
Abstract
The worldwide epidemic of obesity is a major public health concern. Obesity is a major risk factor for noncommunicable diseases such as type 2 diabetes and cardiovascular diseases, clustered in the so-called metabolic syndrome (MS). Other main chronic illnesses are promoted by excessive body weight, including cancer and neurodegenerative pathologies, both affecting a number of people worldwide. In recent years, the primary role of an excess of reactive oxygen species (oxidative stress) resulting from altered redox control in the etiology of all of these pathologies has been unveiled. Interestingly, it appears that oxidative stress is both the cause and the consequence of obesity and associated disorders. This Forum features reviews that recapitulate the current knowledge on the link between oxidative stress and MS in the physiopathology of different biological systems. Antioxid. Redox Signal. 26, 429–431.
M
Our generation is witnessing a huge increase of metabolism affections (Fig. 1), clustered into the term of “metabolic syndrome” (MS): obesity (excess of fat in adipose tissue and blood), insulin resistance (decrease of glucose entry into cells because of altered insulin signaling), diabetes (dysfunctional endocrine pancreas secreting insulin), and cardiovascular diseases (mainly heart disease and stroke). The prevalence of MS has been increasing exponentially in the past decades worldwide, paralleling the obesity epidemic. Overweight and obesity are defined as abnormal or excessive fat accumulation that may impair health. According to the World Health Organization, 39% of adults aged 18 years and more were overweight in 2014, and 13% were obese. Once considered a problem only in high-income countries, overweight and obesity are now dramatically on the rise in low- and middle-income countries, particularly in urban settings. Obesity depends on both genetic and environmental factors, in particular, lifestyles featuring increased nutrient caloric intake but decreased calorie consumption. Overweight and obesity are major risk factors for a number of noncommunicable diseases such as diabetes, cardiovascular diseases, and cancer.
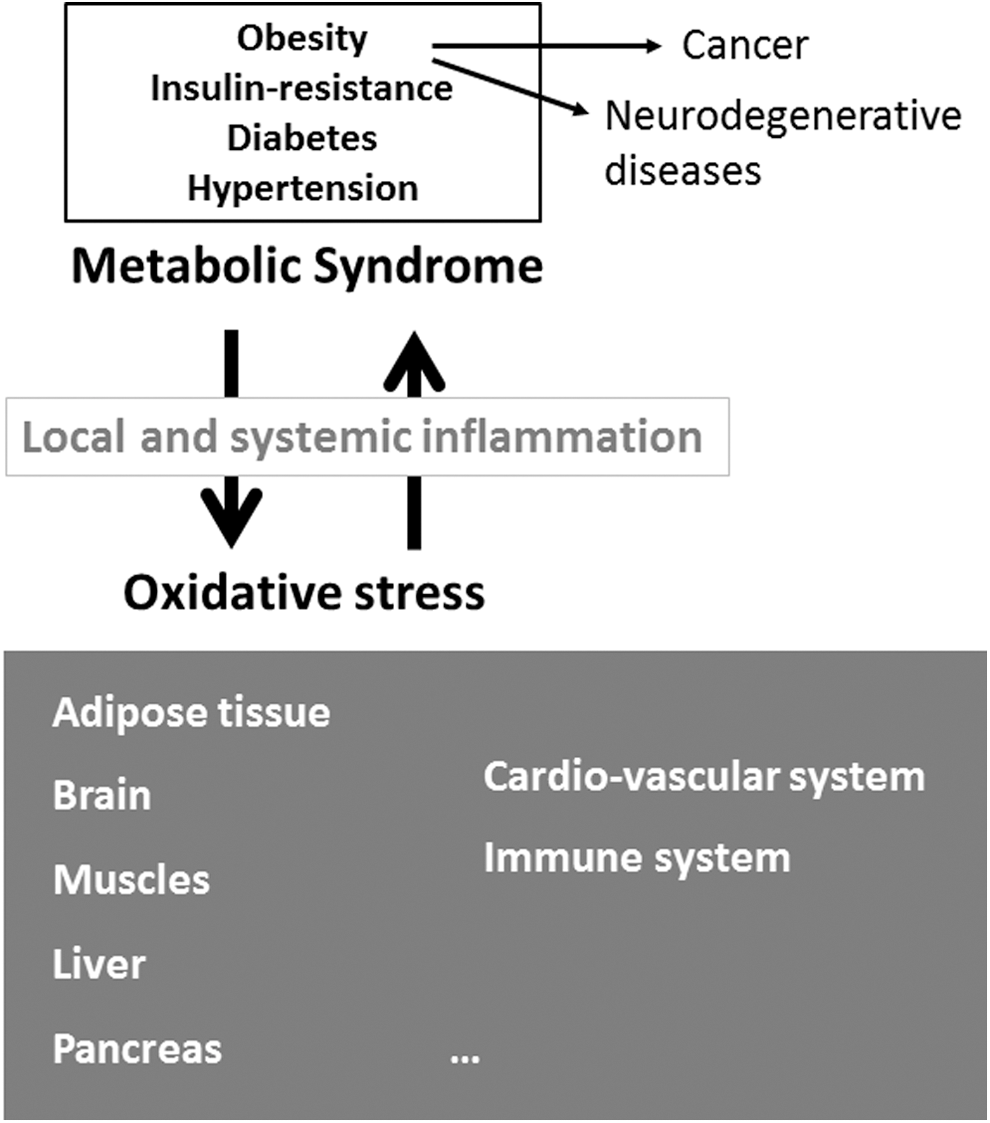
Interestingly, obese individuals often have chronic low-level inflammation, associated with a chronic whole-body oxidative stress. Oxidative stress corresponds to an excess of reactive oxygen species (ROS) resulting from an imbalance between the production and the elimination of ROS in favor of the former. In cells, ROS are mainly produced in mitochondria as by-products of the respiratory chain. Mitochondria are organelles playing a crucial role in cell physiology, particularly in metabolism, as involved in the production of energy (adenosine triphosphate) [ATP] by the respiratory chain, in the metabolism of carbohydrates, amino acids, and lipids (fatty acid oxidation [FAO]), and in apoptosis. In cells, ROS are also generated through the activity of enzymes such as nicotinamide adenine dinucleotide phosphate oxidases and in peroxisomes (fatty acid metabolism). A large battery of antioxidant defenses (enzymes and small molecules) contributes to regulating ROS level.
