
Abstract
Aims:
Repeated use of nonsteroidal anti-inflammatory drugs can induce changes in the redox status, including production of reactive oxygen species (ROS), but the specific details of these changes remain unknown. Overhauser-enhanced magnetic resonance imaging (OMRI) has been used in vivo to monitor the redox status in several diseases and map tissue oxygen concentrations. We monitored the intra- and extracellular redox status in the stomach of rats with indomethacin-induced gastric ulcers using OMRI and investigated the relationship with gastric mucosal damage.
Results:
One hour after oral administration of indomethacin (30 mg/kg), OMRI measurements in the stomach were made following nitroxyl probe administration. OMRI with the membrane-permeable nitroxyl probe, 4-hydroxy-2,2,6,6-tetramethyl-piperidine-1-oxyl (TEMPOL), demonstrated a redox change toward oxidation, which was reversed by a membrane-permeable antioxidant. Conversely, imaging with the impermeable probe, 4-trimethylammonium-2,2,6,6-tetramethyl-piperidine-1-oxyl (CAT-1), demonstrated little redox change. Redox imbalance imaging of a live rat stomach with indomethacin-induced gastric ulcers was produced by dual imaging of 15N-labeled TEMPOL and 14N-labeled CAT-1, in addition to imaging with another membrane-permeable 15N-labeled probe, 3-methoxycarbonyl-2,2,5,5-tetramethyl-pyrrolidine-1-oxyl (MC-PROXYL), and 14N-labeled CAT-1. Pretreatment with MC-PROXYL suppressed gastric mucosal damage, whereas pretreatment with CAT-1 did not suppress ulcer formation.
Innovation:
OMRI combined with a dual probe is a less invasive imaging technique for evaluation of intracellular ROS production contributing to the formation of gastric ulcers in the stomach of indomethacin-treated rats, which cannot be done with other methods.
Conclusion:
This method may be a very powerful tool for characterizing the pathogenesis of various diseases and may have medical applications.
Overhauser-enhanced magnetic resonance imaging (OMRI) combined with a dual probe is a less invasive imaging technique for high-resolution evaluation of intracellular reactive oxygen species production, contributing to the formation of gastric ulcers in the stomach of indomethacin-treated rats, which cannot be done with other methods. This method may also be applicable for redox imaging of other diseases and innovative for drug development and imaging research toward theranostics.
Introduction
Changes in the redox status in the human body, involving the overproduction of reactive oxygen species (ROS) as well as reduction of redox-related biomolecules and antioxidants, have been reported to be associated with the onset and/or progression of various diseases (1, 11, 23). Redox imaging in vivo provides useful information on the redox status in living organisms. Electron spin resonance imaging (ESRI) has been used in vivo to monitor the following: spin clearance in the lungs of mice (38); the production of nitric oxide (NO) in septic mice (53); the thiol redox status in murine tumors (6); intracellular oxidative stress in the hippocampus and striatum of rats with kainic acid-induced epileptic seizures (51); and radical reactions in the head of spontaneously hypertensive rats and stroke-prone spontaneously hypertensive rats (20). ESRI is a direct method for obtaining information about free radicals, but it has very low spatial and temporal resolution. Magnetic resonance imaging (MRI) has high spatial and temporal resolution and can indirectly monitor changes in the shortening of longitudinal relaxation time (T1) by nitroxyl radicals in mice (13, 25). Overhauser-enhanced magnetic resonance imaging (OMRI), which is also called proton electron double resonance imaging or dynamic nuclear polarization-MRI, can give spatial information about free radical distribution based on the Overhauser effect (24, 32). OMRI has been used in vivo to map oxygen concentrations in tissues using triarylmethyl radicals (10, 18); monitor the distribution and clearance of several nitroxyl probes in the abdomen of mice (22); evaluate the pharmacokinetic parameters of nitroxyl probes in whole mice (17); map the redox status in rat brains (36, 48), mouse muscle (7), and mouse skin (8); and monitor the pH of aqueous solutions using pH-sensitive nitroxyl radicals (33). Both the tumor oxygen concentration and microvascular permeability in tumor-bearing mice could be simultaneously obtained with OMRI (28). Recently, we simultaneously imaged the intra- and extracellular redox status using a combination of OMRI and dual-labeled probes (40). Dual imaging of the redox status in vivo with OMRI may be a very powerful tool for characterizing the pathogenesis of various diseases.
Nonsteroidal anti-inflammatory drugs (NSAIDs) cause considerable gastrointestinal damage in association with inhibition of cyclooxygenase (COX) gene expression (42). COX-1 has been reported to be involved in the maintenance of the integrity of the gastric mucosa, mucosal blood flow, and mucus secretion (16, 30). However, inhibition of COX-1 alone is not sufficient to induce ulcer formation (19, 44), indicating that other factors are also involved in the mechanism of NSAID-induced formation of gastric ulcers. Changes in the redox status have been reported to be associated with the onset and/or progression of NSAID-induced gastric ulcers (39, 52). NSAIDs that release NO (45) have been developed to reduce the adverse effects on the gastrointestinal and cardiovascular systems. Nevertheless, the NO-releasing NSAID, naproxcinod, was rejected in 2010 by the U.S. Food and Drug Administration because of lack of long-term controlled studies (9). Novel NSAIDs that release hydrogen sulfide have been shown to be safe in rats (43). Hydrogen sulfide has been reported to increase reduced glutathione levels and suppress oxidative stress induced by hydrogen peroxide in mitochondria (15). Thus, elucidation of the in vivo redox status may promote drug discovery.
Previously, we have reported the redox status in rats with indomethacin-induced gastric ulcers using an in vivo ESR/nitroxyl probe method (41). Using membrane-permeable and membrane-impermeable probes, we demonstrated that the location of ROS generation changed significantly in the intracellular compartment of the gastric tissue. The pathological change was restored by membrane-permeable probes but not by membrane-impermeable probes. In vivo redox imaging of different compartments was not possible because of low temporal resolution of in vivo ESR. However, it is necessary to map the redox changes and determine the ROS-producing area(s) using a free-radical imaging method.
In the present study, the in vivo redox status in the stomach of rats with indomethacin-induced gastric ulcers was monitored by OMRI. The relationship between the redox status and the damage to the gastric mucosa was also evaluated.
Results
To show the effectiveness of OMRI in live animals, we superimposed OMRI with MRI. The MRI magnetic field of OMRI is too low (0.015 T) to provide anatomical information, so we used 0.2-T MRI after the OMRI measurement. Fiducial markers containing 1, 1.5, and 2 mmol/L probe solution were prepared for the superimposition with MRI and sensitivity calibration. The one-turn coil (Supplementary Fig. S1A) was used for ESR irradiation. The intensity of the OMRI image in the transverse plane showed homogenous sensitivity over an 8-mm range, and in the coronal plane it showed good homogeneity throughout the entire plane (Supplementary Fig. S1B), whose dimensions were comparable to those of the stomach of a typical rat. The markers were placed as shown by the arrows in Figure 1A. By superimposing the OMRI image of the spin probe administered orally to the rat with the MRI image using the markers as shown by the arrows in Figure 1B, the probe remaining in the stomach was confirmed. The average image intensities in the fiducial markers were plotted against the probe concentration (Fig. 1C), showing a good correlation up to 2 mmol/L (R 2 = 0.987), which is sufficient sensitivity for in vivo stomach measurements with OMRI (49).

A scheme of spin clearance/ROS scavenging using OMRI is shown in Figure 2. By comparing the temporal OMRI contrast decay between with and without an ROS scavenger, one can elucidate whether ROS such as hydroxyl radicals and superoxides are produced in the region where the nitroxyl probe is localized. Using nitroxyl probes with different membrane permeabilities, we found that ROS production occurred in the intracellular compartment and/or the extracellular compartment. The nitroxyl probes and the ROS scavenger used in this study are summarized in Table 1.

