
Abstract
Introduction
Oxidative stress
A more recent aspect among the above mentioned is the observation that ROS can induce an upregulation of proinflammatory genes (23, 59). This indirect mechanism in which reactive oxygen and nitrogen species act as signaling molecules shows the strong biological potency of these molecules. Many of the target genes are involved not only in inflammatory processes but also in cell aging or tumorigenesis such as p53 (23). Although these processes are yet not fully understood and seem to be much more complex in mammalian cells, oxidative stress is a key mechanism in the pathophysiology of a large number of inflammatory and neoplastic processes. It is regarded as an important factor, especially in severe inflammatory conditions such as acute pancreatitis and sepsis, as well as in chronic pancreatitis (9, 21, 56, 82, 85, 88, 105, 112, 114).
The cellular defense against oxidative stress is probably as complex as the detrimental multi-mechanistic toxicity of the ROS, offering a wide variety of possible therapeutic approaches. Grossly, they can be divided in merely molecular approaches that use a direct chemical redox reaction such as NO donors or vitamins, unspecific enzymatic reactions including especially the glutathione pathway, and specific enzymatic and genetic pathways that require a high level of cellular evolution and have not been used therapeutically.
In prokaryotes, sensing pathways for the detection of reactive oxygen species have been detected and characterized in detail (23). This implies a feedback mechanism, triggered by iron or sulfur-dependent conformational changes of transcription factors, consequently altering the associated DNA operator and leading to activation of defined genes (23). Regarding this background in prokaryotes, it seems coherent that evolutionary high organisms possess even more complex regulatory feedback mechanisms with unspecific, as well as specific and inducible pathways, to face oxidative stress and detoxify its molecular correlates.
Antioxidant agents
Antioxidants are defined as substances that have the capability to reduce oxidative stress—regardless of their origin—by scavenging reactive oxidative species. Various classes of antioxidant substances have been classified and evaluated in experimental as well as clinical studies over the last decades. These include molecules that act directly via a capability to detoxify oxidative species by a chemical reduction, amino acids that take part in enzymatic reactions, micronutrients that serve as enzymatic co-factors, as well as other substances that interfere with metabolic reactions such as the arachidonic acid pathway or expression of transcription factors that are activated during the inflammatory response. Table 1 gives an overview over the classes of antioxidants.
Vitamins
Three vitamins and their derivatives exert strong antioxidant effects, namely vitamin A (β-carotene), C (ascorbic acid), and E (α-tocopherol) (25, 36, 89, 115).
β-carotene is, in its natural form, an antioxidant that is effective especially in the combination with other vitamin-derived antioxidants, namely vitamin C and E. They act by binding free radicals and thereby attenuating their reactivity towards other lipids or protein structures (58, 77,121).
Ascorbic acid is the most commonly known and used antioxidant. Initially known as Vitamin C, ascorbic acid is a monosaccharide antioxidant that neutralizes reactive oxygen species directly by a reduction reaction and can additionally act as a substrate for the enzyme ascorbate peroxidase that detoxifies peroxides. However, this effect is described in plants and can not directly be transferred to the human metabolism (57, 66).
Vitamin E, α-tocopherol is a lipid-soluble antioxidant that protects membrane lipids from being oxidized by reacting with lipid radicals which can be produced during lipid peroxidation (76). By interrupting this chain reaction of peroxidation, tocopherol protects the integrity of cell membranes (48, 60).
Amino acids
Glutamine is an important nonessential amino acid that serves as a NO carrier and has effects on intestinal mucosa, immune function, and acid-base balance in a large number of disorders, which has been shown in numerous in vitro and in vivo studies (103). Glutamine can significantly attenuate pro-inflammatory cytokine release, protect against end-organ damage, and decrease mortality. It is one of the most commonly used additives in nutritional therapy, not only in acute pancreatitis but also in other conditions of severe systemic inflammations (103, 117).
