
Abstract
Nonalcoholic fatty liver disease (NAFLD) is the most common cause of chronic liver disease in children. Several studies suggest that the improvement of oxidative stress is suggested as a possible therapeutic strategy for pediatric nonalcoholic steatohepatitis. We performed a randomized, double-blind placebo-controlled trial to test the potential efficacy, assessed by improvement of oxidative stress parameters and liver ultrasound, and tolerability of a mixture of vitamin E and hydroxytyrosol (HXT) in adolescents with biopsy-proven NAFLD. Four hundred forty consecutive patients were screened, 80 of these with biopsy-proven NAFLD were enrolled. Forty patients received an oral dose of HXT and vitamin E and 40 children received the capsules of placebo for 4 months. Seventy patients completed the study. Patients in the treatment arm showed a decrease of insulin resistance (IR), triglyceride levels, oxidative stress parameters, and steatosis grade. Noteworthy, the steatosis improvement correlates with the levels of advanced glycation end products and carbonylated proteins. The HXT and vitamin E treatment improved the main oxidative stress parameters, IR, and steatosis in children with NAFLD. The use of two natural molecules that may have antioxidant effects seems a promising strategy that could be easily diet integrated to improve NAFLD-related liver damage in children.
Introduction
Nonalcoholic fatty liver disease (NAFLD) is the main cause of chronic liver disease in the pediatric population of the western world. The true prevalence is unknown, but several studies have shown that it varies from 3% to 12% of the general pediatric population with an increase of up to 70% in obese children (5).
NAFLD exhibits a wide spectrum of hepatic disorders, ranging from simple steatosis to nonalcoholic steatohepatitis (NASH) with or without fibrosis, caused by multiple interlocked factors (i.e., lifestyle, epigenetics, and genetics) (5). These factors lead to the development and progression of NAFLD by triggering several molecular damaging pathways. Among them, oxidative stress plays a crucial role. In fact, a huge amount of studies, in animal models and humans, have shown that oxidative stress is involved in the progression of liver injury from simple steatosis to NASH (4). Excessive reactive oxygen species (ROS) and reactive nitrogen species (RNS) attack several macromolecules causing several irreversible oxidative modifications, including protein carbonylation and S-nitrosylation, and induce the production of advanced oxidation protein products (AOPPs) and advanced glycation end products (AGEs) (8).
This is an innovative study because the use of two natural molecules that may have antioxidant effects and improve nonalcoholic fatty liver disease-related liver damage may provide a possible therapeutic strategy that could be integrated to the diet for long-term periods. Moreover, the promising results are certainly attributable to the pharmaceutical formulation used, which differs from all those commercially available for the delivery of the active ingredients in extra virgin olive oil. Indeed, the lipophilic vehicle substantially increases the absorption and bioavailability of the active ingredients and synergizes them, for its richness in polyphenols by itself, increasing the biological activity observed.
In light of these data, some studies have evaluated the effects of therapy with natural and synthetic antioxidants, alone or in combination, in the population affected by NAFLD (2).
The antioxidant property of vitamin E is mainly due to the hydroxyl group on the aromatic ring of tocochromanol, a hydrogen donor able to neutralize free radicals or ROS. Recently, the antioxidant efficacy of vitamin E on RNS has attracted more attention. The RNS include nitric oxide, nitrogen dioxide, and peroxynitrite (2). Vitamin E has been used as monotherapy or with other agents to treat NAFLD or NASH in different clinical trials of variable duration (from 24 weeks to >2 years) reporting a both biochemical and histological improvement of the liver parameters (steatosis, lobular inflammation, balloon degeneration, and fibrosis) (2, 6). Some of the limitations of vitamin E effects could be due to its bioavailability when administered by oral preparations at different dosage and by lack of studies on the effects in long-term use. Interestingly, some studies suggest that vitamin E could be used in combination with other antioxidants to obtain synergistic or additive beneficial effects on the liver damage (2).
Recently, a role of hydroxytyrosol (HXT), a simple phenol of extra virgin olive oil, to improve body composition parameters and inflammation and to modulate the antioxidant profile in healthy volunteers has been reported (1). Moreover, HXT exhibits protective effects on fatty liver in various experimental models (3). In particular, HXT reduced hepatic steatosis, inflammation, and ballooning. This process is associated with the modulation of many enzymatic pathways that promote the oxidation of fatty acids, reducing inflammation, and prevent liver damage (3).
In light of this evidence, the aim of the present study was to undertake a proof-of-concept, randomized, double-blind placebo-controlled trial (RCT) to test the potential efficacy, assessed by improvement of oxidative stress parameters and liver ultrasound, and tolerability of a mixture of vitamin E and HXT in children and adolescents with biopsy-proven NAFLD.
