
Abstract
Introduction
This review addresses several aspects of mitochondrial (dys) function and the involvement of mitochondria in aging, and AD is also discussed. Special attention is given to mtDNA and its repair mechanisms.
Mitochondria: Cell Keepers or Executioners?
The survival of eukaryotic cells greatly relies on mitochondrial function. The classical appraisal of mitochondrial function is based on energy-producing capacity. Nevertheless, the importance of mitochondria to the cells is far more complex and includes a number of functions that span from energy production, calcium (Ca2+) homeostasis, and production of second messengers, to the control of apoptotic cell death (Fig. 1). In addition, the canonical view of mitochondria as bean-shaped organelles has been revoked and redefined to a more dynamic perspective, fusing, dividing, and moving within cells (50). Mitochondria are able to change from a network-like appearance, forming long tubules, to a more individualized state, appearing similar to small round vesicles. The stimuli that alter this equilibrium toward highly branched or completely fragmented morphology are linked to the cell compartmentalization, developmental stage, stress stimulus, and the functional state of the mitochondria, among others (14). Disturbing either mitochondrial fission or fusion may affect mitochondrial membrane stability with possible negative consequences for ETC functionality (38, 116, 40).
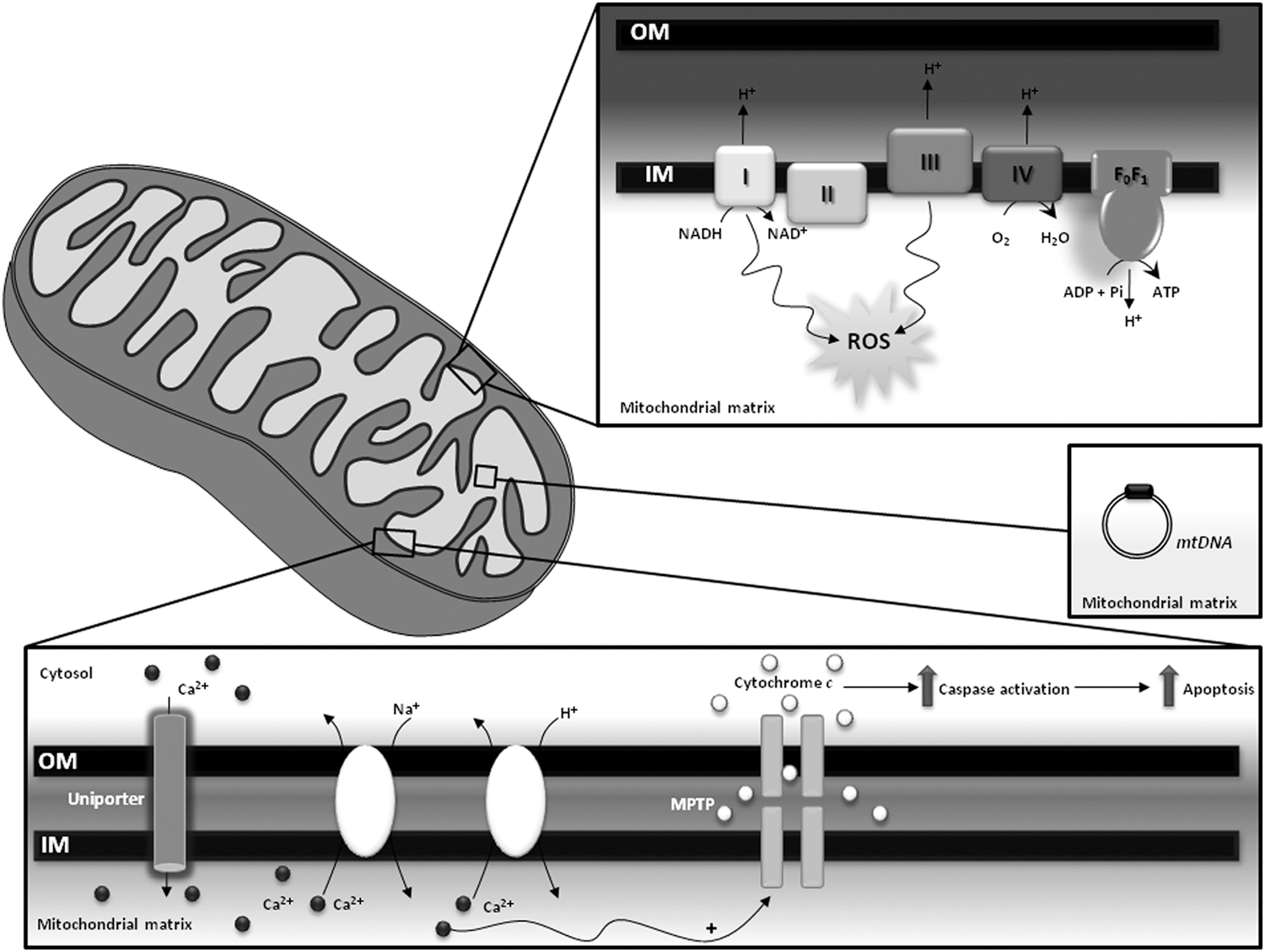
Mitochondrial bioenergetic production depends on the formation of a “protonmotive force,” which is generated through the extrusion of protons to the intermembrane space driven by the electron flow throughout ETC, from complexes with lower to complexes with higher oxidation potentials. Protons are driven back to the matrix through the ATP synthase during ATP production (52). Although the electron flow through ETC complexes is a very efficient process, a small amount of superoxide anions (O2 •−) is produced, due to electron leak mostly from complexes I and III (163, 56, 33, 10). At low/moderate levels, ROS act as second messengers within cells; however, exacerbated ROS production is deleterious for the cell, contributing to a variety of pathological processes (192, 1). Redox imbalance will be further discussed in a subsequent section of the article.
