
Abstract
Antineoplastic agents induce oxidative stress leading to lipid, carbohydrate, protein, and DNA damage. We sought to explore the role of drug-induced oxidative stress on breast cancer patient's survival. We observed that neoadjuvant patients presented a marked raise in DNA damage and protein carbonyl levels after chemotherapy, whereas postchemotherapy DNA repair activity of the KU86 enzyme and total antioxidant capacity of the plasma were higher in the adjuvant group. With respect to patient's survival, we observed that increasing levels of KU86 and antioxidant capacity of the plasma during chemotherapy significantly influenced the survival rates of the patients, protecting from disease recurrence and death. Our results suggest that chemotherapy induces a certain level of systemic oxidative stress, which is maintained along successive clinical interventions and could influence the clinical outcome of the patients. Antioxid. Redox Signal. 15, 903–909.
Introduction
Effects of Chemotherapy on Oxidative Damage and Antioxidant Markers in Blood Plasma
It has been reported that breast cancer patients suffer increased DNA damage, either independently or because (and this is more likely) breast cancer patients have impaired DNA repair mechanisms, particularly those specialized in the removal of oxidative damage (12), and increased serum concentrations of carbonyls (19). Under our experimental conditions, neoadjuvant chemotherapy increased DNA and protein damage, whereas these markers remained unchanged in the adjuvant group after chemotherapy. From these results, it is not possible to discern why adjuvant patients do not present greater DNA and protein damage after chemotherapy, but an association was observed between these data, the activation of DNA repair enzyme KU86, and the increased total antioxidant capacity after chemotherapy in the adjuvant group. It has been well established that solid tumors cannot grow beyond 2 mm if angiogenesis is not activated. Oxidative stress due to tumor size-induced hypoxia is thought to play an important role in cancer angiogenesis and progression (9, 25). Indeed, although the results were not statistically significant, we observed a direct correlation between tumor size and DNA damage before chemotherapy (data not shown), which could contribute to the differences in the levels of oxidative damage markers observed between the groups. On the other hand, the adjuvant patients were subjected to surgery before chemotherapy, which may have modified their oxidative status prior to systemic therapy, given that free radicals are known to be produced by macrophages and neutrophils during healing (18). Potischman et al. (15) contributed to the very scarce data regarding the effects of surgery and chemotherapy on the oxidative status of breast cancer patients, in a study that reported a significant increase in the plasma levels of major antioxidants, such as α-tocopherol and retinol, both in patients subjected to surgery alone and in those treated surgically and with chemotherapy. Accordingly, it seems plausible that, under our experimental conditions, activated antioxidant defense may inhibit the increased presence of oxidative stress markers in the adjuvant group, although basal levels of oxidative damage with respect to chemotherapy administration remain high in comparison with those of the neoadjuvant group.
Innovation
In recent years, oxidative stress and antioxidant status have attracted increasing interest among basic and clinical researchers. Notable improvements in our knowledge about microenvironmental influence on gene expression and the impact of free radicals on key cancer-related processes, such as tumor cell spreading, angiogenesis, and drug resistance, underlie novel scientific approaches to the study of cancer biology in the field of translational oncology. Nevertheless, preclinical or clinical data about the role of oxidative stress status in therapeutic response and survival remain extremely scarce. To the best of our knowledge, this article is the first to report a significant and positive influence of a systemic antioxidant status marker, such as the antioxidant capacity of the plasma, and the activity of KU86, a DNA repair enzyme closely related to the damage inflicted by free radicals, on the survival rates of breast cancer patients subjected to chemotherapy. This is an interesting issue that warrants consideration to design new experiments to gain further insight into its potential therapeutic applications, given that systemic antioxidant status is an exogenously modifiable factor. The novel results described and discussed in this article may serve as a conceptual scaffold for designing experiments to better understand the influence of oxidative stress on the development of antineoplastic treatment resistance and its impact on patient survival rates.