Results
In our study, between March 2017 and April 2018, 440 patients were screened and 80 of these with biopsy-proven NAFLD were enrolled.
Forty patients received an oral dose of 7.5 mg of HXT and 10 mg of vitamin E (treatment arm) and 40 children received the capsules of placebo for 4 months (placebo arm). Seventy patients completed the study; five patients from the treatment arm and five patients from the placebo arm were lost to follow-up. There were no significant adverse events. The dropouts from the treated arm were not associated with any study adverse events but were due to the refusal of children and parents to continue the treatment. Hepatic steatosis at ultrasound was assessed in all enrolled patients: it was severe in 30 (37%) patients, moderate in 34 (42%), mild-to-moderate in 11 (13.5%), and mild in 6 (7.5%). Based on body mass index (BMI), the degree of overweight and/or obesity of the patients was established. Fifteen patients (18.5%) had a BMI >85th percentile, 25 (30.8%) with BMI >90th percentile, and 41 (50.6%) were severely obese (BMI >97th percentile). Dyslipidemia was present in 13 patients (16%), 5 (6.2%) presented with hypercholesterolemia, 7 (8.6%) patients with hypertriglyceridemia, 1 (1.2%) patient with a combined form. In 19 patients (23.5%), hypertension, systolic blood pressure/diastolic blood pressure >95th percentile, was present.
As reported in Table 1, after 4 months by the start of the trial, the children enrolled in the placebo arm exhibited no changes in anthropometrical and biochemical parameters, whereas a statistically significant reduction in the levels of triglycerides and fasting insulin, and improvement in homeostatic model assessment of insulin resistance (HOMA-IR) was found in the treatment arm (Table 2).
Clinical and Laboratory Variables in Placebo and Treatment Arms at Baseline and 4 Months
The significant values are shown in bold.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; DBP, diastolic blood pressure; GGT, γ-glutamyl transpeptidase; HOMA-IR, homeostatic model assessment of insulin resistance; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; SD, standard deviation; WC, waist circumference.
Oxidative Stress Serum and Plasma Biomarkers in Placebo and Treatment Arms
The significant values are shown in bold.
AGEs, advanced glycation end products; AOPPs, advanced oxidation protein products; GSH, reduced glutathione; GSSG, oxidized glutathione; HXT, hydroxytyrosol; PCOs, carbonylated proteins; SNOPs, S-nitrosylated proteins.
Next, several oxidative stress parameters were evaluated as primary endpoint of the study. Table 2 shows several statistically significant changes in both placebo and treatment arms after 4 months. In particular, levels of reduced glutathione (GSH) and the ratio between GSH and oxidized glutathione (GSSG), and vitamin E levels were increased in children treated with placebo. There were many more such changes in children treated with HXT plus vitamin E. In fact, this group of patients displayed increased levels of both forms of glutathione and of GSH/GSSG ratio, and an expected increment of vitamin E and HXT levels. Moreover, after 4 months, the analysis revealed a significant decrease of carbonylated proteins (PCOs), S-nitrosylated proteins (SNOPs), and AGEs, whereas no statistically significant change of AOPPs in children from the treatment arm was observed.
Improvement in liver steatosis was the secondary outcome of the trial. In the treatment arm, there was a significant reduction of severe steatosis, with a significant increase in mild steatosis. In fact, steatosis was absent in two (5.7%) children after treatment (p < 0.05). No difference on steatosis degree in the placebo group (Table 3).
Liver Steatosis Characteristics in Treatment and Placebo Arms at Baseline and at the End of the Study (4 Months)
The significant values are shown in bold.
