
Abstract
Malignant pleural mesothelioma (MPM), an asbestos-related aggressive malignant tumor of mesothelial origin, shows limited response to therapy and overall survival remains very poor. Reactive oxygen species play an important role in asbestos toxicity. Here, we found that the patients with MPM had significantly higher serum levels of thioredoxin-1 (TRX) than control population. The patients with advanced-stage MPM showed higher levels of TRX than those with early-stage MPM. The difference in overall survival between the groups with lower and higher serum TRX levels was significant. Our data suggest that serum TRX concentration could be a useful clinical marker for MPM. Antioxid. Redox Signal. 15, 685–689.
Introduction
Innovation
MPM is an aggressive malignant tumor of mesothelial origin and shows limited response to conventional chemotherapy and radiotherapy. Therefore, diagnosing MPM early is very important. ROS play an important role in asbestos toxicity, which is associated with the pathogenesis of MPM development. TRX is a small redox-active protein that demonstrates antioxidative activity associated with tumor growth. Here, we investigated the serum levels of TRX in 57 MPM patients and compared them with those of a population that had been exposed to asbestos without developing MPM.
We demonstrated that the patients with MPM had significantly higher serum levels of TRX than the population who had been exposed to asbestos but had not developed MPM. Also, we demonstrated that the patients with advanced-stage MPM showed higher levels of TRX than those with early-stage MPM. As the clinical stage of MPM is not related to the presence or absence of pleural effusion, and the early distinction of MPM patients from those with benign asbestos-related diseases is necessary, we propose that measuring serum TRX levels is an easy and useful method for the clinical management for MPM. Moreover, the difference in overall survival between the groups with serum TRX levels that were lower and higher than the assumed cutoff of 60 ng/mL was significant. It is suggested that TRX would be a useful serum prognostic factor for MPM. This is the first report about the relationship between serum TRX and MPM.
In the diagnosis of lung cancer, serum markers such as CEA, CYFRA, proGRP, and SCC play supportive roles to confirm the diagnosis. There have been several reports about candidates for clinically useful markers for MPM. Indeed, some of them have been reported to be useful serum markers for MPM, such as mesothelin and osteopontin (16, 19); however, little is known about their biological functions or effects on MPM cells. For further improvement of the specificity and sensitivity of diagnosis, research into the development of novel biological markers is urgently required.
It is well known that MPM is associated with asbestos exposure (20, 21, 30). The lifetime risk of MPM is closely related to occupational and/or environmental asbestos exposure history (17). Although asbestos usage has recently decreased in Western countries and Japan, the incidence of MPM is expected to markedly increase over the next few decades because there is the long latency period (20–40 years) between asbestos exposure and tumor development (24).
A previous report demonstrated that reactive oxygen species (ROS) such as hydrogen peroxide and superoxide anion are important mediators of malignancies of the human lung and asbestos toxicity (8), which is associated with the pathogenesis of MPM development. In oxidative stress conditions, thioredoxin-1 (TRX), a small redox-active protein that possesses antioxidative activity and acts as a redox-regulating multifunctional protein, reduces the levels of ROS as part of the antioxidant defense (5).
In this study, we evaluated the clinical role of serum TRX in MPM and found that the patients with MPM had significantly higher serum levels of TRX than a population with a history of asbestos exposure, which suggested its usefulness as a marker for MPM.
Results and Discussion
Possible important roles of TRX in MPM
TRX was first identified from extracts of Escherichia coli B as a hydrogen donor that transfers hydrogen from NADPH to ribonucleotide reductase (5). TRX is a 12-kDa multifunctional protein containing a redox-active site (Cys-Gly-Pro-Cys), which undergoes NADPH-dependent reduction by TRX reductase, and reduced oxidized cysteine protein groups. TRX is ubiquitously expressed in various organisms. Human TRX has been cloned independently by two groups: it was first cloned as an IL-2 receptor α chain (CD25)–induced factor in HTLV-1–infected T-cell lines and designated as adult T-cell leukemia–derived factor (27), and another group cloned it as an IL-1–like growth factor produced by Epstein-Barr virus–transformed cells (2).
TRX is ubiquitously expressed in normal tissues and cells, and its expression can also be induced by a variety of physiochemical stresses, such as viral infection, mitogens, ultraviolet irradiation, hydrogen peroxide, and oxidative stress (12). TRX is mainly localized in the cytoplasm, and its secretion mechanism remains unclear. As human TRX was first cloned as a secreted adult T-cell leukemia–derived factor, its expression is markedly enhanced in HTLV-I–infected T cells (27). The plasma TRX level is elevated in certain human diseases including HIV infection and hepatitis C virus infection (13, 26).