Nitroxyl Probes and Reactive Oxygen Species Scavenger Used in This Study
DMTU, dimethylthiourea; ROS, reactive oxygen species.
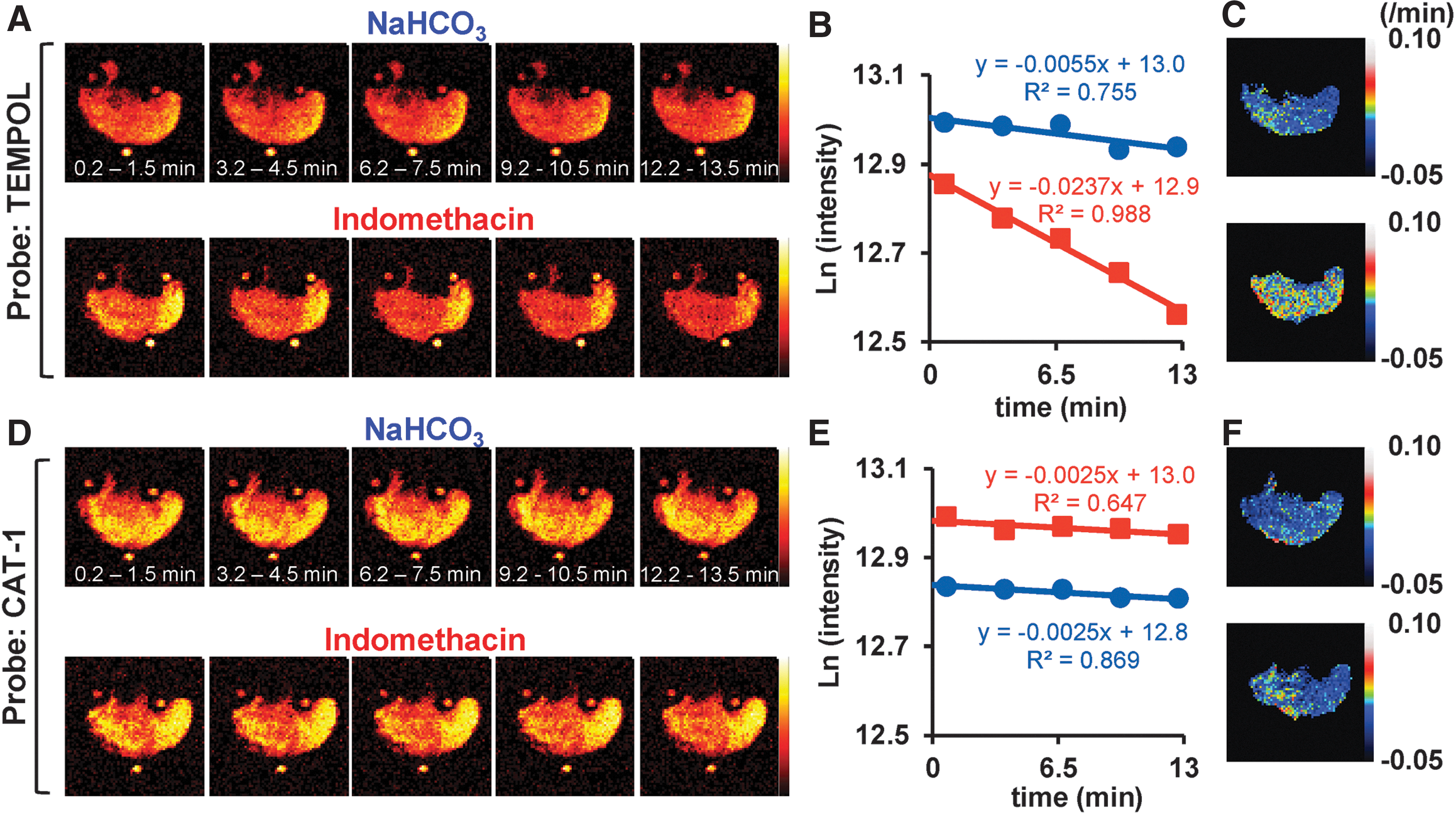
Next, we performed in vivo redox imaging of rat stomachs with indomethacin-induced gastric ulcers using 4-hydroxy-2,2,6,6-tetramethyl-piperidine-1-oxyl (TEMPOL), which is membrane permeable, and 4-trimethylammonium-2,2,6,6-tetramethyl-piperidine-1-oxyl (CAT-1), which is membrane impermeable, to investigate the area of indomethacin-induced changes in the redox status. Temporal TEMPOL images of the stomach in the NaHCO3-treated group and the indomethacin-treated group were obtained as shown in Figure 3A. The semilogarithmic plot of the TEMPOL image intensity as a function of time showed a larger decay rate in the indomethacin-treated group (0.0237) than that in the NaHCO3-treated group (0.0055; Fig. 3B), in accordance with our previous in vivo ESR study (41). The decay rates of the temporal TEMPOL images in the indomethacin-treated group clearly demonstrated faster rates in most of the stomach area compared with those in the NaHCO3-treated group (Fig. 3C). Temporal CAT-1 images of the stomach were obtained as shown in Figure 3D. The semilogarithmic plot of CAT-1 image intensity as a function of time showed the same decay rate in the indomethacin-treated group (0.0025) as that in the NaHCO3-treated group (0.0025; Fig. 3E), which is also consistent with our in vivo ESR study (41). Interestingly, the decay rates of the temporal CAT-1 images in the indomethacin-treated group showed faster decay rates in some areas of the glandular stomach, but negative decay rate values in most of the forestomach area (Fig. 3F). All the data of CAT-1 decay rates in the indomethacin-treated group are shown in Supplementary Figure S2. In rats #1–#3 (Supplementary Fig. S2), the glandular stomach, which corresponds to the left side of the decay rate image, appeared to have a higher proportion of pixels with a positive decay rate than the forestomach, which corresponds to the right side of decay rate image. In rat #4, pixels with a high decay rate were located in the edge of the glandular stomach. Furthermore, there was a positive correlation between the mean decay rate and the gastric ulcer area (R = 0.977, *p < 0.05).
We have previously reported that the enhanced decay rate of the ESR TEMPOL signal intensity in the rat stomach of indomethacin-induced gastric ulcers was due to intracellular ROS production (41). Hence, we examined whether faster decay rates of the TEMPOL image intensity in the rat stomach of indomethacin-induced gastric ulcers are restored by dimethylthiourea (DMTU), a membrane-permeable ROS scavenger. The decrease in TEMPOL image contrast over 12 min observed in the indomethacin-treated group appeared to be largely suppressed by administration of DMTU together with TEMPOL (Fig. 4A). Furthermore, the decay rate images clearly demonstrated the restoration of indomethacin-induced fast decay rates by DMTU (Fig. 4B). The statistical analysis of all the rats used in this experiment is shown in Figure 4C. The decay rates of the TEMPOL image contrast in the NaHCO3-treated group were significantly enhanced by indomethacin treatment (*p < 0.05), and the enhanced rates were significantly suppressed by DMTU (*p < 0.05; Fig. 4C). However, DMTU itself did not alter the decay rates of the TEMPOL image intensity in the NaHCO3-treated group (Fig. 4B, C).

