
Abstract
Reactive oxygen species (ROS) are thought to have effects on T-cell function and proliferation. Low concentrations of ROS in T cells are a prerequisite for cell survival, and increased ROS accumulation can lead to apoptosis/necrosis. The cellular redox state of a T cell can also affect T-cell receptor signaling, skewing the immune response. Various T-cell subsets have different redox statuses, and this differential ROS susceptibility could modulate the outcome of an immune response in various disease states. Recent advances in T-cell redox signaling reveal that ROS modulate signaling cascades such as the mitogen-activated protein kinase, phosphoinositide 3-kinase (PI3K)/AKT, and JAK/STAT pathways. Also, tumor microenvironments, chronic T-cell stimulation leading to replicative senescence, gender, and age affect T-cell susceptibility to ROS, thereby contributing to diverse immune outcomes. Antioxidants such as glutathione, thioredoxin, superoxide dismutase, and catalase balance cellular oxidative stress. T-cell redox states are also regulated by expression of various vitamins and dietary compounds. Changes in T-cell redox regulation may affect the pathogenesis of various human diseases. Many strategies to control oxidative stress have been employed for various diseases, including the use of active antioxidants from dietary products and pharmacologic or genetic engineering of antioxidant genes in T cells. Here, we discuss the existence of a complex web of molecules/factors that exogenously or endogenously affect oxidants, and we relate these molecules to potential therapeutics. Antioxid. Redox Signal. 18, 1497–1534.
I. Introduction
II. T Cell
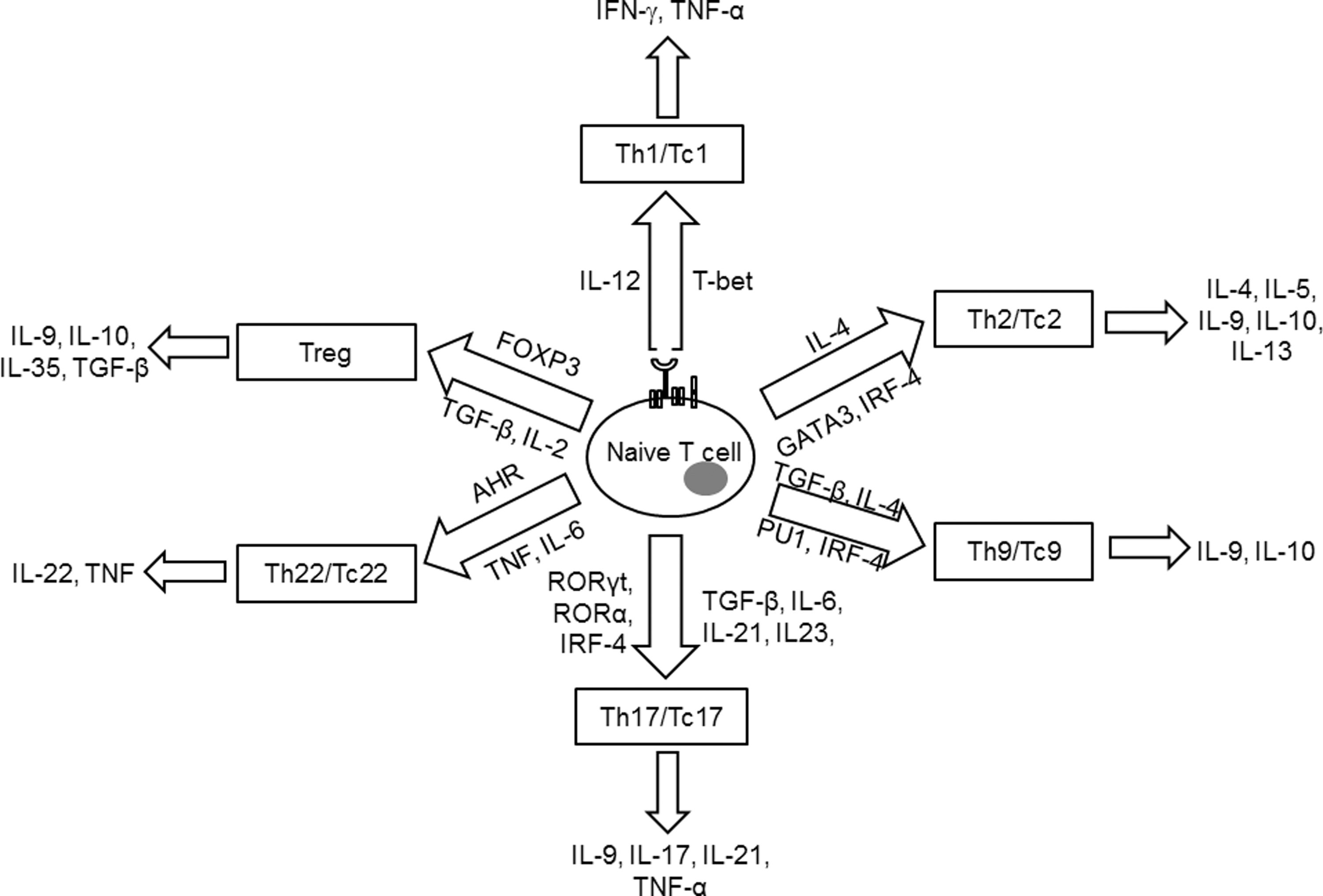
T cells are important in regulating the adaptive immune response to specific antigens. Based on the type of T-cell receptor (TCR) expression, T cells are either gamma delta (γδ) or alpha beta (αβ) T cells. γδ T cells comprise <5% of the total T-cell population, found at their highest abundance in the gut mucosa, consistent with their role in mucosal immunity. This review focuses on the αβ TCR-bearing T cells, which have a major role in controlling tumor or infectious disease along with autoimmune disease severity. αβ T cells are further categorized based on the cell surface expression of the co-receptor molecules CD4 and CD8. CD4+ T cells or T helper (Th) cells have low cytotoxic activity and provide help by activating and modulating other immune cells to initiate the body's response to invading microorganisms. CD8+ T cells, on the other hand, are referred to as T cytotoxic (Tc) cells and are known to destroy/kill cells that have been infected with foreign invading microorganisms. Both CD4+ and CD8+ T cells are important in autoimmunity, asthma, and allergic responses as well as in tumor immunity. During TCR activation in a particular cytokine milieu, naïve CD4+ T cells and CD8+ T cells may differentiate into one of several lineages of Th or Tc, including Th1/Tc1, Th2/Tc2, Th9/Tc9, Th17/Tc17, Th22/Tc22, and iTreg (induced regulatory T cells, T regulatory cells induced from CD25− cells), as defined by their pattern of cytokine production and function (Fig. 2) (325). How these variations may relate to differences in response, survival, and persistence of the lymphocyte subsets under oxidative stress is dictated by innate differences among cytokines and signaling requirements for T-cell development, the networks of transcription factors involved in T-cell differentiation, and the epigenetic regulation of key T-cell cytokines.
III. T-Cell Subsets and Susceptibility to Oxidative Stress
ROS are critical across a broad spectrum of cellular processes, including signaling, tumor progression, and innate immunity. However, the role of ROS in mammalian adaptive immune system development and function remains largely unknown. A recent study demonstrated that thymus-specific elevation of mitochondrial O2•− disrupts normal T-cell development and impairs the function of the mammalian adaptive immune system (40). Emerging evidence reveals that the differentiation state of lymphocytes largely determines their fate in terms of function and persistence. Although several studies describe the functional consequences of oxygen radical-related immuneregulation, relatively little is known about the sensitivity of individual lymphocyte subsets to oxidative stress and how this process affects disease progression. The susceptibility of T cell subsets to oxidative stress is discussed below.
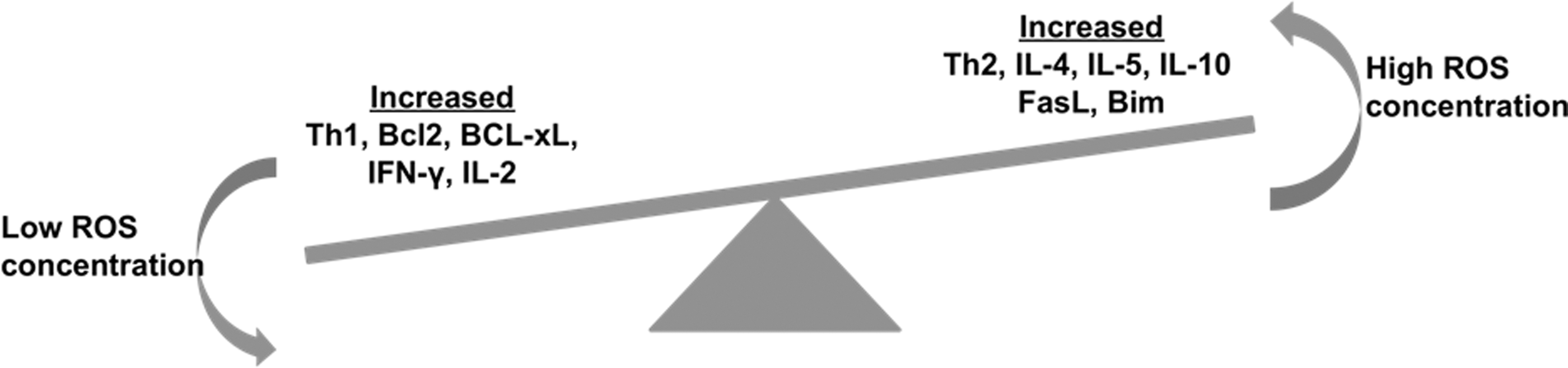
In an adaptive immune response, T cells recruit and activate B cells, CD8+ T cells, macrophages, mast cells, neutrophils, eosinophils, and basophils. In the presence of differentiating signals, naïve CD4+ (Th) and CD8+ (Tc) cells could exhibit either of the known major lineages, namely Th1/Tc1, Th2/Tc2, Th9/Tc9, Th17/Tc17, Th22/Tc22, and iTreg (Fig. 2) (324). These T-cell subsets are marked by differential cytokine production and cellular distribution. They also have the ability to switch from one lineage to another under certain inflammatory conditions. Taken together, T cells are therefore described as plastic (209). This T-cell plasticity may be affected by an oxidative microenvironment, thereby shifting the normal immune response. A recent study showed that the oxidative microenvironment exerts an opposing effect on cytokine secretion by Th1 compared to Th2 cells (77). In this study, in vitro derived Th1 and Th2 clones or T cells derived from autoimmune thyroiditis were used to examine the ability of Th1 or Th2 cells to expand and produce cytokines in response to oxidative stress. Results showed that low doses of hydrogen peroxide (H2O2) reduce the interferon-γ (IFN-γ) production of activated Th1 clones and increase IL-4 secretion by activated Th2 clones (Fig. 3). Importantly, another study has shown that mitochondrial ROS can control T-cell activation by regulating IL-2 and IL-4 expression (129). Kaminski et al. (129) report that an oxidative signal originating from the mitochondrial respiratory complex I regulates T-cell activation-induced expression of the cytokines IL-2 and IL-4. Using a complex I inhibitor or small interfering RNA (siRNA)-mediated downregulation of the complex I chaperone NDUFAF1 (NADH dehydrogenase-1 alpha-subcomplex subunit), they demonstrated that TCR-induced ROS production by complex I is crucial for activation-induced IL-2 and IL-4 expression in resting and preactivated human T cells. Moreover, using T cells isolated from patients with atopic dermatitis, these authors suggest that inhibition of complex I-mediated ROS generation blocks disease-associated spontaneous hyperexpression and TCR-induced expression of IL-4. Thus, oxidative stress plays an important role in the pathogenesis of allergic respiratory diseases and can upregulate Th2-driven inflammation, thereby increasing disease severity, bronchial hyper-responsiveness, and airway remodeling. Similarly, a role of superoxide in modulating Th17 and Th1 T cell responses has also been documented (286). This study showed that T-cell polarization was altered when macrophage and T cell superoxide production involving nicotinamide adenine dinucleotide phosphate oxidase (NADPH) oxidase (NOX) was inhibited. A comparison of the cytokine profile after stimulation with immobilized anti-CD3 and anti-CD28 T cells from NOX-deficient mice showed a skewed Th17 phenotype, whereas T cells from NOX-intact mice exhibited the Th1 phenotype. Similar results were observed in vivo where NOX-deficient NOD mice with a Th17 phenotype exhibited concomitant susceptibility to experimental allergic encephalomyelitis (EAE) and significant protection against type 1 diabetes.
Emerging evidence also indicates that the T-cell differentiation state determines T-cell effectiveness in responding to infection and tumor. Determining the differentiation states to characterize effective T cells is important for designing the vaccination protocols of immunotherapy, which primarily target antigen-specific T-cell activation and expansion. The T-cell subsets could be defined by the expression of a set of cell surface molecules, as depicted in Table 1 (248). The difference in phenotype expression is primarily an outcome of the activation status of these T cells, reflecting their ability to secrete cytokines and kill target cells. In the widely accepted classification scheme based on expression of cell surface molecules, central memory T cells (TCM) are antigen-experienced cells that constitutively express CD62L and CCR7, two surface molecules necessary for cellular extravasations in high endothelial venules and migration to the T-cell zones of the peripheral lymph nodes. In contrast, effector memory T cells (TEM) are antigen-experienced T cells that have significantly downregulated these markers, and hence have a propensity to populate peripheral tissues, such as the liver and lung, as well as inflammatory sites. Other important issues with regard to T-cell subsets of varying phenotype and function are their maintenance and the effect of activation-induced cell death (AICD) after re-exposure to an antigen. The extent of cell death of effectors with the memory phenotype may influence the size of the eventual memory T-cell pool. In addition, the ability of T cells to persist in conditions of oxidative stress, in either an infectious disease state or a tumor microenvironment, determines which pool of T cells persists under these conditions.
The phenotypic expressions or functional attributes are indicated as low (+), intermediate (++), and high (+++).
RA, rheumatoid arthritis; TCM, central memory T cells; TEM, effector memory T cells; Teff, effector T; Treg, regulatory T cell.
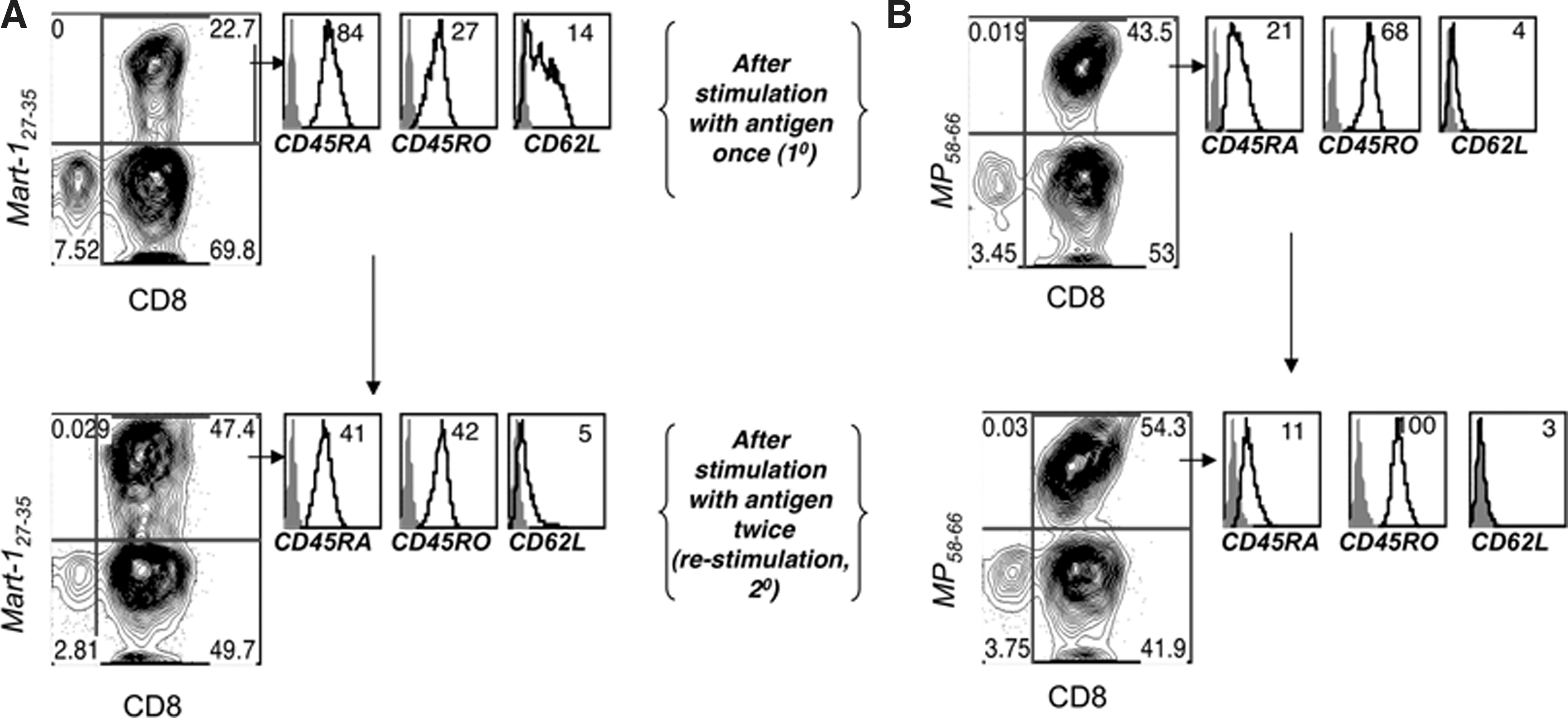
Antigen-specific human CD8+ cytotoxic T lymphocytes (CTLs) with the heterogeneous phenotype (as discussed above) could also be programmed in response to the strength and duration of TCR stimulation. While antigen-mediated repetitive TCR stimulation has been shown to enhance the vaccine efficacy (prime/boost strategies) by increasing the CTL number and function (179), some recent studies have questioned this view (18, 26, 94). In our laboratory, we have characterized the effect of antigen restimulation on T-cell fate in a melanoma epitope MART-127–35-specific self- and influenza epitope MP58–66-specific nonself-reactive CTLs raised from peripheral blood of HLA-A2+ healthy donors as described earlier (183 –185). CTLs expanded from T-cell precursors by a single round of stimulation (primary, 1°) or two rounds (secondary, 2°) with cognate peptide-pulsed autologous dendritic cells were compared for T-cell function and death upon restimulation with cognate peptide-loaded surrogate antigen-presenting cells (APCs), T2 cells. As shown in Figure 4, 1° MART-127–35 and MP58–66 CTLs exhibited less translocation of phosphatidylserine (PS) to the outer layer of the CTL membrane than the corresponding 2° CTLs, as measured by annexin V staining. This PS exposure represents an early hallmark in detecting cells undergoing AICD. The data in Figure 4 show that CTLs that encountered antigen once were less sensitive to TCR restimulation-induced cell death as compared to CTLs that encountered antigen twice. This shows that the T cells are intrinsically modulated after each antigen encounter (and similarly by antigen dose, duration of antigen encounter, or cytokines in their microenvironment) that could affect their persistence or function and thus the immune outcome.