Recent reports have shown that TRX affects a number of cellular responses, including cell growth, inflammation, and apoptosis, and that the redox regulation mediated by TRX is correlated with the pathogenesis of several oxidative stress–associated diseases (6, 28). On the other hand, it is well known that both oxidative stress and hypoxia are common features of tumors. Growing tumor masses need vascular networks. Although angiogenesis occurs in malignant tumors, it does not occur in an efficient manner, leading to switching between hypoxia and re-oxygenation conditions because of the irregular flow of oxygen, which causes oxidative stress (3). As cancer cells are often under high oxidative or hypoxic stress, they express high levels of antioxidant proteins, including TRX. For example, TRX expression is increased in several primary cancers, including lung, cervix, pancreatic, colorectal, breast, hepatocellular, and gastric carcinomas (9, 15, 25).
Serum levels of TRX in patients with MPM as a diagnostic marker
The human lung is more exposed to ROS caused by cigarette smoke and chemical pollutants than any other organ (10). Here, we investigated the serum levels of TRX in patients with MPM and compared them with those of a population that had been exposed to asbestos without developing MPM. We recruited a total of 91 subjects with a history of asbestos exposure. Of them, 57 had confirmed MPM, 19 had pleural plaques and/or asbestosis, and 15 had no asbestos-related lesions despite being exposed to asbestos, i.e., were healthy. Their characteristics are shown in Table 1.
All individuals were exposed to asbestos.
MPM, malignant pleural mesothelioma.
The receiver operating characteristic (ROC) curves for serum TRX levels showed that the patients with MPM had an area under the ROC curves of 0.8178, compared with those with benign asbestos-related diseases (asbestosis or pleural plaques) and those who were healthy despite asbestos exposure (95% confidence intervals [95% CI]: 0.7482–0.8873). At the optimal cutoff value of 60 ng/mL, the diagnostic sensitivity was 71.9% and the specificity was 85.0% (Fig. 1A).
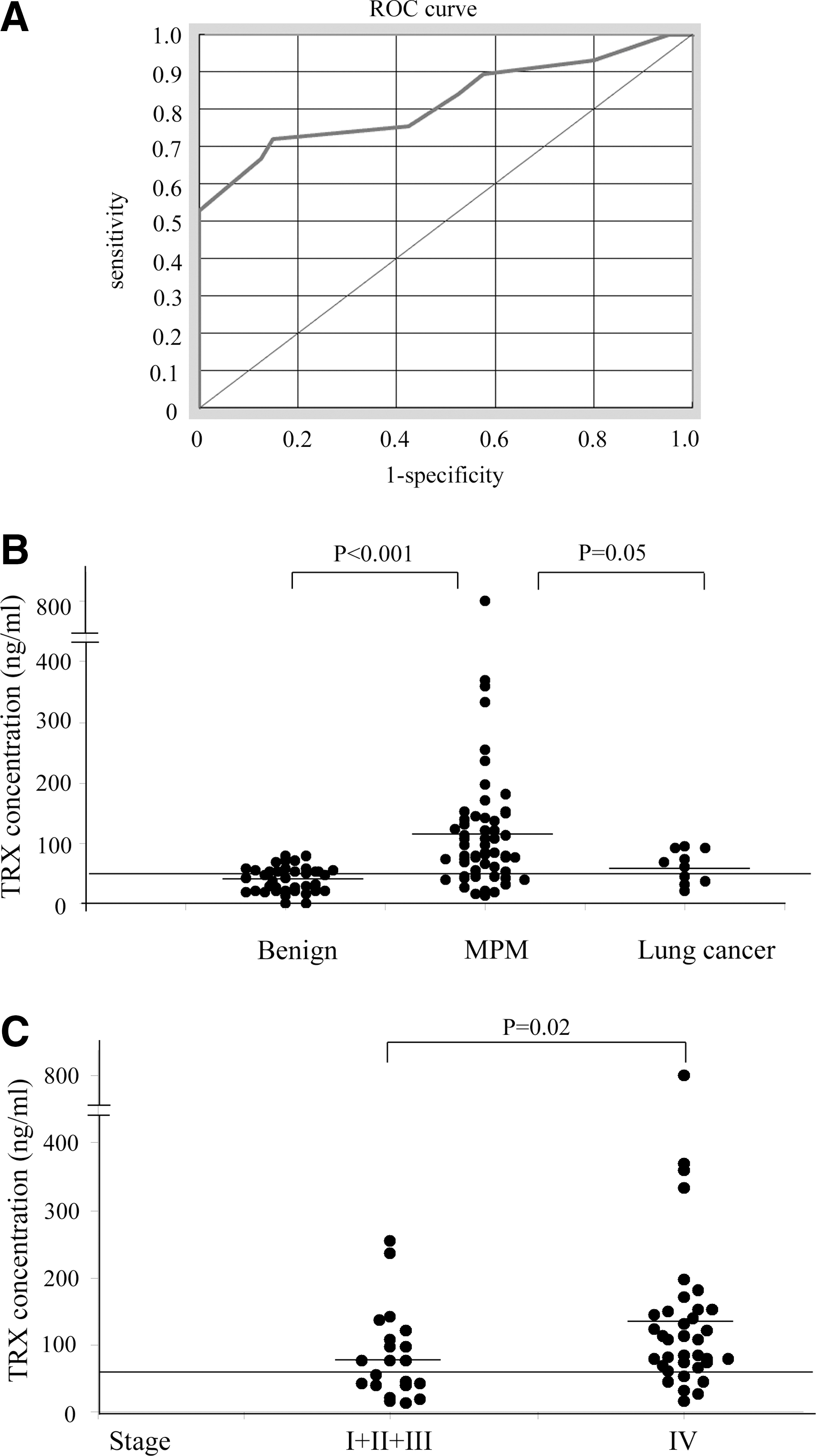
The serum TRX concentration of the patients with MPM was significantly higher (119.1±125.2 ng/mL) than that of the patients with benign asbestos-related diseases (asbestosis or pleural plaques) and the healthy individuals (40.1±20.4 ng/mL) (p<0.0001; Fig. 1B). Serum TRX level of healthy volunteers (n=5; age: 32.0±8.0; male/female: 3/2) who had never been exposed to asbestos was 4.8±2.7 ng/mL. The difference in serum TRX levels between the population with a history of asbestos exposure and the healthy volunteers was not statistically significant, suggesting that not only asbestos exposure but also MPM development is required for the elevation of serum TRX levels.