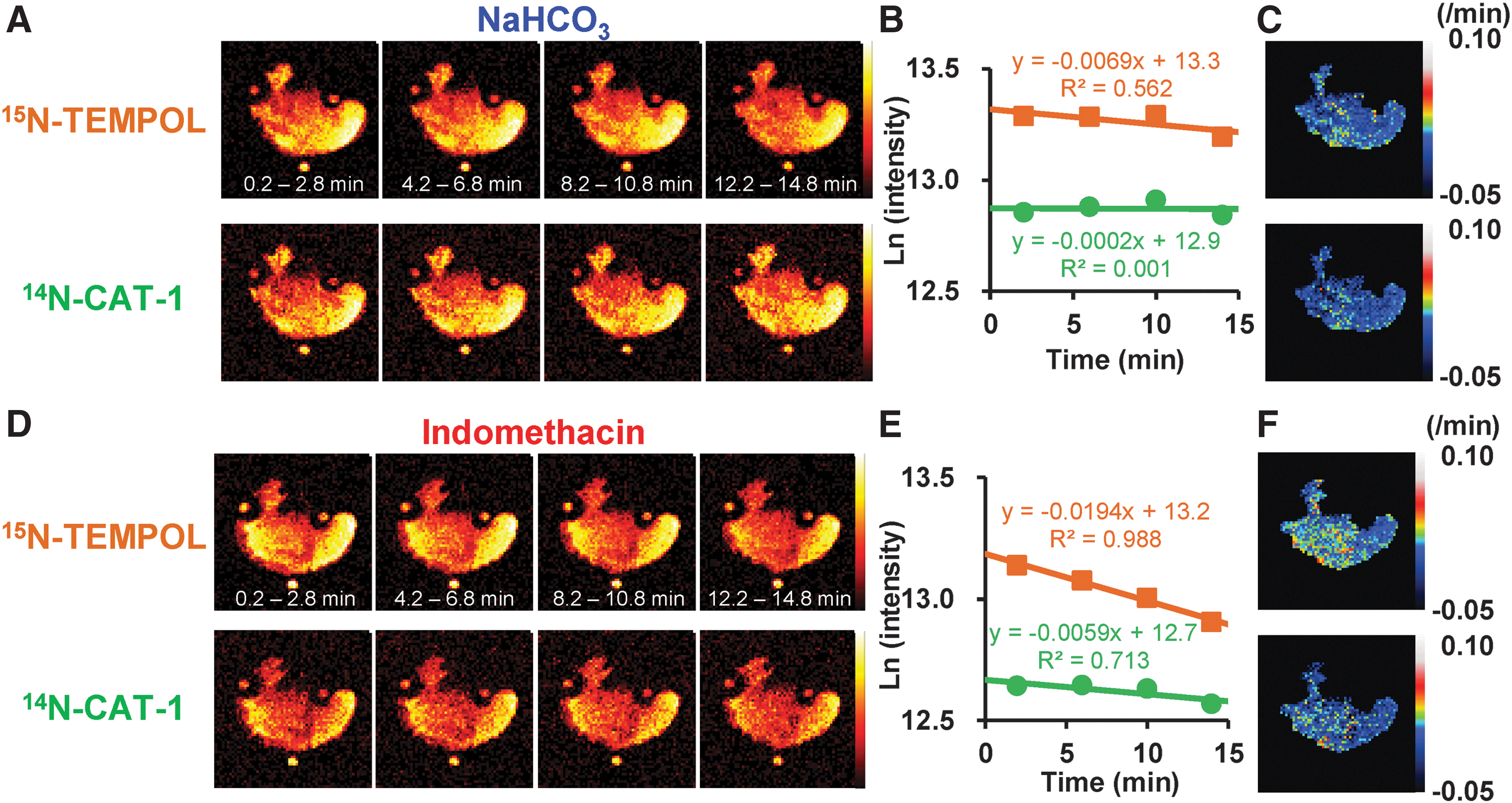
Next, we performed redox imaging of intra- and extracellular compartments of rat stomach with indomethacin-induced gastric ulcers using the OMRI/dual-probe method. Typical data sets of temporal OMRI of an NaHCO3-treated rat and an indomethacin-treated rat are shown in Figure 5A and D, respectively. In the NaHCO3-treated rat, both image contrasts of the intracellular compartment (membrane-permeable 15N-labeled probe) and the extracellular compartment (membrane-impermeable 14N-labeled probe) gave the same shape and barely decreased during OMRI measurements. A semilogarithmic plot of the image intensity of the NaHCO3-treated group as a function of time showed small decay rates of both the 15N-form and 14N-form (Fig. 5B). These decay rates indicated that both nitroxyl probes were barely reduced to their nonparamagnetic forms in the NaHCO3-treated rats. However, in the indomethacin-treated rats, the image contrasts of the intracellular compartment markedly decreased compared with those of the extracellular compartment (Fig. 5D). When the image intensity of the indomethacin-treated group was semilogarithmically plotted against time, the faster decay rate of the 15N-form than that of the 14N-form was confirmed (Fig. 5E). When the decay rate of the TEMPOL image contrast of the indomethacin-treated rat was compared between the dual-probe method and the single-probe method, the decay rate of the 15N-labeled TEMPOL image contrast in the dual imaging (Fig. 5E orange) was comparable with that of the TEMPOL image contrast in the single imaging (Fig. 3B red). When the decay rate of the CAT-1 image contrast of the indomethacin-treated rat was compared, the decay rate of the 14N-CAT-1 image contrast in the dual imaging (Fig. 5E green) was almost the same as that of the CAT-1 image contrast in the single imaging (Fig. 3E red).
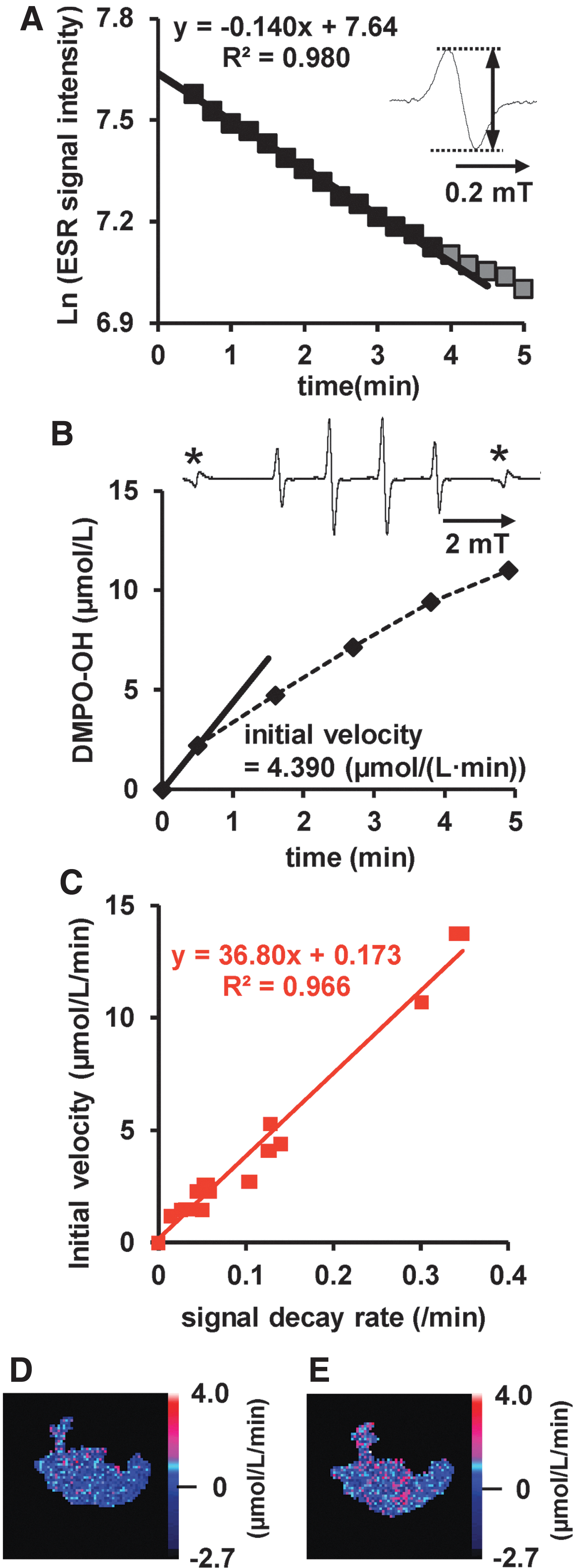
To map the ROS production in rat stomach with indomethacin-induced gastric ulcers, the reactivity of the nitroxyl probes used in this study for ROS was investigated with X-band ESR spectroscopy. The in vitro ESR signal intensity of the nitroxyl probe gradually decreased after the nitroxyl probe was added to the tube containing hydrogen peroxide and iron(II) sulfate (Fig. 6A). The hydroxyl radicals produced by Fenton's reaction were trapped using the spin-trapping reagent, 5,5-dimethyl-1-pyrroline N-oxide (DMPO). The ESR signal intensity of the DMPO-OH spin adduct increased with time (Fig. 6B). The initial velocity of the DMPO-OH formation reaction correlated well with the decay rate of the ESR TEMPOL signal intensity; the regression formula is y = 36.80x + 0.173, where x is the decay rate of the TEMPOL ESR signal and y is the initial velocity of DMPO-OH formation (Fig. 6C; R 2 = 0.966). The initial velocity also correlated well with the decay rate of the ESR signal intensity of 3-methoxycarbonyl-2,2,5,5-tetramethyl-pyrrolidine-1-oxyl (MC-PROXYL) and CAT-1 (Supplementary Fig. S3A and B, respectively). After eliminating the effect of liquid movement on the contrast decay by producing an image differencing between the rate of 15N-form and that of 14N-form, the image differencing was transformed into an image of initial velocity of DMPO-OH formation using the relationship with the TEMPOL decay rates. Because extracellular ROS formation was hardly observed in stomachs with indomethacin-induced ulcers (Fig. 3), the image of initial velocity of DMPO-OH formation roughly reflected the intracellular redox imbalance, including ROS formation. Figure 6D shows the intracellular redox