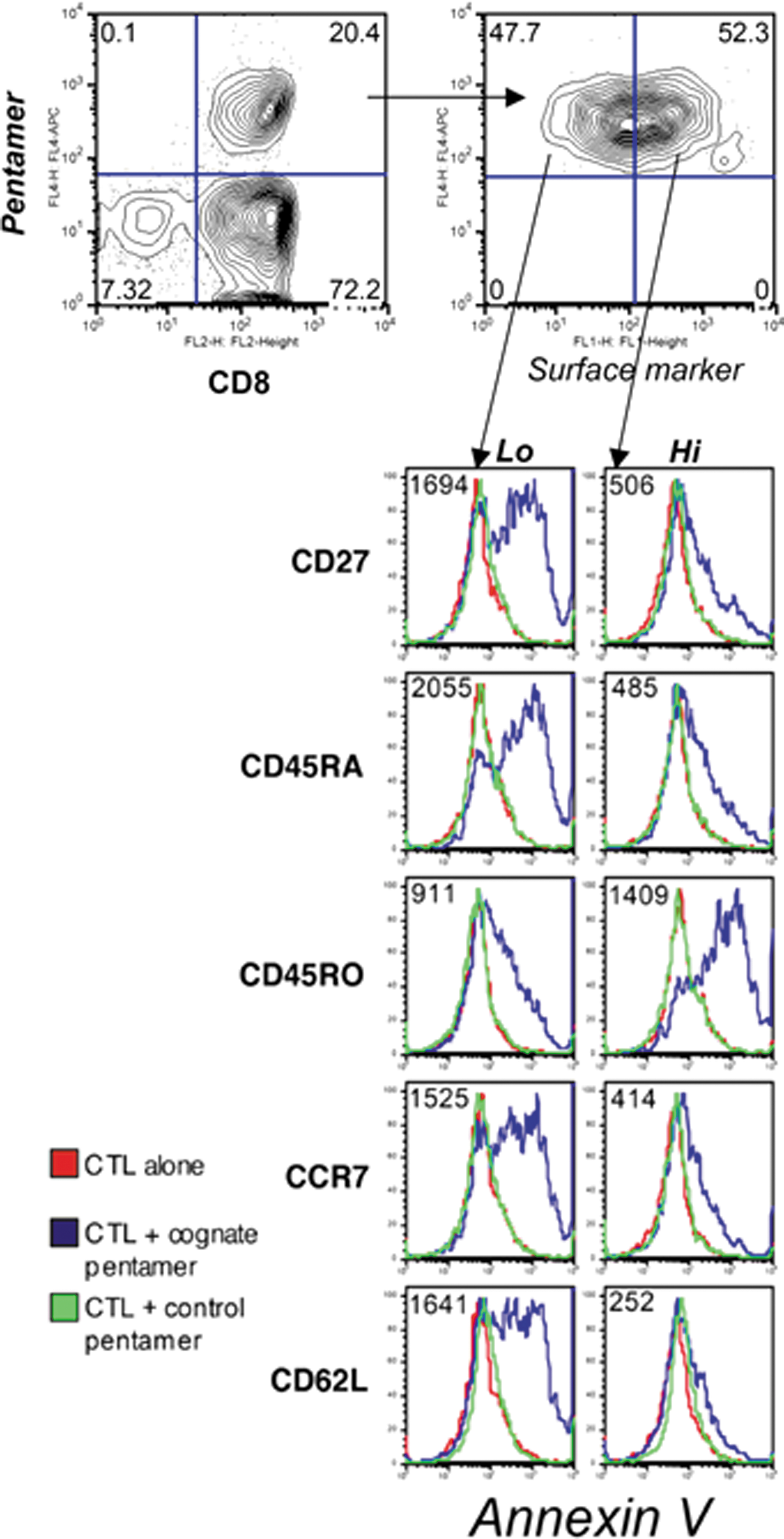
Furthermore, to ascertain contributing factors that would contribute to increased sensitivity to TCR-mediated cell death in 2° CTLs as opposed to 1° CTLs, we examined the expression of various cell surface markers. A representative example is shown in Figure 5. There was an increase in the percentage of antigen-specific CTLs in the 2° CTLs when compared to the 1° CTLs (upper right quadrant in dot plots). MART-127–35-specific CTLs were tracked by using an MHC class I tetramer reagent, which revealed an increase from 23% to 47%, whereas MP58–66 specific CTLs increased from 44% to 54%. Notably, the phenotype concomitantly drifted toward a TEM-like phenotype, with the loss of CD62L, CD45RA, and CD27 levels and the gain of CD45RO expression. As we have reported earlier (185), the nonself influenza epitope-specific CTLs exhibited a more TEM-like phenotype regardless of the number of antigen stimulations. Thus, while a distinct decrease in CD62L and CD27 expression was observed in MART-127–35-specific CTLs, only a slight decrease in already low levels of expression was noticed in MP58–66 specific 2° CTLs when compared to the 1° CTLs. Nevertheless, antigen restimulation significantly decreased the expression of the naïve cell surface marker CD45RA and increased the expression of the memory marker CD45RO on both MART-127–35- and MP58–66-specific CTLs. Since evidence exists for a role of intracellular thiols in ROS production and of cell surface thiol level in T cells' ability to secrete ROS, we further evaluated whether differences in cell surface phenotypes (thereby reflecting qualitatively distinct T-cell subsets) were correlated with cognate antigen-induced cell death. We characterized the difference in TCR-induced annexin V expression (a marker of early apoptosis) in the CTL population with heterogeneous cell surface expression patterns of markers implicated in defining TCM- versus TEM-like subsets. Antigen-specific CTLs stimulated for 4 h with a cognate or control epitope were stained, in parallel, for a panel of cell surface markers and gated for high or low/negative expression for each of these markers and then evaluated for annexin V expression levels. The CTLs exhibiting a TEM-like phenotype (CD27loCD62LloCCR7loCD45ROhiCD45RAlo) were preferentially sensitive to AICD (stained brighter for annexin V), compared with CTLs with a TCM-like phenotype (CD27hiCD62LhiCCR7hiCD45ROloCD45RAhi) (Fig. 6). Thus, antigen-specific CTLs with a TEM-like phenotype preferentially undergo TCR-mediated AICD compared to CTLs with a TCM-like phenotype. The increased sensitivity of TEM-like T cells to TCR-induced AICD could also be correlated to reduced levels of thiols in CD45RO+ T cells as compared to CD45RA+ T cells, as previously shown in our laboratory (184) (Fig. 6).
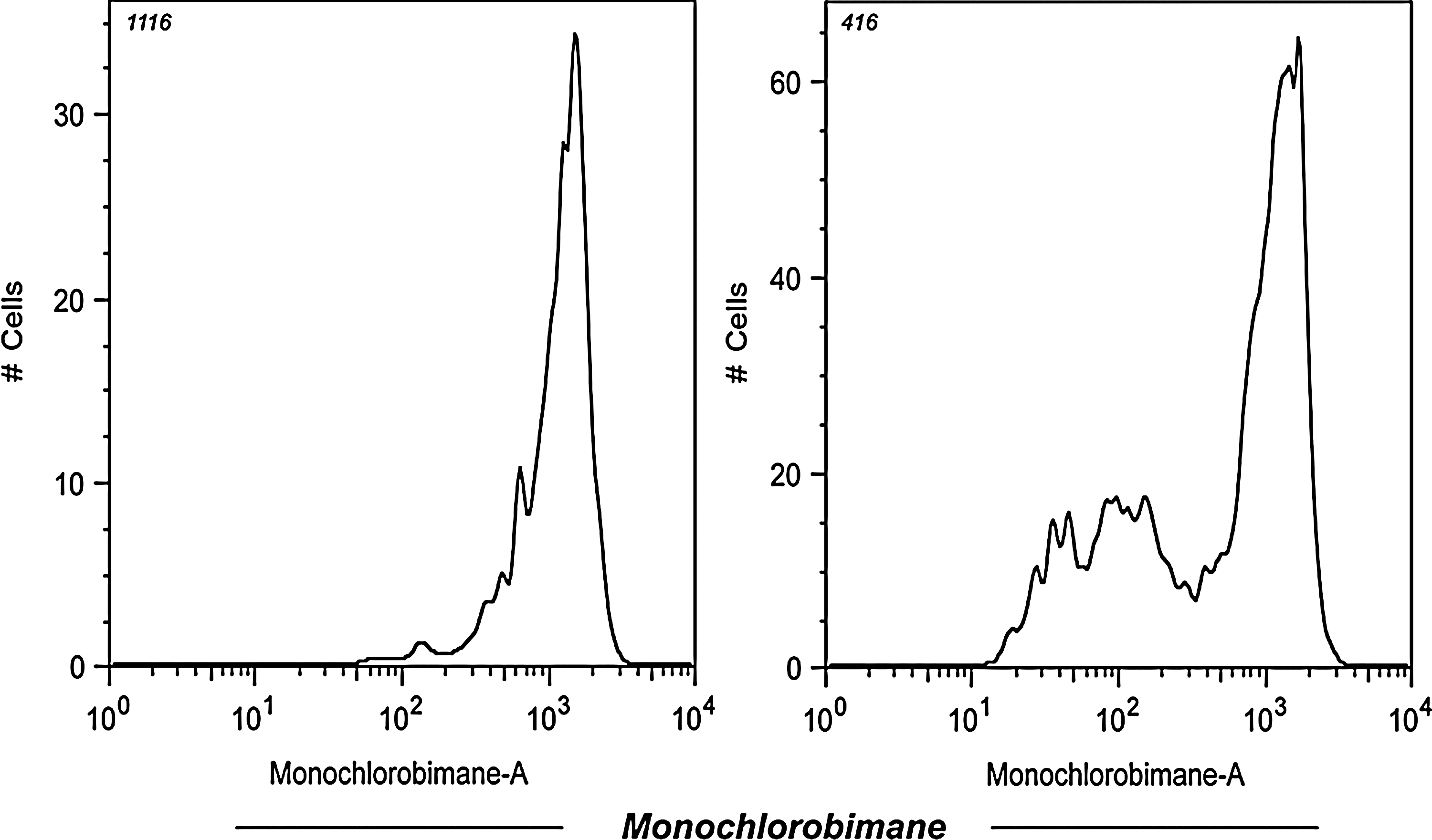
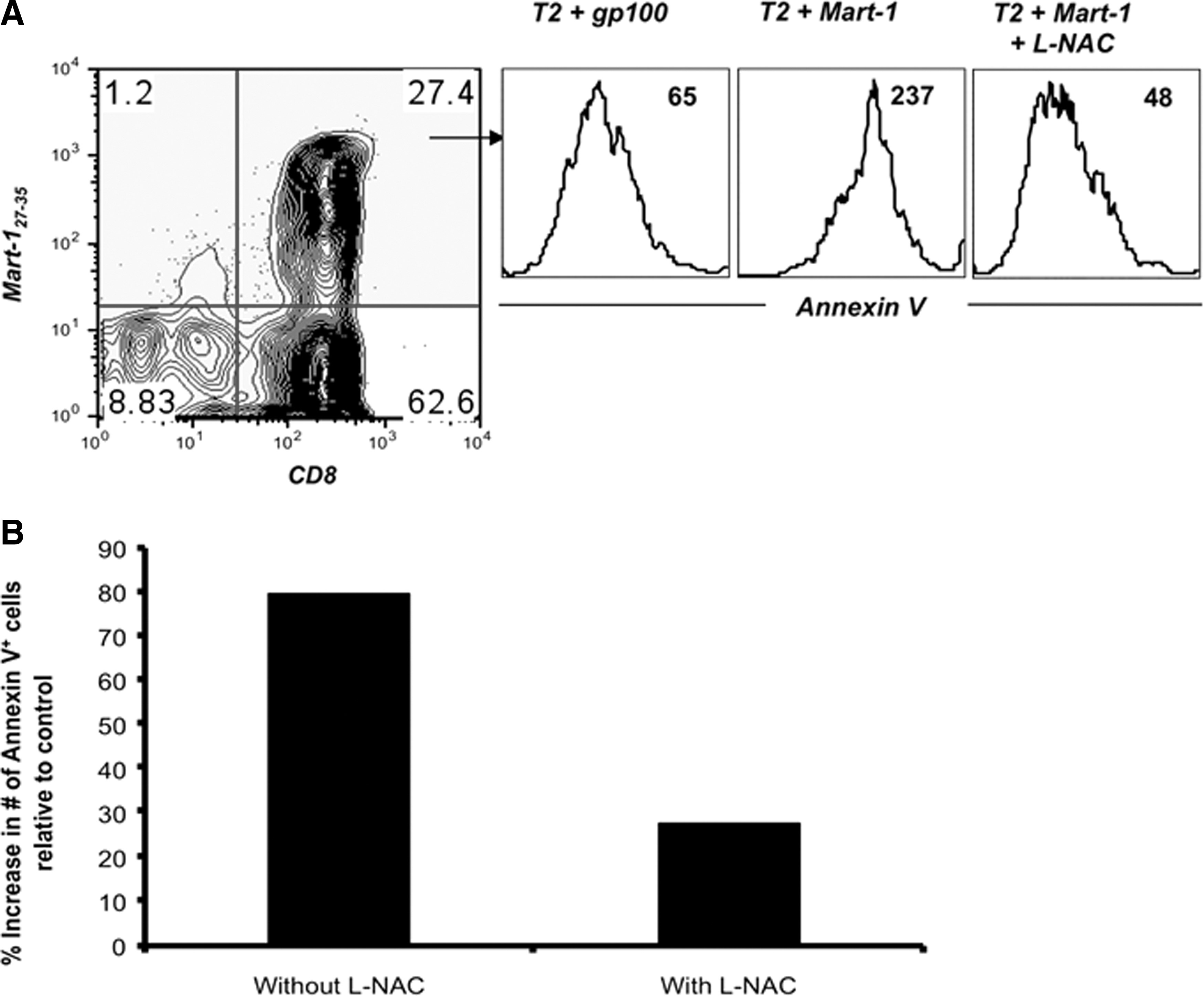
Earlier studies have also shown that human peripheral blood mononuclear cells (PBMCs) stimulated with either HLA-A2-restricted influenza peptide or nonspecific receptor cross-linking, followed by treatment with micromolar (μM) concentrations of H2O2, produce reduced amounts of cytokines (172). This reduction in Th1 cytokines was observed in the memory/effector (CD45RO+) T-cell subset and correlated with a block in nuclear factor kappa B (NFκB) activation. Takahashi et al.(277) have shown that the sensitivity of T-cell subsets of unstimulated human PBMCs to cell death was further investigated by inducing the T cells with low doses of H2O2. This study demonstrated that TEM (CCR7−CD45RA−) cells were particularly sensitive to low doses of H2O2, whereas TCM (CCR7+CD45RA−) are significantly less sensitive (277). Time–kinetic experiments, in which the mitochondrial membrane potential and caspase 3 activities were analyzed, suggested that the mitochondrial pathway is the primary cell death pathway for CD45RO+ T cells when exposed to low levels of H2O2. However, in our laboratory, we reasoned that for an oxidative agent, such as H2O2, to differentially induce cell death, either reduced or oxidized surface molecules must regulate susceptibility to H2O2-mediated apoptosis. Because recent studies have implicated reduced thiols (cysteine–SH) in the function of individual cell surface proteins (81, 245), we evaluated the level of cell surface thiols (cs-SH) on CD45RO+ and CD45RA+ T-cell subsets using a fluorochrome-conjugated maleimide dye, as previously described (245). Our data suggest that CD8+ T cells with a CD45RA+ phenotype express more cs-SH as compared to the T-cell subset with a CD45RO+ phenotype (186). It has also been documented that the overall cs-SH content on cell surface molecules could be correlated to the level of intracellular glutathione (iGSH) (246). Measuring iGSH on CD8+ T cells using the monochlorobimane-staining method (75) revealed higher expression of this key antioxidant molecule in a naïve CD45RAhigh T-cell subset as compared to the antigen-experienced CD45RAlow T-cell subsets (Fig. 7). This finding accords with our data that show that T cells lose thiol expression after proliferation on repeated TCR stimulation. Recent studies have implicated that the levels of cs-SH can be manipulated in vitro by altering the levels of intracellular iGSH or γ-glutamylcysteinylglycine (187). Intracellular GSH is the most prevalent intracellular thiol ubiquitous to all cell types whose function is to maintain the cellular redox state. Other studies have also suggested that a lower capacity to produce ROS is associated with an increased number of reduced thiol groups (–SH) on T-cell membrane surfaces (186). Artificially increasing the number of reduced thiols on T cells either by culturing with reducing agents, such as β–mercaptoethanol (309), or by using N-acetylcysteine (L-NAC), a thiol antioxidant and precursor of GSH, lowered the threshold for T-cell reactivity and enhanced proliferative responses in vitro. Experiments in our laboratory have shown that pretreatment of both tumor epitope-specific primary and TCR-transduced T cells with the thiol donor L-NAC increased cellular thiols and rescued T cells from TCR stimulation-mediated AICD without impairing their functional capacity (Fig. 8). These results suggest that T-cell expansion upon cognate antigen encounter affects the cell surface marker expression, replicative history, and the CTL quality by decreasing its antioxidant capacity.