Correlation Between Oxidative Stress and Patients Clinical Outcome
Since the publication of the results from the National Surgical Adjuvant Breast and Bowel Project B-18 trial and the European Organization for Research and Treatment of Cancer Trial 10902, it is well known that neoadjuvant and adjuvant chemotherapy are equivalent with respect to disease-free survival (DFS) and overall survival (OS) (8, 22). These results were obtained after adjusting for tumor size, among other factors, this being the major criterion regarding preoperative chemotherapy to allow breast conserving surgery. Thus, the results of our multivariate analysis show that greater tumor size significantly shortens time to recurrence and death. Therefore, the variable “group,” dividing the patients into neoadjuvant and adjuvant settings, was eliminated from the final model, as tumor size was included. It is very important to take into account that factors other than tumor size may also influence survival rates and contribute to the clinical outcome. To the best of our knowledge, the present study is the first to report that changes in the activity of DNA repair enzyme KU86 and in the antioxidant capacity of the plasma during chemotherapy may influence DFS in breast cancer patients. As indicated by the results of the multivariate analysis, an increase in KU86 activity has a protective effect against disease recurrence and death, regardless of further systemic therapy. Moreover, higher levels of total antioxidant capacity of the plasma after chemotherapy increase survival rates of women who, subsequent to chemotherapy and surgery (regardless of the sequence of these interventions), undergo hormone therapy. This latter interaction suggests that as oxidative damage becomes increasingly harmful with successive clinical interventions, higher levels of plasma antioxidants improve patients' survival rates, which may be highly significant because microenvironmentally high levels of oxidative stress have been related with the promotion of tumor cell migration, angiogenesis, and metastasis, especially regarding cancer stem cells (CSCs), a specific tumor cell type with self-renewal capacity and multipotency, suspected of being responsible for carcinogenesis, disease recurrence, and reduced survival rates (24, 25). Indeed, it has been suggested that induced oxidative stress may play a role in treatment failure and contribute to the observed disease relapse despite tumor shrinkage (3, 25). With respect to KU86 activity, whether CSCs or other tumor circulating cells use this molecular mechanism to survive in the blood stream and metastasize remains unknown, but previous data point to intracellular glutathione and antioxidant enzymes as the main sources of reducing power in CSCs (5). Nevertheless, it seems reasonable to conclude that increased DNA repair capacity in circulating cells in breast cancer patients subjected to systemic and surgical therapy may contribute to reducing treatment toxicity and cellular mutagenesis.
Concluding Remarks and Future Directions
As a possible cause of treatment failure in breast cancer patients, changes in oxidative status and antioxidant response should be studied carefully to establish an effective strategy for decreasing systemic oxidative stress in patients receiving chemotherapy, because the antioxidant capacity of the plasma is a modifiable factor that could have therapeutic applications. In this respect, several studies have examined chemotherapy toxicity and efficiency and antioxidant supplementation (2, 23). In general, these articles conclude that antioxidant supplementation does not affect chemotherapy efficiency or reduce dose-limiting toxicity, although a lack of adequate statistical power was a common limitation in these studies. Perhaps the question should not be whether antioxidant supplementation is beneficial or detrimental per se to a patient's clinical outcome, but rather whether antioxidant supplementation should be administered during the therapeutic schedule, as suggested by the results of the present study. Our data show that patients who undergo a second clinical intervention in possession of increased levels of systemic antioxidant capacity achieve better survival rates. Nevertheless, larger well-designed studies are needed to clarify the role of exogenous antioxidants in chemotherapy efficiency and toxicity. With respect to this conclusion, our study provides a deeper insight into the oxidative events accompanying chemotherapy in different treatment settings and represents a step forward in the study of the potential application of antioxidants in breast cancer treatment. Foreseeably, the next step should be to identify the plasma antioxidants that confer a survival advantage against breast cancer and to study its protective activity in a lager cohort, followed by a well-designed randomized clinical trial. Indeed, our research group is currently working in this direction, on the basis of the conclusions of the exploratory work discussed in this article.
