
Abstract
Dr. Wulf Dröge is recognized here as a redox pioneer because he has published as first author an article on antioxidant/redox biology that has been cited more than 2000 times and over 10 articles that have been cited more than 100 times. One of the key discoveries (1987) was the stimulatory effect of superoxide radicals and hydrogen peroxide on lymphocyte functions, which triggered a series of studies on the role of reactive oxygen species, glutathione, and its precursor cysteine in physiological and pathological processes. He discovered abnormally low cysteine and glutathione levels in human immunodeficiency virus-infected patients and the age-related decline in the postabsorptive plasma cysteine concentration, which is believed to cause age-related oxidative stress. He developed a theoretical concept of the mechanism of aging and death, which is outlined in his books Avoiding the First Cause of Death and Challenging the Limits of the Human Lifespan. Antioxid. Redox Signal. 14, 2319–2323.
Educational and Professional Training
Summary of Dr. Dröge's Top Contributions
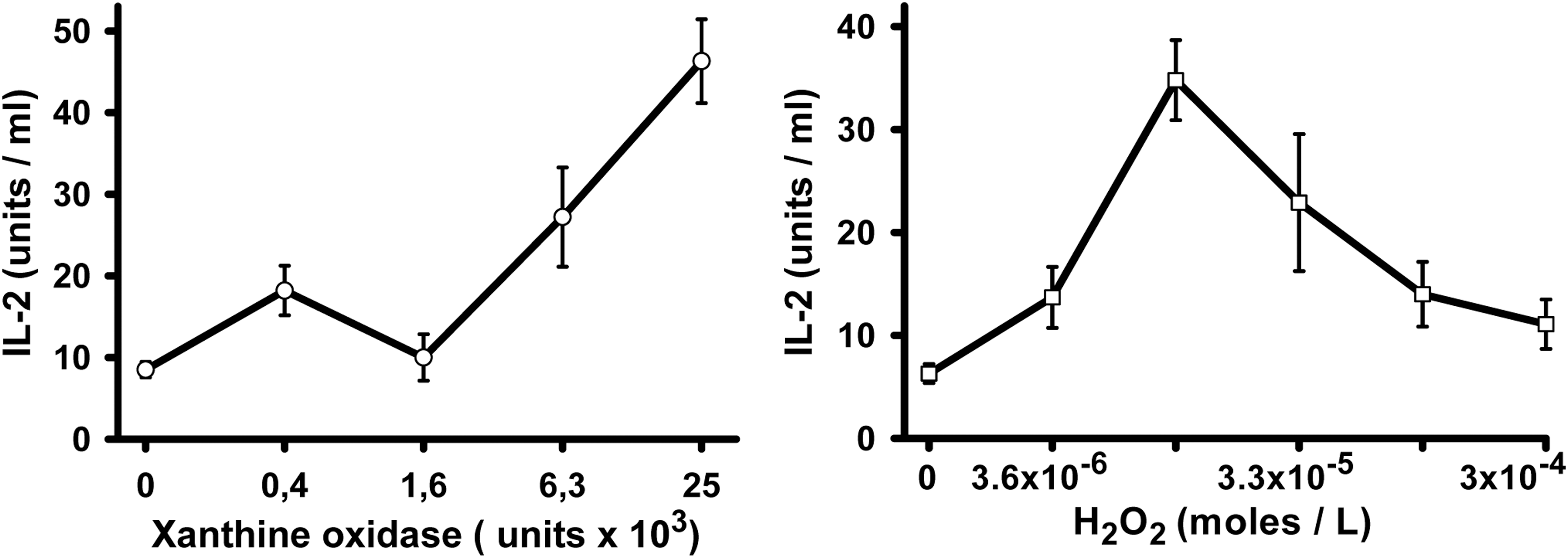
For decades, superoxide radicals and radical-derived reactive oxygen species (ROS) were mainly considered as undesirable byproducts of metabolic processes. Their concentrations in cells and tissues are mainly balanced by the cysteine-containing tripeptide glutathione. In 1987, Dr. Dröge surprisingly found that, in activated T-lymphocytes, superoxide radicals or low micromolar concentrations of hydrogen peroxide increased the production of the T-cell growth factor interleukin-2 (IL-2), an important T-cell protein (27). Superoxide radicals and hydrogen peroxide were subsequently found to stimulate a variety of different cellular signaling pathways. Cysteine and glutathione were shown to inhibit the activation of the transcription factor nuclear factor kappa B (NF-κB), which is critically involved in IL-2 production and in the replication of human immunodeficiency virus (HIV)-1 (24). In 1987/1988, Dr. Dröge and his colleagues discovered that HIV-infected patients and simian immunodeficiency virus (SIV)-infected rhesus monkeys show, on the average, abnormally low plasma cysteine and intracellular glutathione levels (6, 10, 11) and evidence for an excessive conversion of cysteine into sulfate (1). Partial cysteine depletion is possibly one of the strategies that are more widely used by viruses to escape the immune system. A decreasing availability of cysteine was also found to be involved in the process of aging, but this appears to result from a general change in amino acid homeostasis. Based on numerous laboratory studies on redox-regulated signaling processes and complementary clinical investigations, Dr. Dröge eventually developed a new concept of the aging-related oxidative stress as a major cause of death (3, 7).
Description of Key Finding 1