The positive predictive value of high TRX value for MPM was 89.1%, and the negative predictive value was 64.4%. Although the diagnostic sensitivity was not high (71.9%), its positive predictive value was fairly high (89.1%), suggesting that high serum TRX levels are supportive of a diagnosis of MPM. Interestingly, we found that the serum TRX levels of patients with lung cancer involving malignant pleuritis (n=10) were significantly lower (61.3±27.0 ng/mL; p=0.05) than those of the MPM patients (Fig. 1B). The differences in serum TRX levels between the MPM histological groups (epithelioid: 111.0±90.4 ng/mL; sarcomatoid: 104.6±62.8 ng/mL; biphasic: 73.8±19.8 ng/mL; and desmoplastic: 119.4±32.9 ng/mL) were not statistically significant. There were no significant differences in TRX levels among the subjects with benign asbestos-related diseases (asbestosis or pleural plaques) and those who were healthy despite having a history of asbestos exposure (40.1±18.7 and 40.0±23.1 ng/mL).
It has been reported that TRX mRNA is strongly expressed in MPM cells (18), and TRX protein was immunohistochemically detected in MPM tissues (7). Although its precise cellular mechanism has not been fully investigated, these reports indicated that a correlation exists between the TRX system and MPM development. Here, we evaluated the clinical role of TRX as a serum biomarker for MPM and found that patients with MPM had significantly higher serum levels of TRX than control population, suggesting its useful roles as a diagnosing and prognostic marker for MPM.
Serum levels of TRX in patients with MPM as a prognostic marker
An elevated level of plasma TRX was reported in AIDS patients with poor prognoses and was found to be inversely correlated with the intracellular glutathione level. Also, the serum TRX levels of patients with HCV infection increased with the progression of liver fibrosis (26). Therefore, the plasma or serum level of TRX is a good marker of the oxidative stress caused by viral infection.
On the other hand, the overexpression of TRX in cancer cells seems to be associated with the promotion of cancer cell growth, a worse prognosis, and the development of resistance to anticancer agents. These data suggest a role for TRX as a target of cancer therapy or a tumor marker (1).
Here, we demonstrated that the serum TRX levels of the MPM patients gradually increased according to the progression of the disease. The patients with stage IV MPM had significantly higher levels of TRX (139.9±146.1 ng/mL) than the patients with stage I–III disease (82.7±68.0 ng/mL) (stage I: 67.1±25.6 ng/mL; stage II: 110.5±73.0 ng/mL; stage III: 74.5±72.8 ng/mL) (p=0.024; Fig. 1C).