Mitochondria are also intracellular buffers of cytoplasmic Ca2+, thus playing a key role in normal neurotransmission, short- and long-term plasticity, excitotoxicity, and regulation of gene transcription, processes that are highly dependent on Ca2+ levels (35, 152, 208, 153, 210, 169, 154, 203). Ca2+ is internalized into mitochondria via the Ca2+uniporter, a protein that is still to be fully identified and biochemically characterized. Nevertheless, a candidate protein, which was named MCU (from “mitochondrial Ca2+uniporter”), proved to be essential for high-capacity Ca2+ transport into mitochondria in a number of in vitro and in vivo experimental models (13, 48). On the other hand, Ca2+ release is mediated by Na+/Ca2+ or H+/Ca2+ exchangers (203). It was shown that mitochondria are involved in cells' Ca2+ buffering impairment, a situation which occurs in the aging brain and AD (26, 29). The impairment of Ca2+ homeostasis is intimately associated with mitochondrial permeability transition (MPT). MPT is potentiated by oxidative stress, high phosphate concentrations, and adenine nucleotide depletion and is characterized by the opening of a high conductance pore known as mitochondrial permeability transition pore (MPTP) that enables the release of ions and solutes from the matrix to the cytosol (209, 44). The MPTP eventually culminates in cell death due to the release of proapoptotic factors such as cytochrome c and apoptosis-inducing factor (80, 189, 150).
ROS Imbalance in Aging and Alzheimer's Disease
Endogenous production and scavenging of ROS
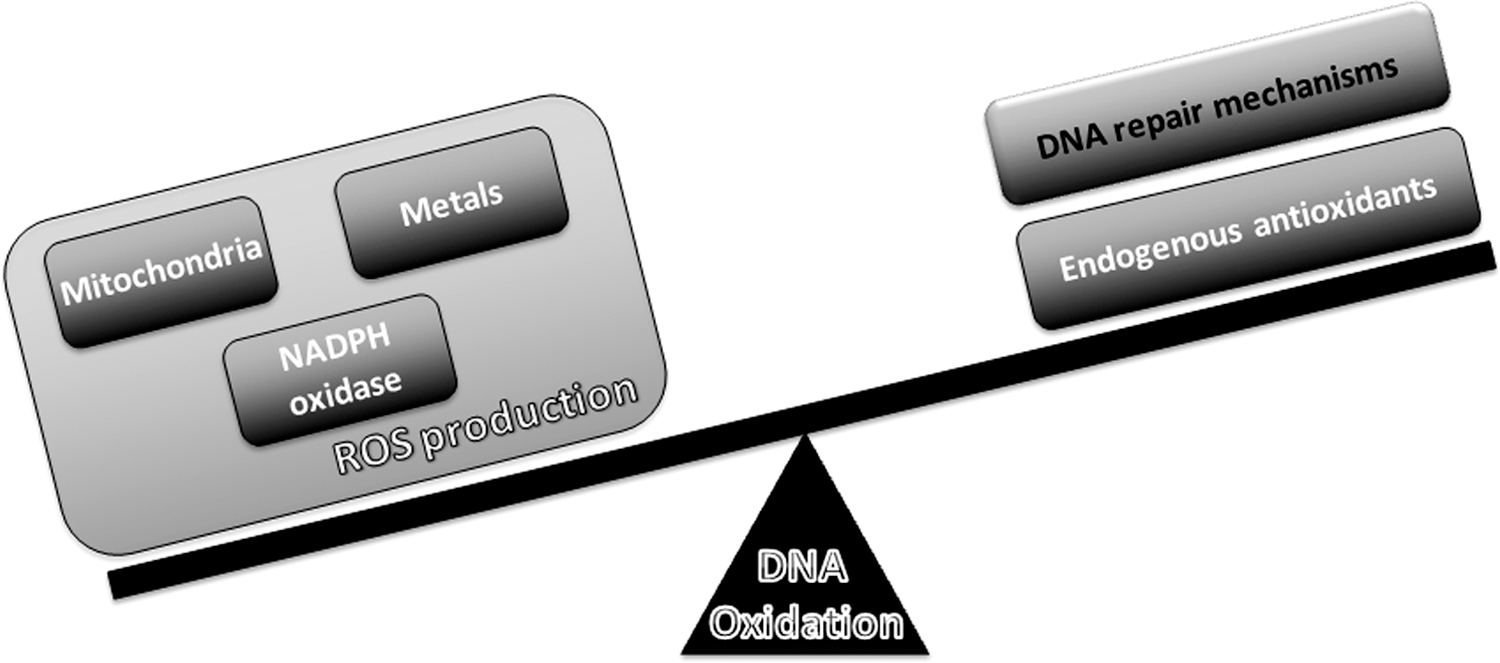
The balance between ROS production and scavenging enables cells to achieve a physiological equilibrium where the levels of free radicals might play a role in cell transduction (178). ROS interfere with the macromolecules of cells; however, under physiological conditions, the cells' quality control systems are able to overcome this damage, avoiding the development of a pathological state (159). During aging, the quality control systems become defective, resulting in an accumulation of damaged components, which, accompanied by a redox disequilibrium, may elicit a pathological condition (156).