In addition, different T-cell phenotypes have differential susceptibility to oxidative stress-induced apoptosis, and this susceptibility is associated with cell surface thiol expression and iGSH. The data discussed above suggest that increased levels of reduced thiol groups and iGSH in a T-cell subset could be responsible for its increased ability to persist in a tumor-induced oxidative stress microenvironment. Our laboratory is currently exploring whether this differential susceptibility to oxidative stress between T-cell subsets correlates with differences in expression levels of genes involved in oxidative stress/ROS metabolism or can be modulated by factors that play an important role in T-cell development and maintenance (such as cytokines, APC, antigen dose, and Toll-like receptors). Our recent data show that IL-15 increases the level of cell surface thiols and the overall antioxidant capacity of CD8+ T cells (138). We also observed that CD8+ T cells cultured in IL-15 result in an increased mitochondrial mass as compared to T cells cultured in IL-2 (Fig. 9A). The increase in mitochondrial mass signifies a higher mitochondrial copy number in the T cells when cultured in the presence of IL-15. Since the mitochondrion is a key regulator of the metabolic activity of the cell and is an important organelle in both production and degradation of free radicals, an increase in higher mitochondrial mass supports our published data that T cells cultured in the presence of IL-15 showed higher ROS and RNS secretion (138). Since mitochondria are produced from the transcription and translation of genes both in the nuclear genome and in the mitochondrial genome, we further evaluated the genes encoded by the mitochondrial genome that are mostly involved in the electron transport chain mitochondrial cytochrome B (MT-CYB), mitochondrial cyclooxygenase 2 (MT-COX2); NDUFA; (NADH dehydrogenase [ubiquinone]-1 alpha-subcomplex subunit). Our data show that cells cultured in the presence of IL-15 have more expression of these mitochondrion-associated genes (Fig. 9B) (24). If other cytokines that also influence the T-cell phenotype also modulate mitochondrial biogenesis is currently under investigation in our laboratory. Our preliminary data evaluating the effect of IL-12-, IL-21-, and IL-17-secreting T cells also show that the antioxidant capacity of T cells is modulated in the presence of these cytokines (unpublished data). Thus, it is evident that cytokines do have the capacity to modulate the redox status of T cells. Moreover, T cells with a different phenotype have differential susceptibility to oxidative stress based on their redox status. This is further supported by the recent observation that CD8+ memory T cells, but not CD8+ effector T (Teff) cells, possessed substantial mitochondrial spare respiratory capacity (SRC), and SRC is a critical regulator of CD8+ T-cell memory development (285). Mitochondrial SRC is the extra capacity available in cells to produce energy in response to increased stress or work and is associated with cellular survival. Thus, understanding the T-cell phenotype and function should hold importance in modulating a disease state that involves T cells. While increasing the antioxidant capacity by thiol donors prevented AICD, a similar strategy may be used to increase the persistence of T cells or modulate the T-cell phenotype (effector vs. memory) by modulating mitochondrial function. Overall, these results show how cytokines control the T-cell phenotype and bioenergetic stability of T cells, and that regulating T cell mitochondrial metabolism may be key in controlling pathogenic disease states (290).

In addition to Teff cells with different phenotypes, naturally occurring regulatory T cells (Tregs) with a strong immunosuppressive capacity and known to play a critical role in the T-cell homeostasis exhibit reduced sensitivity to oxidative stress-induced cell death while maintaining their suppressive function (279, 293). Human Tregs have several defense mechanisms to counteract oxidative stress. Tregs express high levels of cell surface thiols, which are important reducing agents, as well as increased intracellular antioxidative capacity (195). In addition, Tregs express and secrete high levels of thioredoxin-1 (TRX-1), a major antioxidative molecule (196) that is required for cell surface thiol expression and decreases the susceptibility of Tregs to oxidative stress-induced apoptosis. This enhanced antioxidative capacity of Tregs possibly serves as a feedback inhibition mechanism during inflammation and prevents uncontrolled immune reactions by favoring survival of suppressor rather than effector cells. Moreover, Tregs have been shown to interfere with GSH metabolism in dendritic cells and T cells (314), thereby allowing Tregs to survive oxidative stress signals by diminishing GSH synthesis via decreased expression of γ-glutamylcysteine synthetase, the rate-limiting enzyme for GSH synthesis. Tregs also consume extracellular cysteine and partition it more proficiently to the oxidation product, whereas Teff cells divert more of the cysteine pool toward protein and GSH synthesis (314). Initially, a higher concentration of GSH is seen in the nucleus during cell proliferation; later, GSH is redistributed to the cytoplasm. Tregs block the redistribution of GSH in Teff cells. Together, these data suggest that Tregs can modulate sulfur-based redox metabolism, and as a result of this modulation, T-cell activation and proliferation are suppressed. Recently, the importance of macrophage-produced ROS in inducing Tregs has also been highlighted (149). Based on the results of this study, the induction and immunosuppressive function of Tregs are dependent on ROS, and ROS deficiency may lead to decreased Treg induction and hampered T-cell suppression. This study demonstrates that macrophages significantly express both gp91phox and p47phox proteins, more than DCs, and are better in producing ROS and inducing Tregs. Coculturing of CD4+CD25− (Th cells) cells with macrophages and anti-CD3/CD28 demonstrated induction of Tregs (increase in the number of iTregs- CD4+CD25+FoxP3+), which was attributed to increased ROS secretion, since coculture of the same cells in the presence of apocynin (a NOX inhibitor) lowered the number of iTregs and their proliferation. Thus, these findings together highlight the importance of the redox-regulating molecules in skewing the T-cell subset, which in turn could result in modulating the immune status of an individual. In the following section, we further discuss important redox-regulating molecules that could have implications in T-cell response.
IV. T Cell and Redox Regulators
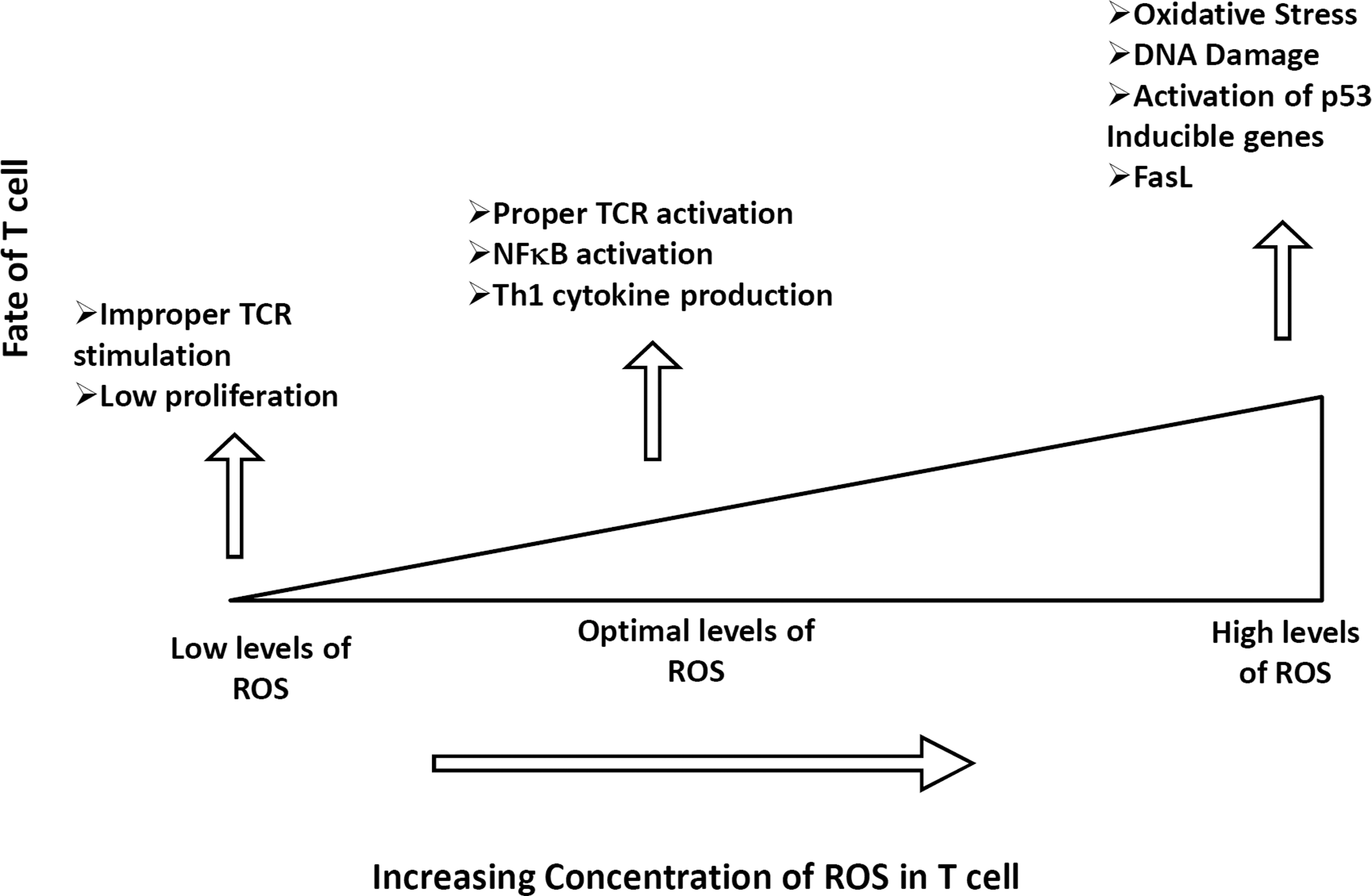
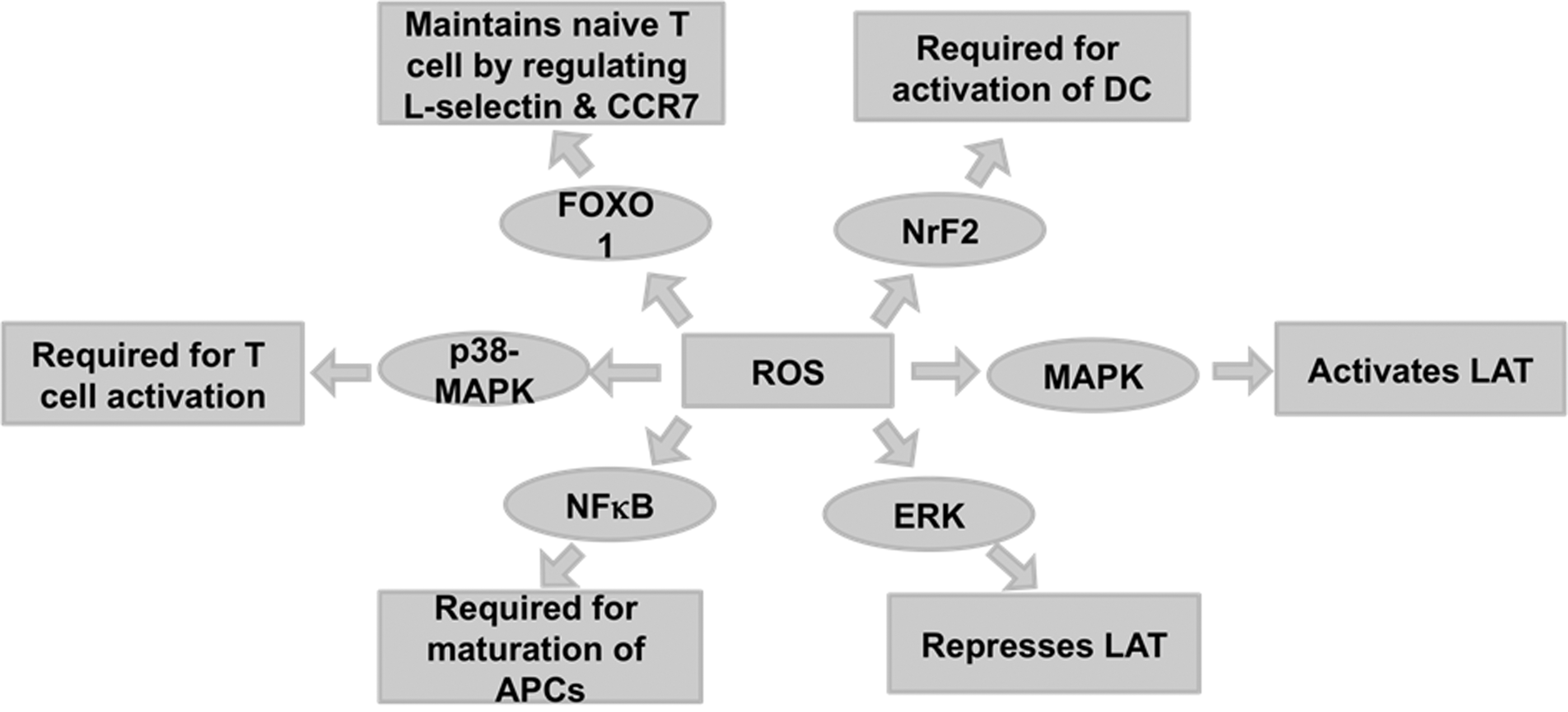
It is well known that TCR activation triggers a number of signaling cascades. Interestingly, an early event in TCR activation activates lymphocyte protein-tyrosine kinase (Lck) by the TCR/CD3 complex. This is followed by recruitment of ζ-chain-associated protein kinase (Zap-70), which further amplifies the response and leads to the activation of multiple pathways, including ERK, mitogen-activated protein kinase (MAPK), and c-Jun N-terminal kinase (JNK). These pathways ultimately determine the cell fate for differentiation and proliferation (36, 160). In addition, the cellular concentration of ROS can also lead to selective activation of several transcription factors such as NFκB, p53, and AP-1. These transcription factors determine the fate of cells, survival versus death. The following section focuses briefly on the roles of reactive molecules in modulation/regulation of the various signaling molecules (Fig. 10).
A. Transcription factors
1. Nuclear factor κB
NFκB is a dimeric transcription factor that is involved in the vital signaling pathway for the activation of proinflammatory cytokines, chemokines, cellular proliferation, and mediators of apoptosis (284). NFκB is also important for the maturation and survival of T lymphocytes, as they are activated upon TCR activation (130). Several studies show that the redox state of a cell can regulate NFκB, which can in turn affect the generation of a robust T-cell immune response (273). NFκB is also shown to be constitutively expressed in acute myeloid leukemia (AML) cells, suggesting that NFκB acts as an antiapoptotic mediator in AML cells. Therefore, when NFκB activation is blocked with pharmacological agents, AML cells undergo targeted apoptosis (76). A study in cardiac dysfunction in type II diabetes demonstrated that enhanced activity of NFκB leads to increased ROS, ONOO−, gp91phox, and NOX1 expression. Therefore, these studies demonstrate that ROS-mediated activation of transcription factor NFκB is a central regulator of T-cell immunity, inflammation, and cell survival.
