among them, 157 women aged 55–74 years were randomly selected and included in the present study. Healthy women (n = 95) were defined as individuals without a history of CVD, diabetes, or cancer before or up to 1 year after blood collection. Nonhealthy women (n = 62) were defined as those with a history of CVD, diabetes, or cancer before or up to 1 year after blood collection. History of CVD and diabetes was determined through linkage to the Swedish Inpatient Register; history of cancer was determined from national and regional Swedish Cancer Registers. BMI was calculated based on measured values of weight and height, as weight (kg) divided by height2 (m2). All women have given written informed consent, and the Regional Ethics Board at Karolinska Institutet (Stockholm, Sweden) and Uppsala University Hospital (Uppsala, Sweden) have approved the investigation.
2. Dietary exposure
Fruit and vegetable intake was estimated from a 96-item food frequency questionnaire completed by the women in 1997. Questions on how often, on average, during the past year the women had consumed different food items were provided, and there were eight different consumption frequency categories to choose from, ranging from never to three times or more daily. The frequency responses were then converted into average consumption (g/day) of each food item. In the present study, total fruit intake included the sum of the fruit items asked in the food frequency questionnaire: oranges/citrus fruits, orange/grapefruit juice, apples/pears, bananas, berries, fruit soups, and other fruits. Total vegetable intake included the sum of the vegetable items asked in the food frequency questionnaire: carrots, beetroots, lettuce/iceberg lettuce, cabbage, Brussels sprouts, cauliflower, broccoli, tomatoes/tomato juice, pepper, spinach, green peas, onions, garlic, mixed vegetables, beans/lentils, and soya products. In a validation study of the food frequency questionnaire, Spearman correlation coefficients between the average of four 1-week diet records and the food frequency questionnaire ranged from 0.5 to 0.7 for fruit items and from 0.4 to 0.6 for vegetable items.
3. Blood samples
Blood samples were collected at a fasting state in evacuated tubes containing ethylenediaminetetraacetic acid. The samples were immediately centrifuged at 2500 g for 10 min, at 4°C in a dark room. Plasma and serum were separated from the blood samples and stored at −80°C until analysis.
4. Analysis of blood carotenoid and cholesterol concentrations
For protein precipitation, 500 μl ethanol containing 0.1% butylhydroxytoluene was added to 500 μl sample, mixed for 15 s, and then standing for 15 min. Carotenoids were extracted by adding 1000 μl hexane containing 0.02% butylhydroxytoluene. Plasma concentrations of lycopene, lutein/zeaxanthin, α-carotene, β-carotene, and β-cryptoxanthin were determined by HPLC, using an apparatus with a UV-VIS detector (Gilson Company, Middleton, WI), chromatographic column C18 RP (4.6 × 250 mm; 5 μm), and guard (Vydac Company, Hesperia, CA). Plasma carotenoids were determined spectrophotometrically at 470 nm with the use of the mixture acetrontrile:hexane:dichloromethane:methanol (ratio 50:20:20:10 and flow rate of 1.0 ml/min). Results obtained were compared with standard curves from standards of lycopene, lutein/zeaxanthin, α-carotene, and β-carotene purchased from Sigma (St. Louis, MO) and β-cryptoxanthin standard from ChromaDex (Santa Ana, CA).
Serum total cholesterol concentrations were measured with Konelab 20 analyzer (Thermo Electron Oy, Vantaa, Finland). Cholesterol reagent was purchased from Thermo Electron Corporation (ref. no 981813, Vantaa, Finland). Analysis of serum cholesterol was performed in a hospital laboratory at Uppsala University Hospital.
5. Plasma EC-SOD activity assay
Plasma EC-SOD activity was measured with a commercial kit (Cayman Chemical Company, Ann Arbor, MI) based on the xanthine oxidase system. Superoxide was generated by adding diluted xanthine oxidase. A tetrazolium salt was used for detection of superoxide, which was measured spectrophotometrically at 450 nm. EC-SOD activity, defined as units (U), was calculated from an equation based on the linear regression from the standard curve. One unit was defined as the amount of enzyme needed to exhibit 50% dismutation of the superoxide radical. Standards and plasma samples were analyzed in duplicates. Inter- and intra-assay coefficients of variations were 8.6% and 7.1%, respectively.
6. Statistical analysis
Statistical analyses were performed with SAS program (Version 9.2; SAS Institute, Cary, NC). Characteristics data were presented as mean ± SD and as percentages for education, smoking status, and supplement use. Characteristic differences were analyzed with analysis of variance. We used residual and goodness-of-fit analyses to test the distribution of plasma carotenoids, fruit and vegetable intake, and EC-SOD activity; no evidence of departure from normality was shown from these analyses; therefore, we used untransformed variables in the analysis. Two women with fruit and vegetable intake outside the range of 133–1572 g/day (±2.5 SD on a log scale) were excluded. The sum of carotenoids was created as the sum of plasma lycopene, lutein/zeaxanthin, α-carotene, β-carotene, and β-cryptoxanthin concentrations. Fruit and vegetable intake was created as the sum of total fruit intake and total vegetable intake. Pearson correlation coefficients were calculated to determine how plasma carotenoids and fruit and vegetable intake were associated with plasma EC-SOD activity. Partial Pearson correlation coefficients were calculated to take into account potential effects of age (years, continuous), BMI (kg/m2, continuous), smoking (never or ever), education (≤12 or >12 years), supplement use (no or yes), and serum total cholesterol concentrations (mM, continuous) on the observed associations. The sum of carotenoids and fruit and vegetable intake were categorized into quartiles, and mean plasma EC-SOD activity for each quartile in healthy and nonhealthy women was determined using a multivariable regression model adjusting for age (years, continuous), BMI (kg/m2, continuous), smoking (never or ever), education (≤12 or >12 years), and supplement use (no or yes). Adjustment for serum total cholesterol concentrations was included in the model for plasma carotenoids and EC-SOD activity analyses. We used Student's t-test to assess differences of mean EC-SOD activity in association with quartiles of sum of carotenoids and fruit and vegetable intake between healthy and nonhealthy women. We considered p < 0.05 as statistically significant.
Footnotes
Acknowledgments
This work was supported by research grants from the Swedish Research Council for Infrastructure and Karolinska Institutet Research Fund.