Effect of superoxide radicals and hydrogen peroxide on the expression of the T-cell growth factor IL-2 in T-lymphocytes
The production of superoxide radicals and hydrogen peroxide by activated macrophages and granulocytes in the inflammatory environment was originally thought to serve as a first line of defense against environmental pathogens. From the immunological point of view, it was of interest to see whether these hazardous ROS may compromise the immunological responses of the lymphocytes in this hostile environment (4). Much to their surprise, Dr. Dröge and his Ph.D. student Steffen Roth found that, in activated T-cells, superoxide radicals or low micromolar concentrations of hydrogen peroxide increased the production of the T-cell growth factor IL-2 (27) (Fig. 1). Subsequent studies revealed that the activation of NF-κB, one of the transcription factors involved in the regulation of IL-2 gene expression, is enhanced by ROS and inhibited by thiol antioxidants such as glutathione and thioredoxin (12, 14, 19, 22, 23, 26, 28, 30, 33). As HIV proviral DNA contains two binding sites for the transcription factor NF-κB, it was not unexpected to see that cysteine or N-acetylcysteine (NAC) inhibited HIV replication in infected lymphocyte and macrophage cell lines, suggesting that the cysteine deficiency in HIV-infected individuals may contribute to viral replication in these patients (24). In addition, it was shown that the HIV-1 Tat protein potentiates TNF-induced NF-κB activation and cytotoxicity by altering the cellular redox status (33).
Description of Key Finding 2
Role of glutathione and cysteine in the cellular crosstalk
The lymphocyte receptor signaling pathway is enhanced by oxidative conditions (19, 22, 27) and accordingly inhibited by high concentrations of thiol antioxidants, whereas lymphocyte proliferation is generally inhibited even by a moderate decrease in intracellular glutathione concentrations. Many studies of immunological reactions in cell cultures have been greatly facilitated by the empirical finding that proliferative responses and certain other functions of lymphocytes are strongly enhanced by thiol compounds. In 1986, Dr. Dröge showed that, even in the intact organism (mouse), immune responses against strong antigenic stimuli can be enhanced by injection of glutathione (8, 25). The detailed analysis showed that proliferative responses of lymphocytes and the development of large CD8+ T-cell blasts, cytotoxic T-cell activity, and lymphokine-activated killer cells are exquisitely sensitive against a moderate depletion of intracellular glutathione, whereas IL-2 production and IL-2 messenger RNA expression were favored by glutathione depletion and inhibited by increasing glutathione concentrations (14, 26). The complex immunological response, therefore, requires delicately balanced intermediate levels of glutathione.