imbalance image of the NaHCO3-treated rat stomach shown in Figure 5A. The rate of intracellular redox metabolism in the NaHCO3-treated rat was low in most of the stomach regions. Figure 6E shows the intracellular redox imbalance image of the indomethacin-treated rat stomach shown in Figure 5D. The rate of intracellular redox metabolism in the indomethacin-treated rat was high in the glandular stomach, while it was quite low in most of the forestomach regions. These findings strongly suggest that intracellular ROS are produced in some regions of the glandular stomach, where gastric ulcers form.
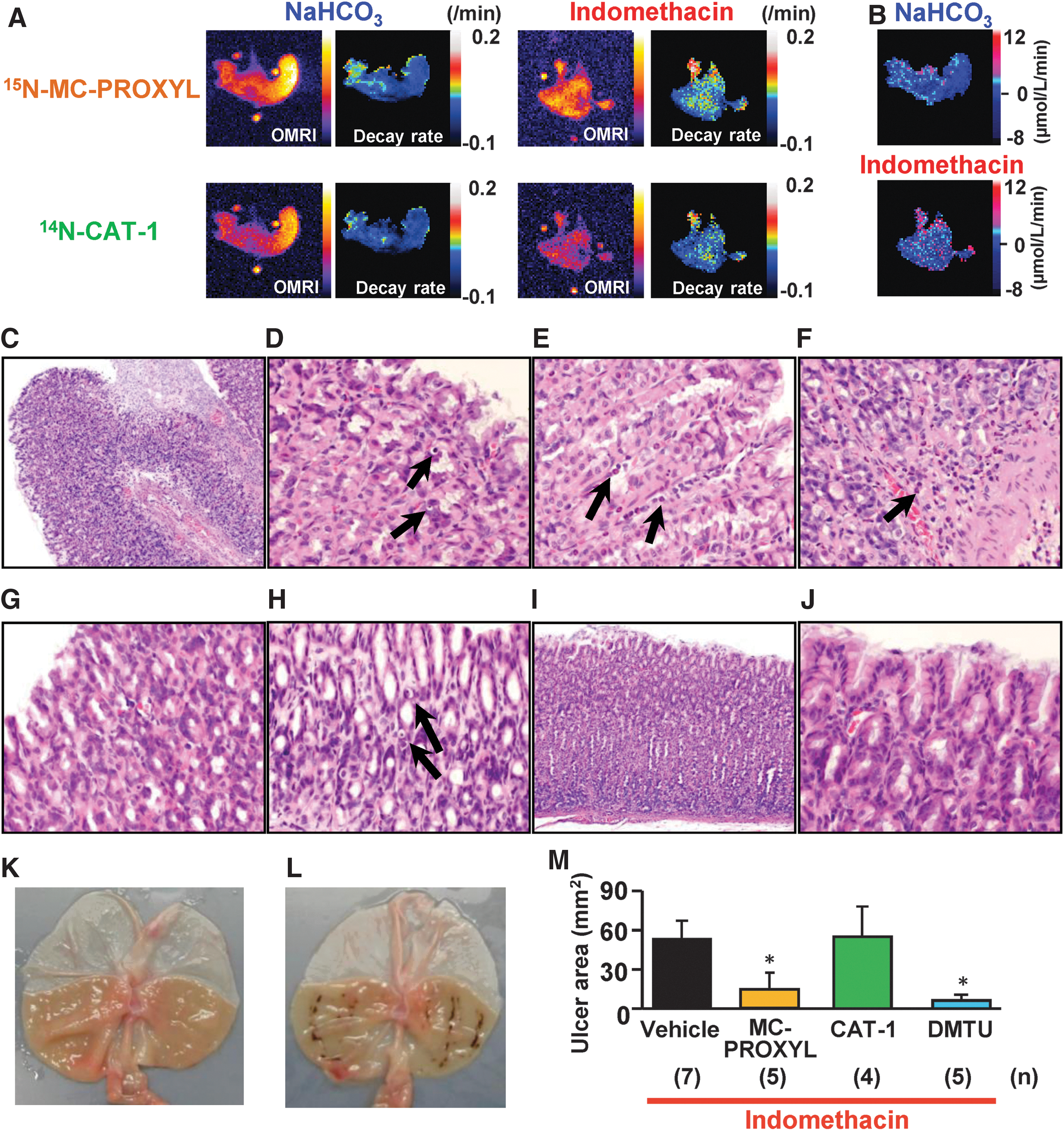
Furthermore, in vivo dual images of the membrane-permeable 15N-labeled MC-PROXYL and the membrane-impermeable 14N-labeled CAT-1 were obtained simultaneously using OMRI (Fig. 7A). In the NaHCO3-treated rat stomach, the decay rates of both 15N-labeled MC-PROXYL and 14N-labeled CAT-1 in the glandular stomach (left side of the image) slightly increased compared with those in the forestomach (Fig. 7A). Figure 7B shows the intracellular redox imbalance image of the NaHCO3-treated rat stomach shown in Figure 7A. The image differencing of 15N-MC-PROXYL decay rates and 14N-CAT-1 decay rates was transformed into an image of initial velocities of the DMPO-OH formation reaction using the corresponding regression equation in Supplementary Figure S3A. In Figure 7B, the intracellular redox imbalance was slightly observed in some spots in the glandular stomach (left side of the image), where decay rates changed in both compartments. In contrast, in the indomethacin-treated rat, the decay rates of 15N-labeled MC-PROXYL markedly increased compared with those of 14N-labeled CAT-1 (Fig. 7A). Figure 7B shows the intracellular redox imbalance image of the indomethacin-treated rat stomach shown in Figure 7A. Intracellular redox imbalance was observed in many of the regions of the stomach. After the OMRI experiment, the concentrations of the probe in the gastric tissue and the stomach washes were determined using X-band ESR spectroscopy (Supplementary Fig. S4). In both groups, the concentration of the membrane-impermeable 14N-CAT-1 in the gastric tissue was lower than that in the stomach washes, whereas the concentration of the membrane-permeable 15N-MC-PROXYL in the gastric tissue was higher than that in the stomach washes (Supplementary Fig. S4). These data confirmed that the membrane-permeable 15N-MC-PROXYL was localized mainly in the gastric tissue, whereas the membrane-impermeable 14N-CAT-1 was not localized in the gastric mucosa but was partially attached to the surface of the gastric mucosa. Furthermore, the involvement of nitroxyl probes in the pathology of indomethacin-induced formation of gastric ulcers was confirmed. The gastric epithelium of one rat showed severe erosion and apoptosis, and moderate infiltration of neutrophils after 1 h of indomethacin treatment (Fig. 7C–F), whereas that of the control was intact (Fig. 7I, J). Pretreatment with 2 mmol/L MC-PROXYL completely suppressed epithelial damage (Fig. 7G), whereas pretreatment with 2 mmol/L CAT-1 did not prevent this damage (Fig. 7H). Typical photos of NaHCO3-treated and indomethacin-treated rat stomachs are shown in Figure 7K and L, respectively. The area of the indomethacin-induced gastric ulcer was also suppressed by MC-PROXYL treatment and by the membrane-permeable antioxidant, DMTU, but not by CAT-1 (Fig. 7M). These results suggest that MC-PROXYL, which showed enhanced decay of the OMRI contrast in the indomethacin group, is also pathologically involved in indomethacin-treated rats.