Oxidative stress is associated with MS, but whether it is the cause or the consequence is a matter of debate; many observations argue that both are true (Fig. 1). This Forum reviews the current understanding of the complex relationship between MS and oxidative stress. It consists of seven review articles related to different biological systems, which are dysregulated during MS-associated oxidative stress.
The first review by Spahis et al. (7) nicely introduces how obesity promotes the development of all metabolic abnormalities clustered in MS, as well as the involvement of oxidative stress in these pathologies. This review, in particular, recapitulates the current knowledge on the primary role of dysfunctional mitochondria in driving chronic oxidative stress.
The second review by Spahis et al. (8) recapitulates the current knowledge on the primary role of oxidative stress in the etiology of fat liver disease (not induced by high alcohol consumption).
The review by Gerber and Rutter (3) relates to the pancreas, a primary organ in metabolism, focusing on its endocrine part secreting insulin: the beta cells of Langerhans islets involved in glucose metabolism. This review summarizes the mechanisms of ROS involvement in the physiological function of these cells (how glucose drives insulin secretion by beta cells). In addition, this review deciphers how ROS are involved in the development of alterations in glucose metabolism occurring in insulin resistance and type 2 diabetes (T2D).
Importantly, the function of neuronal cells in the brain requires glucose at high levels, thus a healthy insulin-dependent metabolism. The review by Campos-Pena et al. (1) describes the impact of metabolic disorders on the development of Alzheimer's disease (AD). Some authors proposed that AD is the type 3 diabetes. The molecular features associated with AD (in particular accumulation of beta amyloid peptide) are related to metabolic defects, including redox deregulation. In that context, dysfunctions of mitochondria (the main source of ROS) play a primary role in AD etiology. T2D has also been associated with increased risk of Parkinson's disease, another debilitating neurodegenerative disease. As MS, neurodegenerative diseases are a main public health issue because their incidence is increasing after the increase in the duration of life. Nevertheless, these diseases are not solely associated with aging; indeed cognitive impairments can also be observed in young MS patients.
The healthy function of muscles relies also on insulin-stimulated glucose uptake, which is reduced during the development of whole body insulin resistance and T2D. The primary role of mitochondrial dysfunction associated with redox alterations in T2D muscles is discussed in a recent review (6).
A low-grade inflammation is also a characteristic of MS (Fig. 1). Affected tissues show local infiltration of immune cells, producing high levels of cytokines and ROS contributing to oxidative stress, and generating a systemic inflammatory state. The review by Morin et al. (5) deals with deregulations of the immune system during obesity, both in adipose tissue and in the systemic circulation. It is now established that these deregulations concern all types of immune cells. This review focuses on T cells, and also reports original data on the CD28 molecule, a major regulator of T cell activation.
The two last reviews are related to the first cause of death, cancer. Obesity increases the risk of many cancers (Fig. 1), through mechanisms involving obesity-associated inflammation as well as alterations of the insulin pathway that promote aberrant proliferation of cancer cells. In addition, one major feature of cancer cells is metabolic reprogramming, which has gained considerable interest in recent years. Regarding redox regulation, most of cancer cells are adapted to oxidative stress, showing high ROS levels as well as important antioxidant defenses. Metabolic changes in the mitochondria (the main source of ROS) in cancer cells are still poorly defined even though progress has been made over the past decade. The role of mitochondria in cancer cells has so far been neglected mostly because the Warburg effect hypothesized that oxidative glycolysis in cancer cells stems from impaired production of ATP by the respiratory chain and thus from defective mitochondria. However, this concept has recently been challenged. Indeed, it was shown that mitochondria are still functional in many subsets of cancer cells and that they are necessary for cell proliferation, and more importantly that this function is targetable in clinical applications (diagnostic, prognostic, and therapy) (4). The review by Gentric et al. (2) nicely recapitulates the current knowledge on cancer metabolic alterations, which both derive from and drive carcinogenesis (they can be both a cause and a consequence of cancer development). The review by Tessier et al. (9) deals with a particular actor of cell homeostasis, the promyelocytic leukemia protein, for which a role in metabolism (FAO) was recently reported, which could impact tumorigenesis.
The role of microbiota in MS is also a very interesting and recent field of research. In the intestine, microorganisms influence food assimilation, produce metabolites, thus dialoguing with the immune system as well as with all organs in the body. Alterations of the microbiota equilibrium (dysbiosis) can generate a systemic low-grade chronic inflammation supporting MS (7).
Finally, clinical issues are raised in most of the reviews of this Forum. Is oxidative stress a good target in the management of MS? If yes, how? These questions are mostly discussed in two reviews of this Forum (3, 7). Acting on diet rather than medication proved to be successful in most T2D patients. Current nutritional recommendations (balanced diet and regular physical exercise) are expected to dampen the increasing prevalence of MS.
Footnotes
Acknowledgments
The author thanks Valérie Depraetere-Ferrier for editing the article, and is grateful to INSERM, CNRS, Aix-Marseille University, INCa, and Fondation ARC for funding.