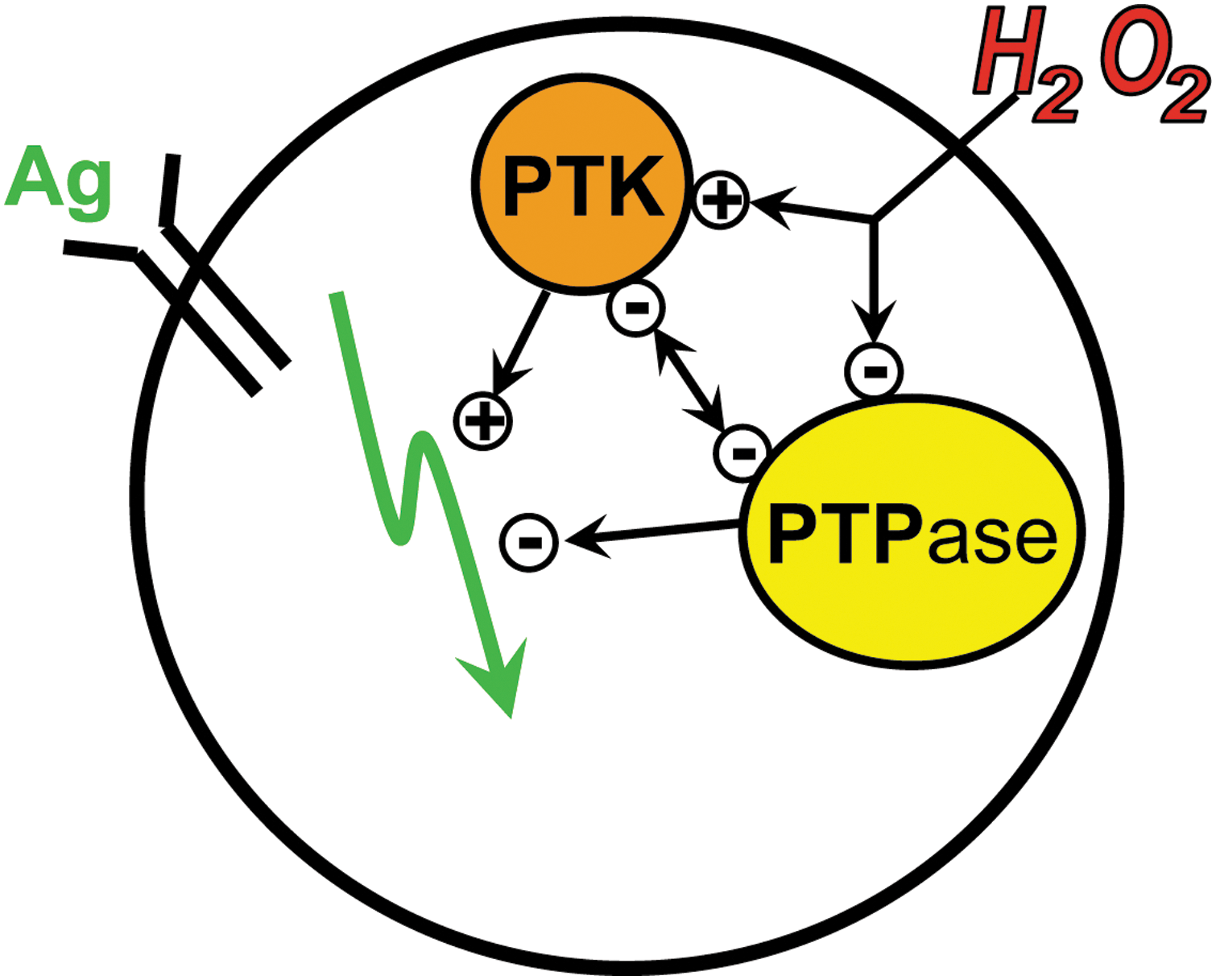
Interactions between different specialized cell types in the immune system have been one of the most important topics in immunology. In this context, Dr. Dröge found that macrophages release cysteine and thereby increase the intracellular glutathione level of lymphocytes and support their proliferative responses (13). Oxygen radicals, hydrogen peroxide, and lactate, in contrast, are examples of small-molecular-weight products from activated macrophages, which facilitate the stimulation of lymphocytes (26, 27). ROS act primarily on protein tyrosine kinases and protein tyrosine phosphatases in the signaling cascade of the lymphocyte receptor for antigens, as schematically illustrated in Figure 2. A metabolic microenvironment with high lactate concentrations (i.e., cells and tissues with high glycolytic activity) causes a decrease in intracellular glutathione levels of lymphocytes and thereby favors the stimulation and production of IL-2 (26). Circulating lymphocytes therefore benefit from the sequential exposure to changing microenvironments.