In cells, there are multiple sources of ROS, including mitochondria, nicotinamide adenine dinucleotide phosphate (NADPH) oxidase (NOX), xanthine oxidase, and nitric oxide synthase (NOS) (147). Mitochondria are recognized as the hub of ROS production during normal aerobic activity. The electrons leak from the ETC directly to molecular oxygen, producing short-lived free radicals such as O2 •−(133, 191). While complex I releases O2 •− only to the matrix, complex III releases O2 •− to both the matrix and intermembrane space (23). O2 •− can be converted into nonradical derivates such as hydrogen peroxide (H2O2) either by a spontaneous dismutation reaction or catalyzed by the manganese superoxide dismutase that resides in the mitochondrial matrix (73). H2O2 can be converted into hydroxyl radicals (•OH) through the Fenton reaction. In the Fenton reaction, a molecule of H2O2 reacts with ferrous iron (Fe2+) to generate ferric iron (Fe3+), hydroxide anion (OH−), and •OH. Fe3+ can be reduced by O2 •−, generating a redox cycle in which the O2 •− facilitates the Fenton reaction by making Fe2+ available (92). Similar to iron, copper also participates in the Fenton reaction, which exacerbates ROS production (60, 85, 157). •OH can also be produced by a direct reaction of O2 •− with H2O2, a reaction known as the Haber–Weiss reaction (92). Mitochondria consubstantiate a microenvironment that is highly enriched in iron, as many mitochondrial enzymes possess heme groups and iron-sulfur clusters in their active centers, making them favorable locations of •OH production (128). Hence, mitochondria are prone to oxidative damage and particularly susceptible to •OH-mediated oxidation, which plays a major role in DNA oxidation. Apart from the ETC, several other sites in the mitochondria have also been reported to generate O2 •−, including pyruvate dehydrogenase, α-ketoglutarate dehydrogenase (171), glycerol-3-phosphate dehydrogenase, and fatty acid β-oxidation (23). Recently, important advances toward understanding mitochondrial ROS generation have been made. Transient quantal O2 •− flashes were observed in excitable cells such as neurons, which are associated with and required for the opening of MPTP, which represents a new facet of mitochondrial ROS (57, 198). To counteract an exaggerated production of ROS, mitochondria possess a very efficient antioxidant system, including glutathione peroxidase, catalase, and peroxiredoxin III, which are responsible for converting H2O2 to water (71).
As mentioned earlier, another source of cellular ROS is the NOX family proteins that are enzymatic complexes which catalyze the electron transfer from NADPH to molecular oxygen and generate O2 •− and its downstream reactive species (16, 65). NADPH oxidase is composed of cytochrome b558 (an heterodimer comprising a 22-KDa alpha-subunit-p22phox-and a glycosylated approximately 91-KDa beta-subunit-gp91phox), several cytosolic proteins (p47phox, p67phox, and p40phox), and the Rac G-protein. According to the new terminology, the NOX family refers to the catalytic subunit of NADPH oxidase, and these include NOX2 and its six homologs (NOX1, NOX3, NOX4, NOX5, DUOX1, and DUOX2)(65). It is known that NOX1, NOX2, and NOX4 are expressed in neurons, astrocytes, and microglia. Under normal circumstances, NOX is latent. However, on stimulation, NOX is translocated to the membrane and forms an heterodimeric enzymatic complex with cytochrome b558 that catalyzes the reduction of molecular oxygen to O2 •−(16).
In this way, compromised mitochondrial functioning, NOX overactivation, or the failure of free radical-scavenging systems could constitute critical events underlying oxidative damage in brain aging and AD.
Oxidative stress in the aging brain
Aging is an inevitable biological process that is characterized by a progressive decline in physiological function, including cognition, and by the increased susceptibility to disease, representing a major risk factor for the development of AD (36, 76). Oxidative stress and mitochondrial malfunction are two interdependent mechanisms that play a central role in brain aging (36). The brain is particularly vulnerable to oxidative damage as a consequence of its high levels of polyunsaturated fatty acids, high oxygen consumption, high content in transition metals, and poor antioxidant defenses (139). Compelling evidence reports that the aging brain is associated with the accumulation of markers of proteins, lipids, and DNA oxidative damage (37, 61, 66, 78, 166, 28). It was previously shown that the aged brain is characterized by increased levels of protein carbonyls, 3-nitrotyrosine, thiobarbituric acid reactive substances (TBARS), and diminished content of cardiolipin and protein thiols (41, 67, 160).
Along with oxidative stress, mitochondrial dysfunction also contributes to the aging brain. The most important functional deficits documented in aged brain are the loss of the mitochondrial membrane potential and OXPHOS capacity, decreased respiration and ATP synthesis, and increased susceptibility to MPTP opening (9, 22, 41, 58, 144).
Oxidative stress in Alzheimer's disease
AD is the most prevalent age-related neurodegenerative disorder that affects approximately 35 million people worldwide (149). Clinically, AD is characterized by the progressive loss of cognitive function and behavioral disturbances (149). These traits are accompanied by two distinctive pathological features, the massive deposition of aggregated amyloid-β (Aβ) peptide in the extracellular space as senile plaques, and the presence of intracellular neurofibrillary tangles, mainly composed of hyperphosphorylated tau protein (34, 131).
The pathogenic road map leading to AD pathology is still not entirely understood; however, multiple pieces of evidence support the key involvement of oxidative stress and mitochondrial malfunction in the onset and progression of the disease (129, 155, 180, 181). Oxidative stress is manifested by the occurrence of elevated levels of oxidatively modified lipids, proteins, and nucleic acids in vulnerable brain regions of AD subjects when compared with age-matched controls (18, 107, 120, 122, 141). Indeed, increased levels of lipid peroxidation products, such as TBARS, malondialdehyde, 4-hydroxy-2-nonenal (HNE), and F2-isoprostanes, were documented in the AD brain, particularly in regions where senile plaques and neurofibrillary tangles typically accumulate (106, 118, 119, 148, 158, 206). With regard to protein oxidation, AD is characterized by increased levels of protein carbonyls and widespread nitration of tyrosine residues in brain cortex and hippocampus (81, 112, 167). An increase in 8-hydroxyguanine (8OHG) and 8-hydroxy-2-deoxyguanosine (8OHdG), markers of RNA and DNA oxidation, respectively, and protein adducts were observed in brain regions that were most affected by AD pathology (108, 140, 142, 156). The role of oxidative stress in AD is further reinforced by the existence of a defective antioxidant defense system (5, 11). A decrease was documented in the activities of the antioxidant enzymes copper/zinc superoxide dismutase (Cu/ZnSOD) and catalase in the frontal and temporal cortex of AD subjects (118). AD subjects also exhibit reduced total antioxidant capacity (176), and a negative correlation was observed between the total antioxidant capacity and the duration of the disease (72).