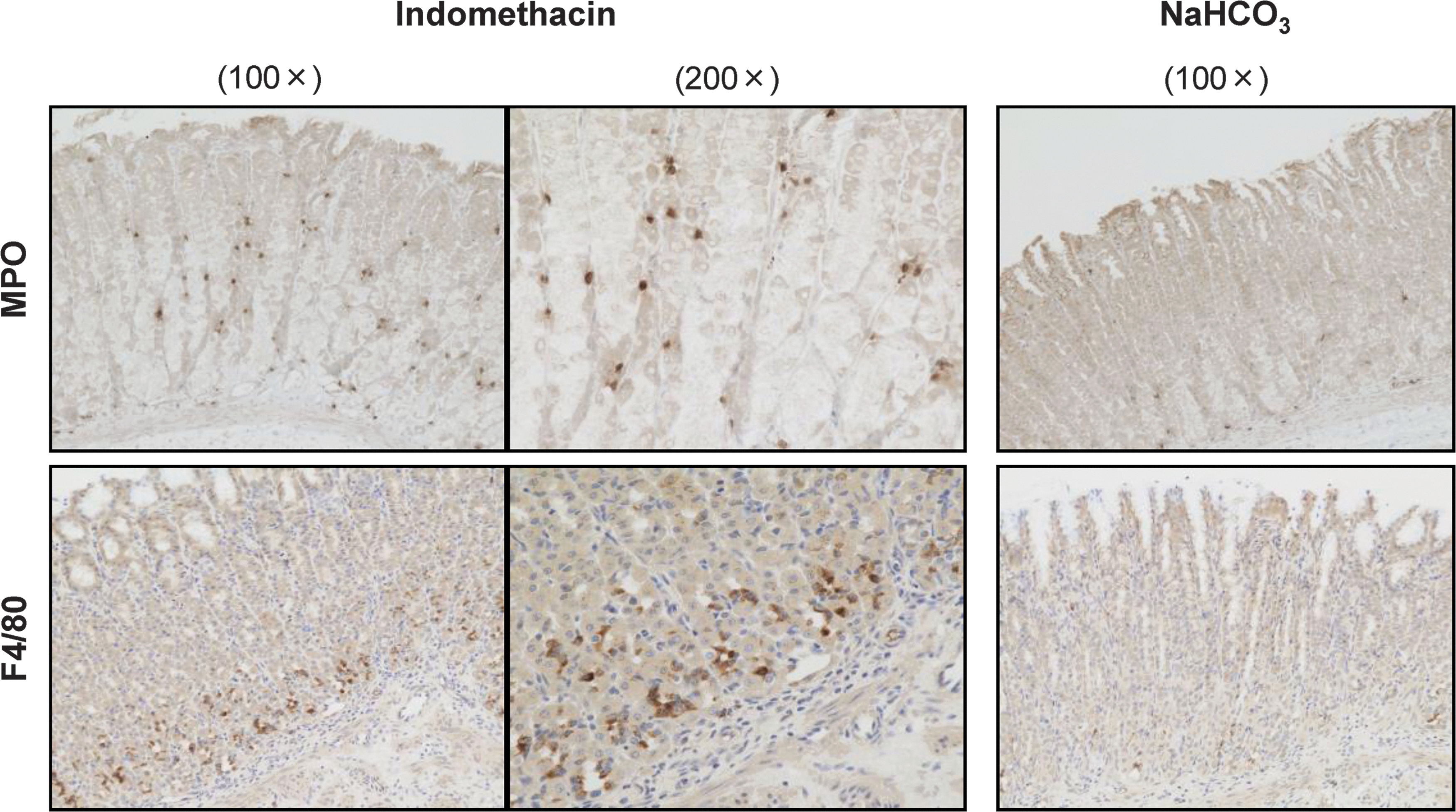
To investigate which cells produce ROS in rat stomach with indomethacin-induced gastric ulcers, immunohistochemical staining of myeloperoxidase (MPO) and F4/80 was performed. As shown in Figure 8, infiltration of MPO-positive cells was observed in the gastric epithelium after 1 h of indomethacin treatment, whereas MPO-positive cells were barely observed in the gastric epithelium of the control. Infiltration of F4/80-positive cells was observed in the bottom of the gastric epithelium after 1 h of indomethacin treatment, whereas there were only a few F4/80-positive cells in the bottom of the gastric epithelium of the control.
Discussion
Using OMRI, we demonstrated that a redox imbalance toward oxidation in rats treated with indomethacin occurred in the gastric mucosal layer, at the surface of the gastric mucosal layer, or in the intracellular compartment of gastric epithelial cells but not in the extracellular compartment of epithelial cells. This is the first study to visualize ROS production in the intracellular compartment in a live rat stomach with indomethacin-induced gastric ulcers using an OMRI/dual-probe method with high spatial resolution.