Notes
Patients and Samples
This study included patients diagnosed with breast carcinoma at the Complejo Hospitalario de Jaen (Jaen, Spain) between 2005 and 2007, for whom chemotherapy was scheduled as part of their treatment. All patients were initially staged based on physical examination, radiologic findings, and pathologic examination of tumor biopsies. Finally, 70 patients were enrolled in this study after giving their signed informed consent. Of these patients, 38 received neoadjuvant chemotherapy and 32 received adjuvant chemotherapy, thus constituting the two experimental groups of this study. Chemotherapy consisted of anthracycline- and/or taxane-based regimens, as determined by the medical oncology team. The pathologic and clinical information was extracted from the medical reports produced in the Oncology Department Registry. Matched blood samples were collected from each patient before and after six cycles of chemotherapy. This study was conducted following the guidelines of the local ethical review board and in accordance with good clinical practices and the tenets of the Declaration of Helsinki.
Blood collection and processing
Matched blood samples were collected from each patient before and after six cycles of chemotherapy. Approximately 5 ml of blood was taken from each patient, by venous puncture, drawn into an ethylene diamine tetra-acetic acid (EDTA)–containing tube (Vacutainer®EDTA Tubes; BD), and centrifuged at 1000 g for 15 min. The plasma was kept in a separate tube and frozen at −80°C. The white blood cells were removed, washed in 3 ml of RPMI 1640 (Sigma-Aldrich), carefully overlain on 5 ml of Histopaque 1077 (Sigma-Aldrich), and centrifuged at 700 g for 30 min. The cells were kept until needed for analysis at −80°C in a cryoprotectant solution containing 90% fetal calf serum (Sigma-Aldrich) and 10% dimethyl sulfoxide (Sigma-Aldrich).
Alkaline single-cell gel electrophoresis (comet assay)
DNA strand breaks were detected using the alkaline comet assay or single-cell gel electrophoresis, as previously described (6, 7). The nucleoids stained with 4',6-diamidine-2-phenylindol dihydrochloride were scored using a Leica DMLS fluorescence microscope (Leica Microsystems). One hundred comets from each gel (scored at random) were scored using computerized image analysis (Komet 3.0; Kinetic Imaging Ltd.) and the percentages of fluorescence in the comet tail (representing the fraction of DNA in the tail) and head (representing the fraction of DNA in the head) were measured.
Plasma protein carbonyl assay
The levels of plasma protein carbonyl groups were assessed using Protein Carbonyl Kit (Cayman Chemical Company), according to the manufacturer's instructions. Total protein concentration in the plasma samples was measured using Biuret Colorimetric Assay Kit (Spinreact S.A. Barcelona). The results were expressed as nmol of carbonyl proteins per mg of total proteins in the plasma.
Determination of the total antioxidant capacity of the plasma
Total antioxidant capacity was assessed using the method described by Re et al. (17). The resulting values were compared with a calibration curve constructed diluting the synthetic antioxidant Trolox (Fluka) (concentration range: 0–20 μM Trolox in the well). The results were expressed as μM Trolox.
DNA repair activity of enzymes replication protein A and KU86
The activity of the DNA repair enzymes replication protein A (RPA) (single-strand breaks) and KU86 (double-strand breaks) was assessed by an immunoenzymatic assay using the Active Motif RPA and KU70/86 DNA Repair Kits (Active Motif), according to the manufacturer's instructions. Previously, the cell concentration in the samples was measured using the hematologic analyzer Sysmex KX21 (Sysmex Corporation), and nuclear proteins of blood lymphocytes were extracted and quantified using the Nuclear Extract Kit (Active Motif) and the Bicinchoninic Acid Kit (Pierce Biotechnology), respectively.