Description of Key Finding 3
Glutathione deficiencies and cysteine supplementation in clinical conditions and aging
To demonstrate the “in vivo” relevance and clinical implications of redox regulation, Dr. Dröge investigated in various clinical conditions the cysteine and glutathione concentrations and the effect of cysteine supplementation (4).
In view of their immunodeficiency, HIV-infected patients were the first to be studied and shown to have abnormally low mean plasma cysteine and intracellular glutathione levels (6, 10). The net loss of sulfur amino acids in HIV infection was determined by the sulfur content of the urine and by the release of sulfate from the skeletal muscle tissue of the lower extremities into the blood. These studies indicated that the muscle of HIV patients is the major site of elevated cysteine catabolism (1). It has been estimated that the muscle tissue of an HIV-infected patient with a body weight of ∼70 kg produces, on the average, an excessive amount of sulfate equivalent to a daily catabolism of >5 g cysteine per day (1). SIV-infected rhesus monkeys were also found to have abnormally low cysteine and glutathione levels (11) and increased muscular sulfate levels (15). The abnormally low cysteine and glutathione levels were subsequently confirmed by Len and Lee Herzenberg at Stanford University and several other laboratories. In view of these findings, Dr. Dröge proposed to treat HIV-infected patients with a cysteine derivative such as NAC (5, 24). In cooperation with various clinical partners, Dr. Dröge performed two randomized, placebo-controlled clinical studies on the effects of NAC in asymptomatic HIV-infected patients with and without antiretroviral therapy, respectively (2). Both studies showed that NAC treatment enhanced several immunological functions and restored the natural killer cell activity to almost normal levels (2). Preliminary evidence suggests that partial cysteine depletion may also occur in other viral infections and may possibly be one of the strategies that viruses are using to escape the immune system.
Oxidative stress is also involved in inflammatory bowel disease as indicated by the abnormally low level of intestinal glutathione biosynthesis in patients with morbus Crohn and ulcerative colitis (31).
In cancer patients, oxidative stress can be both a curse and a blessing. Oxidative stress plays a major role in the tumor toxic effects of chemotherapy and radiotherapy but, incidentally, has a substantial adverse effect on the host tissue of the patient. In cooperation with several clinical partners, Dr. Dröge has shown that the loss of body cell mass (cancer cachexia) is correlated with an oxidative shift in plasma redox status and reversed by treatment with the glutathione precursor NAC (16) or a cysteine-rich protein (32). Incidentally, treatment with a cysteine-rich protein increased survival, handgrip force, and quality of life parameters when compared with casein, a widely used protein supplement low in cysteine (32).
Conspicuous changes in the hepatic glutathione and sulfate concentrations were found in tumor-bearing cachectic mice (17). Similar changes were induced in mice by injection of IL-6.
