
Abstract
NADPH oxidase is known to modulate the arterial tone, but the role of its specific subunits is still unclear. The objective of this study was to compare the role of p47 and gp91phox (NOX2) on artery dilatation. We conducted a multicenter study enrolling 30 patients with chronic granulomatous disease (CGD) (25 with NOX2 deficiency and 5 with p47phox deficiency) and 30 healthy subjects (HS), matched for gender and age, in whom flow-mediated dilation (FMD), serum activity of NOX2 (soluble NOX2-derived peptide [sNOX2-dp]), urinary isoprostanes (8-iso-PGF2α), and platelet production of isoprostanes and NOX2 were determined. Compared to HS, patients with CGD had significantly higher FMD and lower sNOX2-dp and 8-iso-PGF2α levels. Compared to patients with NOX2 deficiency and HS, patients with p47phox hereditary deficiency had intermediate FMD and oxidative stress, that is, higher and lower FMD and lower and higher isoprostanes compared to HS and patients with NOX2 deficiency, respectively. In agreement with this finding, an ex vivo study showed higher inhibition of NOX2 activity and lower isoprostane formation in platelets from patients with NOX2 deficiency compared to platelets from ones with p47phox deficiency. Our observations lead to the hypothesis that oxidants are implicated in artery vasoconstriction. Antioxid. Redox Signal. 18, 1491–1496.
Introduction
Chronic granulomatous disease (CGD) is a very rare genetic disorder (1:250,000 individuals) characterized by life-threatening infectious diseases (5, 7). It is characterized by defective activity of the innate immune system, caused by functional deficiency of the NADPH oxidase subunits (5, 7). Among the NADPH oxidase subunits, the functional deficiency of gp91phox (NOX2), the catalytic subunit of NADPH oxidase localized on cell membrane, is the more-frequent hereditary disorder (<70%) transmitted with an X-linked transmission (5). Conversely, the prevalence of p47phox (one of the cytosolic subunits of NADPH oxidase) deficiency is much less (<30% of CGD) (5); thus, the Italian register for primary immunodeficiency documented only 5 patients with this latter autosomal recessive form of disease (5). When compared to X-CGD, p47phox deficiency is characterized by a milder clinical course and by longer survival, but the reason is still unclear (5, 7).
Innovation
Herewith, we report that patients with hereditary deficiency of NOX2 and p47phox, the catalytic and cytosolic subunits of NADPH oxidase, respectively, have enhanced artery dilatation compared to controls. There was a parallel behavior between oxidative stress and artery dilatation as compared with patients with p47phox deficiency, and those with NOX2 deficiency disclosed lower oxidative stress and higher artery dilatation. These findings reinforce the hypothesis that oxidative stress is implicated in artery vasoconstriction and suggest a different impact of NADPH oxidase subunits in modulating the arterial tone. These data may have potential implication in developing a new therapeutic approach to improve artery dilatation.
Several experimental studies have shown a pivotal role of NADPH oxidase in modulating arterial tone (1). Thus, NADPH oxidase is one of the most important cellular producers of superoxide anion, which blunts NO or inhibits NO synthase (1). Accordingly, an increased arterial dilation in NADPH oxidase knockout animals compared with wild-type animals was observed (1). These results are consistent with a multicenter study on X-CGD showing that NOX2 is implicated in the modulation of human arterial tone via reduced oxidative stress and enhanced NO generation (8).
The role of p47phox on arterial dilatation in humans has never been fully investigated. Previous study provided indirect support to its potential role as a vasoconstrictor molecule, but direct evidence is still lacking (1).
Therefore, the aim of this study was to analyze the different impact of p47phox and NOX2 on oxidative stress and artery dilatation. For this purpose, we conducted a multicenter study enrolling patients with NOX2 and p47phox hereditary deficiency, in whom flow-mediated dilatation (FMD) and oxidative stress were determined.
Results
Clinical characteristics of CGD and HS are reported in Table 1. There were no differences in terms of age, gender, and risk factors of atherosclerosis between CGD and HS. Compared to HS, patients with CGD had significantly higher FMD and lower intima-media thickness (IMT) (Table 1). No difference was found between the brachial resting-vessel sizes of the two groups.
p values in bold are statistically significant; italicized p values are not statistically significant.
CGD, chronic granulomatous disease; FMD, flow-mediated dilation; IMT, intima-media thickness; CRP, C-reactive protein.