Statistical analysis
Quantitative data were expressed as the mean±standard error per group. The general linear model for repeated measures was used to determine significant differences between groups. Chemotherapy status (prechemotherapy and postchemotherapy) was considered as an intragroup factor. Oxidative stress and antioxidant markers were considered as intergroup factors. Statistical significance was established at p≤0.05, p≤0.01, and p≤0.001. With respect to survival analysis, DFS was the primary end point of this study. DFS, in which relapse or death as a result of any cause is considered as an event, was calculated from the date of the first chemotherapy cycle to that of the first event or to the date of censoring if eventless. OS was a secondary end point and was calculated from the date of the first chemotherapy cycle to that of death or that of censoring if alive. Both DFS and OS were analyzed by Kaplan and Meier's method, and the log-rank test was used to test for differences between the curves. Univariate and multivariate analyses were performed for the Cox regression model for survival, using DFS and OS as end points. As all oxidative stress and antioxidant markers were analyzed twice for each patient, before and after chemotherapy, paired data were available for each of these markers. An extended Cox regression model with time-dependent covariates and stratified by the nodal status (negative vs. positive) was employed for univariate and multivariate analyses. Categorical variables such as group (adjuvant vs. neoadjuvant), hormone therapy (yes vs. no), chemotherapy (anthracyclines and taxanes vs. anthracyclines alone), Tastuzumab (yes vs. no), and biological subtype (basal vs. luminal and basal vs. Her2) were added as nontime-dependent covariates to the Cox regression model. Potential prognostic factors were included in the multivariate model following both statistical and clinical–biological criteria. Factors with p≤0.1 in the univariate analysis were included in the multivariate analysis together with significant interactions, such as that between hormone therapy and total antioxidant capacity of the plasma, which were selected on the basis of previous data indicating that circulating sex hormone levels may have a significant impact on the total antioxidant capacity of the plasma and/or particular antioxidants (4, 14). The stepwise backward elimination method with model removal set at p≤0.05 was used in the multivariate analysis to obtain the final model. All statistical analyses were carried out using SPSS 15.0 software.
Results
Patient population and clinical characteristics
