
Abstract
Although the inducible form of nitric oxide synthase (NOS2) was initially shown to be a major player as an antitumor component of the immune response, more recent data have shown that NOS2 expression in cancer cells often predicts poor outcome. Unlike growth factors associated with a single oncogenic pathway, nitric oxide (NO) has a ubiquitous nature wherein it simultaneously mediates major oncogenic pathways from Akt/PI3K and RAS/ERK to HIF1a and TGFb. These interactive loops perpetuate oncogenic mechanism that leads to increased cancer stemness, proliferation metastasis, chemoresistance, angiogenesis, and immunosuppression. Examination of a wide variety of patient tumors demonstrates that NOS2 expression is >50% for most cancers. In many cases, elevated NOS2 has been shown to predict poor outcome in cancer such as ER- breast cancer, glioma, melanoma, cervical, liver, ovarian, and pancreatic. Taken together, NOS2 may be one of the most powerful biomarker and predictors of poor prognosis and an ideal target for cancer therapy. Antioxid. Redox Signal. 26, 963–965.
C
Within the inflammatory milieu, redox biology plays a critical role in communication between these components, which influences both cellular signaling and metabolism. Redox associated with inflammation includes small reactive molecules, which have been traditionally defined as nitric oxide (NO), reactive oxygen species (ROS), and eicosanoids (7). More recently, hydrogen sulfide (H2S)/persulfides and carbon monoxide have merged as additional components to the redox landscape. These molecules have been shown to participate in numerous aspects of cancer biology. For example, during 1980–1990, eicosanoids derived from COX2 were shown to play a significant role in a number of cancers (9). Oxidative stress and ROS have been shown to impact both the treatment and progression of many types of cancers. The discovery in the 1980s that NO and reactive nitrogen species were endogenously synthesized by macrophage was the start of the field of NO and cancer. Early in this field, studies showed that NO was both a tumoricidal agent and a source of carcinogenic nitrosamine, suggesting that these reactive species may have either pro- or antitumorigenic properties.
Since their initial discoveries, these redox species were found to play many different and often contradictory roles in cellular communication. Over the course of the 1990s, NO was shown to be a direct genotoxic species, interfering with DNA repair and through the formation of carcinogenic nitrosamines (9). However, at the same time, NO was also shown to have a critical antitumoricidal function in various cancers especially in leukemias. These properties were associated with alterations in the expression levels of the inducible form of nitric oxide synthase (NOS2), the isoform that produces high sustain amounts of NO. Later it was shown that transfection of NOS2 into human cancer cells leads to increasingly aggressive tumors in vivo despite being less proliferative in vitro (8). Further research demonstrated that there was a key link between NO levels and p53, wherein NOS2 was inhibited by p53 and that higher levels of NO increase stabilization of p53 (8). This link between NOS2 and p53 provides a critical piece of the puzzle in the dichotomy of NOS2. Leukemic cells that were p53 mutated or null were much more resistant. P53 and NOS2 knockout mice had dramatically increased cancers.
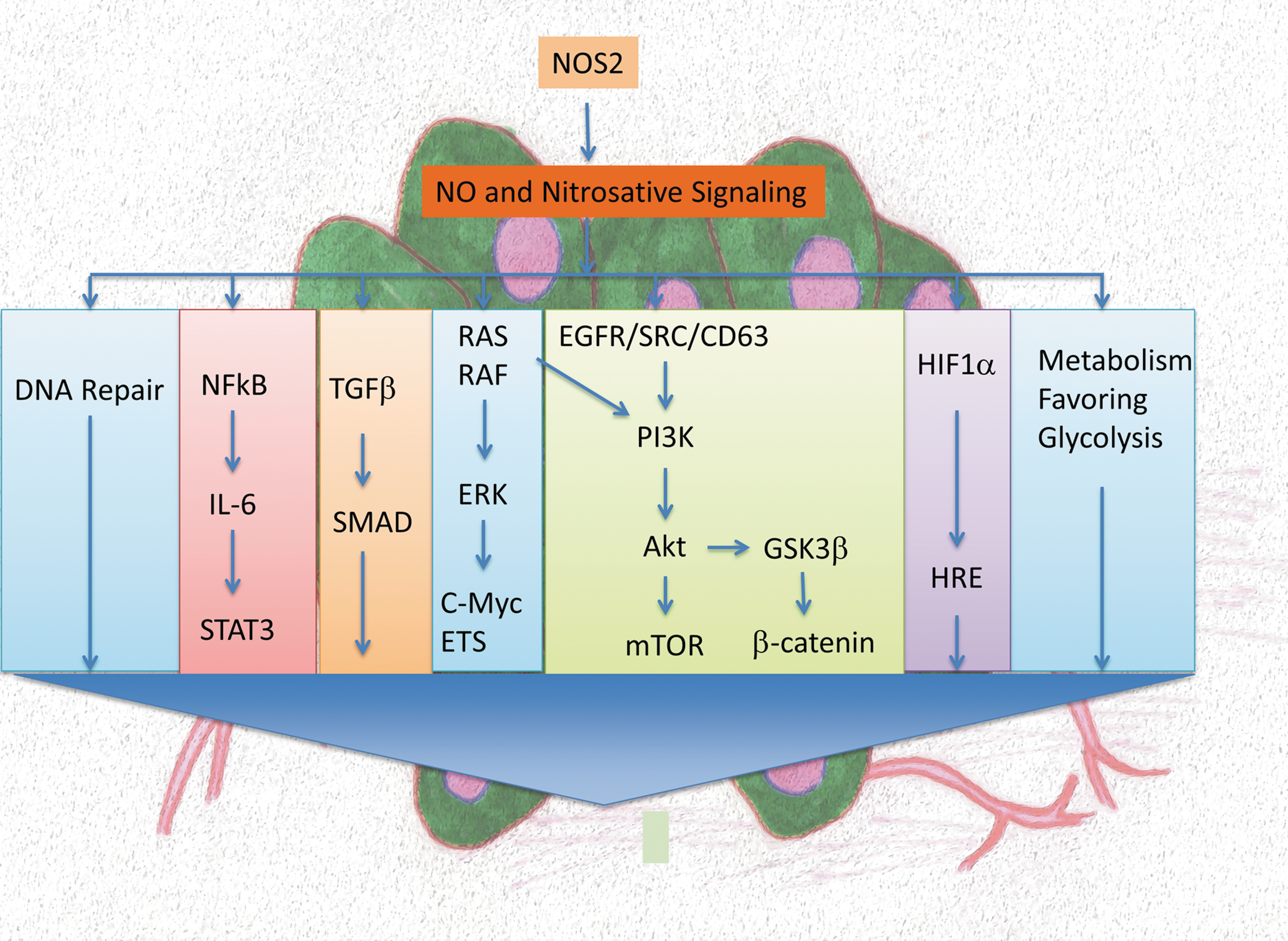
The use of NO-donor compounds was a critical in vitro tool toward the elucidation of concentration- and time-dependent effects of NO on signal transduction mechanisms. An important insight was gained as to why NO can activate cancer-promoting pathways such as Akt/ERK/HIF while also increasing p53, which results in growth arrest and apoptosis (7). As we learn more about NO and cancer, these levels can be critical in orchestrating the immune response to tumors while other levels induce angiogenesis and metastasis. This dichotomy is what makes NO role in cancer hard to pin down. By the mid-2000s, it became apparent that the regulation of different pathways by NO was dependent on the steady-state concentration and temporal profile. NO concentrations between 1 and 50 nM primarily regulated cGMP-mediated