Different oxidative stress was detected between the two groups. Thus, compared to HS, urinary excretion of 8-iso-PGF2α and soluble NOX2-derived peptide (sNOX2-dp) levels were lower in patients with CGD (Table 1). Correlation analysis carried out by Spearman test showed that FMD inversely correlated with sNOX2-dp (Rs=−0.648, p<0.001; Fig. 1A) and urinary excretion of 8-iso-PGF2α (Rs=−0.387, p=0.002; Fig. 1B).

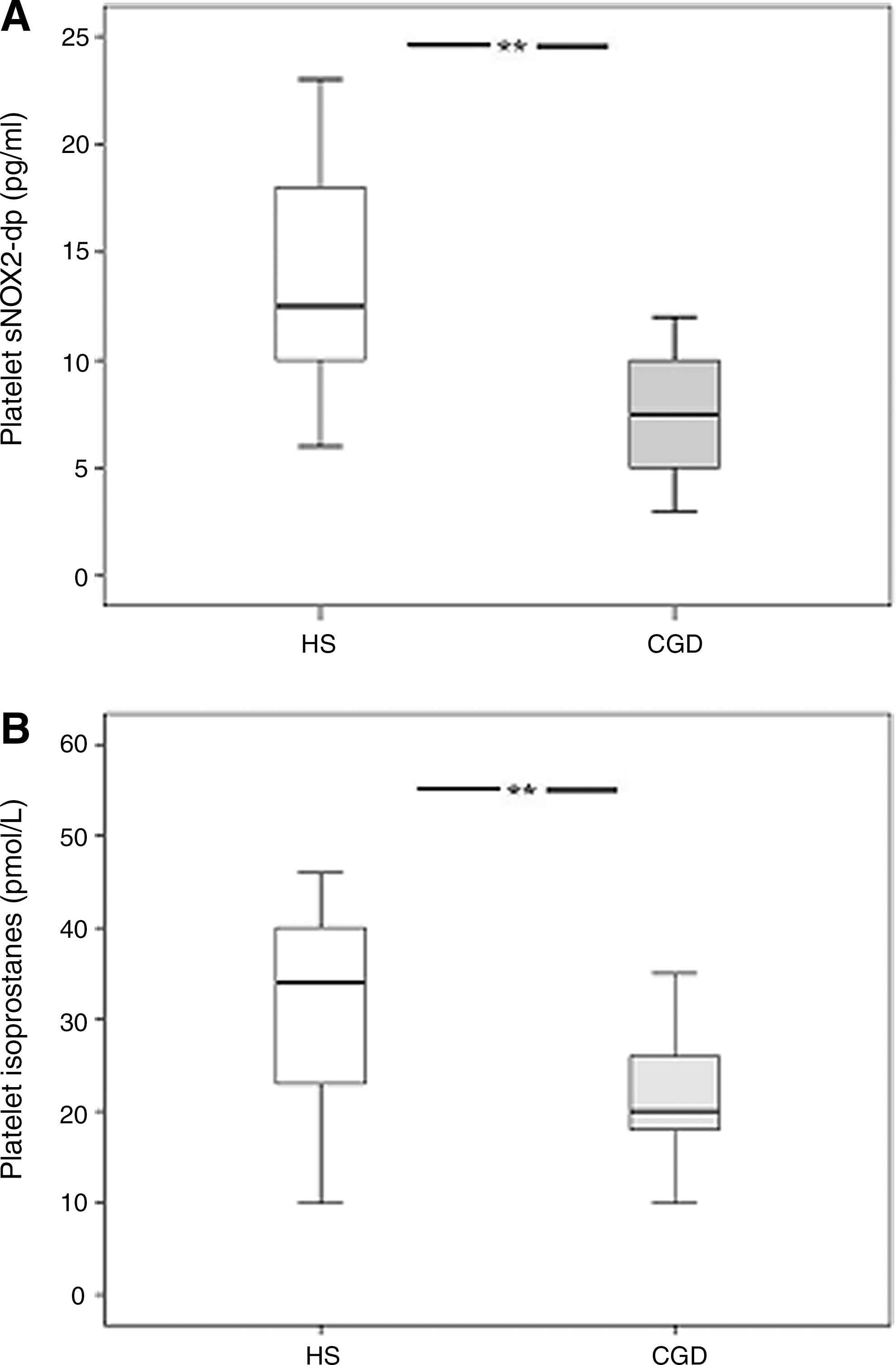
These data were supported by an ex vivo study that was performed in patients with CGD and HS to investigate platelet formation of isoprostanes and platelet sNOX2-dp. Compared to HS, patients with CGD had significantly lower sNOX2-dp concentration and 8-iso-PGF2α formation (Fig. 2A, B).