2. p53. p53, one of the most important tumor suppressor proteins, is vital for protecting cells in oxidative stress by maintaining genomic integrity
DNA damage is the most common outcome in cells after oxidative stress. p53 arrests proliferation of such cells and triggers signals to undergo apoptosis to overcome DNA damage (132, 180, 225). However, studies reveal that p53 can protect against DNA damage from ROS-induced oxidation by upregulating several antioxidant genes such as glutathione peroxidase 1 (GPX1) (243). This study illustrates that p53−/−-deficient mice develop lymphomas by 6 months of age, whereas the p53−/− mice supplemented with the antioxidant L-NAC diet were significantly protected from developing lymphomas. While a direct crosstalk between p53 signaling and ROS production is not clearly understood, it has been shown that T cells require low concentrations of ROS for proper activation and signaling. However, accumulating ROS may lead to activation of p53 and p53-inducible genes, leading to apoptosis (225). Additionally, high levels of ROS may result in the phosphorylation and stabilization of p53 and subsequent activation of apoptotic signals as seen in other biological systems and diseases (283). In vitro and in vivo studies using p53−/− mice suggest that p53 is important in regulating apoptotic signals in T cells (266). Based on recent evidence, p53 is a key regulator of T-cell maturation and of the differentiation of α/β T cells in the thymus (210).
Moreover, p53 plays a significant role in controlling the cell cycle at the mitotic phase of antigen-specific proliferating T cells (17). Interestingly, infiltration of immune cells, specifically the tumor-infiltrating T cells (TILs), Tregs, and tumor-associated macrophages, was associated with p53 mutations in ovarian cancer patients (259). Based on recent DNA microarray studies, Desaint et al. (60) showed that 42 differentially expressed genes were identified in cells in response to H2O2 treatment. Interestingly, 17 of the 42 genes (∼40%) were targets of p53 (60), demonstrating a role for oxidative stress regulation in p53-mediated immune responses. Polyak et al. have shown that p53 can induce the expression of different genes such as proline oxidase, which upregulates ROS production in cancer cells (225, 239). The tumor suppresor p53 has also been shown to regulate mitochondrial ROS production by altering the expression of the mitochondrial antioxidant enzyme, manganese superoxide dismutase (MnSOD) (109, 240). Therefore, an impaired communication between the mitochondria, p53, and the nucleus is implicated in several disease conditions. Taken together, p53 is important in regulating T-cell maturation and proliferation, but the p53-induced expression of mitochondrial ROS in primary T cells warrants further research.
3. Forkhead transcription factors of class O
Forkhead transcription factors are well known for their role in maintaining immune system function (39, 212). Recent data have highlighted the role of the forkhead transcription factors of class O (FoxO) in oxidative stress and in differentially regulating persistence of T-cell subsets (49). This study reports that the Mst1-FoxO-signaling pathway is important in maintaining the survival of naïve T cells by increasing the expression of downstream antioxidant molecules, such as SOD2 and catalase. As a result of the increase in FoxO-mediated expression of SOD2 and catalase, T cells are resistant to oxidative-stress-induced apoptosis.
Riou et al. also demonstrated that survival of ex vivo isolated TCM is increased, because they are more resistant to both spontaneous and Fas-induced apoptosis than cells with the TEM phenotype, resulting in their increased persistence in vitro (238). Moreover, this study reports that ex vivo TCM express increased levels of the transcriptionally inactive form of FoxO3a (phosphorylated FoxO3a) and decreased levels of the downstream proapoptotic molecule, Bim. Recent studies have also demonstrated that TCM are less sensitive to H2O2 in comparison to TEM (277). Therefore, these results indicate a role of FoxO3a in redox regulation of T cells and protection from apoptosis. This type of protective role of FoxO3a is also implicated during human immunodeficiency virus (HIV) infection, where FoxO3a regulates the survival of central memory CD4+ T cells during HIV infection (291). Furthermore, FoxO1 and FoxO3a have been shown to regulate the transcription of p27Kip1, Bim, and L-selectin in response to IL-2 in murine and human T lymphocytes (72, 270). Interestingly, Kerdiles et al. have demonstrated that FoxO1 regulates the development of functional Tregs, and that FoxO1 is required for survival and homing of naïve T cells to secondary lymphoid organs (139).
In a recent study, FoxOs were reported to be critical in regulating cell cycle, in inhibition to apoptosis, and mediators of resistance to physiologic oxidative stress in hematopoietic stem cells (HSCs) (282). This is an important finding, since the results from this study show that there was a marked increase of ROS in FoxO-deficient HSCs compared to wild-type (WT) HSCs, which correlates with changes in the expression of ROS-regulating genes. The importance of the FoxO-signaling pathway in cellular tolerance to increased intracellular ROS and maintenance of peripheral naïve T-cell homeostasis is also substantiated in other studies (49). Thus, FoxO proteins play an essential role in regulating physiologic oxidative stress, and thereby promote enhanced survival of myeloid and lymphoid cells in response to ROS.
4. Nuclear factor erythroid-2-related factor 2
The nuclear factor erythroid-2-related factor 2 (Nrf2) transcription factor regulates the basal and inducible expression of a wide array of antioxidant genes. In a recent study, regulation of the cellular redox level and Th1/Th2 balance was shown to protect against the development of pulmonary fibrosis in a preclinical model of pulmonary fibrosis where C57BL/6 mice and Nrf2-deficient mice were administered bleomycin intratracheally (140). Similarly, the absence of Nrf2 has been shown to exacerbate experimental autoimmune encephalomyelitis, suggesting that activated Nrf2 attenuates autoimmunity and proinflammatory conditions (126). Comparisons of disease severity in WT and Nrf2 knockout mice after immunization with myelin oligodendrocyte glycoprotein (MOG) 35–55 revealed that the clinical progression of the disease is marked by rapid onset and increased severity in the Nrf2 knockout mice. In addition, in the Nrf2-deficient mice, increased immune cell infiltration and glial cell activation in the spine were observed in conjunction with increased levels of expression of inflammatory enzymes (inducible NO synthase [iNOS], phox-47, gp91-phox, and phox-67), cytokines (IFN-γ, IL1-β, tumor necrosis factor [TNF]-α, and IL-12), and chemokines (B lymphocyte chemoattractant [BLC] and monokine induced by IFN-γ [MIG]). These results further substantiate that Nrf2 can modulate an autoimmune neuroinflammatory response by regulating proinflammatory enzymes, the pro-oxidant enzymes.
Nrf2 can also modulate the T-cell response by regulating oxidative stress-induced activation of dendritic cells. A recent study suggested that disruption of the transcription factor Nrf2 in dendritic cells leads to increased oxidative stress, and in response to allergic, airborne pollutants, a Th2-like immune response is elicited in these Nrf2-deficient dendritic cells (305). Nrf2 deficiency has been further implicated in the decline of Th1 immune response in the course of aging (141). Moreover, the observed decrease in Th1 immunity in aged mice could be restored by administering either an Nrf2 agonist, sulforaphane, or a thiol precursor, L-NAC. Mechanistic studies using Nrf2-deficient T cells suggest that Nrf2 deficiency enhances the sensitivity to Fas-mediated apoptosis by regulating the intracellular levels of GSH, a major intracellular antioxidant (194). Taken together, these studies suggest that Nrf2 regulates T-cell immunity by fine-tuning the redox equilibrium.
B. Mitogen-activated protein kinases
1. c-Jun N-terminal kinase
Recent research has suggested that ROS and RNS act as signaling molecules in the activation of JNK, commonly known as stress-activated protein kinase, leading to apoptosis (262). While it is known that CD3 and CD28 co-stimulation is required for JNK activation, IL-2 production (64), and IL-2 gene transcription in Jurkat cells (human CD4+ T cell line) (184), recent studies have demonstrated that JNK signaling is important for Teff cell function, but not for naïve T-cell activation (64). Furthermore, reports by Dong et al. showed that T cells isolated from JNK1 and JNK2 knockout mice can be stimulated to produce IL-2, but they cannot functionally differentiate into Th1 and Th2 lineages (63, 315). Pani et al. also demonstrated that treatment of T cells with the mitogen concanavalin-A (ConA) upregulates ROS and JNK, whereas use of L-NAC (a ROS scavenger) inhibits ConA-stimulated thymocyte proliferation and JNK upregulation (216). Therefore, JNK may play an important role in redox signaling.
Earlier studies from our group have also shown that T cells reactive to melanoma epitope MART-127–35 and influenza matrix protein MP58–66 have increased JNK phosphorylation when reactivated with a cognate epitope (207). Moreover, this upregulation in JNK phosphorylation is inhibited when T cells are pretreated with a superoxide dismutase (SOD) mimetic Mn (III) tetrakis (5,10,15, 20-benzoic acid) porphyrin (MnTBAP). Inhibition of ROS also rescues these antigen-specific T cells from TCR restimulation-induced cell death, suggesting that ROS inhibitors prevent AICD in primary CTLs by blocking JNK activation. Thus, JNK has a crucial role in the signaling cascade leading to T-cell activation and proliferation in response to immunogenic stimuli.
2. Extracellular signal-regulated kinases
It is known that extracellular signal-regulated kinase (ERK) signaling plays an important role in the early phase of naïve T-cell activation and positive selection of T cells (1, 55). Furthermore, MAPK has been identified as a critical regulator of CD95/Fas-mediated apoptosis in T cells (110). CD95/Fas-mediated apoptosis is important in the negative selection of T-cell development and in later stages of T-cell activation when activated T cells are no longer needed and are now triggered to undergo CD95/Fas-mediated AICD. Koike et al. have reported that ERK activation plays a critical role at late stages (after 2 h of activation) of T-cell activation, and that ERK2 has specific functions in the activation, proliferation, and survival of CD8+ T cells (146). As suggested by D'Souza et al., ERK2 is required for proliferation of activated CD8+ T cells without co-stimulation and is responsible for increased T-cell survival (55).
Using a Zap-70-deficient Jurkat T cell line (P116) in their studies, Griffith et al. found that Zap-70 is required for the H2O2-induced activation of ERK in T cells (90). However, they also reported a Zap-70-independent pathway for activation of ERK. TCR activation of T cells has also been shown to activate ERK within 15 min, and moreover, low concentrations of H2O2 may be required for proper ERK activation (61). Thus, low concentrations of ROS may positively regulate ERK activation, and higher concentrations may negatively affect ERK signaling in T cells.
3. p38-MAPK
The p38-MAPK kinase pathway is activated in response to numerous cellular stress stimuli and cytokines. Known for its ability to induce apoptosis, p38-MAPK can regulate the cells' survival signals in response to external stimuli. For example, cellular stress such as DNA damage can elicit a survival signal where p38-MAPK can regulate the G2/M and G1/S cell cycle checkpoints (280). In response to treatment with UV radiation or a DNA-damaging agent (8-MOP), the p38-MAPK pathway was activated in Jurkat T cells, suggesting that p38-MAPK is important for T-cell survival (38). Several studies also show that the p38-MAPK pathway is responsible for differentiation of naïve CD4+ T cells into effector cells. It may also be responsible for Th17 subset differentiation (208). Moreover, it is also required for the production of IFN-γ from CD8+ T cells (237). One study has suggested that T cells infected with Vibrio vulnificus undergo cytotoxic cell death by a p38-mediated production of ROS (143). Jurkat T cells that are exposed to a pathogenic bacterium, V. vulnificus, require NOX, which induces the production of ROS, thereby leading to the death of the infected T cells. This substantiates the role of p38-MAPK in ROS production in infected T cells.
V. Key Molecules in Redox Regulation
To protect against oxidative damage, cells have developed an antioxidant defense mechanism that maintains cellular redox homeostasis. Many antioxidant molecules have been identified to regulate the redox status of a cell and play a major role in regulating immunological functions (Table 2). Under conditions of endogenous or exogenous oxidative stress, the altered expression of these molecules affects cellular function. We briefly introduce these molecules with reference to T cells in the following section and further discuss their role in specific diseases in section VII.
NFκB, nuclear factor kappa B; TCR, T-cell receptor; Treg, regulatory T cell.
A. Antioxidant/redox proteins
1. Superoxide dismutase
SOD may protect cells from oxidative damage by catalyzing the dismutation of two molecules of superoxide anion into water and H2O2. SOD has three known isoforms: SOD1, SOD2, and SOD3. While copper/zinc SOD (Cu/ZnSOD or SOD1) is present in the cytosolic fraction, manganese superoxide dismutase (MnSOD or SOD2) is located in the mitochondrial fraction, and SOD3 is extracellular (101). Based on studies using transgenic mice, mutations in the SOD1 gene have been shown to be associated with the familial form of amyotrophic lateral sclerosis (ALS), suggesting that SOD1 is important in preventing oxidative-stress-associated diseases (121). In contrast, using a tetracycline-inducible system, Zou et al. were able to show that the extracellular form of SOD (SOD3) is important in preventing oxidative-stress-induced diseases and injuries (327). In this section, we will focus on the role of SOD2 in protecting cells from oxidative-stress-induced damage.
SOD2 functions primarily to protect mitochondrial components from superoxide anions, which are liberated as a normal byproduct of respiration. Mitochondrial Complex I and Complex III are estimated to produce superoxide anions from about 1%–5% of oxygen consumed as a consequence of normal respiration. MnSOD is the cell's primary defense mechanism against free radical-mediated damage and is important in regulating oxidative and apoptotic signals (217). Another study has suggested that overexpression of the human MnSOD transgene in hematopoietic progenitor cell line 32D cl3 cells and other cell lines results in stabilization of the mitochondria and reduction in radiation-, TNF-α-, or cytokine withdrawal-induced cell death (70)
Furthermore, based on the results of a study using a T-cell-specific manganese SOD2 conditional knockout mouse, SOD2-KO leads to increased O2•− production, apoptosis, and developmental defects in the T-cell population, resulting in immunodeficiency and susceptibility to the influenza A virus H1N1 infection (40). This phenotype was rescued with mitochondrial-targeted superoxide-scavenging drugs. These findings demonstrate that the loss of regulated mitochondrial superoxide production leads to aberrant T-cell development and function, and further suggests that manipulations of mitochondrial superoxide may significantly alter clinical outcomes resulting from viral infections.
2. Glutathione peroxidase
GPX is an important group of antioxidants responsible for reducing peroxides. Their importance arises from their ability to protect cells from ROS-induced damage to lipids, proteins, and nucleic acids (226). This type of protective effect is seen in vitro and in vivo, where GPX1 is responsible for reduction of ROS production in cells after TCR activation and also protects cells from ROS-induced apoptosis (306). A recent study demonstrated that GPX1-deficient CD4+ T cells produced more intracellular ROS and IL-2 than WT cells. Moreover, the study also showed that the GPX1-deficient CD4+ cells have a greater proliferation rate than the WT cells. In support of the pivotal role of GPX in protecting cells from ROS-induced apoptosis, studies using an 8E5 HIV-infected human T-cell line have suggested that these cells are more susceptible to H2O2-induced apoptosis as a result of catalase and GPX deficiency (306). GPX1-deficient cells exhibit Th1 phenotype when exposed to TGF-β and IL-6, anti-IL-4 antibody, and anti-IFN-γ antibody, therefore suppressing the Th2 and Th17 phenotype of these cytokine-treated cells. Thus, these results show that deletion of GPX1 skews the phenotype of T cells toward the Th1 phenotype by suppressing Th2 subset development. Therefore, GPX1 is important not only for reducing intracellular ROS accumulation but also for regulating Th1 cell proliferation and differentiation.
3. NADPH oxidase
NOX, a membrane-bound enzyme complex made up of six subunits, is a major source of ROS that participates in signal transduction of nonphagocytic cells. Recent studies have demonstrated the important role of NOX in shaping Th responses and as a signaling intermediate to modulate Th17 and Th1 cell responses (286). Upon CD3 and CD28 activation, T cells from NOX-deficient mice were primarily of the Th17 phenotype, whereas NOX-intact cells differentiated into the Th1 phenotype. Corroborating evidence is seen in a study by Purushothaman et al., where mice deficient in the NOX catalytic subunit gp91(phox) demonstrated gp91's role as an important regulator of T-cell function (228).
Briefly, IL-2 withdrawal results in a significantly reduced level of apoptotic cell death of gp91(phox)-deficient T (T−/−) cells as compared to the WT T cells (T+/+). That is, gp91 (phox)-deficient T cells are resistant to apoptosis. Furthermore, activated T−/− cells displayed improved survival after activation by superantigens in vivo, where in vitro activated T−/− cells were adoptively transferred into congenic hosts. Thus, NOX is an important regulator of adaptive immunity. Mechanistic studies have shown that NOX-derived ROS direct Treg-mediated suppression of CD4+ Teff cells, a process that is subject to inhibition by thiol-containing antioxidants, NOX inhibitors, or neutrophil cytosolic factor 1 (Ncf1) (p47phox) -deficient Tregs and Teff (68). Thus, NOX play an important role in T-cell susceptibility to ROS and modulate T-cell function.