We selected 2 mmol/L as the concentration of OMRI probes for stomach imaging because the OMRI image intensity of the fiducial markers showed a probe concentration-dependent increase in the range of up to 2 mmol/L, which is consistent with our previous report (29), and most of the orally administered probe solution remained in the stomach during the OMRI. OMRI provides a high-resolution map of the decay rates of nitroxyl probes administered into rodents. Interestingly, in the indomethacin-treated rat stomach, the CAT-1 decay rates differed according to the stomach site, as the enhancement of CAT-1 decay rates was not observed in the forestomach, but in the glandular stomach (Fig. 3F and Supplementary Fig. S2). We showed the functionality of the CAT-1 probe in an in vitro experiment (Supplementary Fig. S3), and we have previously reported the signal decay enhancement of the CAT-1 probe and its recovery by intratracheal administration of the antioxidant enzyme, catalase, together with the probe in the lungs of mice treated with diesel exhaust particles (12). We have previously reported no enhancement of decay rates of CAT-1 ESR signal intensity in the indomethacin-treated rat using in vivo ESR spectroscopy (41). Furthermore, we confirmed that CAT-1 solution administered orally was mostly localized in the gastric cavity, not in the gastric tissue (Supplementary Fig. S4). Based on these results, we expected no increment in CAT-1 decay rates in the overall stomach of indomethacin-treated rats. This discrepancy may stem from the reaction of the CAT-1 probe with ROS such as hydroxyl radicals leaking into the gastric cavity because of the tissue destruction and/or the temporary movement of probe solution to the forestomach due to the peristaltic motion. Severe histological destruction of the gastric epithelium of indomethacin-treated rats was observed (Fig. 7C–F) and high decay rates appeared to be localized in the glandular stomach, where the gastric ulcers form (Supplementary Fig. S2), however, whether the sites of enhanced decay rates corresponded to the position of the tissue destruction could not be investigated in this study. In the area of positive decay rates, mostly seen in the glandular stomach of the indomethacin-treated rat, ROS would be released extracellularly. Both neutrophils and macrophages infiltrating into the inflamed tissue are believed to be ROS sources that can be released extracellularly at the site of infection or intracellularly in the phagolysosome following phagocytosis of bacteria (31). We observed infiltration of MPO-positive cells and F4/80-positive cells into the glandular stomach epithelium of indomethacin-treated rats (Fig. 8). The degree of inflammatory infiltration appears to still be low because the OMRI was performed 1 h after indomethacin treatment, that is, during the early phase of indomethacin-induced gastric ulcer formation. Thus, we believe that the positive signal area may be where extracellular ROS are released from neutrophils and macrophages moderately infiltrating into the glandular stomach. If CAT-1 is oxidized to its oxoammonium cation form by ROS and this oxoammonium cation is moved to a non-ROS-producing area by peristaltic motion, the oxoammonium cation form may be reversed to the CAT-1 radical form because the redox potential toward oxidation of the ROS-producing area would be recovered in the non-ROS producing area. Thus, we believe that the negative signal may be due to movement of the solution that includes the oxidized form by peristaltic motion and the recovery from the oxidized form to the radical form. Mapping of the decay rates enabled us to clearly visualize the difference in the redox status according to the stomach sites. It is difficult to reveal the difference in the redox status using the region of interest (ROI) analysis, as it gave the same rate in the indomethacin-treated rat and the NaHCO3-treated rat when the entire stomach was selected as the ROI.
Because the membrane-permeable MC-PROXYL can pass the blood/brain barrier and the cell membrane, it is widely used for redox measurement of the brain and other organs (20, 47, 51). We showed that the OMRI/dual-probe method using 15N-labeled MC-PROXYL and 14N-CAT-1 is also applicable to redox imaging of the rat stomach. It is important to show that the dual probes used in the OMRI/dual-probe method are localized correctly and that the changes in the redox status in the intracellular and extracellular compartments can be detected simultaneously. Using X-band ESR spectroscopy, we confirmed that a membrane-permeable probe containing MC-PROXYL administered orally permeated into the gastric mucosa, and that a membrane-impermeable probe containing CAT-1 administered orally attached to the inner wall of the gastric epithelium and could not permeate into the gastric mucosa (Supplementary Fig. S4). These results strongly suggest that the membrane-permeable probe and membrane-impermeable probe can be detected simultaneously in the intra- and extracellular compartments of the stomach of rats with indomethacin-induced gastric ulcers.
In this study, DMTU was used as an ROS scavenger because we have previously reported the restoration of enhanced decay rate of in vivo ESR signal intensity by DMTU in indomethacin-treated rats (41). We confirmed that the enhancement of decay rates of the TEMPOL image intensity was due to intracellular ROS production, which is consistent with the results of the in vivo ESR study. This result is also supported by our observations that ulcer formation was suppressed by pretreatment with MC-PROXYL or DMTU, and the ineffectiveness of CAT-1 against gastric ulcers. However, the OMRI image intensity decay would be influenced not only by ROS production but also by dynamic movement of gastric liquid due to peristaltic motion. In fact, we found several pixels with negative values, which means a temporal increase in image intensity in the decay rate image of NaHCO3-treated rats. Furthermore, in the in vivo ESR study and the OMRI/single-probe study, we could not simultaneously obtain the data of the MC-PROXYL experiment and CAT-1 experiment because these techniques cannot separate the multispectral information of probes. Thus, it is difficult to determine the sites and/or the amount of ROS production. In the OMRI/dual-probe method, the peristaltic motion of the stomach would actively move the 15N-MC-PROXYL and 14N-CAT-1 solutions in the gastric cavity, and hence, we assume that the movement of 15N-MC-PROXYL from one pixel to other pixels by peristaltic motion within one imaging time would be the same as that of 14N-CAT-1. An orally administered membrane-permeable probe and its nonmagnetic form converted by ROS and reducing substances would freely move in and out of the cell. The apparent diffusion coefficient of membrane-permeable nitroxyl radicals in the water phase and in the lipid bilayer at 37°C has been reported to be about 4 × 10−10 (m2/s) and 2 × 10−10 (m2/s), respectively (5). The movement distance of membrane-permeable nitroxyl radicals in the intracellular compartment crossing the epithelial cells by simple diffusion within one imaging time (3 min) would be 0.3–0.4 mm, which is smaller than one pixel size (0.5 mm). This means that the effect of diffusion from one pixel to other pixels would be negligible. Hence, subtraction of image intensity rates between the 15N-form and the 14N-form in an identical pixel should eliminate the effect of the peristaltic motion on the decay rate. Moreover, considering the NaHCO3-treated rat results, the effect of one-electron reduction in the nitroxyl probe on the decay rates in the stomach measurement would be small compared with the degree of decay caused by ROS production and there would be a small difference among probes used in this study, in the case of stomach measurements. Furthermore, because the extracellular ROS production is much smaller than the intracellular ROS production in the indomethacin-induced rat stomach, the image differencing would roughly reflect the intracellular ROS production. Therefore, OMRI can simultaneously provide real-time redox information about different compartments in a live animal with high spatial resolution. ESRI is also applicable for dual imaging, although it entails a long and complex process (26). Single-photon emission computed tomography can also provide simultaneous imaging of multiple radioisotopes based on the different energies of the emitted photons, but exposure to radioisotopes is inevitable and quantitative images are limited because of photon scatter and cross talk (3).
The immunohistological study showed the infiltration of both neutrophils and macrophages into the epithelium of the indomethacin-treated rat stomach (Fig. 8). With regard to the location, the neutrophils infiltrated into the gastric epithelium, whereas most of the macrophages infiltrated into the bottom of the gastric epithelium. Because it is thought that the membrane-permeable probe administered into the stomach would permeate the entire epithelium during the acquisition of several OMRI images, considering the apparent diffusion coefficient and Supplementary Figure S4, the membrane-permeable probe would be able to detect ROS production by both neutrophils and macrophages in the gastric epithelium. However, because CAT-1 attaches to the inner wall of the gastric epithelium, which is different from the macrophages' localization region, the membrane-impermeable probe, CAT-1, may not detect ROS production by macrophages unless CAT-1 can easily access the bottom of the epithelium, where macrophages infiltrate on serious injury. Furthermore, the involvement of ROS production by macrophages in the acute gastric lesion induced by indomethacin may be small because indomethacin-induced gastric erosion appears to occur at the upper side of the epithelium (Fig. 7C). Thus, ROS production by activated neutrophils would be mainly associated with the lesion formation. When the gastric epithelial injury is triggered by indomethacin, infiltration of neutrophils into the injured tissue is induced. The infiltrated neutrophils would produce ROS in the phagolysosome to kill bacteria invading the gastric epithelium and some of the produced ROS would be released outside. Large amounts of ROS released by the infiltrated neutrophils would damage not only the bacteria but also the neighboring cells, which may induce further infiltration. The types of ROS produced in mice with indomethacin-induced gastric ulcers remain unknown, but it is presumed that superoxides and hydroxyl radicals, both of which can be detected with OMRI as shown in Figure 2, would be produced from NADPH oxidase and MPO, which exist in activated neutrophils. The mitochondrial electron transport chain has been reported as a source of intracellular ROS in indomethacin-induced gastrointestinal damage (2, 37). We observed some apoptotic cells in the gastric epithelium of indomethacin-treated rats (Fig. 7D). Because apoptosis is reportedly associated with mitochondrial damage (4), intracellular ROS leakage from the mitochondrial electron transport chain may partially be involved in the intracellular ROS production observed with OMRI and ulcer formation in this study.