During the course of AD, oxidative damage is also coupled to a progressive decline of the mitochondrial function (127). This notion is supported by an extensive literature which reports that AD is characterized by reduced cerebral energy metabolism (8), impaired activities of the tricarboxylic acid cycle enzymes (25, 121, 162), and defects in the mitochondrial ETC (21, 32, 45, 146, 96, 193). The most consistent defect at ETC level is the decline in cytochrome c oxidase (COX) activity, an effect that is positively correlated with Aβ concentration, as determined by in vitro studies (30). During AD progression, Aβ is translocated toward mitochondria (88, 186), enabling its interaction with critical redox centers of the subunit I of COX (6, 7) and Aβ-binding alcohol dehydrogenase (ABAD) (111, 187). The interaction of Aβ with the subunit I of COX and ABAD potentiates mitochondrial dysfunction and further increases ROS production in a vicious cycle. There is also evidence which supports a role for mtDNA mutations in the development and progression of AD (83).
Another important aspect is the role of redox-active metals in AD-related oxidative damage. Indeed, disruption of iron homeostasis has been suggested to be a trigger of oxidative stress and an early neuropathological event in AD (64). It was demonstrated that iron-mediated enhancement of oxidative stress occurs in preclinical AD (168), and increased redox-active iron is found in the cerebrospinal fluid from AD subjects (103). Besides its effects on oxidative status, redox-active metals also potentiate Aβ aggregation, aggravating AD pathology (27). Indeed, iron, zinc, and copper participate in the initiation of Aβ-mediated seeding process and Aβ oligomerization (86).
NOX overactivation is another pathogenic step underlying exacerbated oxidative damage in AD pathology (65). Mounting evidence suggests that the NOX system may be altered in AD, as indicated by the increased levels of p47phox and p67phox in the membrane fraction of AD brains, which foster the idea that NOX is overactivated in AD (55). Microglial expression of NOX subunit p22phox is also enhanced in the AD brain (3). A deficiency of NOX2 in transgenic AD mice reduces oxidative stress and improves cerebrovascular function and memory deficits without affecting Aβ levels or senile plaques (145), which reinforces the role of NOX in AD-associated oxidative damage. Importantly, aggregated Aβ stimulates O2 •− and H2O2 production in microglial cells and induces the translocation of Rac from the cytosol to the membrane, supporting the idea that Aβ can affect NOX2-mediated pathways (126, 200).
Overall, these findings indicate that mitochondria, NOX, and oxidative stress are important contributors in AD-related neurodegeneration.
mtDNA Oxidation and Repair Deficiency
mtDNA oxidation and repair mechanisms
Mitochondrial dysfunction and apoptosis can also be triggered by point mutations, nucleic acid modifications, and large-scale deletions in mtDNA (104, 100). It has been reported that mtDNA damage is 10- to 20-fold higher, more extensive and persists longer when compared with nDNA (175, 204). mtDNA is particularly susceptible to oxidative damage, because it is not compacted around histones and is localized near the ETC, which is a major source of ROS. In addition, mtDNA has none or few noncoding regions, increasing the chances of mutagenicity in coding regions (4, 156). Mitochondria are highly enriched in iron microenvironments, thus favoring the formation of •OH that, due to its short half-life, preferentially reacts with mitochondrial components, including mtDNA (192, 130). In addition, the oxidation of HNE can originate epoxide forms that interact with DNA bases (110, 91). During aging and in neurodegenerative disorders, nitric oxide (NO) interacts with O2 •−, resulting in the formation of peroxynitrite (ONOO−), which contributes to mtDNA damage, including single-strand breaks (182, 194, 190).
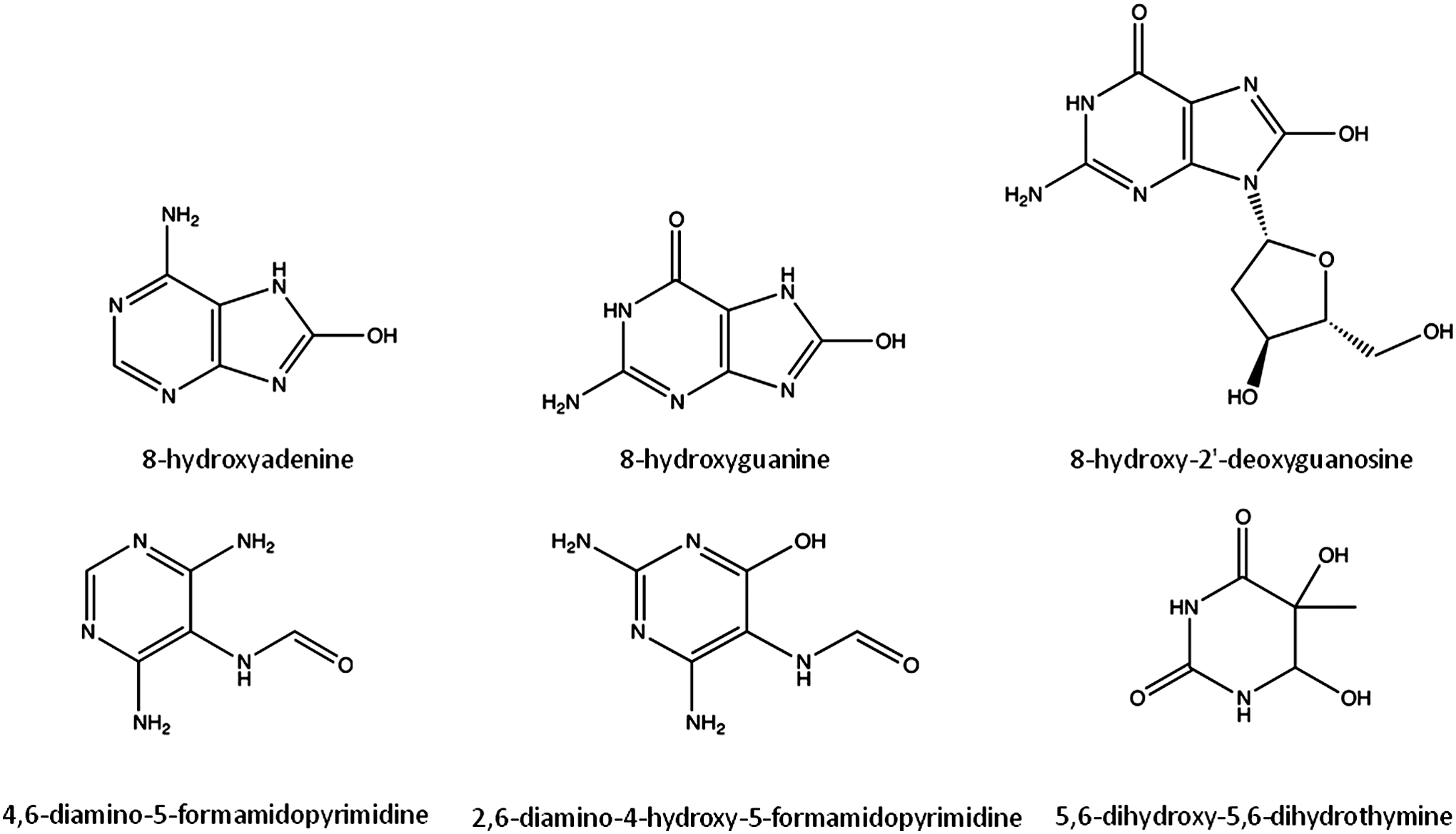