To explore if there were differences between patients with hereditary deficiency of NOX2 and p47phox, a substudy comparing the two groups and HS was performed. Clinical characteristics of patients with NOX2 deficiency, patients with p47phox deficiency, and HS were similar with no significant differences among them (Table 2). Compared to HS and patients with NOX2 hereditary deficiency, those with p47phox hereditary deficiency had intermediate changes of FMD and oxidative stress (Table 2 and Fig. 3A). Thus, patients with p47phox hereditary deficiency had higher and lower FMD compared to HS and patients with NOX2 deficiency, respectively (Fig. 3A). No significant difference of IMT was found among the three groups (Table 2 and Fig. 3B). Also, patients with p47phox hereditary deficiency had higher urinary isoprostane excretion compared to patients with NOX2 deficiency, but lower compared to HS (Table 2 and Fig. 3C).

Expressed as median (interquartile range).
p values in bold are statistically significant.
In accordance with this finding, patients with p47phox hereditary deficiency had higher and lower sNOX2-dp compared to patients with NOX2 deficiency and HS, respectively (Table 2 and Fig. 3D).
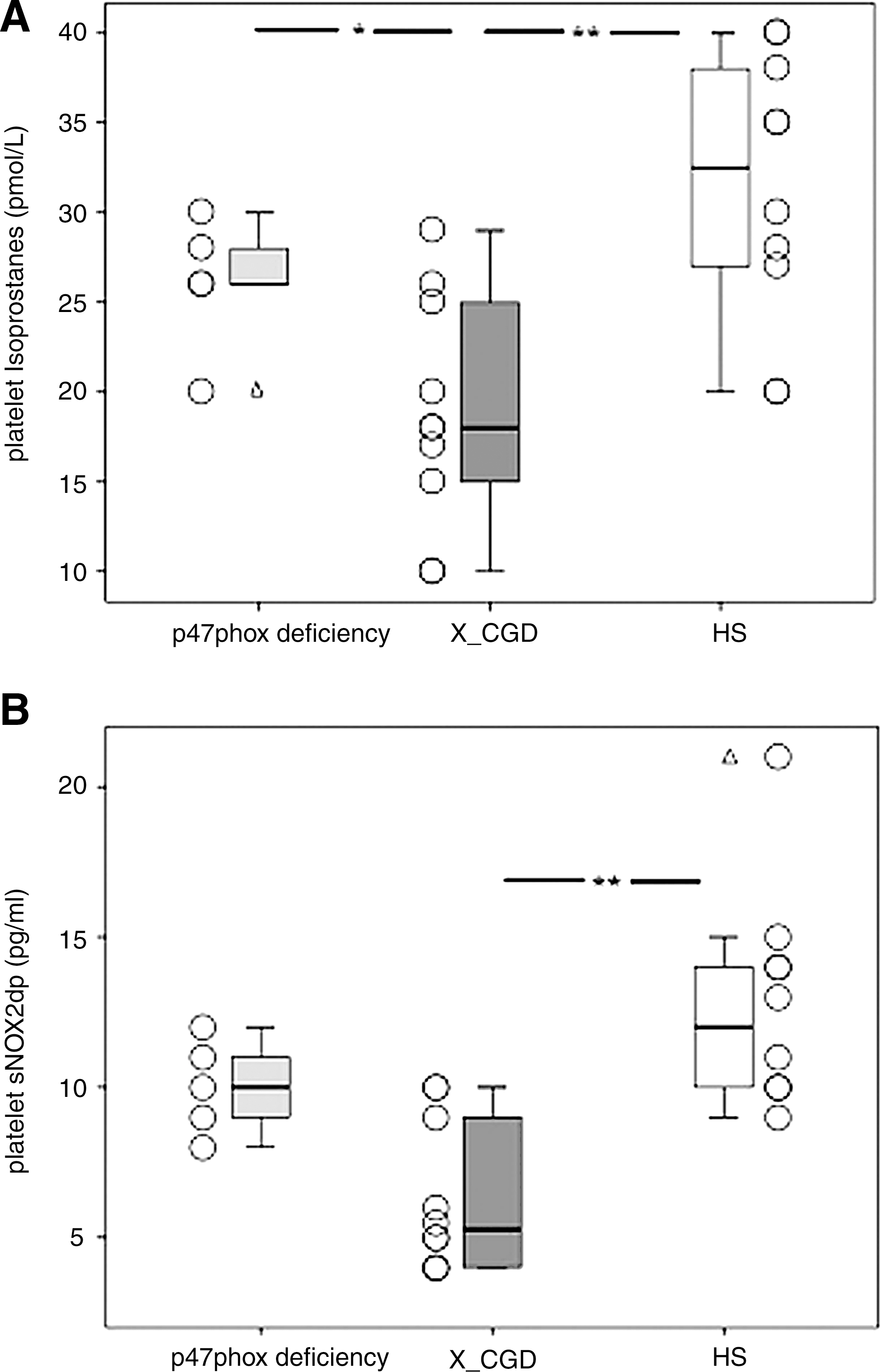
These data were supported by an ex vivo study that showed higher and lower platelet isoprostanes in patients with p47phox deficiency compared to patients with NOX2 deficiency and HS, respectively (Fig. 4A); also, patients with p47phox deficiency showed higher and lower platelet sNOX2-dp compared to patients with NOX2 deficiency and HS, respectively (Fig. 4B).