To study the relationship between serum TRX levels and the patients' clinical courses, we separated the patients based on their serum TRX levels at the time of the first measurement. Among the 57 MPM patients, we were able to closely follow-up 56 patients for 1400 days. The first group included patients with serum TRX levels lower than 60 ng/mL, the cutoff value that we used. In this group of 16 patients, the mean serum TRX value was 34.2 ng/mL (interquartile range: 21.2–43.6). The other group included the remaining 40 patients with serum TRX levels higher than 60 ng/mL, whose mean serum TRX value was 160.0 ng/mL (interquartile range: 79.6–151.4). The difference in overall survival between the two groups was significant (p=0.030; Fig. 2), which suggested the usefulness of serum TRX value as a marker for estimating prognosis. On the other hand, Kahlos et al. (7) reported that there was no significant association between TRX expression in the tissues of MPM patients and survival. Although they assessed the levels of TRX expression using the staining intensities of resected specimens, we consider that serum TRX levels are more closely associated with the general condition of the patient.

Moreover, Cox's regression analysis was performed on 56 MPM patients for whom data on age, sex, histology, stage, and serum TRX level were available, and an independent statistically significant prognostic effect of stage on survival (IV versus I–III; HR, 3.15; 95% CI: 1.23–8.04; p=0.017) was found.
Several studies have demonstrated that overexpression of TRX enhances cancer cell growth (4). In addition, high levels of TRX expression have been shown to correlate with highly invasive and metastatic tumor activity (11). Further, high levels of TRX and other antioxidant proteins have also been shown to be correlated with resistance to various chemotherapeutic agents such as cisplatin (23). From these observations, TRX seems to play an active role in both cancer growth and cancer progression through the inhibition of apoptosis, the stimulation of metastatic and invasive activity, and chemotherapy resistance. The present data suggests that TRX also plays an important role in tumor progression of MPM and could be a useful marker for prognosis of the patients with MPM.
Materials and Methods
Patients and serum samples
We studied the TRX levels in sera collected from 91 individuals who presented at the Department of Respiratory Medicine of Hyogo College of Medicine Hospital from 2005 to 2007. All of the individuals had a documented asbestos exposure history. Fifty-seven individuals had MPM, which was diagnosed using histopathological samples by pathologists skilled in the diagnosis of MPM. All patients were classified according to the staging system of the International Mesothelioma Interest Group (22). Thirty-four individuals had benign asbestos-related diseases (asbestosis or pleural plaques) or were healthy despite their previous asbestos exposure. The study was approved by our ethics committee in accordance with the 1975 Declaration of Helsinki. Informed consent was obtained from all patients. Serum samples were collected before treatment, immediately frozen in liquid nitrogen, and stored at −80°C until use.
Measurement of TRX
Serum TRX concentrations were measured using an enzyme-linked immunosorbent assay (ELISA) kit (Redox BioScience, Kyoto, Japan) according to the manufacturer's instructions.
Statistical analysis
The nonparametric Mann–Whitney U test was used to compare two groups of serum samples. In all tests, a p-value of <0.05 was considered significant. To estimate the significance of serum TRX values, ROC curves, area under the ROC curves, and their 95% CI were calculated using standard techniques. To obtain appropriate serum level cutoff values, we calculated the total sensitivity and specificity for each cutoff value and then chose the cutoff values that maximized each factor. Estimates of the probability of survival were calculated by the Kaplan–Meier method and compared using the log-rank test. To evaluate the prognostic significance of TRX with regard to the survival of patients with MPM, Cox's proportional hazards regression analysis was carried out.
Footnotes
Acknowledgments
The authors thank Ms. Hidemi Kitai for providing technical assistance. This work was supported by grants from KAKENHI, a Grant-in-Aid for Scientific Research (C) (20590936), Funds for Cancer Research from the Hyogo Prefecture Health Promotion Association, and Special Coordination Funds for Promoting Science and Technology (H18-1-3-3-1).
Author Contributions
C. Tabata, R. Tabata, and T. Nakano designed the research. C. Tabata and R. Maeda performed the research. C. Tabata, R. Eguchi, and Y. Fujimori collected data. C. Tabata and R. Tabata analyzed and interpreted the data. C. Tabata performed statistical analysis. C. Tabata and R. Tabata wrote the manuscript.