All four bases (purines- adenine, guanine; pyrimidines- cytosine, thymine) and the respective deoxynucleosides are highly susceptible to oxidative damage. The main products of DNA oxidation include 8-hydroxyadenine (8OHA), 8-hydroxyguanine (8OHG, and its deoxynucleoside equivalent, 8OHdG), 5,6-dihydroxy-5,6-dihydrothymine, and ring-opened lesions (4,6-diamino-5-formamidopyrimidine, FapyA, and 2,6-diamino-4-hydroxy-5-formamidopyrimidine, FapyG) (Fig. 2) (117). Overall, more than 20 oxidized base adducts can be formed from ROS attack on the DNA (42, 172). Nevertheless, guanine has the lowest oxidation potential, being the most readily oxidized base (130). 8OHG and 8OHdG, along with FapyG, are the most studied and common forms of oxidized DNA bases (53, 95). While mutagenesis is stimulated by the accumulation of 8OHdG by pairing with adenine as well as cytosine (113), the FapyG lesions inhibit DNA synthesis (143, 114).
Base excision repair (BER) is the primary nuclear and mitochondrial repair pathway for oxidative DNA damage. BER is evolutionarily conserved and is responsible for recognizing, excising, and replacing a wide number of DNA modifications that are characterized by small base modifications (99, 82). Generally, the BER machinery consists of several proteins that act in an ordered multistep cascade:(i) the recognition and excision of the damaged base;(ii) the incision of the DNA backbone in the abasic (AP) site; (iii) the generation of a 3′-OH and a 5′-P moieties in the DNA termini; (iv) the synthesis of the missing nucleotide; and (v) the sealing of the remaining DNA nick (Fig. 3) (205). This mechanism is essentially the same for nDNA and mtDNA repair; however, the isoforms of some enzymes involved in the process may differ from the nucleus to the mitochondria, even though all of them are nuclear encoded (199). The initial removal of the damaged base is accomplished by substrate-specific DNA glycosylases that hydrolyze the N-glycosidic bond between the modified base and the DNA backbone (54, 87). DNA glycosylases can be divided into two distinct functional groups: (i) a monofunctional group of enzymes with glycosylase activity only, which includes hydroxymethyl-uracyl DNA glycosylase (UDG) whose mitochondrial isoform UDG1 is generated by alternative splicing (31, 136); (ii) a byfunctional group of enzymes with intrinsic 3′AP lyase activity, in addition to glycosylase activity, which include 8OHG DNA glycosylase (OGG1), the human endonuclease III homolog (NTH1), and Nei-like homologs (NEILs)(68). Oxidized bases are generally removed by bifunctional DNA glycosylases. OGG1 has two isoforms, α-OGG1 that localizes to both the nucleus and mitochondria and β-OGG1that localizes in mitochondria (137). NTH1 has a putative mitochondrial targeting sequence, which allows its localization to mitochondria (185, 173, 94). NEILs are localized in the nucleus and mitochondria (77, 84, 132). In human cells, oxidative pyrimidine lesions are generally excised by NTH1 or NEILs; whereas oxidative purine lesions are excised by OGG1 (132, 77, 89). 8OHG lesions are primarily repaired by OGG1 (97, 47). The step after the removal of the damaged base by glycosylases is the incision of the DNA backbone in an adjacent site to the AP site. This stage is characterized by different types of lyase activity, either occurring immediately 5′ to the AP site or 3′ to the AP site depending on whether the excision step was accomplished by monofunctional or byfunctional glycosylases, respectively (49, 201). Indeed, AP endonuclease (APE1) is responsible for the incision of the DNA backbone after UDG1 removal of the modified base (49, 201). APE1 localizes to both the nucleus and mitochondria (62, 151, 202). Moreover, the byfunctional glycosylases are capable of incising the DNA backbone, leaving a DNA single-strand break. The final steps of the repairing process may undergo two distinct subpathways, the short- or long-patch BER (SP-BER or LP-BER, respectively). The SP-BER involves the incorporation of a single nucleotide into the gap by DNA polymerase. The LP-BER involves the incorporation of several nucleotides, typically 2 to 7, followed by the cleavage of the resulting 5′(91). Finally, the nick left behind by DNA polymerases needs to be sealed, a process performed by ligases, ligase I (nucleus) in the case of LP-BER, and ligase III (nucleus and mitochondria) in the case of SP-BER (70). The polymerase responsible for the mtDNA repair synthesis is polymerase γ (74, 93).