Discussion
This study provides evidence that the hereditary deficiency of specific NADPH oxidase subunits has different impact on artery dilatation among patients with CGD. In particular, patients with hereditary deficiency of p47phox showed lower FMD compared with patients with NOX2 deficiency. As patients with p47phox deficiency disclosed higher generation of reactive oxygen species (ROS) compared to ones with NOX2 deficiency, our data suggest that artery dilatation is negatively influenced by oxidative stress.
Previous studies demonstrated that activation of NADPH oxidase negatively influences vascular tone (1, 8); thus, patients with CGD, who are affected by hereditary deficiency of NOX2, disclosed enhanced FMD, while obese patients, who had NOX2 upregulation, disclosed impaired FMD compared to controls (8). This finding suggested that oxidative stress is one of the factors regulating artery dilatation in humans, as oxidative stress was decreased in patients with CGD and increased in obese patients.
In the present study, we further extend the concept that oxidative stress is implicated in modulating artery dilatation by investigating different subgroups of CGD. Thus, CGD is an interesting clinical model to explore the relationship between artery dilatation and oxidative stress because the hereditary deficiency of NADPH oxidase subunits may be associated with a different rate of ROS formation. Accordingly, the present study shows that patients with hereditary deficiency of the cytosolic subunit p47phox express more activation of NADPH oxidase and produce more isoprostanes than patients with NOX2 hereditary deficiency. These findings were corroborated by an ex vivo study showing more profound inhibition of NOX2 activity and isoprostane formation in platelets from patients with NOX2 deficiency compared to platelets from patients with p47phox deficiency. An important implication of these data is that the deficiency of the catalytic subunit of NADPH oxidase, that is, NOX2, elicits deeper reduction of oxidant species compared to the deficiency of a cytosolic subunit such as p47phox deficiency. This likely explains why patients with p47phox hereditary deficiency experience a milder clinical course than patients with NOX2 hereditary deficiency (3, 7).
This different impact of the two NADPH oxidase units on oxidative stress is useful to interpret the behavior of artery dilatation in the population with hereditary deficiency of the two subunits. Thus, while our study confirms that patients with CGD, globally considered, have enhanced FMD, analysis of FMD in the two groups with hereditary deficiency of p47phox or NOX2 showed a different behavior in as much as patients with NOX2 hereditary deficiency had higher FMD compared to patients with p47phox hereditary deficiency. As the rate of oxidative stress was higher in patients with p47phox deficiency compared to ones with NOX2 deficiency, these findings imply that oxidative stress strongly influences artery dilatation and support experimental studies indicating that oxidative stress plays a pivotal role in modulating the arterial tone (1). In accordance with the hypothesis that oxidative stress negatively influences artery dilatation, FMD was indirectly correlated with either sNOX2-dp or urinary excretion of isoprostanes. As oxidative stress is implicated in reducing the activity and biosynthesis of NO, which has a key role in artery dilatation (2), an implication of our study is that the activity and/or biosynthesis of NO may be differently modulated in patients with p47phox and NOX2 hereditary deficiency; however, we have no data that directly support such hypothesis, and further study is necessary to explore it.
The study has implications and limitations. An important limitation of the study is the sample size of patients with p47phox hereditary deficiency. We recognize that this is a potential drawback of the study, but the prevalence of this hereditary deficiency is so low that it would not be possible to study this population in a single country. Therefore, a multicenter study involving more countries is necessary to support our results. For this reason, we believe that our data, indicating that patients with p47phox hereditary deficiency have enhanced FMD compared to controls, but lower FMD compared to patients with NOX2 hereditary deficiency, should be considered preliminary and warrant further investigation.
