
Abstract
In the present study, we tested the hypothesis that oxidative stress could be implicated in myocardial damage during the acute phase of pneumonia. NOX2 activation, the catalytic subunit of NADPH oxidase, and high-sensitivity cardiac troponin T (hs-cTnT) elevation have been analyzed in two hundred forty-eight consecutive patients hospitalized for community-acquired pneumonia. Serum NOX2-derived peptide (sNOX2-dp), a marker of NOX2 activation, and 8-isoprostaglandin F2α (8-iso-PGF2α), a marker of oxidative stress, were measured upon admission; serum hs-cTnT and ECG were measured every 12 and 24 h, respectively. One hundred thirty-five patients (54%) showed elevated serum levels of hs-cTnT (>0.014 μg/L). A logistic regression analysis showed sNOX2-dp (p<0.001), Pneumonia Severity Index score (p<0.001), renal failure (p=0.024), and ejection fraction (p<0.001) as independent predictors of elevated serum levels of hs-cTnT. Serum sNOX2-dp was linearly correlated with hs-cTnT (Rs=0.538; p<0.001) and 8-iso-PGF2α (Rs=0.354; p<0.001). The study provides the first evidence of a significant association between serum cardiac Troponin T elevation and NOX2 upregulation in patients with pneumonia. This finding raises the hypothesis that NOX2-derived oxidative stress may be implicated in myocardial injury and that its inhibition could be a novel therapeutic strategy to limit it. Antioxid. Redox Signal. 20, 2949–2954.
Introduction
C
Epidemiological studies have shown that respiratory tract infections are associated with an increased risk for the development of acute cardiovascular events (2). Furthermore, markers of myocardial injury, such as elevated blood levels of T Troponin, have been detected in pneumonia (1), a phenomenon that may be associated with poor outcome. Even if systemic inflammation has been suggested to elicit myocardium damage, the underlying mechanism is still elusive.
Recent studies focused the attention on the fact that pneumonia may be complicated by cardiac damage. In the acute phase of pneumonia, we found that >50% of patients disclosed elevation of cardiac Troponin T indicating that a large amount of patients are affected by myocardial injury. The article reports for the first time that cardiac T troponin elevation is associated with upregulation of serum NOX2 suggesting NOX2-derived oxidative stress as a mechanism favoring myocardial injury. Thus, pharmacological inhibition of NOX2 might represent a new therapeutic strategy to limit myocardial injury and prevent cardiac complications.
Reactive oxidant species (ROS) are chemically unstable molecules, which are key elements of systemic inflammation and may provoke cellular damage. Among the enzymatic pathways producing ROS, experimental and clinical evidence focus on the central role of NADPH as the key enzyme in producing ROS into the cells (5). No data regarding NOX2-derived ROS have been reported in pneumonia so far. We speculated that in pneumonia, NOX2 may be upregulated and associated with myocardium injury as assessed by serum cardiac T Troponin. Therefore, the aim of the study was to measure the NOX2 activity, as assessed by soluble NOX2-derived peptide (sNOX2-dp) (7), and isoprostanes, as assessed by 8-isoprostaglandin F2α (8-iso-PGF2α), a reliable marker of oxidative stress (7), along with T Troponin in a population affected by pneumonia.
Results
Two hundred forty-eight patients hospitalized for CAP were recruited (150 males; 98 females; age: 71±16 years). Most of the patients had arterial hypertension (70%). A history of coronary heart disease (CHD) was present in 37% of patients, a history of stroke in 12%, type 2 diabetes mellitus (T2DM) in 25%, chronic obstructive pulmonary disease (COPD) in 35%, peripheral artery disease (PAD) in 7%, and dyslipidemia in 20%. History of paroxysmal atrial fibrillation was present in 11% of patients, while 16% were affected by chronic (persistent or permanent) atrial fibrillation. Twenty percent of patients had severe renal failure (i.e., a glomerular filtration rate<30 ml/min). Forty-five percent of patients were treated with aspirin, 33% of CAP patients received statins.