One practical importance of dual imaging is that the number of experimental animals required for collecting data would decrease. However, the temporal resolution is decreased compared with single imaging because dual imaging takes two times as the single imaging, when the spatial resolution is the same. The image-contrast decay obtained from the OMRI/single-probe method using a nitroxyl probe localizing in the intra- or the extracellular compartment could include the influence of peristaltic motion in the case of the gastrointestinal tract. Hence, we need to pay attention to the redox imaging of the gastrointestinal tract obtained using the OMRI/single-probe method. Imaging of both compartments using dual probes enables us to cancel the effect of the peristaltic motion on the contrast decay by image subtraction and to properly visualize in which compartment the redox imbalance occurs. The biological importance of dual imaging is that elucidating the compartment in which the redox imbalance occurs will help understand the nature and source of ROS, when the finding of dual imaging is combined with findings from other experiments. If only extracellular ROS production is observed with the OMRI/dual-probe method, the ROS origin candidates would be inflammatory cells such as neutrophils and macrophages. Our method in combination with other experiments such as immunohistological staining or OMRI using inhibitors that inactivate inflammatory cells will help identify the origin of ROS and investigate the nature of ROS. We have previously reported that intracellular redox imbalance before the onset of dextran sodium sulfate-induced colitis in mice was changing to be both intra- and extracellular redox imbalance as the severity of colitis increased using in vivo ESR spectroscopy (50). In such a case, the redox imaging obtained using the OMRI/dual-probe method would be effective for non (less)-invasively monitoring the severity of disease and elucidating the link between redox imbalance and disease. In the future, the OMRI/dual-probe method may be clinically applied, which would provide a novel diagnostic approach without endoscopic examination.
This OMRI/dual-probe method is also applicable to mouse experiments. It is important to obtain temporal OMRI images with high sensitivity and spatial resolution to perform mechanistic studies. If an ESR irradiation coil suitable for the target region in a mouse is prepared, redox imaging with high spatial resolution and high sensitivity can be obtained. If it will be confirmed that the in vivo spin clearances of both probes are slow enough for obtaining several OMRI images in a healthy mouse and a diseased or genetically modified mouse using the OMRI/single-probe method, then disease models and genetic modifications of not only the gastrointestinal tract but also of other organs such as the liver and kidney would be applicable. For brain application, direct injection of dual probes into the brain or use of a probe that would stay in the brain blood vessels for extracellular redox imaging would be required for dual imaging of both compartments, because it is generally difficult to permeate a hydrophilic compound in the circulating blood through the blood/brain barrier.
There are some limitations to the application of OMRI to redox imaging of the stomach or other organs. In the OMRI/single-probe method for stomach imaging, the decay rates of OMRI image intensity include the effect of the peristaltic motion of the stomach. In the OMRI/dual-probe method, the effect of the peristaltic motion on the decay rates is eliminated, but it is difficult to simultaneously evaluate the intra- and extracellular ROS production. If the movement of the gastric liquid due to the peristaltic motion is monitored by another imaging method, such as MRI for small animals, and its effect on the decay rates of the nitroxyl probe could be estimated, then ROS production in both compartments could be simultaneously evaluated. However, in the case of intravenous injection of the nitroxyl probe, the reduction and metabolism of the nitroxyl probe may influence the decay rates. In fact, the rate of ESR signal decay of the nitroxyl probe reduced by ascorbic acid has been reported to correlate with the redox potential of the nitroxyl probe (46). In such cases, nitroxyl probes that are less reactive toward the reducing substances, but more reactive toward ROS should be selected for the OMRI/dual-probe method.
The OMRI/dual-probe method may be a novel tool for less invasive evaluation of the intracellular ROS-producing area with high resolution in small animals with NSAID-induced gastric ulcers. Because it usually takes 10–15 min to obtain a redox map, it would be suitable for efficacy evaluation of drug candidate compounds discovered by screening. Furthermore, the OMRI probe, with which an intracellular redox change was detected in rats with indomethacin-induced gastric ulcers, showed restoration of gastric mucosal injury at the same concentration as in the OMRI measurement. We expect that progress in the development of OMRI probes with a medicinal effect may lead to theranostics, which are developed for diagnosis and treatment of diseases (14).
Materials and Methods
All procedures and animal care were approved by the Ethics Committee of Animal Experiments, Faculty of Pharmaceutical Sciences, Kyushu University (Fukuoka, Japan) (animal ethical permission number: A19-055-0). The study protocol was conducted according to the Guidelines for Animal Experiments of the Faculty of Pharmaceutical Sciences of Kyushu University and the ARRIVE guidelines.
Chemicals
TEMPOL (176141-25G), N,N′-dimethylthiourea (D188700-100G), indomethacin (I8280-5G), and ethyl carbamate (U2500-100G) were purchased from Sigma-Aldrich Chemical Co. (St. Louis, MO). CAT-1 (T506) was purchased from Molecular Probes, Inc. (Eugene, OR). 14N-MC-PROXYL, 15N-MC-PROXYL, and 15N-TEMPOL were synthesized by our research team as described previously (34, 40). DMPO (LM-2110) was purchased from LABOTEC Co., Ltd. (Tokyo, Japan). NaHCO3 (199-05985), hydrochloric acid (080-01066), iron(II) sulfate heptahydrate (094-02942), and hydrogen peroxide (081-04215) were purchased from Wako Pure Chemical Industries, Ltd. (Osaka, Japan). All other chemicals were available commercially and were of reagent grade.
Animal treatment
Male Sprague-Dawley rats (5 weeks old, 120–160 g) were purchased from Kyudo Co. (Tosu, Japan) and acclimatized for 1 week before experiments under the conventional housing environment. Rats were housed in open cages (n = 4–5 per cage). Food (MF; Oriental Yeast Co., Tokyo, Japan) and water were available ad libitum. Animals were fasted for 24 h with free access to water for up to 1 h before the experiment. Gastric mucosal ulcers were induced by oral administration of indomethacin (30 mg/kg) in a 5% NaHCO3 solution.