An implication of the study is that modulating NADPH oxidase activity may represent a novel tool to enhance artery dilatation. However, the extension to which NADPH oxidase activity may be reduced without interfering with the activity of innate immune system is a critical issue that should be taken into account in future. Based on the clinical history of patients with p47phox hereditary deficiency, the inhibition of this specific NADPH oxidase subunit could have lower negative impact on the innate immune system compared to the inhibition of NOX2, but further study is necessary to explore such hypothesis. Furthermore, the impact of other NOX isoforms such as NOX1, NOX4, and NOX5 on artery dilatation should be investigated in vivo to explore their interplay with NOX2 activity.
Conclusion
The analysis of two genetic models associated with a different production of oxidative species further supports that NADPH oxidase-generated ROS have a role in eliciting artery vasoconstriction. The fact that artery vasoconstriction is related to the rate of ROS formation suggests that inhibiting specific NADPH oxidase subunits may be a novel future approach for modulating artery dilatation.
Notes
Methods
Study population
We conducted a multicenter study in collaboration with the Italian Primary Immunodeficiency Network. Among the 60 patients with CGD registered in the National database (5), 30 were not included in the study due to the presence of acute infections or critical physical conditions or unwillingness to participate in the study. The remaining 30 patients, who were NOX2 (n=25) or p47phox (n=5) deficient, were included.
X-CGD was diagnosed as previously described (5). All patients with X-CGD were under treatment with itraconazole, trimethoprim, and sulfamethoxazole. HS matched for gender, age, and atherosclerotic risk factors were screened from routine visits. Subjects were excluded from the study if they had liver insufficiency, serious renal disorders (serum creatinine >2.8 mg/dl), cancer, myocardial infarction, unstable angina, acute cerebrovascular disease, deep venous thrombosis, or were in treatment with statins or antioxidant vitamins or if they were current smokers.
The study was approved by the Ethics Committee. Each subject enrolled gave informed consent to participate in the study.
Blood sampling
After overnight fasting (12 h) and supine rest for at least 10 min, blood samples were collected in vacutainers between 8 and 9 a.m. (Vacutainer Systems, Belliver Industrial Estate) and centrifuged at 300 g for 10 min to obtain supernatant, which was stored at −80°C until use.
Urinary and platelet 8-iso-prostaglandin F2-α and serum and platelet nitrite/nitrate assays
Urinary and platelet 8-iso-Prostaglandin F2-α and serum and platelet nitrite/nitrate were measured as previously described (6, 9).
Serum and platelet sNOX2-dp
sNOX2-dp, a marker of NADPH oxidase activation, was detected in serum and platelets by ELISA method as previously described by Pignatelli et al. (6).
FMD and carotid IMT
Ultrasonography assessment of FMD and IMT was performed as previously described (4).
Statistical analysis
Data are presented as mean±standard deviation (SD) unless indicated otherwise. Categorical variables were reported as counts (percentage); independence of categorical variables was tested by χ2 test. The correlation analysis was carried out by Pearson correlation test. Student's t-test for unpaired data was used for the comparison of mean values. We performed a linear mixed-effect models to compare means across the groups. We used subject-specific random intercepts that were assumed to arise from Gaussian distributions, with clusters of random effects identified by the matched triplets (patients with p47phox hereditary deficiency, patients with X-CGD, and controls). The group indicators were included as fixed effects. Results were further confirmed by nonparametric tests with the rank transformation.
Statistical significance was defined at p<0.05. Statistical analysis was performed with SPSS 18.0 for Windows (SPSS, Inc., Chicago, IL).
Sample size determination
On the basis of the data emerged by previous studies (8, 9), we computed the minimum sample size with respect to a two-sample Student's t-test, considering as (i) relevant difference for FMD variation to be detected between the patients with CGD and controls ≥5%, (ii) SDs homogeneous between groups=3%, and (iii) type I error probability α=0.05 and power 1−β=0.90. This resulted in a minimum sample size of nine subjects for each group. Sample size calculations were performed using software nQuery Advisor®, version 5.0, (Statistical Solutions, Saugus, MA).
Footnotes
Acknowledgment
This study was supported by a grant from the University of Rome “La Sapienza” (PRIN 2008) (funds to F.V.).