4. Catalase
Catalase is an important antioxidant enzyme responsible for conversion of H2O2 to H2O and O2. The antioxidant and protective functions of catalase in T-cell lines (CCR-CEM acute lymphoblastic leukemia [ALL] cell lines) have been previously demonstrated (252). Recently, catalase has been identified as a critical factor for maintaining activated T cells at high density during ex vivo expansion of T cells in adoptive T-cell immunotherapy (168). This study highlighted the importance of cell density in T-cell activation, proliferation, survival, and apoptosis in ex vivo cultures. In addition, the study implicated a role for increased catalase secretion in high-cell-density culture supernatants that were able to rescue oxidative stress-mediated, activated T-cell death. The importance of catalase in protecting T cells from ROS was further substantiated in a recent study where T cells transduced with catalase, using a retroviral vector, enhanced the survival of CD4+ T cells under oxidative stress (11). Taken together, these results show that catalase is an important modulator of T-cell-mediated immunity.
5. Glutathione and cell surface thiol
GSH, a nonprotein thiol, acts as an antioxidant and prevents cellular damage from ROS. The synthesis of GSH in cells may be disrupted during aging and under pathologic conditions such as diabetes mellitus (251) and cystic fibrosis (37). Apoptotic stimuli result in the decrease of cellular GSH, generation of ROS, and RNS, and is important in downstream signaling involving the Fas ligand (75). Maintaining optimal GSH levels in the cellular microenvironment is critical, as its depletion may lead to the progression of certain diseases, including HIV (246) and arthritis (81, 116). The GSH level has been shown to decrease as HIV disease progresses, and low GSH in subjects with advanced HIV disease predicts poor survival and impaired T-cell function. These studies suggest that the decreased production of ROS is associated with an increased number of reduced thiol groups on the T-cell surface, thereby modifying T-cell function in an immune response.
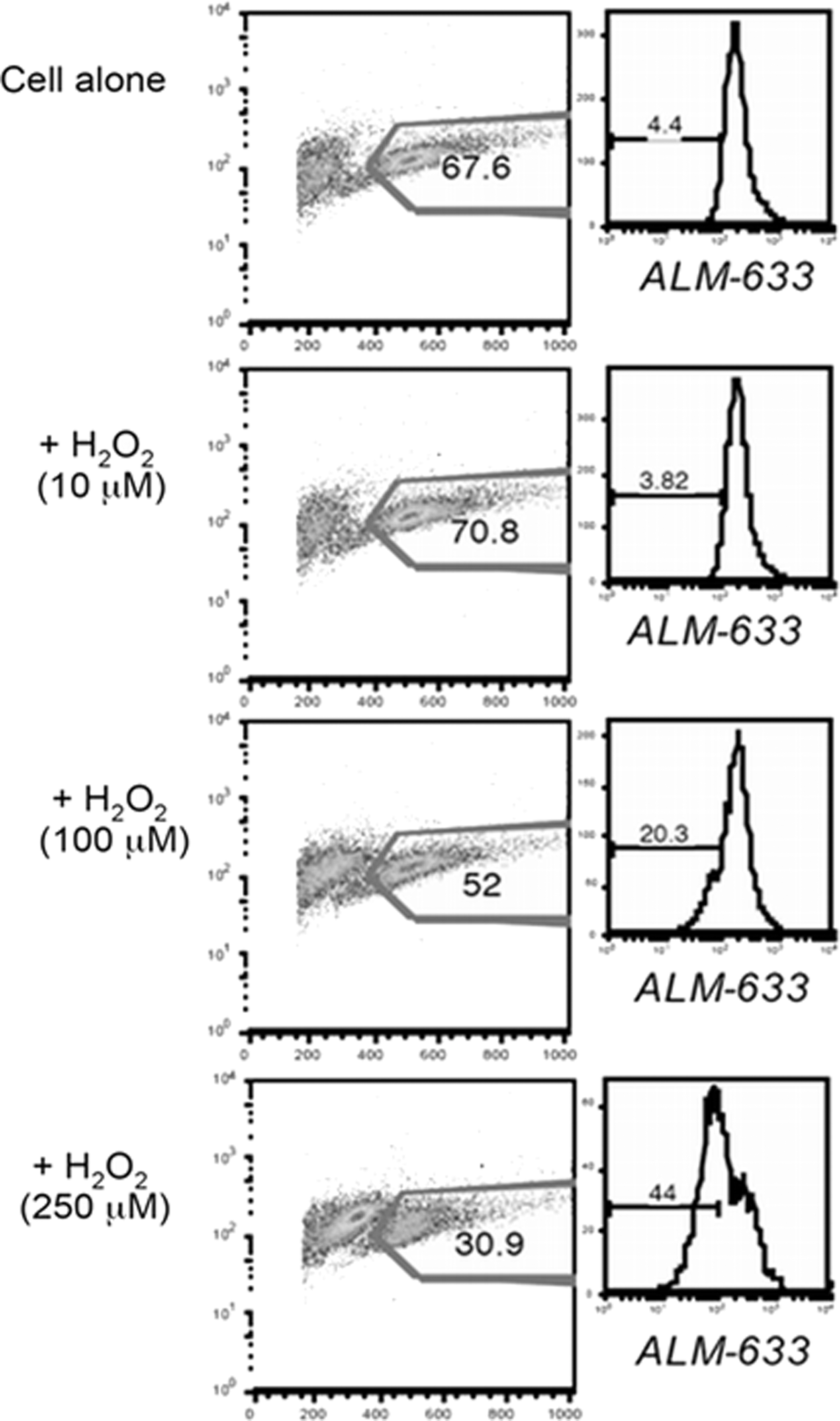
Interestingly, our data show that the TEM subset (known to be more sensitive to AICD or apoptosis) expressed less cs-SH, while the T-cell subset with TCM phenotype (relatively resistant to AICD or apoptosis) expressed more cs-SH (unpublished observation). Furthermore, a decrease in the percentage of T cells with reduced thiols is noticeable after treatment with increasing dose of H2O2 along with a concomitant decrease in the number of viable cells, as seen in the scatter plot (Fig. 11). These data suggest that the high cell surface thiol-bearing cells would survive better in an oxidative microenvironment, and thiol levels on T cells could play an important role in T-cell persistence and immune outcomes.
6. Thioredoxin
TRXs are a large family of proteins with cysteine-containing redox-active centers that are important mediators of scavenging H2O2 (235). TRX has been shown to protect lymphoid cells from apoptosis by its peroxide-scavenging activity (120). In a recent study, 28 children with T-cell acute lymphoblastic leukemia (T-ALL) were evaluated for total lymphocyte count, and the results suggested that a higher lymphocyte count is associated with higher level of TRX expression in T-ALL patients. Moreover, exogenous treatment with TRX increased proliferation of lymphocytes in vitro, suggesting that TRX is important in T-cell proliferation (261). Our recent work shows that CD8+ cells cultured in presence of IL-15 increase ROS and TRX1, therefore increasing T-cell survival (138). Another study illustrated that Tregs produce higher amounts of TRX, which may result in increased tolerance to oxidative stress (196). Therefore, TRX expression in response to oxidative stress is important for T-cell function and survival.
7. Vitamins
Vitamins are important nonenzymatic antioxidants that play an important role in immunological responses (Table 3). A recent report suggests that vitamins play an important role not only in normal growth but also in strengthening immunological responses (170). For example, β-carotene, a precursor of Vitamin A, is known to enhance production of IL-2 and IFN-γ in T lymphocytes in an in vivo model system (312). Vitamin A and D are required for proper homing of T cells to the gut and skin, respectively (182). DCs in the gut-associated lymphoid organs produce enzymes to convert Vitamin A to retinoic acid, which induces the surface expression of the T-cell gut-homing receptor, CCR9 (119). However, retinoic acid suppressed the expression of the skin-homing receptors, CCR4, E-lig, and P-lig. Similarly, DCs in the skin draining lymph nodes have the ability to convert Vitamin D to 1,25(OH)2D3, where 1,25(OH)2D3 is known to induce the expression of the skin-homing receptor, CCR10 (264). Interestingly, Vitamin D and the Vitamin D receptor (VDR) are important for a TCR response to antigen stimulation. VDR is highly expressed on active T cells, whereas naïve T cells do not express VDR (298). Induction of VDR expression and phospholipase C isoenzyme is required for T-cell signaling and activation. Vitamin D deficiency has been shown to increase Th17 and Th9 cells and reduce the Treg population, thereby promoting autoimmune diseases, such as multiple sclerosis (MS), type I diabetes, systemic lupus erythematosus (SLE), and rheumatoid arthritis (RA) (44, 178, 215). Taken together, Vitamin A and D are important for regulating T-cell-mediated immunity in the gut and skin.
AICD, activation induced cell death; GPX, glutathione peroxidase; HIV, human immunodeficiency virus; hPBMCs, human peripheral blood mononuclear cells; IFN-γ, interferon-γ; iNOS, inducible NO synthase; MnSOD, manganese superoxide dismutase; ROS, reactive oxygen species; Th, T helper; TNF, tumor necrosis factor.
Vitamin C, another important nonenzymatic antioxidant, is associated with increased production of IL-12 by DCs when activated with ascorbic acid (AA). Moreover, T cells activated with AA-treated DCs produce higher amounts of Th1-polarizing cytokines (IL-2 and IFN-γ) as compared to the Th2-polarizing cytokines (IL-5 and IL-10) (124). Therefore, Vitamin C can modulate the T-cell responses by increasing Th1 bias. In addition, in vitro and in vivo studies have suggested that Vitamin E can enhance IL-2 production, T cell proliferation, and redistribution of ζ-chain-associated protein kinase 70 (Zap70) protein–tyrosine kinase, and its substrates (linker of activated T cells [LAT] and Vav) to immune synapses in aged mice compared to young mice (177, 191, 307). Zap70, LAT, and VAV redistribution is involved in downstream signaling in T cells, which are required for cytokine gene transcription. Vitamin E has also been shown to be important in neutralizing the ROS-mediated damage of membrane lipids in age-associated, impaired CD4+ T cell function. Taken together, the immune system is enhanced with Vitamin E supplementation. These studies therefore suggest that vitamins with antioxidant capacity may be important molecules involved in redox regulation of T cells.
VI. Web of Redox Regulation Molecules
Redundant pathways that regulate the production of ROS and RNS are known to exist, and a balance between pro-oxidant and antioxidant molecules maintains low cellular oxidative stress. However, due to exogenous factors (pollutants or ionizing radiation) or endogenous factors (inflammation or chronic viral stimulation), genes that regulate the cells' susceptibility to oxidative stress are differentially expressed, leading to pathogenesis.
Recent studies have demonstrated that engagement of the TCR induces rapid production of ROS (Fig. 12). Moreover, ROS production modulates T-cell signal transduction and gene expression (16, 61). Under conditions of normal TCR activation, T cells contain relatively low-to-moderate levels of ROS (61, 105). Since ROS have the ability to diffuse short distances, they are characterized as small signaling molecules. However, a repetitive stimulation of the TCR or stimulation with a high dose of antigen, or exposure to H2O2, could increase ROS concentrations, leading to T-cell hyporesponsiveness or death (106). Furthermore, data from other cell types have suggested that ROS could promote either apoptosis or necrosis, depending upon the amount of cellular ROS (74, 326). Abundant ROS promote lipid peroxidation (LPO), macromolecular damage, and necrotic cell death, and a decreased amount of ROS promotes changes in cell signaling and cell function (131).

Interestingly, T cells activated in vivo and subsequently cultured briefly in vitro exhibit features of necrosis (i.e., rapid membrane permeability) and apoptosis (i.e., caspase-dependent DNA fragmentation and nuclear condensation) (292). When viewed under an electron microscope, these activated T cells clearly exhibit many of the hallmarks of apoptosis (i.e., nuclear condensation, cell shrinkage, and loss of the nuclear membrane) (292). Notably, all of these cell death characteristics (both apoptotic and necrotic) can be prevented by culture with antioxidants, thereby suggesting a role for ROS in different forms of cell death (105, 252, 254). However, the molecular mechanisms that regulate T-cell fate and downstream signaling upon ROS exposure are largely unknown and are currently major topics of interest in T-cell research.
The mitochondrion is a primary source of cellular energy and ROS, and is functionally important in regulating CD8+ T cell activity (318). When transgenic CD8+ T cells were incubated with increasing doses of rotenone (an electron transport complex I inhibitor used to block mitochondrial function), production of H2O2, calcium flux, and ERK1/2 phosphorylation were decreased within minutes of T-cell activation. Failure to undergo signal transduction resulted in decreased T-cell division initiated by peptide-coated cells, CD3/CD28 Abs, and PMA/ionomycin stimulation. Decreased function after rotenone incubation was not phenotype specific. That is, naïve, effector, and memory CD8+ T cells exhibited decreased production of both IFN-γ and TNF-α after peptide stimulation. Furthermore, incubation with rotenone decreased degranulation of effector and memory cells, a critical step in the cytolysis of infected cells. These data suggest that electron transport complex I is required for CD8+ T-cell function.
Moreover, activation of T cells is associated with an increase in ROS and an increase in the level of reversible cysteine sulfenic acid production. Reversible cysteine sulfenic acid is a reactive oxygen intermediate (ROI), which is important in the formation of disulfide bonds and GSH conjugation, suggesting that reversible cysteine sulfenic acid is an important ROI in regulating multiple cell-signaling processes associated with T-cell activation (188). Analysis of specific proteins revealed that the protein tyrosine phosphatases SHP-1 and SHP-2, as well as actin, underwent increased sulfenic acid modification after TCR stimulation. Subsequent experiments revealed that the reversible formation of cysteine sulfenic acid was critical for ERK1/2 phosphorylation, calcium flux, cell growth, and proliferation of naïve CD8+ and CD4+ T cells. Inhibition of reversible cysteine sulfenic acid formation decreased TNF-α production more than IFN-γ. Taken together, these results suggest that reversible cysteine sulfenic acid formation is an important regulatory mechanism by which CD8+ T cells can modulate signaling, proliferation, and function.
Analysis of individual intracellular signaling molecules in the redox state has demonstrated the importance of redox regulation of signaling molecules in vivo. In addition to AP-1 and NFκB, the binding of several transcription factors is modulated by redox status, including c-Myb (199) and p53 (96), JNK (Jun NH2-terminal kinase)/SAPK (stress-activated protein kinase) (104) and MAPK/ERK (244), and src family PTK kinase, such as Lck (100). Our group recently identified a role for ROS in regulating T-cell death upon repetitive TCR stimulation (207). We have demonstrated that an SOD mimetic compound, MnTBAP, protects MART-127–35-specific CTLs from AICD without interfering with the IFN-γ response and without inhibiting JNK phosphorylation (207). Other studies have also shown that mitochondria have a role in ROS-mediated upregulation of FasL (92). While ROS are known to participate in AICD regulation by induction of CD95L expression, the mechanism and signal transduction pathways necessary for ROS-induced AICD are still areas of intense research. Kaminski et al. have shown that the proximal TCR-signaling machinery, including Zap70, LAT, SH2 domain-containing leukocyte protein of 76 kDa (SLP76), phospholipase Cgamma1 (PLCgamma1), and protein kinase C theta (PKC-theta), are crucial for ROS production (128). Kaminski et al. (128) further report that PKC-theta is translocated to the mitochondria and suggest that PKC-theta-dependent ROS generation by mitochondrial complex I is essential for inducing AICD. Furthermore, in cells depleted of mitochondrial DNA, mitochondria were identified as the source of activation-induced ROS (128). Briefly, inhibition of the mitochondrial electron transport complex I assembly by siRNA-mediated knockdown of the chaperone NDUFAF1 blocked ROS production. This signal was found to be essential for CD95L expression, where inhibition of complex I assembly by NDUFAF1-specific siRNA prevents AICD.
Interestingly, studies indicate a role of MnSOD inactivation during Fas (CD95)-mediated apoptosis in Jurkat T cells (217). This study illustrated that after oligomerization of the Fas receptor, MnSOD is selectively degraded during apoptosis. In the presence of cycloheximide, an inhibitor of protein synthesis, the cell death rate and MnSOD degradation were accelerated. MnSOD cleavage was partially inhibited in the presence of the pan-caspase inhibitor, z-VAD-fmk, suggesting that caspases may mediate cellular protection by stabilizing antioxidant enzymes and thereby controlling oxidative stress (217). Therefore, functional MnSOD is important in regualting oxidative-stress-mediated apoptosis of T cells.
T cells also have the capacity to generate NO upon antigen stimulation, which may affect signal transduction, Fas ligand surface expression, and apoptotic cell death of mature T lymphocytes. The involvement of iNOS in the generation of T-lymphoctye-derived NO and its role in inhibiting T lymphocyte proliferation have been documented (108, 135). Vig et al. have shown that iNOS production in activated T cells regulates T-cell death and immune memory (295). Thus, it has become clear that iNOS activity also regulates the development, differentiation, and/or function of T cells and B cells and also affects natural killer (NK) cells (30). The role of NO in mediating T-cell cytokine production and signal transduction in histidine decarboxylase knockout mice (HDC-KO mice) has also been recently documented (147). In the HDC-KO mice, with a defect in endogenous histamine production, an increase in IFN-γ mRNA and protein expression levels of splenocytes was reported to be associated with a significant increase (2.5-fold) in NO production, compared to the WT animals. Furthermore, histamine treatment decreased NO production from both WT and HDC-KO mouse T lymphocytes. These results indicate that, in addition to its direct effects on T-lymphocyte function, histamine regulates cytokine production and T-cell signal transduction through its effects on NO production.