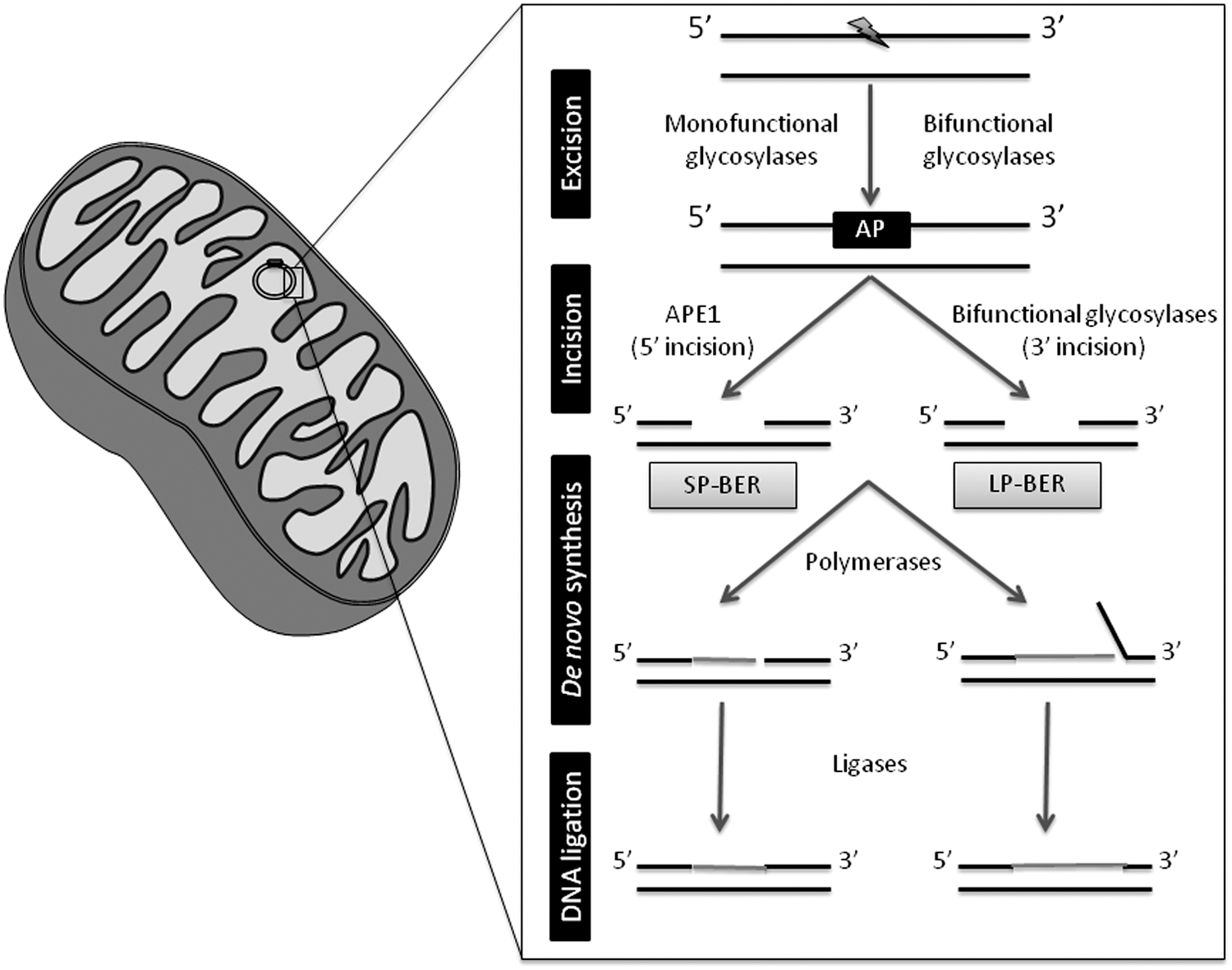
Despite the current knowledge on the mechanisms that maintain the genomic integrity, particularly mitochondrial genome, it is of great interest to gain more insight into the real importance of each enzyme and each subpathway involved in the repair process. Indeed, the repair of mtDNA oxidative damage was thought to be mediated solely by SP-BER (17, 174); however, in recent years, LP-BER was also demonstrated to counteract the accumulation of oxidative damage to mtDNA (Fig. 3)(2, 105, 184, 207).
Aging
Aging has been established as being the main risk factor for the development of late-onset neurodegenerative disorders such as AD. The accumulation of oxidative damage plays a key role in the aging process, as postulated by the free radical theory of aging (75). Age-associated oxidation of mtDNA results from an increased oxidative attack to the nucleic acids and a reduced efficacy in mtDNA repair machinery, namely BER (Fig. 4). Indeed, the aging brain is characterized by an increased oxidative damage to mtDNA noticed by the formation of 8OHdG, which is the most common marker of oxidative DNA damage (123). Notably, in human subjects (42–97 years), a progressive augment in 8OHdG was reported in both nDNA and mtDNA with aging; however, the extent of increase of 8OHdG is ten-fold more in mtDNA compared with nDNA (123). The increased susceptibility of mtDNA, compared with nDNA, was also observed in aged brains of other mammalian species (12). An age-associated impairment of mitochondrial BER machinery, particularly OGG1, UDG, APE1, and polymerase γ, has been reported (90, 39). Moreover, five specific brain areas were shown to have deficits in mitochondrial BER, namely caudate nucleus, frontal cortex, hippocampus, cerebellum, and brain stem (90). A recent study demonstrated that brain cortical and hippocampal mtDNA glycosylases behave differently in cortical and hippocampal mitochondria of rodents (68). Hippocampal mtDNA glycosylases present lower activity when compared with cortical glycosylases. Importantly, brain cortical mtDNA glycosylases show an age-dependent decrease in their activity; while hippocampal glycosylases present only minor alterations (68). These findings highlight how mitochondrial heterogeneity influences the susceptibility of these organelles to damage. In fact, it was also shown that synaptic mitochondria are more susceptible to Ca2+ overload and the induction of MPTP than nonsynaptic mitochondria (24, 134), which reinforces the idea that synaptic mitochondria, including their DNA, are more vulnerable to injury.