The demographic and clinical characteristics of the patients included in this study are shown in Table 1. In brief, most of the patients were aged between 40 and 59 years old at diagnosis and there was a high proportion of women with ductal carcinoma, later stage, high histological grade, oestrogen receptor positive, progesterone receptor positive, and Her2 receptor negative.
Results are presented as n (%) of 38 patients and 32 patients per neoadjuvant and adjuvant groups, respectively.
AJCC, American Joint Committee on Cancer.
Oxidative damage markers
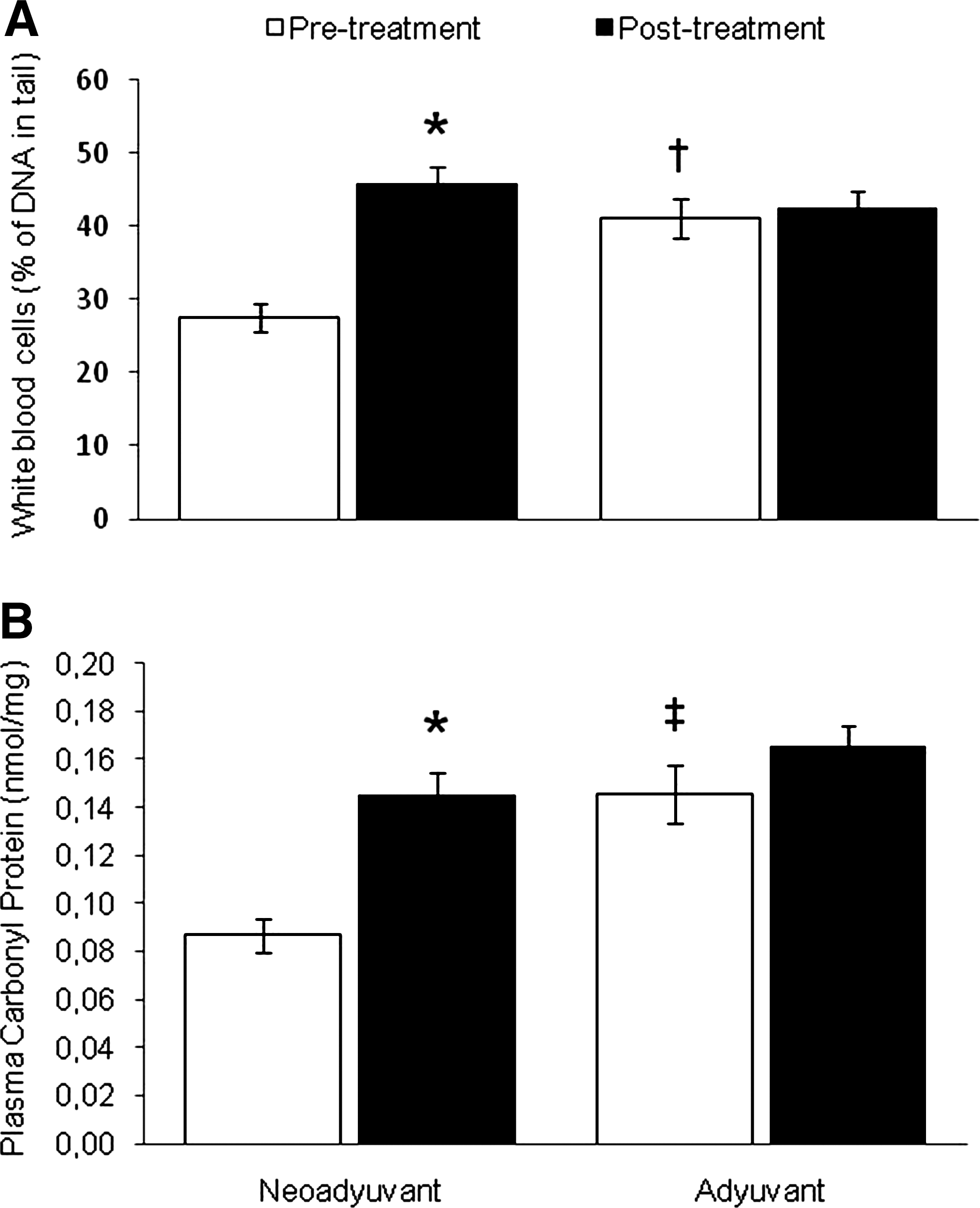
Under our experimental conditions, DNA damage increased in the neoadjuvant group after chemotherapy. Concerning differences between groups for the same treatment period, the neoadjuvant group presented a lower percentage of DNA in tail before treatment with respect to the adjuvant group (Fig. 1A). A similar results profile to that presented for DNA oxidative damage was found in relation to plasma protein carbonyls (Fig. 1B).
DNA repair activity and total antioxidant capacity of the plasma
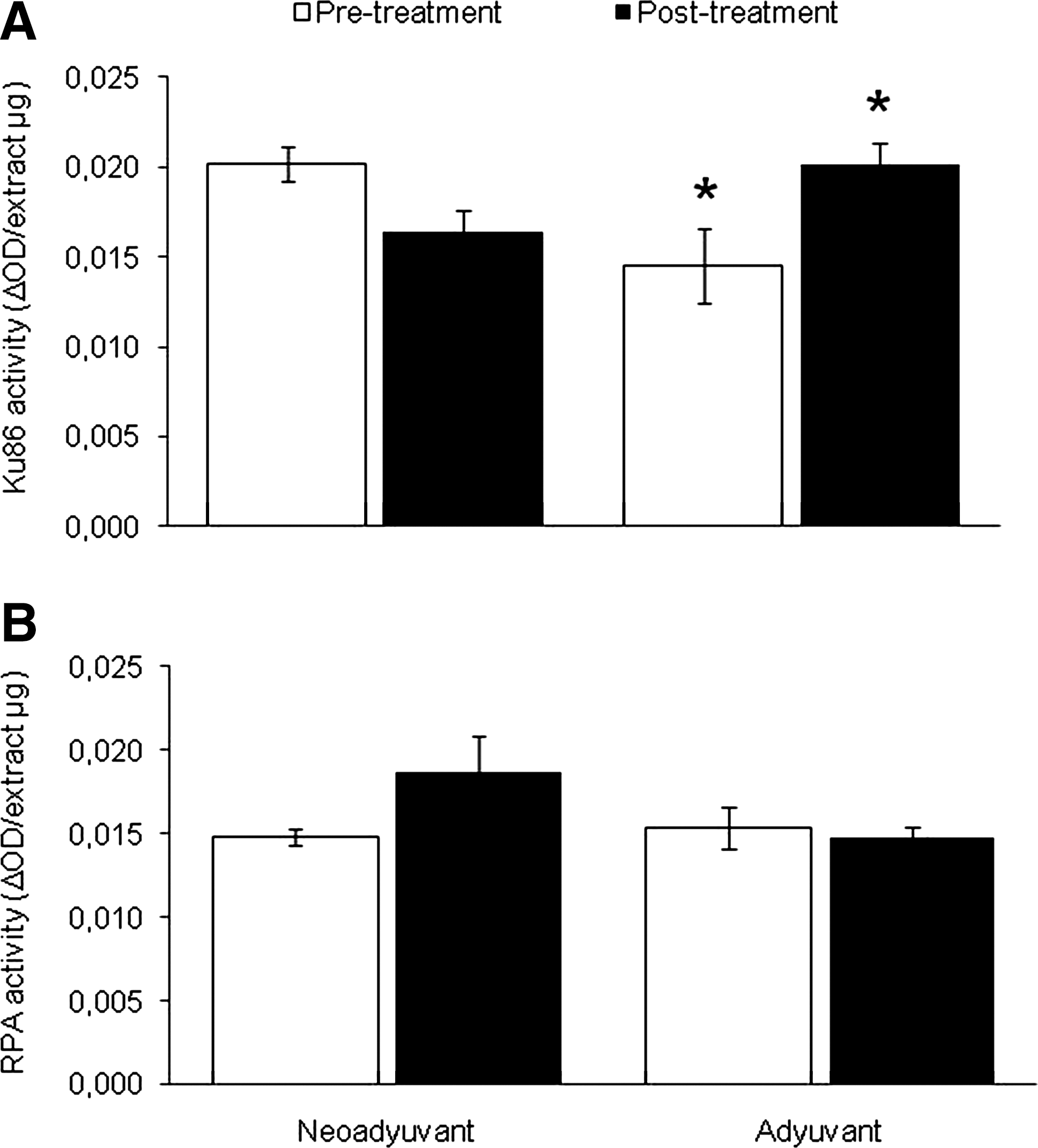
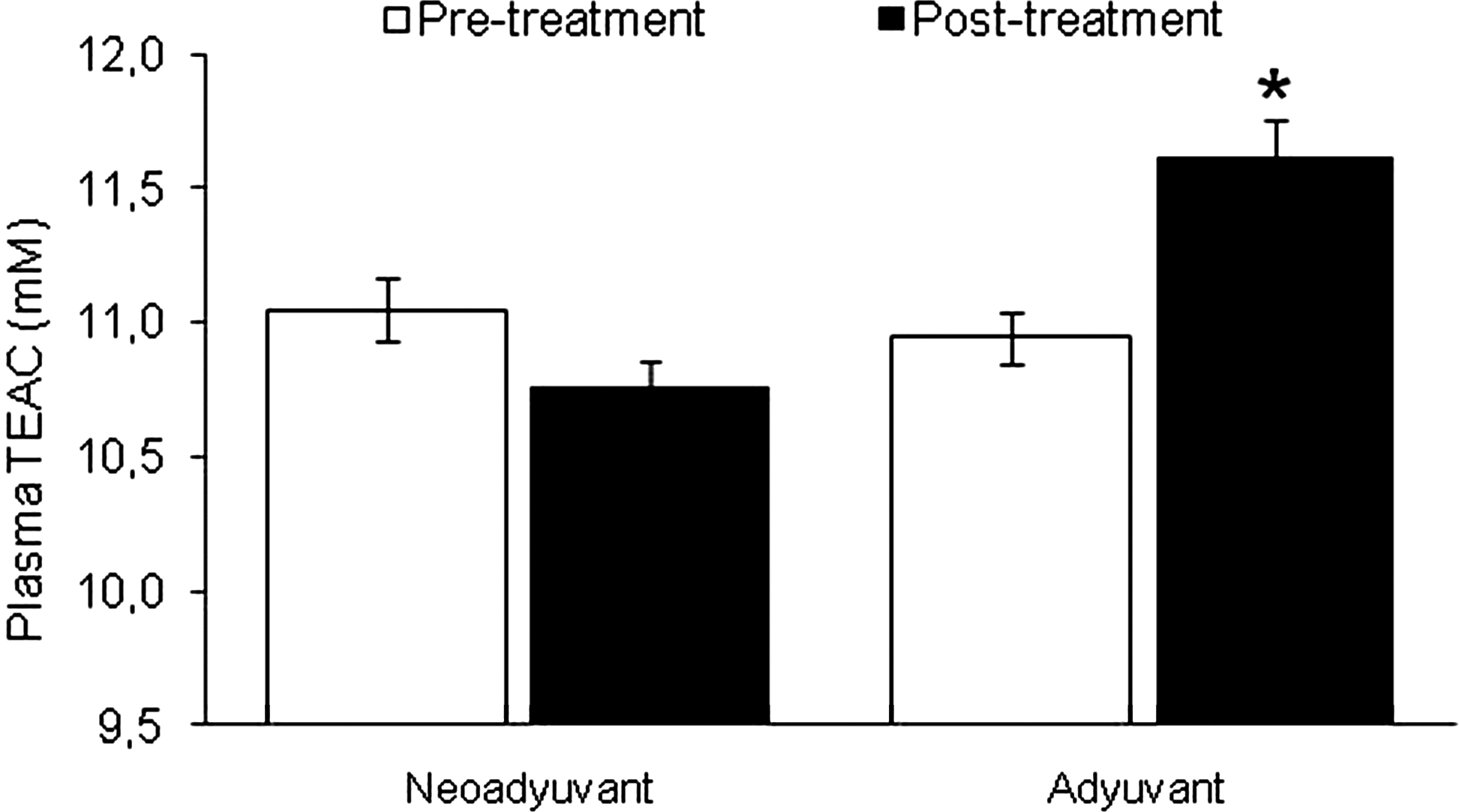