While these observations describe causes and effects of various ROS species, it should also be noted that the quantitative and qualitative effects of ROS are affected by other factors that include age, gender, ethnicity (linked to gene polymorphism of antioxidant genes), external environment, and degree of inflammation. These factors form a complex web that regulates the susceptibility of an individual to oxidative-stress-mediated diseases.
VII. Role of Redox Regulation in Human Diseases
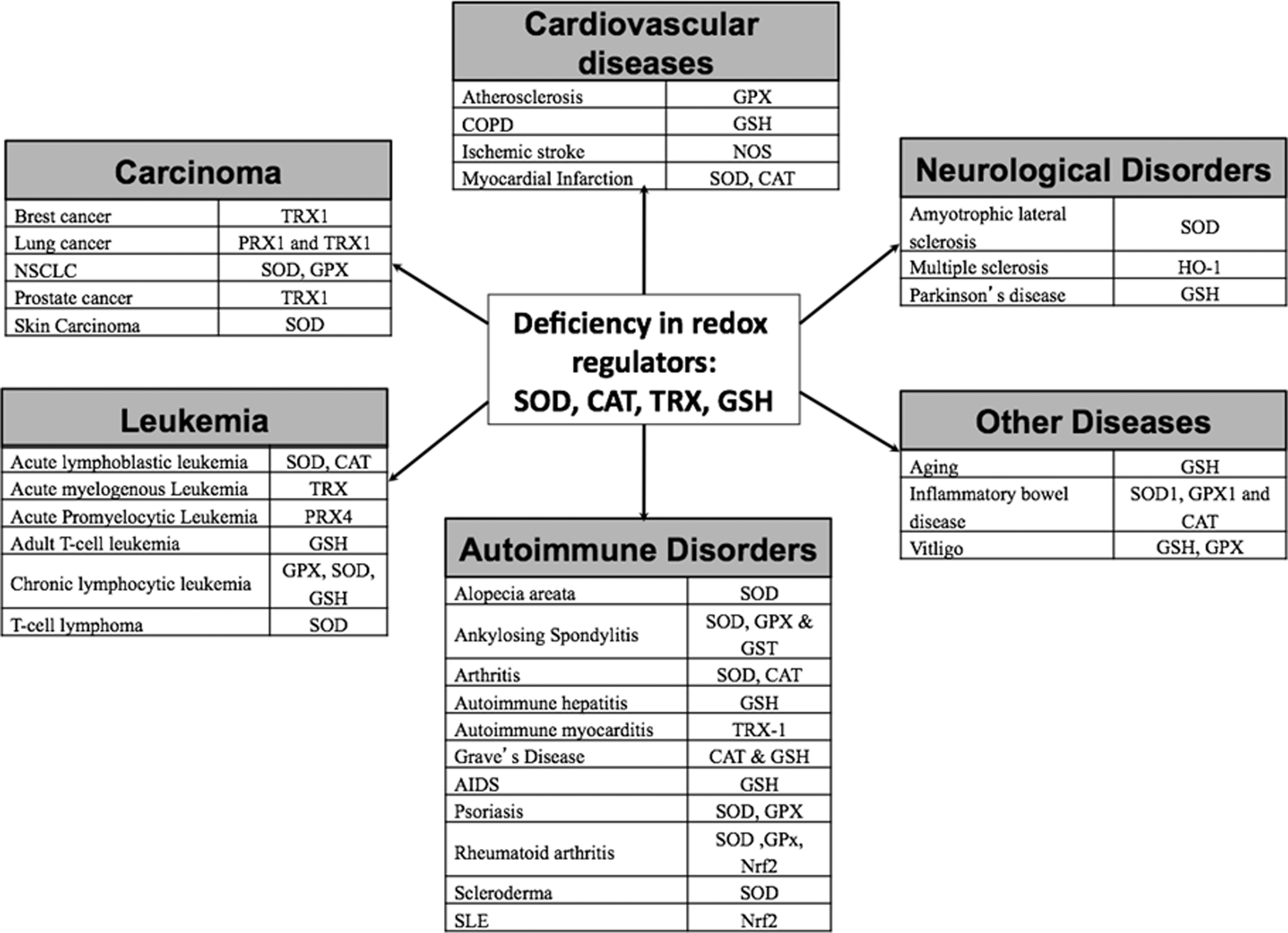
As discussed in previous sections, ROS are essential for efficient and proper execution of a large number of cellular processes, including signaling induced by exogenous factors. However, ROS are highly reactive, where excessive and prolonged ROS production, disturbance in redox regulators, or an imbalance in the expression of antioxidant enzymes can considerably damage cellular constituents. Thus, ROS balance is implicated in the onset of various diseases (Fig. 13). However, this review focuses on diseases related to T-cell pathogenesis arising from direct effects of a pro-oxidant microenvironment.
A. Autoimmune disorders
1. Rheumatoid arthritis
RA is a common autoimmune disease characterized by chronic inflammation of the synovial joints, where T cells have a defined role in the pathogenesis of this disease (73). While the exact mechanism of ROS-associated RA has not been established, recent studies suggest that oxygen free radicals play an important role in such chronic inflammatory diseases (213). Based on studies using animal models for human RA, Olofsson et al. demonstrated that a polymorphism in the Ncf1 (p47phox ) gene leads to reduced oxidative burst and increased activation of arthritogenic T cells, thereby increasing the severity of arthritis (211). Furthermore, NOX2-derived ROS can suppress antigen-dependent T-cell reactivity and reduce the severity of the disease in animal models (82, 189). Interestingly, an oxidative burst-inducing pharmaceutical compound known as phytol (3,7,11,15-tetramethyl-2-hexadecene-1-ol) has been used to treat arthritis-prone Ncf1DA rats (115). The investigators in this study propose that the higher oxidative burst by phagocytes may lead to apoptosis of autoreactive arthritogenic T cells in this model of RA. Increased concentrations of ROS activate phagocytes, and activated phagocytes are known to increase the overall production of TNF-α and IL-1β. These cytokines are then responsible for activation of NFκB (197). The resulting constitutive feedback loop leads to the activation of NOX-signaling pathways, increased oxidative stress, and cytokine production. This attracts leukocytes, memory T cells, macrophages, and other inflammatory cells in synovial joints, leading to degradation of cartilage and bone. The high oxidative stress levels in the synovial fluid of RA patients lead to the hyporesponsiveness of the T cells in the synovial fluid in these inflamed joints (91). This finding was later demonstrated to result from oxidative-stress-mediated membrane displacement of a protein called LAT. Proper anchorage of LAT and the activation of T cells were seen upon supplementing the cell with GSH. Furthermore, persistent ROS production in RA synovial fluid T cells is associated with Ras and Ras-proximate-1 (Rap1)-signaling proteins (233). These signaling molecules play an important role in T-cell stimulation. It was demonstrated that activation of Ras is necessary for intracellular ROS production, while activation of Rap1 can block Ras-dependent ROS production. These studies suggest that impaired redox regulation of synovial fluid T cells may be associated with the pathogenesis of RA.
2. Systemic lupus erythematosus
SLE is an autoimmune disease characterized by acute and chronic inflammation of various tissues, prominently the kidneys, skin, joints, or the central nervous system. SLE mainly occurs due to production of autoantibodies due to an imbalance in cytokine secretion and antioxidant molecules in SLE patients (15). Interestingly, ROS-modified IgG has been associated with the induction of circulating SLE autoantibody where neoepitopes elicit an immune response in SLE patients (7). Other studies have suggested that increased endogenous NOS (201), reduced oxidative burst (58), and decreased expression of SOD, catalase (CAT), and GSH (260) could potentially lead to T-cell-mediated immune responses in SLE. Earlier studies have demonstrated that oxidative stress leads to the downregulation of TCR ζ-chain expression in patients who have undergone surgery (117). This type of oxidative stress-induced downregulation is seen in T cells isolated from SLE patients (83, 84). While it is known that the ζ-chain is important for TCR signaling and activation, lower GSH levels, elevated levels of ROS, subsequent T-cell activation, together, lead to prolonged mitochondrial hyperpolarization and ATP depletion in SLE. Furthermore, decreased expression of ζ-chain and low levels of GSH prevent the regeneration of ζ-chain in SLE T-cells. Taken together, these fundamental studies in TCR signaling suggest a critical role of oxidative stress-induced downregulation of TCR signaling via mitochondrial transmembrane potential regulation in SLE patients.
3. Type 1 diabetes
Type 1 diabetes is an autoimmune-induced disease in which T cells recognize pancreatic β-cell antigens and initiate leukocyte infiltration. The ROS generated by the initial insult to the islets stimulate the activation of redox-dependent NFκB and other transcription factors. This stimulation leads to an increase in the production of proinflammatory cytokines, such as TNF-α, IL-1β, and ROS, which eventually damage the pancreatic β-cells. Moreover, innate derived ROS are critical for T-cell activation, as they stimulate production of these cytokines from APCs while enhancing T-cell proliferation and activation (285). Therefore, oxidative stress has a high impact in the development of type 1 diabetes. Moreover, there are several other factors associated with the etiology of type 1 diabetes, including environmental factors, genetic susceptibility, deficiency, and diet.
Islets contain low levels of antioxidant enzymes such as SOD1, GPX1, and CAT, suggesting that pancreatic β-cells are highly susceptible to oxidative stress (156). Adoptive transfer of the diabetogenic T-cell clone (BDC-2.5) has been shown to induce diabetes in young NOD-SCID mice, which can be delayed or prevented altogether by treating the recipient mice with the SOD mimic AEOL-10113 before the adoptive transfer of the BDC-2.5 clone (223). Therefore, this study supports the finding that the pancreatic β-cells are highly susceptible to oxidative-stress-induced apoptosis. Moreover, oxidative stress has been shown to induce diabetes-associated vascular dysfunction leading to diabetic nephropathy, retinopathy, and cardiomyopathy (85, 278). Thus, modulating ROS can serve as an important therapeutic tool to treat type 1 diabetes and its vascular complications.
B. Cardiovascular disorders
1. Atherosclerosis
Atherosclerosis is a cardiovascular disease marked by chronic inflammation of the blood vessels. Oxidative stress and inflammation result in the infiltration of activated inflammatory cells from the coronary circulation into the arterial wall, leading to the pathogenesis of atherosclerosis (25). It is known that accumulation of low-density lipoprotein (LDL) on the internal membrane of arteries (intima) and prolonged oxidative modification of LDL molecules by ROS lead to formation of atheroslerotic lesions. Oxidative modification of LDL can initiate an inflammatory response (99). Ammirati et al. have recently reported a significant correlation between increased circulating TEM and the generation of atherosclerotic lesions and high LDL production (9). Activated T cells are known to contribute to the proinflammatory components of atherosclerosis. Ammirati et al. suggest that TEM are responsible for atherosclerotic lesions (9). These authors further suggest that TEM subsets that express HLA-DR, CXCR3, and CCR5 are recruited into the atherosclerotic plaques. Frostegard et al. demonstrated that exposing monocytes and T cells to oxidized LDL for 72 h leads to an increase in IL-2 receptor expression and DNA synthesis (78). The results indicate that oxidized LDL may induce migration of monocytes, thereby leading to the formation of atherosclerotic plaques. Based on murine in vitro and in vivo studies, elevated homocysteine (Hcy) levels were thought to be an independent risk factor for atherosclerosis (321). The autooxidation of Hcy-generated ROS significantly promoted ConA-induced proliferation and partially inhibited apoptosis of cultured, activated mouse splenic T lymphocytes. Furthermore, the in vivo studies using ApoE-knockout mice, with hyperhomocysteinemia, have significant T-cell proliferation in response to ConA and increased intracellular ROS. These data suggest that oxidative stress is involved in the chronic inflammatory progression of atherosclerosis and suggest that ROS production is a key factor in the progression of cardiovascular diseases.
2. Cerebral ischemia/stroke
A stroke is an interruption of the blood supply to any part of the brain leading to the rapid loss of brain function. Oxidative state plays a key role in the regulation and control of numerous signal transduction pathways in neurons (53, 198). Microglial cells and astroglial cells are direct effector cells of the CNS. Several studies present evidence that activated microglial cells, in response to ischemia, have the potential to release several proinflammatory cytokines such as TNF-α, IL-1β, and IL-6, as well as other potential cytotoxic molecules, including NO and ROS (167). IL-1-induced inflammation initiates the expression of chemokines CXCL1 and CXCL2 (181). Moreover, these chemokines may cause the infiltration of neutrophils. A recent study has identified infiltration of interleukin-17-producing γδ T cells 3 days after the onset of ischemia in a mouse model. The study also demonstrates that blocking T-cell infiltration reduced the infract size (263). Moreover, Liesz et al. have indicated that Tregs may delay brain damage after stroke (159). It is well known that hypertension is a high risk factor for stroke-induced death, and recently, a role for T cells in angiotensin II-induced hypertension has been proposed by Guzik et al. (93). Angiotensin II induces T-cell activity, proinflammatory cytokine production, and infiltration in perivascular fat. Based on these in vivo studies, angiotensin II can stimulate peripheral blood T cells to produce TNF-α and IFN-γ as well as express tissue-homing receptors, all of which lead to the development of hypertension and vascular dysfunction. Hoch et al. have further demonstrated that angiotensin II is important in activating T cells, in inducing the expression of tissue-homing markers, and in producing the proinflammatory cytokine, TNF-α (107). The researchers further suggest that an autocrine loop exists in T cells where T-cell-derived angiontesin II activates T-cell NOX, thereby inducing ROS production, and subsequently TNF-α production. Therefore, angiotensin II-induced hypertension is associated with the accumulation of T cells in perivascular fat, and moreover with T-cell accumulation in atherosclerotic lesions. These studies would then suggest that there is an indirect and direct association of T-cell activity, hypertension, and stroke. Moreover, deletion of SOD3 in the circumventricular organ can increase T-cell activation, leading to increased angiotensin II-induced vascular superoxide production and vascular inflammation because of T cell and leukocytein filtration (164). Therefore, redox regulation of T cell may play an important role in the pathogenesis of stroke.
C. Cancer and metastasis
The role of ROS in cancer cells has long been suspected, and growing evidence suggests that cancer cells are under increased oxidative stress in comparison to normal cells. Szatrowski et al. and other groups have demonstrated enhanced ROS production, along with overproduction of antioxidant enzymes, in cancer cells (267, 275). Moreover, hypoxia-induced ROS production in the tumor milieu is associated with loss of genomic stability and downregulation of DNA repair pathways (31). For example, oncogenes c-myc and an allele of RAS2 (val19) have been shown to induce ROS production in tumor cells (221). While the oncogenic c-myc increases ROS production, induces DNA damage, and regulates p53 function, oncogenic RAS2 constitutively activates the cAMP-PKA pathway resulting in the increase in ROS production. Tumor-associated macrophages (TAMs), myeloid-derived suppressor cells (MDSCs), and activated granulocytes produce significant amounts of ROS and NO, which leads to oxidative stress-induced downregulation of immune responses (151, 256, 275). In advanced cancer patients, activation of granulocytes and the granulocyte-derived H2O2 is associated with the systemic T-cell suppression. Increased ROS production is seen in cancer cells as compared to normal cells, including primary leukemia cells isolated from patients with chronic lymphocytic leukemia, CLL (221, 323).
Zhou et al. (323) have further suggested that treating these cells with 2-methoxyestradiol, an SOD inhibitor, has a cytotoxic effect on these cancer cells. This would imply that it would be beneficial if anticancer therapies are directed to regulate ROS production in cancer cells, but not in normal cells. For example, a recent study demonstrates a novel DR5 (TRAIL R-2) monoclonal antibody, AD5–10, generates ROS production in Jurkat leukemia cells. As a result of the ROS production, JNK is activated, and mitochondrial membrane potential is lost, and intracellular GSH and oxidized glutathione (GSSG) levels are decreased, and endonuclease G is translocated from the mitochondria into the cytosol, all of which lead to the selective apoptosis of the leukemia cells in vitro (45). Moreover, Jurkat, a human acute lymphocytic leukemia cell line (Jurkat T-ALL), transfected with a dominant-negative (DN) form of JNK (but not of p38), enhanced NFκB activation, reduced caspase-8 in death-inducing signaling complexes (DISCs), and reduced damage to mitochondria, thereby inhibiting AD5–10-induced cell death in the DN-mutant cells.