processes whereas NO >500 nM leads to an increase in stress responses such as p53 (7). Between 100 and 500 nM, it was found a pro-oncogenic level that leads to activation of pathways involving RAS/ERK, PI3K/Akt/β-catenin, HIF-1α, NrF2, and TGFβ. This intermediate level of NO could directly stimulate most of the major signaling pathways associated with cancer. Unlike, epidermal growth factor or other growth factors, this level of NO is a “universal driver of these oncogenic pathways” that are often associated with poor outcome in patients (Fig. 1). Interestingly, NOS2 was the only isoform that could achieve these levels of NO for sustained periods of time, suggesting that NOS2 may have a role in both protumorigenic and antitumorigenic processes (7).
Although these in vitro and in vivo findings provided new insight, it still does not definitely provide a road map without clinical data. Over the past decade, however, there have emerged a number of clinical trials showing NOS2 is present in a large number of cancers. This redox enzyme has been found present in more than 50% of glioma, breast, prostate, pancreatic, melanoma, liver, cervical, ovarian, nasopahgeal, lung, stomach, colon, and esophageal cancer patients (summarized in [2]). Like its inflammatory cousin COX2, this enzyme is prevalent in many tumors and is often coexpressed with each other. Importantly, NOS2 has been shown to predict poor patient outcome in breast, glioma, melanoma, pancreatic, stomach, liver, and colon cancers. In many cases, it correlates with increased vascular and metastatic potential (summarized in [2]).
In this Forum, these articles present discussions on the different mechanisms of NO and NOS2 that shape the tumor microenvironment that determines prognosis in different cancers. Tran et al. showed that NOS2, but the isoforms, was associated with poor survival with glioblastoma. NOS2 can be induced in human and murine glioma lines, which increase protumorigenic phenotype of migration and vascularization. Burke et al. discuss elevated levels of NOS2 in prostate cancer, showing that prolonged physiological levels of NO can result in transformation of prostate epithelial cells to a stem-like phenotype, implicating NO as a promoter of progression (ref in Forum). Like other ductal cancers, pancreatic cancer also expresses NOS2, leading to poor outcome. Breast cancer has high NOS2 in both ER+ and ER−, but only ER- and NOS2 are prognostic indicators for poor outcome. Finally, gastrointestinal (GI) cancer and liver cancer have high frequency of NOS2, leading to poor outcome. In this article, the authors discuss the different mechanism to NOS2 in different GI-related tissues. Brune et al. discuss the role of macrophage in the dichotomy of NOS2 in its tumoricidal as opposed to promotion of cancer through myeloid derived suppressor cells. These articles paint a story that shows the ubiquitous nature of NOS2 and its role in cancer progression.
Many cancers that have elevated NOS2 are associated with bacterial or viral infection, for example, cervical, gastric, prostate, esophageal, and liver cancers. In hepatocellular carcinoma, NOS2 and COX2 were not associated with noninfected but only with hepatitis C virus and hepatitis B virus-induced cancer (4). HPV infection associated with cervical cancer shows elevated NOS2 (6). An excellent example of a pathogen-associated elevation of NOS2 is gastric cancer that is associated with helicobacter (1, 3). An example of virus infection associated with NOS2 is cervical cancer. Interestingly, NOS2 has a positive prognosis at an early stage, but in later stages, NOS2 is a poor predictor of prognosis and like other solid cancers leads to more vascularization and metastasis. Finally, the metabolic environment in the tumor including hypoxia can lead to increased NOS2 expression. As pointed out in the article by Brune in this Forum, hypoxia can induce S1P macrophages, leading to COX2 and interleukin-6, thus leading to possible initiators and enhancement of NOS2 expression in tumor cells (ref in Forum). All in all, NOS2 has a central role in the progression of tumor. It is often said that, “Cancer is the wound that does not heal” and NOS2 has a central role perpetuating inflammatory pathways that contribute to poor patient outcome (5).