N-Acetylcysteine is a molecule that serves as an antioxidant by binding radicals itself via its SH-group. In addition, it can serve as a donor that provides cysteine for the synthesis of glutathione (40, 54, 109).
S-Adenosyl-methionine and glutathione represent two agents that are regarded as the key substances in biological defense against reactive species. Both are highly metabolically active agents that take part in the cellular mechanisms of amino acid-based scavenging. S-adenosyl-methionine is a precursor of glutathione which can quickly be used for synthesis of cysteine and glutathione (32, 63). Glutathione itself contains three amino acids and is the molecule that can be oxidized under transfer to its dimeric derivative glutathione disulfide and exerts a great capability to detoxify reactive species by this process. Human cells contain a high amount of glutathione and recreate this pool by the activity of glutathione synthase, the key enzyme for this reaction (118).
Micronutrients
Selenium is a micronutrient that is present in all human tissues and is of essential function for various enzymatic reactions. It is usually bound to amino acids such as methionine for storage and cysteine in its biologically active form. The most important selenium-dependent enzymes are the glutathione peroxidases which protect cell membranes from oxidative damage, as well as the enzymatic reductases that are essential for protein conformation, transcription factor activity, and redox processes (49).
Omega-3 fatty acids
Based on the observation that polyunsaturated omega fatty acids play an important role in the metabolism of lipid mediators, namely arachidonic acids and eicosanoids, it has been hypothesized that omega-3 fatty acids exert an inhibitory function on inflammatory processes via the eicosanoid pathway (51). These lipids have the potency to inhibit the formation of omega-6 fatty acids-derived pro-inflammatory eicosanoids (e.g., prostaglandin and leukotriene derivatives). Furthermore, they can generate several potent anti-inflammatory lipid mediators (e.g., resolvins and protectins). The latter suppress the activity of nuclear transcription factors (e.g., NFκB) and inhibit the production of pro-inflammatory enzymes and cytokines, (e.g., COX-2, TNF-α, IL-1β). Therefore, nutritional supplementation with polyunsaturated omega-3 fatty acids has quite commonly achieved acceptance in daily nutritional recommendations, although high power studies to support these effects are still lacking.
Others
Allopurinol is an inhibitor of the enzyme xanthine oxidase which is responsible for the formation of superoxide radicals. Besides this indirect antioxidative effect, it has the capability to directly scavenge free hydroxyl radicals (1, 22). This can be regarded as a double—direct and indirect—protective effect against the oxidative stress mediated by these molecules.
Di-methyl sulfoxide (DMSO) is an antioxidant that has a direct protective effect against lipid peroxidation by its ability to scavenge reactive oxygen species. It has been found to regulate transcription factor activation in experimental models of sepsis (14, 15). However, a relevant toxicity has been attributed to this substance which has, after initially promising results in clinical settings, restricted its use mainly to in vitro and experimental applications (3, 65).
Curcumin is a spice-derived antioxidant, originally extracted from the yellow ginger-like Curcuma longa. It is composed of aromatic polyphenols, containing OH groups that are responsible for its antioxidative effect. Furthermore, it is an inhibitor of nuclear factor kappa B, which explains its strong anti-inflammatory, antiseptic, and anticancer activities (4).
Besides the above mentioned antioxidants, many others have been used in experimental approaches to examine and inhibit oxidative stress in acute and chronic pancreatitis. Yet, these studies have not led to further clinical trials and are therefore not relevant for the therapy of patients with AP or CP to date.
Pantoprazole, which is widely used as a proton pump inhibitor, possesses reactivity towards hydroxyl radicals (91). This mechanism is not the major aim in the routine use of this drug, but rather regarded as a side effect. Nonetheless, there are several studies that demonstrate effects of proton pump inhibitors on inflammatory conditions (67, 110), such as an inhibition of leukocyte migration and an interference with interleukin liberation as well as a protective effect in experimental AP (44).