Elevated serum levels of high-sensitivity cardiac Troponin T (hs-cTnT) (>0.014 μg/L; median 0.039 μg/L and interquartile range [IQR] 0.024–0.116 μg/L) were found in 135 (54%) of the CAP patients within 48 h from admission.
Table 1 shows baseline characteristics of CAP patients categorized by hs-cTnT levels (>or ≤0.014 μg/L). Patients with higher hs-cTnT levels were older, had a higher prevalence of CHD history, T2DM, hypertension, renal failure, COPD, chronic atrial fibrillation, PAD, and a higher prevalence of aspirin treatment. Moreover, patients with hs-cTnT>0.014 μg/L showed a higher Pneumonia Severity Index (PSI) score and a lower ejection fraction. Serum sNOX2-dp as well as serum isoprostane levels were significantly higher in patients with hs-cTnT >0.014 μg/L.
Data are expressed as medians [interquartile ranges].
CAP, community-acquired pneumonia; BMI, body mass index; COPD, chronic obstructive pulmonary disease; hs-cTnT, high-sensitivity Troponin T; hs-CRP, high-sensitivity C-reactive protein; PAD, peripheral arterial disease; PSI, Pneumonia Severity Index; T2DM, type 2 diabetes mellitus.
In a logistic regression analysis, sNOX2-dp, PSI score, renal failure, and ejection fraction remained independently associated with elevated serum levels of hs-cTnT (Table 2).
After adjusting for age, BMI, T2DM, hypertension, history of CHD, COPD, PAD, chronic and paroxysmal atrial fibrillation, dyslipidemia, hs-CRP, use of statins and aspirin (none of these variables was significant).
CI, confidence interval; OR, odds ratio.
In the overall population, serum sNOX2-dp was linearly correlated with hs-cTnT (Rs=0.538; p<0.001) and isoprostanes (Rs=0.334; p<0.001).
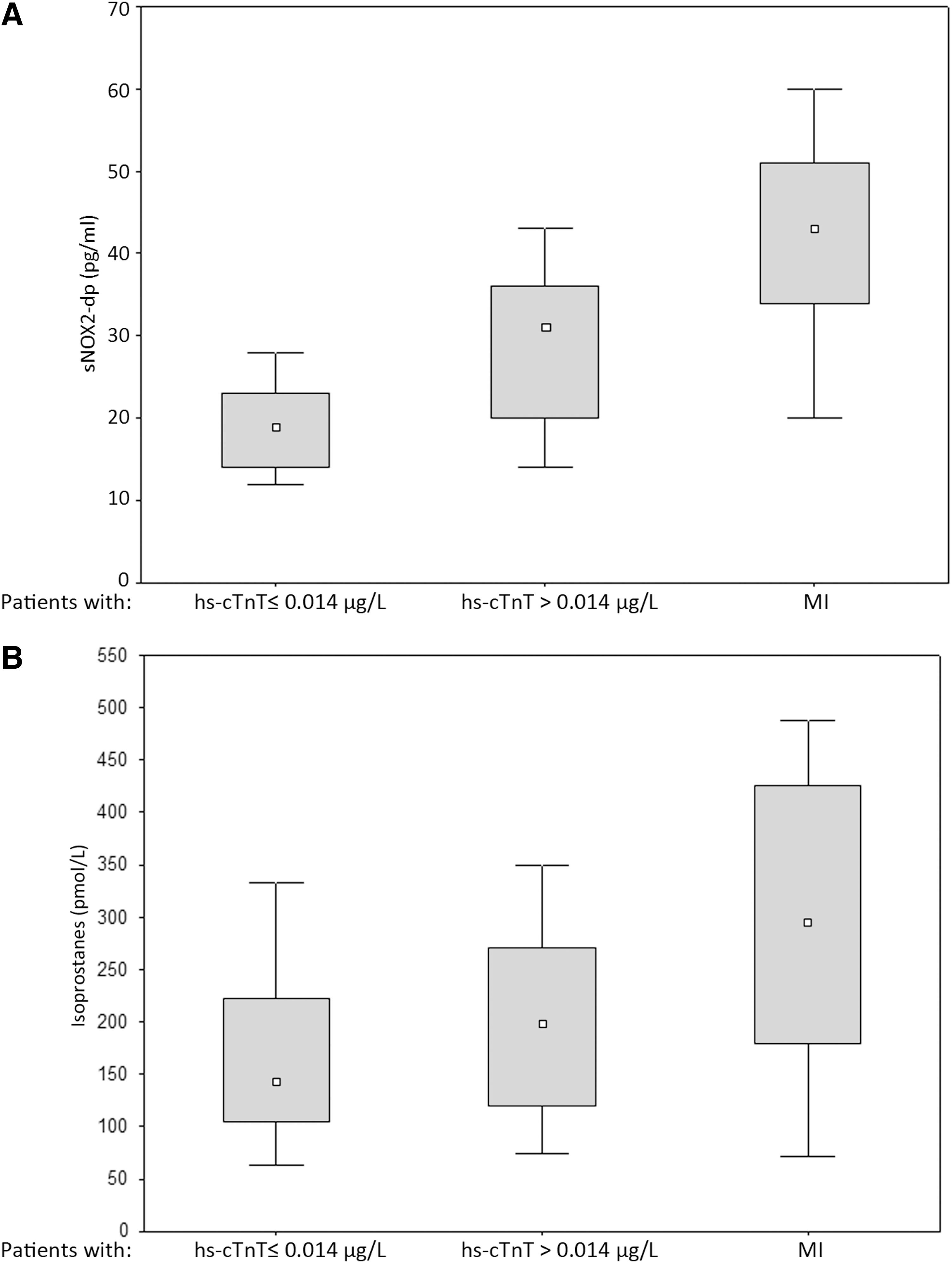
Twenty-nine (12%) patients showed cardiac troponin elevation and signs of myocardial infarction (MI), which were diagnosed according to the universal definition proposed by the Joint ESC/ACCF/AHA/WHF Task Force (8).
Dividing the population in three groups: (i) patients without troponin elevation (hs-cTnT median and IQR: 0.010 [0.010–0.012] μg/L), (ii) patients with no MI-related troponin elevation (hs-cTnT: 0.032 [0.023–0.061] μg/L), and (iii) patients with signs of MI (hs-cTnT: 0.298 [0.143–0.543] μg/L), a progressive and paralleled increase of both serum sNOX2-dp and isoprostanes was found (p<0.001) (Fig. 1).