The use of pro-oxidants to increase ROS as well as inhibitors of antiapoptotic proteins has been employed to control tumor growth. Several preclinical and clinical studies have used inhibitors of the Bcl-2 family of proteins to induce apoptosis in cancer cells by primarily involving the mitochondrial apoptosis pathways (145). Jurkat and HeLa cells transfected with a tetracycline-regulated Bcl-2 expression system were used in redox signaling studies to determine the role of Bcl-2, ROS, and GSH levels in apoptotic signals. Based on the results presented in this study, ABT-737 (pan-Bcl-2 inhibitor) induces caspase activation and apoptosis by decreasing GSH levels, with a concomitant increase in ROS (111). In summary, these studies validate rational molecular approaches that target antiapoptotic pathways involving ROS when developing novel combination therapies for cancer treatment in synergy with other strategies.
Strategies employed by the tumor cells to evade cell death include immune tolerance to malignant cells, impaired antigen presentation, tumor-induced immune suppression, negative co-stimulatory pathways, and dysfunctional TCR signaling that contributes to the resistance to AICD (230). In addition to these strategies, recent studies have suggested that deregulation of critical signaling pathways, in particular Notch, PI3K/Akt, MAPK, Jak/STAT, and TGF-β, may contribute to T-ALL and T-cell non-Hodgkin's lymphoma. A recent study identified IL-7 as a survival factor required for early T-cell differentiation and normal T-cell proliferation (20). IL-7 induces the activation of the JAK/STAT, MEK/ERK, and PI3K/Akt signaling pathways in T-ALL cells, where PI3K signaling is shown to induce Bcl-2 expression, and is required for the proliferation and survival of T cells. The elevated levels of ROS seen in T-ALL cells is attributed to the PI3K/Akt/mTOR pathway-dependent induction by IL-7, and this overexpression of ROS requires NOX activity and mitochondrial respiration (265). Furthermore, the same group of researchers have shown that T-ALL cells require glucose uptake for ROS production in T-ALL cells treated with IL-7. Moreover, the study also demonstrates that IL-7 increases the expression of the glucose transporter GLUT1 in a PI3K-dependent manner. These observations suggest that substrates of molecular pathways activated by microenvironmental factors regulate the viability and proliferation of T-ALL cells and provide the means for the development of novel treatment strategies.
Interestingly, immunosuppressive cells known as MDSCs can impair CD8+ T-cell immunity by increased production of ROS, which inhibits ζ-chain expression in T cells (200). In addition, MDSC induced the nitrosylation of the TCR tyrosine residues on the surface of antigen-specific CD8+ T cells, thereby inducing T-cell dysfunction. Tacke et al. have demonstrated that chronic Hepatitis C virus infection can lead to MDSC-mediated suppression of T-cell response by generating ROS, suggesting that MDSCs are important in regulating T-cell-mediated immune responses (276). Moreover, based on this report, MDSCs suppress T-cell responsiveness by upregulating the expression of p47phox, a component of the NOX2 complex, which is important in ROS production. A recent study demonstrated that Nrf2 deficiency creates a responsive microenvironment for metastasis to the lung, where MDSCs of Nrf2-deficient mice induced overproduction of ROS compared to the WT mice (255). Therefore, the increased pulmonary metastatic potential of tumor cells in Nrf2-deficient mice can be attributed to the overproduction of ROS. Moreover, greater numbers of inflammatory cells, including MDSCs, were identified in the lung and bone marrow of Nrf2-deficient mice with metastatic cancer. Cancer cells have efficient antioxidant mechanisms to survive high levels of ROS. Some of these defense mechanisms include upregualtion of peroxirodoxins (Prx) and TRX in response to oxidative injury (43, 229). In addition, the predominance of other suppressive immune cells (such as Tregs and MDSCs) that are innately high in antioxidant molecules aid in the development of cancer and evade effector immune response. Redox-modulating strategies thus are important as controls of cancer development and progression.
D. Neurological disorders
1. Amyotrophic lateral sclerosis
ALS is marked by the progressive loss of motor neurons, neurofilament inclusions, astrocytosis and muscle atrophy, inflammation, and T-cell infiltration. ALS is caused by a mutation in the SOD1 gene, which renders SOD1 inactive, resulting in the oxidative damage of motor neurons. To date, there are several transgenic mouse models for human ALS with specific mutations in the Cu2+/Zn2+ SOD1 gene, including SOD1G93A, SOD1G37A, SOD1G85R, SOD1D90A, and SOD1G93A transgenic rat model. Currently, the SOD1G93A transgenic mouse model is used to test therapeutic agents to treat ALS and to understand ALS disease progression at the molecular level (123). While earlier studies have demonstrated reduced counts of Tregs and monocytes in ALS, a recent study suggests that Tregs (CD4+CD25+FoxP3+) are recruited to the CNS to prevent or attenuate the neurodegenerative process by stimulating the secretion of anti-inflammatory cytokines (144). On the contrary, Tregs have been shown to help in protecting ALS from progression, and FoxP3 is lost in later stages of this disease. Furthermore, injecting CD4+ T cells has been shown to increase the survival of mSOD1 mice, a murine model of human ALS (23). Another study has identified that CD154 (co-stimulatory CD40 ligand on T cell) can further activate the immune response when bound to CD40 on APCs, a promising therapeutic target for ALS (22). Taken together, these studies would suggest that understanding the molecular mechanisms of microglial-derived inflammatory signals would be important in treating this neurodengerative disease, and further research in regulating microglial-derived ROS and cytokine expression is warranted.
2. Multiple sclerosis
MS is a CNS demyelinating, inflammatory disease marked by a significant decrease in the number of oligodendrocytes (OLs). MS is associated with axonal degeneration and irreversible neurological disabilities (29). EAE is a well-established animal model for MS with a Th1 cytokine-induced active phase of the disease (69). That is, during the active phase of this disease in EAE, TNF-α, IL-2, and myelin/OL glycolprotein-specific antibodies are actively produced. Moreover, oxidative stress-induced heme oxygenase-1 (HO-1), a heat shock protein, is overexpressed in the CNS of EAE mice (163). Other studies have shown that erythropoietin (EPO) and EPO-induced upregulation of endogenous HO-1 repress immune responses to EAE in MOG-EAE mice to protect the neuronal cells from oxidative stress-triggered cytotoxicity (46). Intraperitoneal administration of EPO was shown to reduce clinical severity by significantly repressing immune responses by the Th1 and Th17 lymphocyte populations at the site of the lesions and increasing systemic Th2 and Treg populations. The initial infiltration of autoreative CD4+ Th1 cells in the brain lesions of MS is followed by the upregulation of proinflammatory cytokines, TNF-α as well as IL-17, a proinflammatory cytokine secreted by Th17 cells (214). Based on studies using uncoupling protein 2 (UCP2)-deficient mice, UCP-2 normally functions to reduce the production of ROS during infection, and in EAE, UCP-2 has a protective response (297). This study further illustrates that UCP-2-deficient mice have modified their immune response where CD4+ T cells produce significantly higher levels of proinflammatory cytokines; for example, TNF-α and IL-2 and the CD4+ and CD8+ T cells upregulate ROS production. Further research to limit demyelination in MS by developing antioxidant therapies directed toward Th1- and Th17-mediated immune responses in MS is warranted.
3. Parkinson's disease
Similar to ALS, Parkinson's disease (PD) is a neurodegenerative disease marked by activated microglia (innate immune cells of the CNS) and infiltrating T cells at sites of neuronal injury. In PD, predominantly, the M1 microglial phenotypes are present in the injured neurons, where M1 microglia are responsible for secreting proinflammatory cytokines (i.e., TNF-α and IL-1β), ROS, and NO, all of which lead to neurotoxicity, (13). Inflammation of phagocytic microglia, release of cytokines, T cells, and complement activation play a role in damaging neurons, in particular, the dopaminergic neurons. In PD patients, the pigmented dopaminergic neurons in the substantia nigra part of the midbrain are triggered to undergo apoptosis; based on recent evidence, two mutations in the α-synuclein gene have been linked to the autosomal dominant form of this disease (165). Interestingly, the α-synuclein gene mutation is associated with accumulation of dopamine in the dopaminergic neurons in PD patients. The instability of dopamine's catechol ring structure can apparently undergo spontaneous oxidation, leading to excessive ROS production and increasing oxidative-stress-induced death of dopaminergic neurons in PD patients. A greater understanding of the T-cell population that mediates these effects, as well as the molecular signals involved in PD progression, should identify new targets for neuroprotective immunomodulation to treat these devastating neurodegenerative diseases.
E. Skin disorders
The skin is constantly exposed to endogenous and environmental pro-oxidant agents, which lead to the generation of harmful ROS. Although healthy skin is equipped with a large number of defense mechanisms, including antioxidant systems that attenuate the harmful effects of ROS, the increased or prolonged presence of free radicals can override ROS defense mechanisms and mediate numerous cellular responses that can contribute to the development of a variety of skin disorders.
1. Psoriasis
Psoriasis is a common inflammatory disease of the skin and joints, triggered by an immune response to endogenous (self) and exogenous factors (bacterial or viral). Formation of psoriatic lesions is thought to be elicited by the complex cross-talk between keratinocytes and components of the innate and acquired immune system. Psoriatic keratinocytes possess an enhanced ability to resist apoptosis, which might be one of the key pathogenic mechanisms in psoriasis. In addition, statistically significant decreases in erythrocyte catalase, GSH, SOD levels, and GPx activities were noted in psoriatic patients (322). The observed increase in erythrocyte malondialdehyde suggests that the cells were in a perioxidative state. Based on these results, oxidative stress plays a significant role in the progression of psoriasis.
Furthermore, subsequent studies have suggested that antioxidant strategies could prove to be beneficial treatments for psoriasis. The cellular signaling pathways, such as MAPK/AP-1, NFκB, and JAK-STAT signal transducers and activators of transcription, are known to be redox sensitive and are involved in the progression of psoriasis (299). Interestingly, psoriasis has been suggested to be an autoimmune response to streptococcal throat infection. Patients with psoriasis have CD4+ and CD8+ T cells that are reactive to antigen determinants on streptococcal M-protein and type-1 keratins. Therefore, molecular mimicry has been proposed as the method of eliciting autoimmunity in psoriatic lesions (288).
2. Scleroderma
Scleroderma is a chronic autoimmune disease characterized by fibrosis, vascular injury, and increased collagen deposition in the skin (313). There are two forms of scleroderma: limited cutaneous systemic sclerosis (SSc) and diffuse cutaneous SSc (dcSSc). While hands, arms, and face are affected in patients with SSc, dcSSc involves fibrosis of a large area of the skin and at least one other internal organ: the kidney, heart, or lung (51). Murine models of SSc and dcSSc were used to understand the role of ROS in the pathogenesis of SSc (258). Briefly, Balb/c and immunodeficient Balb/c SCID mice were injected with pro-oxidative agents, bleomycin, or phosphate buffered saline. Based on histological, biochemical, and immunological studies, ROS played a significant role in SSc, and the specific oxidation of autoanitgen has been shown to induce systemic sclerosis. Moreover, Servettaz et al.(258), demonstrate that the type of ROS determines the form of SSc. Peroxynitrites induced limited SSc, which exhibit skin fibrosis and serum anti-CENP-B IgG, whereas hypochlorite or hydroxyl radicals induced diffuse SSc with cutaneous and lung fibrosis and serum anti-DNA topoisomerase I antibodies. This finding suggests that decreased antioxidant levels and increased accumulation of ROS are key components in the progression of scleroderma.
Recent investigations have suggested that in addition to ROS production, apoptosis is involved in the progression of scleroderma (313). Patients with SSc have high serum levels of soluble Fas, which would protect autoreactive T cells from FasL-induced apoptosis. In these same patients, spontaneous apoptosis of CD8+ T cells was also observed, suggesting that the T-cell imbalance leads to autoimmunity in patients with SSc. However, this is based on the stage of the SSc disease. Based on recent findings, effector peripheral blood CD8+ T cells upregulate the expression of profibrotic cytokine IL-13, thereby leading to the observed cellular toxicity in SSc patients (79). Interestingly, current immunotherapy regimens focus on regulating the immune system in scleroderma with conventional methods (nonselective immunosuppression), T-cell- or B-cell-targeted therapies, HSC transplantation, antifibrotic treatments, or immunomodulatory agents (175).
3. Vitiligo
Vitiligo is a condition caused by the loss of pigmentation of the skin as a result of apoptosis of epidermal melanocytes. Biochemical, neurological, environmental, genetic, and immunological factors have all been associated with the activation of vitiligo (87). Moreover, a melanocyte-specific T-cell-mediated immune response has been implicated in the development of vitiligo. Recently, activated, type-1 Teff cells were histologically identified in the perilesional margins of the depigmented skin, suggesting that skin-homing melonocyte-specific CTLs are responsible for the depigmentation in vitiligo patients (289). Furthermore, using an explant model for vitiligo, Van Den Boorn et al. (289) were able to demonstrate that the perilesional T cells induce apoptosis of melaoncytes only in the pigmented skin explants. Other studies have suggested that ROS and H2O2 production impairs biological processes (87). Tyrosinase is a rate-limiting enzyme required for melanogenesis, and in the presence of ROS and/or H2O2, the activity of this enzyme is impaired, resulting in the loss of melanocytes in vitiligo.
F. Viral diseases
1. Human immunodeficiency virus
Oxidative stress appears to contribute to HIV infection in humans, where ROS may play a critical role in HIV replication. A number of studies have demonstrated that GSH levels and acid-soluble thiol levels are decreased in AIDS patients, while plasma glutamate concentrations are increased (34, 65, 66). Moreover, GSH levels are decreased in plasma, lung epithelial lining fluid, and PBMCs in HIV-infected patients. In addition to confirming earlier findings that HIV-infected individuals have decreased GSH levels, recent studies suggest that LPO, which is associated with oxidative stress, is significantly higher in HIV-infected patients (301). These findings suggest that HIV-infected patients have increased oxidative stress, and the efficacy of treating these patients with antioxidants remains to be determined. Rhesus monkeys infected with simian immunodeficiency virus (SIVmac251), a closely related animal model of HIV, have significant loss of plasma thiol levels (i.e., decreased cysteine levels) and increased glutamate concentrations within 2 weeks of infection (67). Based on these studies, GSH depletion and the concomitant increase in ROS are correlated with the pathogenesis of HIV-infected patients.
This knowledge was exploited to initiate clinical trials employing antioxidant therapy to treat AIDS patients. The first study of this kind used the antioxidant NAC, a cysteine prodrug that was shown to block HIV expression in chronic and acute infection models as well as block HIV replication in normal PBMCs. NAC restores GSH levels and maintains normal levels of thiols during oxidative stress (241). The observed antiviral effect of NAC is due to inhibition of viral stimulation by ROS that are produced in response to chronic stimulation of HIV-specific T cells and inflammatory cytokines (241, 269). An earlier study by Sandstrom et al. demonstrated that T-cell lines infected with HIV are highly susceptible to apoptosis. Moreover, they also demonstrated that GPx deficiency in HIV-infected human leads to apoptosis of CD4+ T cells (253). Other studies have supported the above finding, and moreover, these studies also demonstrated that CD4+ T cells have lower concentration of active GPx and SOD and have a high concentration of H2O2 (86). Therefore, other strategies to replenish antioxidant molecules are being actively pursued by researchers worldwide.
2. Influenza
Influenza virus, an orthomyxovirus family of RNA viruses, infects the epithelial cells lining the throat and lung. Several studies show that influenza virus infection leads to changes in pro-oxidant levels and oxidative stress (204). Based on animal studies, cells lavaged from the lungs of influenza virus-infected mice have been shown to possess an enhanced superoxide generation capacity (222). Moreover, xanthine oxidase is overexpressed in these mice, suggesting that influenza infection leads to oxidative stress. Reports also suggest that influenza virus-infected cells show lower levels of GSH (203).
Influenza virus is also known to cause neutrophil dysfunction and activate neutrophil respiratory-burst responses. Teff cells are responsible for controlling inflammation in the lungs during influenza infections by producing anti-inflammatory cytokines such as IL-10 (271). Changes in redox regulation in Teff cells during influenza infection may affect the onset of disease. When transgenic mice expressing human Trx1 were infected with influenza virus, NFκB activation and production of higher amount of TNF-α and IL-6 were shown to increase inflammation and severity of the disease (88). Another study using NOX2-deficient mice infected with influenza virus showed a decrease in titers of virus in comparison to WT. However, NOX2 deletion does not show any difference in CD8+ Teff cells. Moreover, this study confirmed that treatment with the NOX2 inhibitor, apocynin, has the ability to reduce viral titer, inflammation of the respiratory tract, and cell superoxide production (296). Taken together, these studies suggest that influenza infections change the redox balance of T cells.
G. Aging
Aging and age-related diseases, including cancer, Alzheimer's disease, atherosclerosis, and metabolic disorders, are associated with low-grade inflammation, oxidative stress, and production of NFκB-dependent proinflammatory cytokines, such as IL-1, IL-6, and TNF-α. While the aging process has been associated with the decline of adaptive immunity, referred to as immunosenescence, innate immunity appears to be upregulated, leading to the expression of proinflammatory cytokines. Moreover, NFκB signaling, NAD-dependent deacetylase sirtuin 1 (SIRT1), and p53 have been implicated as key regulators of aging and age-related diseases (249, 317). NFκB has been further shown to act as a link between the innate and adaptive immunity in the aging process, and age-dependent activation of NFκB signaling is tissue specific (2, 250).