Acute Pancreatitis
Clinical aspects
Acute pancreatitis (AP) can be caused by various etiological factors. About 80% of all cases are related to either bile stones or excessive alcohol consumption. Rare causes include metabolic disorders such as hypercalcemia or hyperlipidemia, as well as drug side effects or autoimmune disorders. Acute pancreatitis is characterized by inflammation of the exocrine pancreatic tissue (Fig. 1) and disturbance of pancreatic microcirculation (12). However, ischemia of the pancreas is not only a secondary phenomenon during the progression from mild to severe disease in the course of AP of other origin, but can also primarily induce AP as it is well defined for post-transplantation AP (26, 95, 107). Besides the transplantation setting, in which an ischemia-reperfusion-associated damage is obvious, various other conditions can be associated with pancreatic ischemia, leading to subsequent inflammation of the organ (2, 13, 28, 43, 79). Thus, other etiologies have to be ruled out to define pancreatic ischemia as the cause for AP. Ischemic acute pancreatitis is often not considered as a different entity of AP, although this has to be clearly differentiated as the prognosis is often poor and therapy remains difficult (2). Depending on the severity of acute pancreatitis of any etiology, irreversible perfusion failure with consecutive tissue hypoxia and necrosis complicate the course of the disease and trigger systemic inflammatory and septic complications (12).

Clinically, the mild edematous course, which is observed in about 85% of the patients and usually resolves without further complications, is not associated with any mortality. This mild course of AP has to be differentiated from the severe and necrotizing course of the disease, which affects the remaining 15% of all patients with acute pancreatitis (Table 2) (12). Despite all progress in intensive care medicine, the severe form of acute pancreatitis is still associated with a mortality of approximately 20%. Due to the limited pathophysiological understanding, therapy of acute pancreatitis remains symptomatic. The only causative approach is possible in gallstone pancreatitis when the initially obstructed bile duct that leads to a congestion of the pancreatic duct as well can be cleared by an extraction of the concrement with subsequent decompression. This can lead to complete relief of the symptoms if performed early. To prevent recurrence of the disease, early cholecystectomy is essential in these patients (98). In accordance with the international guidelines, the symptomatic therapy consists of supportive care with infusion therapy, pain medication, antibiotic treatment if indicated, ICU care, and organ replacement therapy with mechanical ventilation, hemofiltration, and cardiocirculatory support (99).
When perfusion failure of the pancreatic tissue has reached a macro-vascular level, necrosis becomes evident and can be easily visualized in contrast-enhanced CT scan. However, sterile necrosis is still a condition that can be therapeutically handled conservatively. When necrosis remains sterile, patients may recover with a residual and functionally active tissue amount that does not necessarily require endocrine or exocrine substitution. Alternatively to atrophy and finally disappearance of necrotic areas, the tissue defect can cause fluid collections that may remain as asymptomatic pseudocysts, but may also cause clinical symptoms due to compression of nearby structures, rupture, bleeding, or secondary infection that may lead to interventional or surgical therapy in the long-term course (42). In contrast to late pseudocyst infection, the critical step of early infection of necrotic tissue, which in general severely worsens the prognosis of the patient, has to be differentiated. Infection of pancreatic necrosis is usually diagnosed by CT-guided fine-needle aspiration and direct microscopic examination after staining (12). The supposed source of infection is the intestinal bacterial environment. Due to an intestinal barrier dysfunction, bacterial endotoxins reach the interstitial space and the circulation (37, 96). Therefore, the occurrence of infected necrosis turns the local event of a severe AP into a systemic disease that can affect all organ systems, most often the lung and the kidneys (12).
This conversion is—despite the theoretical advantage of a systemic antibiotic prophylaxis—not safely preventable (96). A large number of studies have been published with regard to this question during the last 2 decades (72). A recent Cochrane Database systematic (106) review has failed to give clear evidence, as all of the available studies that were included were underpowered. Only imipenem had an effect with regard to pancreatic infection, but also failed to reduce mortality. Consequently, today various guidelines from societies in different countries exist that show great differences in methodological quality (62).