Discussion
This study provides evidence that >50% of patients with pneumonia have enhanced levels of serum T Troponin indicating that pneumonia is complicated by myocardial damage. The simultaneous upregulation of NOX2 and isoprostanes as well as the significant association between NOX2 upregulation and T troponin suggest that oxidative stress is implicated in myocardial damage observed during pneumonia.
Pneumonia and myocardial injury
Previous studies have already shown that pneumonia is complicated by high T troponin levels indicating an association between infectious diseases and myocardial injury; in particular, Chang et al. (1) have recently reported that, at admission, 19% of patients with pneumonia have elevated T Troponin, but the underlying mechanism was not investigated. Whereas we confirm these findings, the prevalence of high T Troponin levels of our population is much higher. The reason for this difference can be explained by the fact that, in our population, the levels of T Troponin were measured not only at baseline, but also every 12 h during the first days of hospitalization. Thus, the occurrence of an increase of T Troponin could be detected until after 48 h from hospital admission indicating that myocardial damage should be investigated throughout the intrahospital stay.
Pneumonia and MI
Among patients with elevated hs-cTnT, 29 (12%) had signs compatible with MI. Previous studies have shown that pneumonia may be complicated by MI; most of these studies were retrospective and the rate of MI ranged from as low as 1.2% to as high as 10.7% (3). In the only prospective study reported so far, Corrales-Medina (3) found a rate of 3.6% during a follow-up of 7 days; such a rate could be underestimated because only CK-MB was used as a marker of myocardial necrosis.
Pneumonia and NOX2 activation
Systemic inflammation has been suggested to play a major role in eliciting myocardial damage. Thus, pneumonia is associated with a marked increase of proinflammatory cytokines, which may favor vascular and myocardial damage.