BER enzymes are negatively modulated by covalent modifications in an age-dependent manner putatively due to decreased acetylation (183) or iron/copper dyshomeostasis (79). Notably, a general trend toward increasing heteroplasmy with the aging process has been observed, due to a gradual accumulation of alterations in mtDNA throughout life (170). These results are in accordance with previous observations of increased mtDNA deletions (15, 98) and somatic mutations (164) with age in the substantia nigra. A causal relation between the malfunction of BER machinery and neurodegeneration has been established, which is further associated with behavioral alterations (102).
Alzheimer's disease
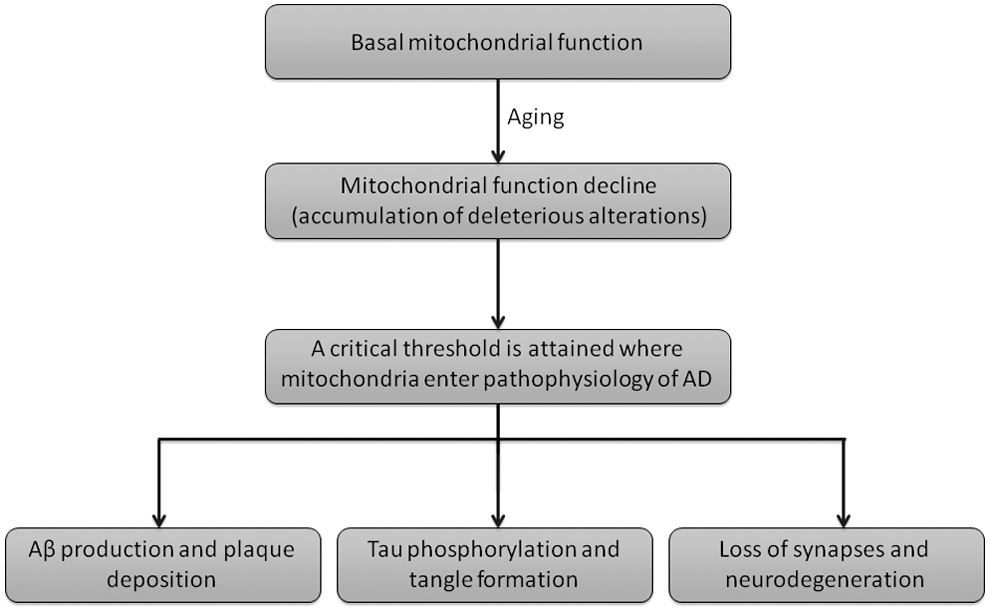
Mitochondrial dysfunction and exacerbated generation of ROS are well known features of AD. Moreira (130) and de la Monte (46) reported that AD brains present increased fragmentation of mtDNA, reduced mtDNA content and mass, reduced level of COX, and evidence of apoptotic cell loss. Despite no causative mtDNA mutations being linked to AD, some polymorphic variations can occur, having implications in enzymatic activities, such as COX (109). Some mtDNA mutations have been associated with increased incidence of AD (195, 43). Likewise, a reduction in the level of ND6 complex I transcript in AD has been reported (43). AD brains present increased mtDNA mutations that are enhanced in an age-dependent manner, when compared with control cases (43). Nevertheless, and despite no causative mutations in mtDNA being currently known, mitochondrial dysfunction has been proposed to precipitate Aβ deposition, neurofibrillary tangle formation, and, ultimately, neurodegeneration (Fig. 5) (179, 180).
Although several studies demonstrate that oxidation of both nDNA and mtDNA is increased in AD brains (63, 124, 197), mtDNA oxidation has been found to be 10-fold higher than nDNA in frontal, parietal, and temporal lobes of AD patients (197). The simultaneous increased oxidation of mtDNA and deficiency of DNA repair could enhance the lesion to mitochondrial genome, potentially leading to neuronal loss. Indeed, Shao et al. (161) demonstrated that mitochondrial OGG1 activity is decreased in the frontal and temporal lobe of late-stage AD, and in the temporal lobe of MCI patients, compromising the removal of oxidatively damaged bases from mtDNA. Opposing results were recently reported in the brains of the triple transgenic model of AD (3×Tg-AD), in which no changes between the synaptosomal BER activities of presymptomatic and symptomatic AD mice were found (69). The contradictory observations reported in human and mice AD brains can be easily explained by the fact that the disease process in 3×Tg-AD mice is the result of a genetic manipulation, as those animals harbor the human amyloid precursor Swedish mutation, presenilin-1 M146V (PS1(M146V)) knock-in mutation, and tau (P301L) mutation; whereas in sporadic AD patients, mitochondria malfunctioning and oxidative stress are considered causative agents (155). Notably, rodents that were engineered to express an inducible mutant form of UDG1 show a decline in cognitive performance, as evaluated by the Morris water maze test (102). Furthermore, and similarly to that described in AD (198), rodents expressing mutant UDG1 also display abnormal mitochondrial dynamics (101), which supports the idea that impaired BER machinery may also play a role in AD.