The impact of surgical interventions has continuously decreased over the last 2 decades. Thus, the therapy of acute pancreatitis is a domain of conservative management today. Operative approaches are no longer recommended unless there are proven infected necrosis in the pancreatic or peripancreatic tissue as mentioned above or other life-threatening complications such as bowel perforation or bleeding (47). In case of infected necrosis, which is a secondary event caused by bacteria that translocate from the gastrointestinal tract (37), the therapeutic approach must be directed towards mechanical removal of infected necrotic tissue (47, 113). Organ-preserving necrosectomy is the surgical technique of choice for treatment of infected pancreatic and peripancreatic necrosis. Morbidity is low in techniques that provide postoperative exit channels for further slough and infected debris (continuous postoperative lavage, closed packing) (12, 113). In addition, there is general agreement that surgery in severe pancreatitis should be performed as late as possible, preferably 3–4 weeks after the onset of symptoms (10, 31, 113). The high mortality in infected pancreatic necrosis despite surgery has led to the development of several minimal invasive techniques, including radiological, endoscopic, and minimal invasive surgery as alternative procedures that gain more and more acceptance today (104, 113). A recently published randomized multicenter trial from the Netherlands showed a beneficial effect of a minimally-invasive step-up approach in the treatment of infected pancreatic necrosis compared to open surgery in terms of reduced major complications, although overall mortality was not reduced in the study collective (104).
Pathophysiology of acute pancreatitis
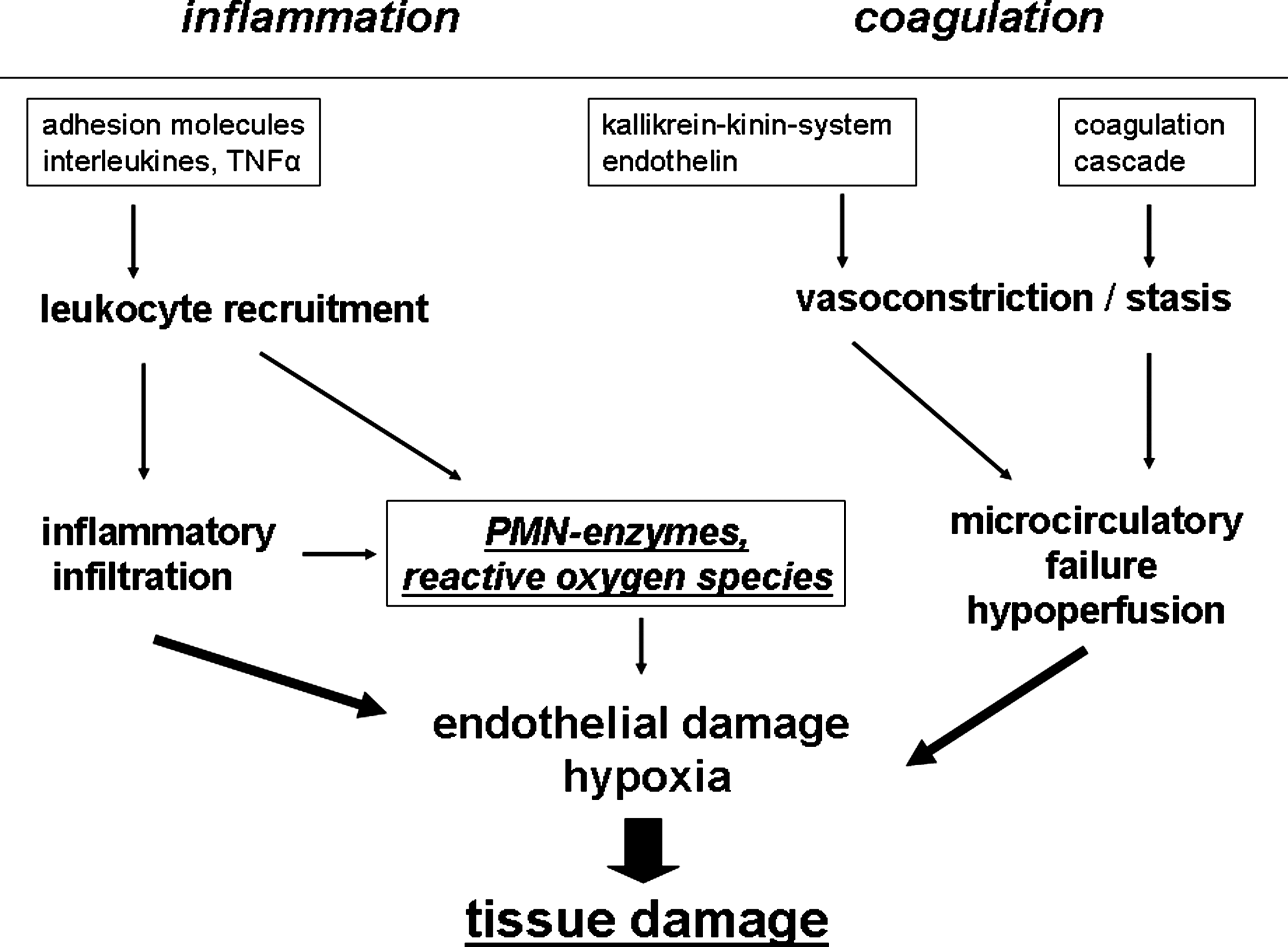
Different pathways of inflammatory and coagulatory proteins interact with various cell types, especially leukocytes and platelets, in the pathophysiology of AP (Fig. 2). Two striking features decide about the clinical course and the severity of acute pancreatitis: the development of systemic inflammatory response syndrome (SIRS) in the early phase of the