Among the inflammatory mechanisms eliciting myocardial damage, oxidative stress could play a major role as ROS may determine lipid, protein, and DNA oxidation leading to cell death (9). So far, no data exploring the behavior of oxidative stress have been reported in pneumonia. We found that serum sNOX2-dp and isoprostanes were elevated in patients with elevated T Troponin indicating a potential interplay between oxidative stress and myocardial damage. Of particular interest was the finding of a progressive increase of serum sNOX2-dp and isoprostanes coincidentally with cardiac T Troponin elevation, suggesting a potential interplay between the rate of NOX2 activation and myocardial injury. Consistently with this, higher sNOX2-dp levels were detected in patients with signs of MI who, in fact, exhibited higher T Troponin levels. Logistic regression analysis reinforced the concept that NOX2 activation was associated with T troponin levels independently from other clinical variables associated with T Troponin elevation, such as PSI, renal insufficiency, and ejection fraction. Concerning the inverse association between T Troponin and ejection fraction, it could be tempting to speculate that such an inverse association reflects myocardial injury induced by pneumonia, but the lack of previous echocardiograms precludes definite conclusions.
Our data lead to speculate that, in pneumonia, myocardial injury may be mediated by NOX2 upregulation. This hypothesis is consistent with previous reports indicating that the equilibrium of the redox balance is crucial for the health of cardiomyocytes (9). In fact, oxidative stress has been proved to have several detrimental effects on the myocardium, such as apoptotic cell death, hypertrophy, fibrosis, dysfunction, and dilatation (9).
The mechanism accounting for NOX2 upregulation in patients with pneumonia has not been investigated in the present study and requires further investigation. Several mechanisms, however, could be implicated in NOX2 upregulation, including interaction of specific microbial ligands with the immune system cell surface receptors or interplay between inflammation mediators, such as endotoxins or cytokines and NOX2 (5).
Limitations and implications
Despite the association between serum T Troponin and NOX2 regulation, a cause–effect relationship cannot be firmly established because of the observational nature of the study. To address this issue, an interventional study should be done to explore if a reduction of serum T Troponin may be achieved with NOX2 inhibitors. The implication of our observation is that statins could be an interesting therapeutic option, as they have been shown to inhibit NADPH oxidase (7). Interestingly, a retrospective study by Douglas et al. (4) reported a lower mortality among people with pneumonia on statin treatment.
A limitation of the study is that we used sNOX2-dp, which maximally reflects NOX2 activity from blood cells, including platelets and white cells (7), as a mirror of cardiac NOX2; therefore, we do not have elements to definitely indicate that NOX2 from the heart muscle is upregulated and elicits cardiac damage in situ. We cannot exclude, however, that myocardial damage may occur as a consequence of systemic oxidative stress elicited by infectious diseases.
Conclusions
The study provides the first evidence of a significant association between serum Troponin elevation and NOX2 upregulation in patients with pneumonia, suggesting that NOX2-derived oxidative stress may be implicated in myocardial injury. This finding may represent a scientific background to test the hypothesis that NOX2 inhibition is a tool to limit cardiac damage in patients with pneumonia.
Notes
Patient selection
The study was conducted at the four centers of the University-Hospital Policlinico Umberto I, Rome. All patients, admitted to the four Units with CAP through the emergency department from October 2011 to April 2013, were Caucasian and lived in the center and south of Italy; they were prospectively recruited and followed up. Two hundred forty-eight consecutive patients who fulfilled the following criteria were enrolled in the study after providing written informed consent: (i) age 18 years or over; (ii) clinical presentation of an acute illness with one or more of the following signs or symptoms suggesting CAP (6): presence of rales, rhonchi, bronchial breath sounds, dullness, increased fremitus and egophony, fever (>38.0°C), tachycardia, chills, dyspnea, coughing (with or without productive cough), and chest pain; and (iii) the presence of new consolidation(s) on chest X-ray. Pneumonia was considered as CAP if it was diagnosed upon hospitalization and the patient had not been discharged from an acute care facility within 14 days preceding the clinical presentation.