OMRI measurement
Indomethacin (30 mg/kg) or NaHCO3 was orally administered to rats. One hour later, a 3-cm incision was made on the upper abdomen of each rat under anesthesia (ethyl carbamate, 2 g/kg body weight). In the DMTU experiment, after 1 mL of TEMPOL (4 mmol/L) and 1 mL of DMTU (133 mmol/L) were mixed, 1.5 mL of the mixture was orally administered to the rats (final concentration of TEMPOL and DMTU was 2 and 67 mmol/L, respectively). The ESR surface coil and fiducial markers containing 1, 1.5, or 2 mmol/L of the same kind of probe solution, which was orally administered, were placed on the stomach. OMRI of the gastric region was started 0.2 min after oral administration of the nitroxyl probe or the mixture of 14N-labeled nitroxyl probe and 15N-labeled nitroxyl probe. OMRI images of the dual probes with different membrane permeabilities (combination of 15N-TEMPOL and 14N-CAT-1, or 15N-MC-PROXYL and 14N-CAT-1) were obtained as reported by Utsumi et al. (40). OMRI experiments were undertaken on a custom-built (Philips Research Laboratories, Hamburg, Germany) human whole-body magnet (ø 79 cm, length 125 cm) with a surface coil for ESR irradiation (24 mm i.d.) customized for imaging of the stomach (Supplementary Fig. S1A). The resonant circuit consisted of a single-turn loop coil, a parallel coaxial line formed by 50-Ω coaxial cables, a half-wave line balun, and trimmer capacitors for matching and tuning, as reported previously (27). The operating frequency of the ESR one-turn coil was 220.6 MHz. In the single-probe imaging experiments, the ESR field strength was 7.5 mT. In the simultaneous imaging experiments, the ESR field strength was 6.0125 mT for 14N-CAT-1 and 6.565 mT for 15N-MC-PROXYL. The nuclear magnetic resonance (NMR) field strength was 14.530 mT and the NMR frequency was 617 kHz for all OMRI experiments. Typical OMRI scan conditions were as follows: repetition time (TR), 1200 ms; echo time (TE), 25 ms; ESR irradiation time (TESR), 400 ms; number of averages, 1; 64 phase-encoding steps; and ESR power, 12.1 W. The pixel size was 0.5 × 0.5 mm with a slice thickness of 8 mm. The field of view (32 mm) was represented by a 64 × 64 matrix. Scanning time was 79.2 s for the single-probe imaging and 156.0 s for the simultaneous imaging. According to Li et al. (21), the specific absorption rates in our OMRI experiments were estimated to be 5.2 W/kg. Four images with ESR irradiation were undertaken every 3 min for the single-probe imaging or every 4 min for the simultaneous imaging, and then, one image without ESR irradiation was taken. OMRI images and contrast decay rates were processed with an Excel macro program and ImageJ 1.40g software (35). Conventional MRI experiments were done on a 0.2-T MRI system (Hitachi Medical Corporation, Tokyo, Japan) using a standard T1-weighted enhanced pulse sequence. Typical scan conditions for MRI were: TR, 500 ms; TE, 25 ms; number of averages, 4; and 64 phase-encoding steps. The slice thickness was 2.5 mm. The field of view (200 mm) is represented by a 64 × 64 matrix. OMRI images were superimposed with the MRI image by registering the fiducial markers.
In vitro ESR study of the reaction between nitroxyl probes and ROS
TEMPOL, MC-PROXYL, CAT-1 (final concentration: 10 μmol/L), or DMPO (final concentration: 1 mol/L) was added to an Eppendorf tube containing hydrogen peroxide (final concentration: 50 μmol/L, pH 2), and ferrous sulfate (final concentration: 10 μmol/L) was added to the tube. The spectra of the nitroxyl probe and DMPO-OH spin adduct were recorded using X-band ESR spectroscopy JES-FA100 equipped with X-band microwave unit ES-FA100/BU (JEOL Ltd., Tokyo, Japan). The decay rate of the nitroxyl probe ESR signal intensity was determined by the slope of the semilogarithmic plot of ESR signal intensity of the center peak as a function of time (min; Fig. 6A). The initial velocity of the DMPO-OH formation reaction was determined by the slope of the line through points at 0 and 0.5 min in the plot of the DMPO-OH ESR signal peak area as a function of time (min; Fig. 6B). The initial velocities of the DMPO-OH formation reaction were plotted as a function of decay rates of the nitroxyl probe ESR signal intensity and the regression formula was obtained. Typical X-band ESR measurement conditions for the spin probing experiment were ESR magnetic field, 336.0 ± 0.4 mT; time constant, 0.3 s; sweep time, 10 s; number of averages, 1; modulation, 0.2 mT; and ESR power, 10 mW. Typical X-band ESR measurement conditions for the spin trapping experiment were ESR magnetic field, 336 ± 5 mT; time constant, 0.3 s; sweep time, 1 min; number of averages, 1; modulation, 0.1 mT; and ESR power, 5 mW.
Determination of probe distribution in the stomach by X-band ESR spectroscopy
14N-MC-PROXYL or 14N-CAT-1 solution (1.5 mL of 2 mmol/L) was administered orally 1 h after indomethacin treatment. After 15 min, the gastric tissue, the remaining solution in the stomach, and the stomach washes (5 mL) using phosphate-buffered saline (pH 7.4) were collected. The collected gastric tissue in phosphate-buffered saline (5 mL/g tissue) was homogenized using POLYTRON-Aggregate (KINEMATICA AG, Luzern, Switzerland). The probe concentration in the gastric tissue homogenate, the remaining solution in the stomach, and the stomach washes were determined by X-band ESR spectroscopy JES-FA100 equipped with X-band microwave unit ES-FA100/BU (JEOL Ltd.). Typical X-band ESR measurement conditions were ESR magnetic field, 337.7 ± 5 mT; time constant, 0.3 s; sweep time, 2 min; number of averages, 1; modulation, 0.1 mT; and ESR power, 10 mW.
Histology and microscopy evaluation of gastric mucosal injury
15N-MC-PROXYL solution or 14N-CAT-1 solution (1.5 mL of 2 mmol/L) was administered via the oral route 15 min before indomethacin treatment, and then, 1 h after, specimens of mucosal tissue were collected from the gastric corpus, pyloric, and cardiac regions. All specimens were fixed overnight in 10% neutral-buffered formalin and embedded in paraffin. Sections (thickness, 5 μm) were cut, mounted on glass slides, dried overnight, and stained with hematoxylin and eosin.
To examine the effect of nitroxyl radicals on the formation of lesions in the gastric mucosa, 14N-MC-PROXYL, 14N-CAT-1, or DMTU (0.18 mmol/kg at a time) was administered orally 5 min before, and 1 and 2 h after indomethacin treatment. The extent of gastric mucosal injury in rats treated with indomethacin was investigated by microscopy. Stomachs were removed, inflated with 10 mL of 1% formaldehyde, and opened along the greater curvature. The ulcer area (mm2 per glandular stomach) was determined under a dissecting microscope with a square grid micrometer.
Immunostaining
Rat stomach tissue samples were collected from the gastric corpus and cardiac regions 1 h after indomethacin treatment, fixed overnight in 10% neutral-buffered formalin, and embedded in paraffin. The tissue blocks were sectioned at 10 μm thickness using a microtome and the tissue sections were mounted on glass slides. For immunostaining, after incubation with 3% H2O2 and skim milk, sections were incubated with the appropriate primary antibody at 4°C overnight. Monoclonal antibodies for F4/80 (T-2006) purchased from BMA BIOMEDICALS (Augst, Switzerland) were used to detect macrophages. Rabbit anti-MPO antibodies (ab9535) purchased from Abcam (Cambridge, United Kingdom) were used to detect neutrophils. Next, tissue sections were washed in phosphate-buffered saline and incubated with secondary antibodies labeled with horseradish peroxidase for 30 min. For detection of horseradish peroxidase, sections were stained with the Vectastain ABC Kit (Vector Laboratories, Burlingame, CA) and DAB Reagent Set (SeraCare Life Sciences, Milford, MA). Images were then obtained with a confocal laser microscope equipped with a digital camera.
Statistical analyses
Statistical analyses were carried out using StatView 5.0. Data were analyzed by two-way analysis of variance with the Tukey–Kramer test as a post-hoc test. Data are mean ± standard error. A value of p < 0.05 was considered statistically significant.
Footnotes
Acknowledgments
This work was supported by Grants-in-Aid for Scientific Research (A) (grant number 22249003) and for Young Scientists (B) (17790035 and 23790049) from the Ministry of Education, Culture, Sports, Science and Technology of Japan. Support was also provided by the Innovation Center for Medical Redox Navigation from the Ministry of Education, Culture, Sports, Science and Technology of Japan, Development of Advanced Measurement and Analysis Systems from the Japan Science and Technology Agency (JST), and by the JSPS Core-to-Core Program (19004) from the Japan Society for the Promotion of Science. The authors acknowledge Prof. L.J. Berliner (University of Denver) for critical comments regarding this article, and Prof. M. Tsuneyoshi (Fukuoka Sanno Hospital) and Prof. T. Yao (Juntendo University) for scientific support and advice on the histological study. They thank Michal Bell, PhD, from Edanz Group for editing a draft of this article.
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.