disease, and the development of necrosis with subsequent superinfection of necrosis in the later phase with consecutive systemic septic complications including multiorgan failure and eventually the death of the patient. As described above, the mild edematous and self-limiting form of acute pancreatitis is usually uncomplicated with full recovery of the patient. This form is not associated with mortality. Therefore, the progression from edema and reversible hypoperfusion of the pancreas to ischemia and necrosis represents the key step in the pathophysiology turning a treatable disorder into a potentially lethal disease. Leukocyte–endothelium interaction is an early step of the inflammatory response and has been characterized as a central step in the pathophysiology of AP (45, 46, 55). The reversible events with margination of leukocytes from the blood stream and temporary adhesion to the endothelium have been described as a rolling motion of these cells and represent the precondition for the further firm adhesion, migration, and extravasation of the cells into the interstitial space, the morphological correlate of which is the inflammatory tissue infiltration (Fig. 3) (46, 78). Based on this knowledge, numerous clinical and experimental studies have focused on microcirculatory changes of pancreatic perfusion during acute pancreatitis (69, 111, 107). Attention was paid especially to erythrocyte flow patterns, leukocyte–endothelium interaction, and rheological approaches to reconstitute perfusion and inhibit irreversible tissue damage (55, 107, 123). Perfusion failure of the pancreas begins within the capillaries and proceeds to the larger vessels such as postcapillary venules and finally arteriolar and arterial vessels (95, 107). Two different pathophysiological pathways participate in this vicious circle, namely the inflammatory and the coagulation cascade. In addition, vasoactive mediators such as endothelin can aggravate perfusion failure by vasoconstriction of the precapillary vessels as well as systemic hypotension due to septic cardiocirculatory failure and interstitial fluid extravasation during severe acute pancreatitis (84, 95).