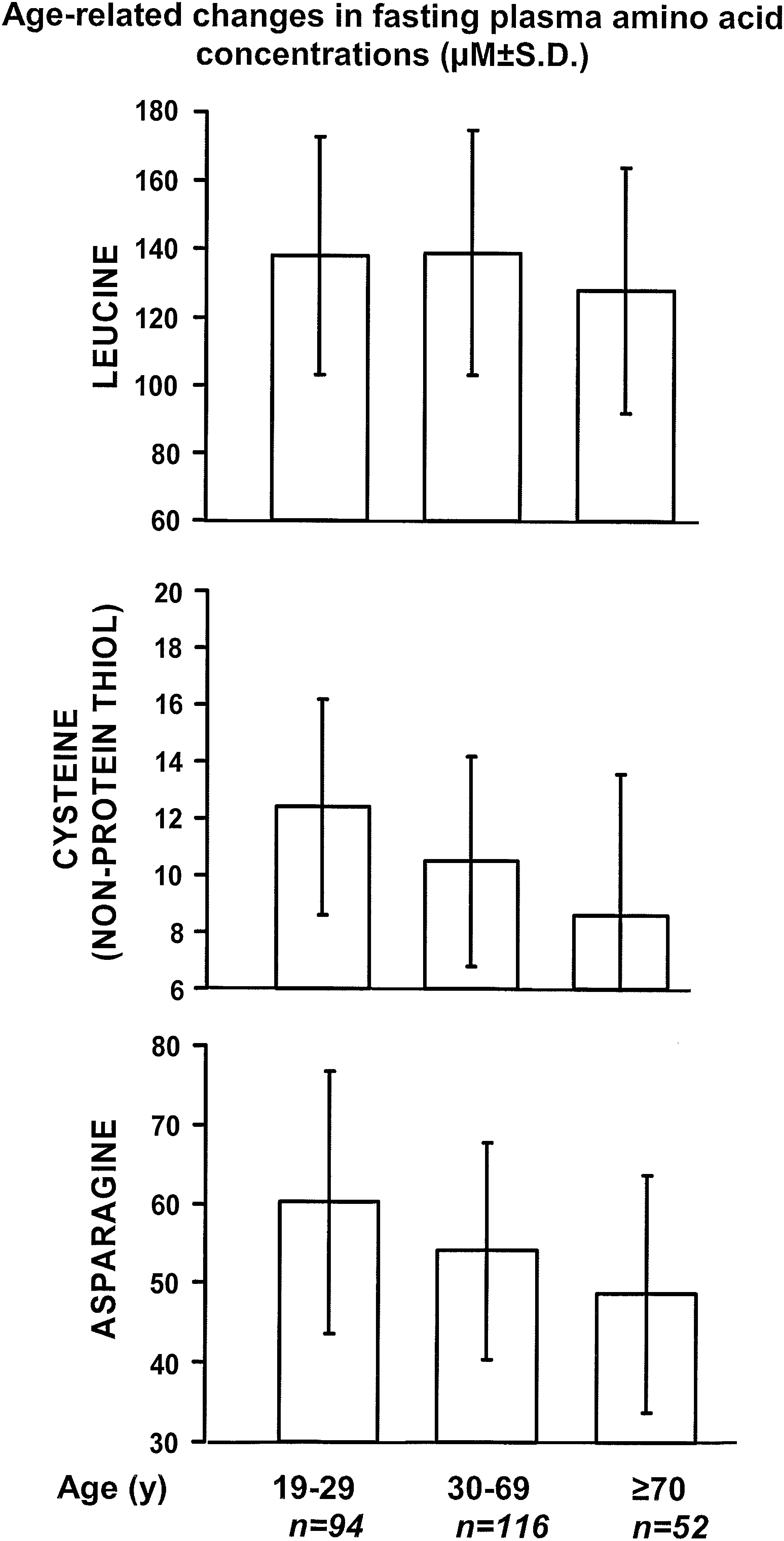
Last but not least, Dr. Dröge has shown that the plasma cysteine concentration in the so-called postabsorptive period (i.e., in the early morning after a period of starvation) declines in the course of aging (7, 9, 16). This decrease in cysteine concentration begins already in the third decade of life and is believed to be the major cause of the age-related increase in oxidative stress. The loss of cysteine in HIV infection is typically associated with an increased cysteine catabolism in skeletal muscle tissues and an increased export of sulfate out of this tissue into the blood, but such a muscular sulfate excretion has not been found in healthy elderly persons (unpublished observation). The detailed analysis of the age-related changes rather indicated that the decrease in plasma cysteine concentrations is in this case caused by a change in amino acid homeostasis because it is associated with a corresponding decrease in plasma asparagine concentrations and, to a lesser extent, by a decrease in amino acids that typically occur in the plasma at relatively higher concentrations (3, 7, 9) (Fig. 3). The age-related decline in the limiting glutathione precursor cysteine, therefore, appears to result from a decreasing ability to recruit free amino acids from ones own skeletal muscle proteins during periods of starvation. As this process is mainly mediated by the autophagic protein catabolism and controlled by the insulin receptor signaling cascade, these findings provide a link between the age-related increase in oxidative stress and the increased lifespan that was found in several animal mutants with a defect in the insulin signaling pathway (3, 7, 9).