KU86 activity (Fig. 2A) varied significantly between groups, being lower before chemotherapy and higher after chemotherapy in the adjuvant setting compared with the neoadjuvant setting. RPA activity (Fig. 2B) did not significantly change after treatment among any of the studied groups and did not vary between groups before or after the treatment. Total antioxidant capacity of the plasma (Fig. 3) showed increased values in the adjuvant group after chemotherapy and was significantly lower in the neoadjuvant group compared with the adjuvant group after chemotherapy treatment, although no differences between the groups were found before treatment.
Oxidative stress during chemotherapy and clinical outcome
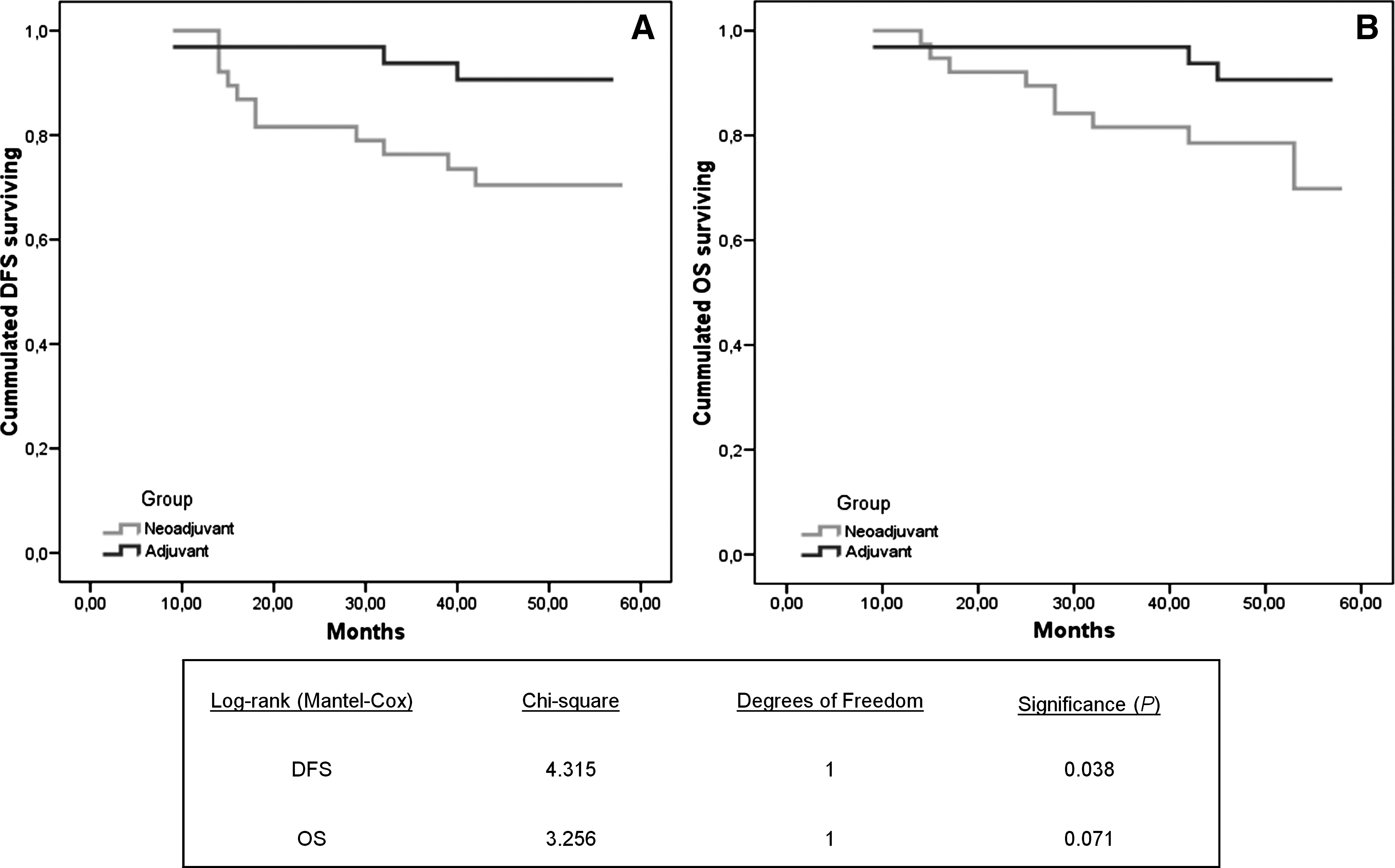
DFS and OS were evaluated with a mean follow-up time of 50.1 months (range: 9–58 months). The mean DFS times were 3.97 and 4.51 years in the neoadjuvant and adjuvant patients, respectively, whereas the median OS was 4.21 years in the neoadjuvant group and 4.55 years in the adjuvant group. The log-rank test revealed statistically significant differences between the DFS rates of the two groups (p=0.038) (Fig. 4). Tables 2 and 3 show the results of the univariate and multivariate analyses. In brief, KU86 activity and total antioxidant capacity of the plasma were associated with better DFS and OS, whereas higher tumor size was associated with shorter survival rates.
CI, confidence interval; DFS, disease-free survival; HR, hazard ratio; OS, overall survival; TEAC, trolox-equivalent antioxidant capacity; RPA, replication protein A.
Footnotes
Acknowledgments
This work was supported by a grant from the Health Research Fund of the Spanish Ministry of Science and Innovation through the Carlos III Health Institute (ISCIII) [PI06/90388]. L. Vera-Ramirez was supported by a predoctoral grant from the “Fundacion para la Investigacion Biosanitaria de Andalucia Oriental-Alejandro Otero (FIBAO)” Research Foundation. S. Granados-Principal was supported by a predoctoral grant from the Spanish Ministry of Science and Innovation. The authors thank the patients who made this study possible. The authors also thank Ms. Capilla de la Torre and Ms. Manuela Exposito for their contribution to patient selection and statistical work, the oncologists and nurses at the Department of Oncology of the Complejo Hospitalario de Jaen for their collaboration, and Mr. Glenn Harding for professional editing of this article for use of English.
Abbreviations Used
This work was carried out at Department of Oncology, Complejo Hospitalario de Jaen, Jaen, Spain and Institute of Nutrition and Food Technology “José Mataix,” Biomedical Research Center, Health Sciences Technological Park, University of Granada, Granada, Spain.