Since therapy of AP can not be started prophylactically in the clinical setting, all therapeutic approaches are limited with regard to an inhibition of certain pathophysiological steps. Antioxidants have been demonstrated to be beneficial in the experimental setting when applied prophylactically, but failed to improve survival in experimental pancreatitis when administered after a therapy-free interval. Moreover, this limits the translation of any experimentally generated data to a successful pharmacological intervention today. Patients usually present within 24–36 hours after the onset of symptoms. During this period, a lot of initial events in the inflammatory reaction have already taken place and some of them already triggered irreversible consequent steps. For this reason, therapy of AP to date remains merely symptomatic. A targeted causal interference is not yet possible and promising upcoming approaches to be introduced in the clinical practice are lacking.
In addition to the local inflammatory processes, remote effects such as pulmonary complications also determine severity and clinical course during early SIRS, as well as late sepsis in AP. The observation of platelet and leukocyte activation in the pulmonary microcirculation is accompanied by xanthine and xanthine oxidase activity as markers of neutrophil-generated reactive species, indicating oxidative stress as an important factor of tissue damage (29, 33 –35). Neutrophil tissue infiltration of the lung is an especially striking event during acute pancreatitis that explains oxidative stress. However, oxidative stress in the lung is not a monofactorial leukocyte-triggered process, but can be regarded as a positive feedback mechanism as reactive molecules themselves lead to an activation of other mediators, for example P-selectin, which has been shown in experimental studies (33). The correlation with P-selectin accumulation, increased myeloperoxidase activity, as well as superoxide radical generation such as H2O2 and increased activity of heat shock protein 72 in the lung or enzymes like poly-ADP ribose synthetase show that many different pathways of oxidative stress are strongly involved in these pathophysiological events (33, 35).
Recent clinical findings (17) strongly support the central role of myeloperoxidase during oxidative stress in AP, especially for remote effects like AP-associated lung injury that are triggered and promoted by this aggressive molecule. In 86 patients, serum myeloperoxidase levels during early moderate and severe AP were strongly elevated compared to healthy controls and correlated well with proinflammatory cytokine levels, lung injury, infectious complications, and disease severity.
After the role of local oxidative stress in acute pancreatitis was described about 25 years ago (85), a large number of experimental studies has dealt with this issue. Four central events are responsible for the toxic effect of reactive oxygen species in the pancreatic acinar cell: lipid peroxidation, protein modification, mitochondrial membrane depolarization, and DNA fragmentation.
Lipid peroxidation as one central aspect of cellular membrane damage (41) is attenuated in the experimental setting by melatonin (19, 30), with the effect of a restoration of cellular membrane integrity. These results suggesting a protective effect of melatonin have not yet been reproduced in the clinical setting of AP.
Oxidatively modified proteins have been observed as early as 30 min. after the onset of experimental AP (80) and have also been described in the clinical setting in the serum of patients suffering from severe AP (116). These structurally damaged proteins can lead to an impaired acinar cell function but are also observed in distant organs such as the lung (39) which may be an explanation for systemic organ failure and the beneficial effect of several systemically administered antioxidants among which N-ACC and other NO donors have been regarded as promising therapeutic agents due to their efficacy and low rate of side effects in the experimental setting (24). Disappointingly, these results could not be reproduced clinically, even when they were given prophylactically to prevent post-ERCP pancreatitis (53).
Mitochondrial membrane depolarization causes severe mitochondrial dysfunction and possibly cell death. Mitochondria are the central organelles for ATP generation via oxidative phosphorylation (52). Reactive oxygen species induce a depolarization of the mitochondrial membrane in acinar cells. This leads to an interference with physiological mitochondrial function and can consequently cause acinar cell necrosis (73, 74). The underlying mechanism is a calcium overload response with an inhibition of the plasma membrane Ca-ATPase (11). Consecutive membrane depolarization leads to a severe disturbance of cytochrome and ATP balance and can eventually induce irreversible cell damage (7, 11).