In view of the massive loss of skeletal muscle function and the increase in inflammatory cytokine concentrations in the course of aging, Dr. Dröge and his colleagues also investigated the effect of cysteine supplementation on these parameters in frail elderly patients. This clinical trial showed that cysteine supplementation during a 6-week program of physical exercise caused an additional increase in muscle function on top of the effect of exercise alone and a relative decrease in the concentration of the inflammatory cytokine tumor necrosis factor alpha (18).
Additional Achievements
Insulin receptor signaling and O2 chemosensitivity
In addition to the redox regulation of the immune system, Dr. Dröge and his colleagues investigated several other signaling pathways including the hypoxic ventilatory response and erythropoietin production as indicators of O2 chemosensitivity (21) and the insulin receptor signaling pathway (20, 29). The kinase activity of recombinant insulin receptor kinase fragments and of the intact insulin receptor was shown to be increased by hydrogen peroxide (29) and the insulin reactivity in vivo was shown to be decreased in persons supplemented with NAC (20). As the insulin receptor signaling cascade has been implicated in lifespan extension in several longevity mutants of animals, and more specifically in the regulation of autophagy and amino acid homeostasis, the redox responsiveness of this signaling cascade suggested that the age-related decrease in cysteine and glutathione levels under starving conditions may be part of a vicious cycle (7, 9) and critically involved in the mechanism of aging and death (3).
Recent Position
Dr. Dröge was a retired professor of immunology and cell biology at the University of Heidelberg and head of a department at the German Cancer Research Center in Heidelberg. He was also a senior consultant of Research and Development at Immunotec, Inc., in Montreal, Canada.
According to Dr. Dröge, “It is a great privilege of a scientist that she or he can enjoy fundamentally new insights and see the secrets of life unfolding. Our generation had the pleasure to see the field of redox physiology unfolding all the way from basic biology to clinical medicine.”
Professor Wulf Dröge thanked all colleagues of his laboratory at the National Cancer Research Center in Heidelberg as well as his clinical partners from the University Hospitals of Heidelberg and Mannheim who made these studies and clinical trials possible. Mrs. Ingrid Fryson wrote practically all the texts cited in this report.
Footnotes
Abbreviations Used
Editor's note: While this article was in process, Dr. Dröge unexpectedly passed away on December 18, 2010, one day after his 71st birthday. This work was not subjected to the standard full-length review to accommodate for the time-sensitive nature of emergent circumstances.
Author note: Ralf Kinscherf is a professor for anatomy and cell biology (chair) and head of the Department of Medical Cell Biology at the University of Marburg, Germany. He studied biology and sports/sports science at the University of Heidelberg, Germany, and worked as a postdoctoral fellow in Dr. Dröge's department at the German Cancer Research Center on clinical projects and complementary laboratory studies in the field of redox physiology.
For a list of frequently cited articles published by Prof. Dröge, see Supplementary Tables S1 and S2, available online at
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.