The aging process appears to shift the T-cell population from CD45RA+ naïve T cells to CD45RO+ memory cells, but these T cells have impaired antigen responsiveness (161, 250). Furthermore, CD4+ T-cell-mediated activation of B-lymphocytes and the decrease in the number of CD8+ T cells are observed in the aging process, contributing to the downregulation of adaptive immunity in the aged and age-related diseases. Recently, an in vivo model of spontaneous arthritis in aged mice suggested that NAPDH oxidase 2 (NOX2) deficiency induced the production of proinflammatory cytokines, reduced ROS, and increased the number of IL-17-producing Th17 cells while decreasing the Treg population (155). Several other studies show aging-associated shift in production of proinflammatory cytokines (IL-17, IL-1β) associated with coronary heart diseases (54). Moreover, a study by Daynes et al. has shown that this imbalance, increased proinflammatory cytokine production, may be due to an impairment of peroxisome proliferator-activated receptor-α (57). Taken together, aging may induce imbalance in production of ROS, which leads to cytokine imbalance, thereby increasing susceptibility to various disorders. Moreover, the Th17 and Treg balance may be important in regulating the downstream immune response associated with aging. As previously mentioned, aging is associated with impaired T-cell function due to increased protein and DNA damage (220). T cells exhibit diminished TCR signaling in aged individuals, and this T-cell dysfunction has been attributed to ROS-mediated damage to cellular components.
During the aging process, adaptive immune response is decreased, which has also been attributed to the oxidative stress-induced shortening of the telomeres of T- and B-lymphocytes (136). Similarly, chronic oxidative stress has been shown to reduce the telomere length in human endothelial cells, leading to the premature senescence of these cells. Based on these studies, it is possible that age-related T-cell dysfunction may be due to this shortening of the telomere in T cells (268). Furthermore, CD4+ and CD8+ T and B cells have shortened telomeres in association with age progression. That is, with age, telomere shortening is observed in T cells, and more importantly, the rate at which telomeres are lost is different between the two T-cell populations. Based on these recent findings, telomere integrity of T cells as well as oxidative stress induction in these cells are important in regulating the aging process and in regulating the progression of age-related disease.
H. Gender-related differences in the oxidative stress response and T-cell immunity
Gender disparity in redox imbalance and susceptibility to apoptotic signals results in the increased risk of cardiovascular pathogenesis (174), asthma (171), melanoma (127), and lung cancer (287). Whether or not the gender-dependent regulation of oxidative stress and apoptosis is associated with T-cell immune response in these diseases is unknown and warrants further investigation. However, these studies on gender-related pathogenesis further suggest that female hormones play a significant role in regulating autoimmunity. For example, T-cell chemokine response is regulated by estrogen expression, and the chemoreceptors are important for T-cell homing (i.e., to the spleen) as well as T-cell response to antigen stimulation (190). Based on the results of this study, female mouse-derived CD4+ T cells overexpress CCR1-CCR5 and exhibit increased tyrosine phosphorylation in response to estrogen and MIP-1β stimulation, respectively. However, the molecular mechanisms involved in inducing expression of chemokine receptors on T cells in response to estrogen stimulation are currently under investigation.
It is well known that estrogen is an important factor in determining female gender bias in autoimmune diseases. Estrogen has further been implicated in regulating iNOS mRNA, iNOS protein, and nitric oxide expression in activated T cells (133). Moreover, an increased level of nitric oxide is associated with tissue injury in autoimmune diseases that predominantly manifest in females, such as RA, MS, SLE, and glomerulonephritis. While moderately high levels of nitric oxide protect immune cells from apoptosis, chronic infections or pathologies can induce very high levels of nitric oxide expression, resulting in immune cell apoptosis or necrosis. Interestingly, after injury, estrogen stimulation can lead to the dysregulation of cell-mediated immune responses by modulating proinflammatory cytokine expression, such as TNF-α, IL-1β, and IL-6 (28). Similarly, estrogen binds to the estrogen receptor on T cells, and T-cell activation is enhanced in female patients with SLE (236). This upregulation of T-cell activation results in impaired regulation of autoantibody production, thereby enhancing the overall immune response in female SLE patients. These studies, therefore, support gender-dependent responses in susceptibility to oxidative stress, apoptosis, and T-cell immune response.
VIII. Gene Mutation and Polymorphism in Oxidative Stress and Diseases
Recent discoveries of potentially causal single-nucleotide polymorphisms (SNPs) and advancements in the use of high-throughput genotyping techniques for complex diseases hold great promise. This has led to large-scale genetic association studies such as the HapMap (haplotype mapping) Project and the Cancer Genome Project. Such studies should be helpful in the future in the prognosis of human diseases and should guide clinical decisions in treating human diseases. It is well known that SNPs can modulate protein expression, thereby effecting disease susceptibility. SNPs and mutations in antioxidant genes may lead to the modulation of the cellular redox state, effecting T-cell activation and/or T-cell proliferation. Moreover, individuals with diverse SNPs will respond differentially to T-cell therapy. Therefore, investigating SNPs in antioxidant and redox-regulating genes is of critical importance in the diagnosis, prognosis, and treatment of human diseases.
Genetic studies have shown that polymorphic variants of antioxidant genes may also increase susceptibility to lymphoma (Table 4). Ishikawa et al. showed that two mutations (G13886A and 13884insC) in ND6 (the gene responsible for coding NADH subunit 6) resulted in a deficiency in respiratory complex I activity and is associated with overproduction of ROS (118). The mutation-bearing mice had greater tumor progression and metastasis; however, when treated with ROS scavengers, metastasis was suppressed. Mutations in antioxidant genes have been shown to be associated with ROS imbalance and are therefore associated with increased disease susceptibility (89). For example, mutations in the catalase gene are associated with diabetes mellitus, hypertension, and vitiligo. Interestingly, gene polymorphisms in redox regulation genes such as cytochrome b light chain (CYBA) and aldoketo reductase family 1, member A1 (AKR1A1) show increased risk to T-cell and non-Hodgkin's lymphoma (153). Moreovoer, the ser/leu polymorphism in the NOS2A gene modulates risk for B- and T-cell lymphoma by twofold (302). Similarly, mutations in human SOD1 have been shown to cause an inherited form of ALS (257). Moreover, a variant of the promoter region of the catalase gene shows increased risk for vitligo in Chinese people, suggesting that catalase is important in regulating apoptosis of melanocytes (162). Another recent study implicated mitochondrial ROS in the production of proinflammatory cytokines in an autoinflammatory disorder caused by missense mutations in the TNFR1 gene, known as type 1 TNF receptor (TNFR1)-associated periodic syndrome (TRAPS) (35). This study suggested that TNFR1-mutant cells exhibit altered mitochondrial function with enhanced oxidative capacity and mitochondrial ROS generation. Pharmacological blockade of mitochondrial ROS efficiently reduced inflammatory cytokine production after LPS stimulation, suggesting that mitochondrial ROS may be a novel therapeutic target for TRAPS and other inflammatory diseases. The above studies suggest that a mutation or polymorpism in antioxidant genes could play an important role in disease susceptibility.
AKR1A1, Aldoketo reductase family 1, member A1; CAT, catalase; CYBA, cytochrome b-245, alpha-polypeptide; MPO, myeloperoxidase; NADPH, nicotinamide adenine dinucleotide phosphate-oxidase; Ncf1, neutrophil cytosolic factor 1; NHL, non-Hodgkins lymphoma; NOX, NADPH oxidase; NQO1, NADPH quinone oxidoreductase-1; NRF2, nuclear factor erythroid-2-related factor 2; PON1, paraoxonase-1.
Antioxidant gene polymorphisms may also increase susceptibility to several autoimmune diseases and lymphomas (Table 4). Polymorphic variants in antioxidants and redox-regulating genes lead to differential susceptibility to diseases. This may be due to up- or downregulation of antioxidants. For example, cytochrome P450 2E1 (variant -CYP2E1*5) is associated with increased risk to ALL by 2.8-fold, when compared to individuals with the WT alleles (150). Moreover, individuals with gene variants of paraoxonase-1 (PON1) enzyme have shown to have better CD4+ T-cell counts in comparison to individuals with the WT allele of PON1 (219). Table 4 briefly discusses gene polymorphisms in redox regulators that are associated with increased susceptibility to the corresponding disease.
IX. Therapeutic Strategies to Overcome Oxidative Stress-Induced Diseases
Recent studies have also focused on development of therapeutics by targeting the antioxidants that regulate the cellular redox state to restore proper T-cell function. In fact, we and others have used antioxidants to rescue T cells from oxidative stress (207). Our data suggest that pretreatment of melanoma epitope-reactive MART-127–35 and influenza matrix protein MP58–66 with MnTBAP rescues them from repetitive TCR stimulation-induced cell death by quenching ROS species and inhibiting JNK phosphorylation (207). In another study, in vivo administration of MnTBAP protected antigen-specific T cells from contraction after chronic antigen exposure in primary lymphocytic choriomeningitis virus (LCMV) infection (154). Another widely used antioxidant compound is NAC, a cysteine prodrug that replenishes intracellular GSH (14). NAC has been used successfully to treat GSH deficiency in acetaminophen toxicity, bronchitis, Alzheimer's, diabetes, cystic fibrosis (232), and HIV infection, (103, 176). Impaired T-cell function in cancer patients is associated with decreased expression of IL-2R as well as impaired responsiveness to anti-CD3, all of which could be restored with NAC treatment as seen in in vitro experiments. Therefore, restoration of GSH levels may restore T-cell function and antigen responsiveness with the treatment of NAC.
With recent advances in molecular techniques, efforts have been made to increase the cellular expression of antioxidant genes in T cells. Based on a recent study, CD4+ and CD8+ T cells retrovirally transduced with a catalase gene preserved the function of the T cells and evaded H2O2-mediated cell death, with marked resistance to ROS (11). These results have raised promise for gene therapy-based strategies to elevate the antioxidant capacity of Teff cells. Doing so could be important for increasing cell persistence in an oxidative tumor microenvironment, which may subsequently improve immunotherapy for patients with advanced cancer or chronic viral infections. Similar strategies have been used to protect cells from oxidative-stress-induced injury, where adenovirus-delivered SOD and CAT genes are overexpressed in ischemic lung tissue (56), cortical neuronal cells (80), and retinal pigment epithelial cells (234). Targeted delivery of catalase has also been used as a strategy to inhibit tumor metastasis, since H2O2, at sub-lethal concentrations, can act as intracellular second messengers to increase the transcription of genes that regulate the proliferation of tumor cells in metastatic lesions (206). Therefore, catalase can regulate ROS-mediated tissue injury and tumor metastasis. In addition to catalase, inhibitors of molecules involved in oxidative stress signaling have been used in studies where inhibitor treatment results in impaired T-cell function and promotes tumor progression. Inhibitors that target arginase 1 (Arg 1), NOS2, or peroxynitrate scavengers are able to block the immune suppressive capacity of MDSCs, and thereby restore specific T-cell responses in mouse tumor models (32, 33, 59, 152). Interestingly, inhibitors of the iNOS-peroxynitrate pathway have also been shown to enhance memory responses and block AICD in both mouse and human T cells (305). Moreover, the data presented in this study are consistent with other data, suggesting that free radicals are important in the maintenance of immune memory, and that iNOS is important in maintaining T cell homeostasis (305).
Dietary products and supplements are also known for their antioxidant properties and could potentially be useful as therapeutic agents (3, 122). The active antioxidants in dietary products, such as green tea, carrots, turmeric, and other vitamins, can modulate the T-cell immune response (Table 3). The well-studied curcumin (extracted from turmeric) induces antitumor activity in T-cell leukemia by blocking the JAK-STAT pathway (231). Based on in vivo studies, curcumin is known to restore circulating CD4+ T cells and IL-2 production (142) and to induce the STAT5a-mediated expression of the antiapoptotic protein Bcl2 (27), suggesting that reduced rates of apoptosis may be an underlying mechanism by which restoration of circulating T cells is achieved.
Similarly, specific vitamins have antioxidant function (Table 3). Vitamins A and D are required for proper homing of T cells to the gut and skin, respectively, which requires the expression of specific chemokine receptors (182). Another example of a strategy to target the harmful effects of ROS on T-cell function is the administration of high doses of dietary Vitamin E, a known antioxidant (98, 173). Based on these results, dietary Vitamin E supplementation, followed by chemotherapy treatment, increased the number of IL-2- and IFN-γ-producing T cells as well as increased NK-cell activation, thereby suggesting that Vitamin E supplement is helpful in improving immune function in these patients. Moreover, Vitamin E has been shown to suppress the activity of transcription factors NF-κB and AP-1, and suppressed CD95L mRNA expression leading to the protection of T cells in HIV-1-infected individuals (173). Therefore, the use of dietary supplements as antioxidants is a major area of research, and their role as immune modulators, as well as anti-inflammatory and anticancer agents, makes them promising candidates for future therapeutics.
Another useful method for modulating oxidative stress in T cells could be through micro-RNA-regulated expression of ROS-associated genes. miRNA are short noncoding RNA, 18–24 nucleotides in length that post-transcriptionally regulate gene expression by affecting the degradation and translation of target mRNAs (97). Efforts to gain new insights into understanding the role of miRNAs in regulating oxidative stress-related gene expression in different cell systems are being conducted, including auditory cells (303) and cardiac myocytes (47). Similarly, the effects of ROS on miRNA expression, the role of miRNAs in ROS-mediated gene expression and T-cell function, and as potential therapeutic targets are of current interest. Interestingly, a recent study has indicated that miRNA 128a regulates production of ROS by inhibiting the Bim-1 oncogene in cancer stem cells and thereby promotes cellular senescence (294). A role for miRNA-21 in controlling NO-mediated apoptosis has also been shown in endothelial cells that were subjected to shear stress (304). In addition, miR144/miR-451 protects erythrocytes from oxidative stress by a 14-3-3z- (phospho-serine/threonine-binding protein) and FoxO3-mediated mechanism (319). Megenta et al. demonstrated that miR-200c and miR-141 are upregulated in oxidative stress and play key roles in ROS-induced apoptosis of endothelial cells (169). While it is not known if miR144/miR-451- or miR-200/miR-141-mediated pathways are involved in protecting T cells from oxidative stress, recent evidence suggests that miR-155 inhibits IFN-γ signaling in CD4+ T cells (19). Interestingly, miR155 is also important in maintaining Treg homeostasis by targeting the suppressor of cytokine signaling 1 (SOCS1) protein in a Foxp3-mediated pathway, suggesting that miRNAs are important in regulating T-cell function (166). Moreover, ROS-regulated miRNA (miR-27b) overexpression has been shown to suppress NFκB activation in mouse macrophage cells, RAW264.7 (281). Whether or not miR27b is involved in regulating NFκB activation in T cells remains to be determined. These studies highlight that miRNA may be important for maintaining redox homeostasis by regulating the expression of target mRNAs associated with ROS production. Thus, targeting miRNA to regulate oxidative stress and influence expression of targeted genes that are important in disease pathogenesis could be an important future strategy.
X. Conclusion
The studies described in this review reveal that redox balance is critical for modulating T-cell activation, proliferation, and persistence. A balance of various antioxidants is required for the regulation of the cellular redox status, such as GSH, vitamins, SOD, GPX, NOX, and p53. Proper redox status will lead to proper T-cell signaling and activation. However, an imbalance in redox molecules can activate different signaling pathways, ultimately shifting the T-cell phenotype (61). In addition, the differential susceptibility of T-cell populations based on the cell surface marker expression (as identified in sections II and III) is an area that needs further investigation in most disease states. Earlier studies have looked broadly at either CD4+ or CD8+ T cells without considering the vast heterogeneity (effector, memory, and regulatory) that exists in the T-cell lineage. Therefore, it would be important to consider a comprehensive characterization of these T-cell subsets that could potentially be correlated to disease pathogenesis and progression.
The studies cited in this review lead us to conclude that, despite the redundancy in factors that regulate cellular oxidative stress in other model systems, a combination of basic, translational, and clinical research may provide further insight in T-cell immunomodulation and immunotherapeutic strategies. Manipulation of the cellular redox state could be a strategy that results in the modulation of T-cell subsets, thereby improving current immunotherapeutic approaches to treat cancer, autoimmunity, and infectious diseases.
Footnotes
Acknowledgments
This work was supported by a grant from the NIH (R01CA138930 to SM) and start-up funds from Department of Surgery at MUSC. We apologize to our colleagues for not citing all primary research articles owing to space restrictions. We are thankful to Dr. Christina V. Johnson in the Department of Microbiology & Immunology at MUSC and Dr. Thomas G. Smith in Center for Academic Excellence/Writing Center, and Dr. Jennifer G. Schnellmann within the Scientific Editing and Publications Office at MUSC for their critical suggestions in preparation of this article.