DNA fragmentation during AP has to be regarded as another severe event caused by oxidative stress (94). When this process reaches a damage level beyond the capacity of cellular of repair mechanisms, cell death is inevitable. The initiation of DNA fragmentation can be explained by oxidatively produced adducts of base and sugar residues, which may lead to single-stranded breaks as well as cross-links to other molecules and even double-stranded breaks (94). Physiologically, these irregularities can be corrected by intracytoplasmatic and intranuclear DNA repair proteins. When homeostasis of these regulatory proteins is disturbed or their function is impaired, the cell enters a state of vulnerability and can not restore normal DNA structure due to impairment of its defense strategy. In the experimental setting, this mechanism has been demonstrated in pancreatic acinar cells exposed to oxidative stress (94). Furthermore, not only acinar but also endothelial cells underlie these pathomechanisms (6), resulting in endothelial dysfunction, which may play an additional role especially in edema generation and cell transmigration in AP.
A special focus must be put on the time course during the pathophysiology of AP. As mentioned above, numerous serious steps take place within the first hours after onset of AP that determine the severity of the disease. This can be seen in the early increase of inflammatory markers such as interleukins 6, 8, and 18 (70, 122) and the impairment of pancreatic microcirculation that occurs as early as 6–8 hours after onset of AP (45). In the clinical setting, markers of inflammation increase within the first 3 days (70). The most useful markers are IL-6, IL-8, tumor necrosis factor (TNF-alpha), C-reactive protein (CRP), and procalcitonin (PCT) (5, 70, 81). In the clinical routine, especially PCT and CRP are used as they can predict a severe course with the highest accuracy (81, 87). All of these markers increase on the first day after the onset of symptoms which demonstrate the early and systemic response to local pancreatic pathological effects. However, parallel to the inflammatory changes, visceral afferent sensory neurons are stimulated in this early phase of the acute process (93). These afferent inputs are transmitted to the spinal chord and the higher sensory centers, resulting in the typical clinical symptom of severe abdominal pain radiating to the back. This symptom is mostly the first clinical manifestation of AP and still represents a therapeutic challenge (93).
Pain generation as an important aspect of AP can be addressed with regard to oxidative stress and consecutive cellular damage from various points of view.
First, pain generation is a consequence of the inflammatory response at the level of the injured tissue which fulfils the criteria of the nociceptive pain concept. Stimulation of nociceptors in the dendritic branches of sensory neurons creates electrical activity resulting in central nervous pain sensation (20, 86). Among others (e.g., adenosine, histamine, substance P), this stimulation is exerted by loss of pH as well as free radicals that modulate the interstitial environment (18, 101).
Second, mitochondrial activity is altered not only in acinar cells of the pancreas as mentioned above, but also in neuronal cells due to a depolarization of the mitochondrial membrane (108). This influences the coupling of mitochondrial function and neuronal activity as mitochondria play a central role in the neuronal metabolism (52). Third, oxidative stress modulates intraneuronal signaling via an interference with calcium and potassium currents (120). This observation provides an additional explanation for a possible pain reduction by reduction of oxidative stress.
Commonly used drugs that interact with these pathways are nonsteroidal anti-inflammatory drugs (NSAIDs) that are effective in the prostaglandin and eicosanoid pathways. The clinical benefit of NSAIDs can be regarded as an unspecific anti-inflammatory effect that mediates a reduction of reactive oxygen species, resulting in less nociceptive stimulation. There is no high evidence study that has ever compared NSAID application to other drugs in AP, yet NSAIDs represent a standard treatment in AP to supplement or replace stronger analgesics, following the WHO guidelines for pain management (20).
Clinical studies
In chronic pancreatitis, antioxidative treatment—especially for the most striking clinical feature of chronic, long-lasting, and therapeutically challenging pain—is well established and has been meanwhile investigated in larger randomized controlled trials (16) that favored a combination of selenium, methionine, vitamins E, C, and b-carotene (8). In contrast, therapeutic application of antioxidants in acute pancreatitis is much less evidence based and can not be supported by a comparable number of successful studies, which has led to a certain kind of therapeutic nihilism regarding this topic (50). However, it should be kept in mind that the pathophysiology of an overwhelming acute inflammatory condition can not be compared to a chronic situation which allows a much longer adaptation. Therefore, severe acute pancreatitis—in contrast to chronic pancreatitis—may require a multi-pragmatic approach in which antioxidants could play a certain role but must certainly not be regarded as a single therapeutic pathway of unlimited efficacy.