More studies are needed to clarify the involvement of defects in mtDNA and its repair mechanisms in AD development. Furthermore, caution should be taken in the analysis and interpretation of results obtained with AD transgenic mice, as these animals mimic the familial cases of the disease, which represent less than 5% of all AD cases. In this line, it would be interesting to perform studies in rodents subjected to the intracerebroventricular administration of streptozotocin (icvSTZ), which are considered animal models of sporadic AD.
Conclusion
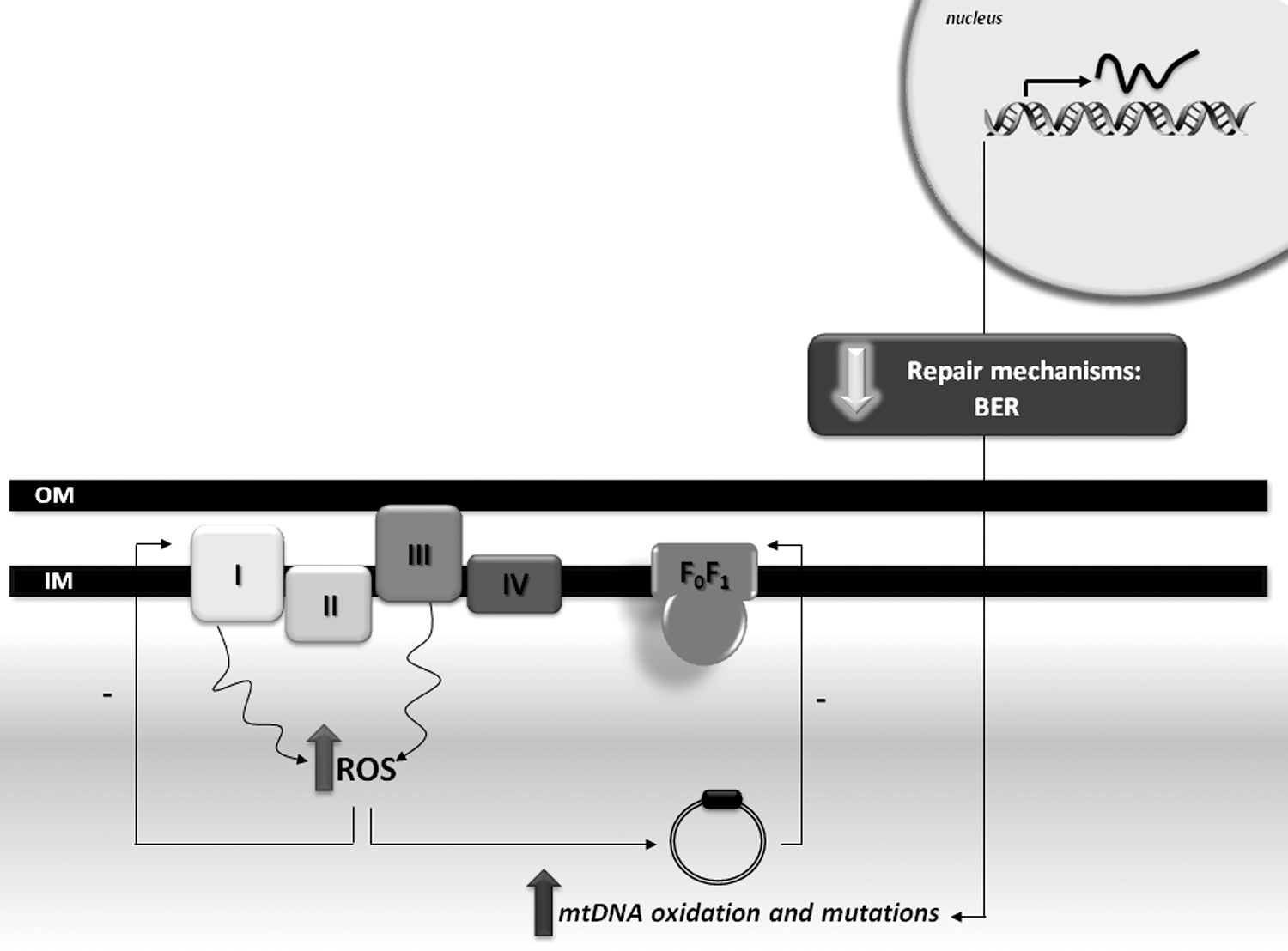
Mitochondria are major producers of ROS that under low/moderate levels act as second messengers. However, during aging and age-related diseases, an increased production of mitochondrial ROS associated with a defective scavenging system culminate in a redox imbalance and high levels of oxidatively damaged biomolecules. Mitochondrial dysfunction is currently accepted as a pathological hallmark of AD, which is considered an early event in disease pathogenesis. The accumulation of oxidative lesions to mtDNA occurs during aging and is also a prominent feature in AD, along with the failure in BER machinery. The observation that mtDNA oxidation occurs during aging and in the prodromal stage of AD strongly supports the idea that mitochondrial abnormalities are causative agents in AD. Whether mtDNA oxidation is a determinant for the onset of disease is yet to be clarified, namely if there is any threshold that triggers the disease process. Nonetheless, it is tempting to propose that the impairment in OXPHOS results in an exacerbation of ROS generation that increases the probability of mtDNA mutations in a positive feedback loop, a situation which is potentiated by a defective BER machinery (Fig. 6). The clarification of BER in AD also opens new windows for therapeutic intervention that are aimed at effectively repairing damaged mtDNA.
Footnotes
Acknowledgments
Renato X. Santos is the recipient of a PhD fellowship from the Fundação para a Ciência e a Tecnologia (SFRH/BD/43972/2008). Work in the authors' laboratories is supported by Fundação para a Ciência e a Tecnologia and Fundo Europeu de Desenvolvimento Regional (PTDC/SAU-NEU/103325/2008 and PTDC/SAU-NMC/110990/2009). This project was also supported by a grant from the National Institute on Minority Health and Health Disparities (G12MD007591) from the National Institutes of Health.