Patients were excluded from the study if one of the following criteria applied: radiographic evidence of preexisting infiltrates; severe sepsis or immunosuppression (HIV infection, chemotherapy, high dose of immunosuppressive agents such as prednisone); presence of malignancy; pregnancy or breast feeding; documented severe allergy to antibiotics; and health care-associated pneumonia (6).
Baseline assessment
Data on demographic characteristics, comorbidities, and empirical antibiotic therapy were collected. Severity of illness at presentation was quantified by the PSI, a validated prediction score for 30-day mortality in patients with CAP (6). Immediately after diagnosis of CAP, routine blood laboratory tests, serum hs-cTn, high-sensitivity C-reactive protein (hs-CRP), and arterial blood gas tests were performed. Thereafter, serum hs-cTnT and 12-lead ECG were repeated every 12 and 24 h, respectively; M-mode and two-dimensional color Doppler echocardiography were performed within 2 days from hospital admission. The ejection fraction was measured by using the modified Simpson's rule.
The present study was conducted according to the principles stated in the Declaration of Helsinki. The institutional review board approved this prospective, observational study, which was registered at ClinicalTrials.gov (Identifier: NCT01773863).
Laboratory analysis
Serum levels of hs-cTnT levels were measured by the Elecsys 2010 (Roche Diagnostics) in a dedicated core laboratory. According to the manufacturer, the 99th percentile cutoff point of the hs-cTnT was 0.014 μg/L, and a coefficient of variation of <10% was achieved at 0.013 μg/L.
Serum levels of sNOX2-dp were detected by the ELISA method as previously described (7). The peptide was recognized by a specific monoclonal antibody against the amino acidic sequence (224–268) of the extra membrane portion of NOX2. Values were expressed as pg/ml; intra-assay and interassay coefficients of variation were 5.2% and 6%, respectively.
Serum isoprostanes, as assessed by 8-iso-PGF2α, were measured by a previously described and validated EIA assay method (7). Intra- and interassay coefficients of variation were 2.1% and 4.5%, respectively.
Statistical analysis
Categorical variables were reported as counts (percentage) and continuous variables are expressed as mean±standard deviation (SD) or median and IQR. Differences between percentages were assessed by the chi-square test or the Fisher exact test. The Student's unpaired t-test and Pearson product-moment correlation analysis were used for normally distributed continuous variables. Appropriate nonparametric tests (the Mann–Whitney U test and the Spearman rank correlation test) were employed for all the other variables.
The bivariate and multivariate effects of prognostic factors and treatments on the endpoint (hs-cTnT elevation within 48 h from admission) were assessed by means of logistic regression models. Wald confidence intervals and tests for odds ratios and adjusted odds ratios were computed based on the estimated standard errors. In addition to sNOX2-dp and 8-iso-PGF2α levels, possible independent variables considered were as follows: age, gender, body mass index, PSI, history of CHD, or stroke, T2DM, dyslipidemia, hypertension, renal failure, COPD, chronic or paroxysmal atrial fibrillation, PAD, hs-CRP, and the use of statins and aspirin.
For multivariate models, model selection was performed using forward stepwise regression based on Akaike information criterion.
Only p-values lower than 0.05 were considered as statistically significant. All tests were two tailed and analyses were performed using computer software packages (SPSS-13.0, SPSS, Inc.).
Sample size
The minimum sample size was computed considering (i) an expected rate of hs-cTnT elevation of 19% (1), (ii) a relevant difference in NOX2 levels to be detected between the groups (patients with or without hs-cTnT elevation) |δ|≥8 pg/ml, (iii) a standard deviations between the groups, SD=10 pg/ml, and (iv) a type-I error probability α=0.05 and power 1-β=0.90. This resulted in n=174 patients.
Footnotes
Acknowledgment
This work was supported by a grant from the Sapienza-University of Rome (Ateneo Federato 2009 to F.V. - C26F099L4K).
Author Disclosure Statement
No competing financial interests exist.