Seven randomized controlled studies have investigated antioxidants as a therapeutic approach in AP (71). In the monotherapeutic approaches, glutamine was used in four studies and vitamin C in one investigation. Overall, 166 patients with AP were included in these studies evaluating either placebo treatment or glutamine for 7–10 days. However, outcome in these studies showed heterogeneous results. The study by Xue et al. (119) that included 38 patients in each arm and represents the largest collective, showed very encouraging results with decreased rates of infections, organ dysfunction, surgical interventions, and even mortality. These results are not supported by the other three studies, including the one by Fuentes-Orozco et al. (38) who included 44 patients. In these studies, no difference with regard to mortality, hospitalisation, and infectious complications was detected between control and treatment group. Concerning vitamin C as a monotherapy, Du et al. (27) could demonstrate an improvement in the clinical course of AP in terms of fewer symptoms like vomiting and fever, combined with a faster improvement in laboratory parameters and a better long-term outcome with shorter hospitalization and less complications.
In an antioxidative combination treatment, Sharer et al. (90) administered S-adenosyl methionine and N-acetyl cysteine to 79 AP patients. This treatment failed to demonstrate any improvement in APACHE II score, complication rates, duration of hospital stay, and mortality. Comparable observations were made in a study by Siriwardena et al. (92) who included N-acetyl cysteine, selenium, and vitamin C in a triple therapy, which was not effective in any outcome parameter such as disease severity score, hospitalization, and mortality.
Another recent clinical trial by Sateesh et al. (83) investigated the effect of a combined antioxidant treatment on early AP under the hypothesis that an early intervention might have a beneficial effect on the systemic inflammatory response syndrome (SIRS) and may prevent further related complications. Based on previous findings that showed increased levels of oxidative stress in the early phase of AP compared to healthy volunteers (98), their RCT included 53 patients within 72 h after the onset of symptoms. Thirty were treated with a standard approach, 23 received additional therapy with vitamin C, N-acetyl cysteine, and antoxyl as an oral preparation with an observation period of 7 days (83). Length of hospital stay and biochemical markers of oxidative stress were defined as outcome criteria. They could show a tendency towards shorter hospital stay and significantly reduced oxidative stress marker levels. Despite these encouraging results, the study was clearly limited due to the small number of patients, and pain intensity was not explicitly investigated as an outcome parameter.
In a meta-analysis on the effects of antioxidative nutritional support on the clinical course of AP, McClave et al. (68) chose nutrition indices, stress markers, and markers of the inflammatory and immunological response as outcome measures for potential beneficial effects and analyzed 27 RCT on this topic. Major conclusions of this study were that enteral nutrition offers benefits in terms of infectious morbidity and length of hospital stay with a tendency towards reduced organ complications, but no influence on mortality in comparison to parenteral nutrition.
This was at least partly attributed to decreased oxidative stress, as specific supplements such as arginine, glutamine, omega-3 polyunsaturated fatty acids, and probiotics were associated with a positive impact on patient outcome. However, the meta-analysis failed to show an effect of enteral nutrition when compared to standard treatment without nutrition.
In conclusion, no clear clinical treatment recommendation was concluded from these observations, although the favorable effect of early nutrition by supplementation with modulators of inflammation and systemic immunity seems reasonable. Still the results of all available studies are heterogeneous; none of the applied antioxidative agents could demonstrate a reproducible beneficial effect on the course and severity of AP and its complications in high-quality trials. Therefore, from the data available today, antioxidative treatment can not be recommended as a clinical standard treatment.