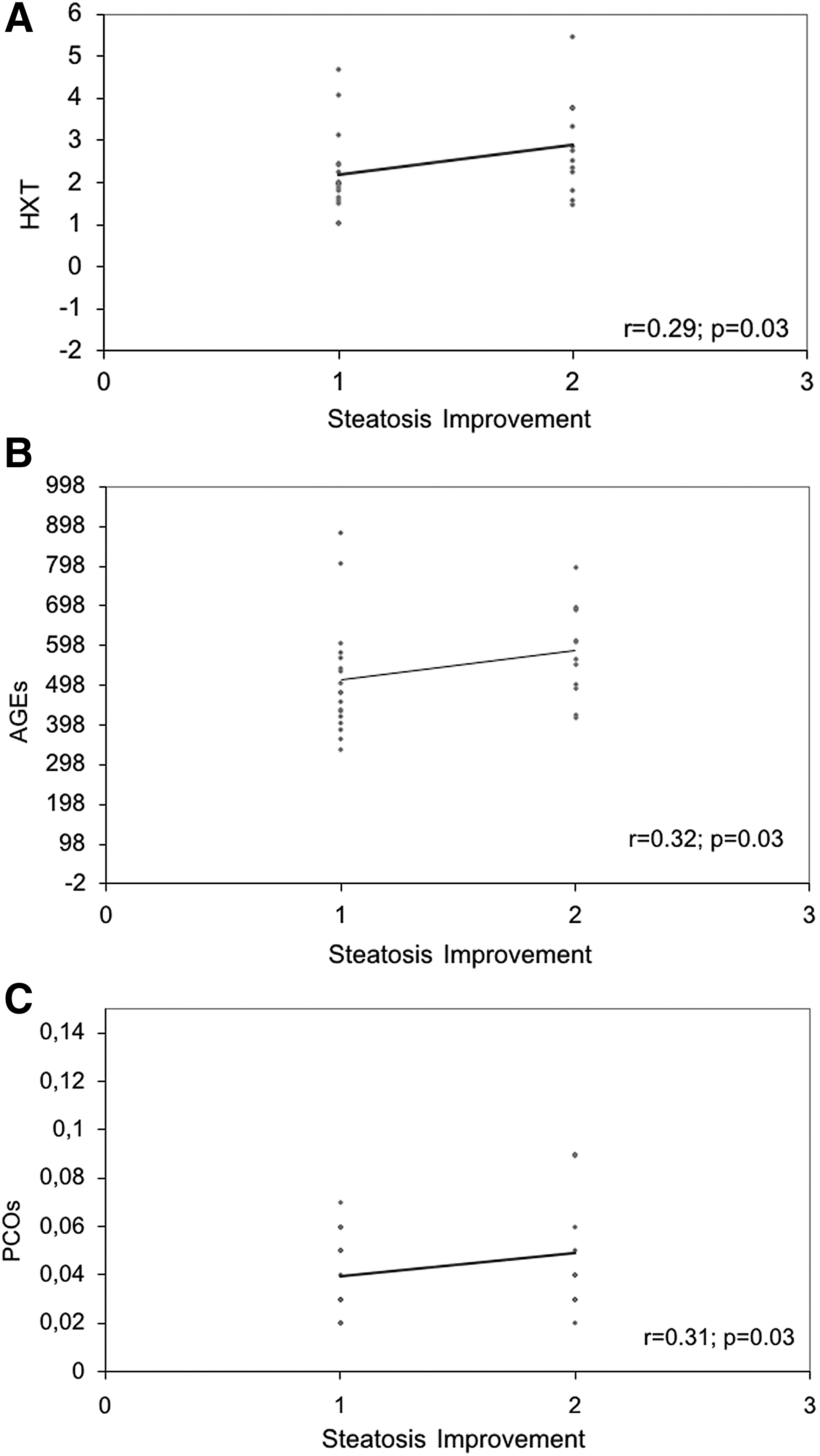
Finally, since only the treatment arm exhibited an improvement of steatosis, we performed a correlation analysis among these factors and oxidative stress parameters after 4 months of treatment.
Pearson's correlation analysis, in treatment arm, showed that the improvement of steatosis negatively correlated with the GSH/GSSG ratio (r = −0.23, p = 0.05) and positively correlated with the levels of HXT (r = 0.29, p = 0.03), AGEs (r = 0.32, p = 0.03), and PCOs (r = 0.31, p = 0.03) (Fig. 1A–C).
Among the metabolic parameters, fasting insulin and consequently HOMA-IR positively correlated with the levels of vitamin E (r = 0.29, p = 0.03) and PCOs (r = 0.42, p = 0.01), whereas triglycerides positively correlated with the GSH/GSSG ratio (r = 0.25, p = 0.04) and AOPPs (r = 0.41, p = 0.02).
Discussion
This study is the first proof-of-concept study that points to investigate the tolerability and effects of combined therapy with HXT and vitamin E in children with NAFLD.
The combined therapy with HXT and vitamin E was found to be well tolerated by children with NAFLD enrolled in the study. Different from the placebo, the treatment induced several changes in oxidative stress parameters, improvement of steatosis, and some metabolic parameters. This is consistent with the increased concentrations of vitamin E and HXT at T1, confirming the successful intake of the drug by patients.
Data demonstrated that after 4 months the anthropometric parameters remained almost unchanged in both groups (placebo and treatment arms). However, children in the treatment arm showed a concomitant reduction of fasting insulin and HOMA-IR. It is known that the reduction of insulin resistance (IR) is a very important result because it represents one of the predisposing factors for the progression of NAFLD toward NASH, and it has been already reported that vitamin E is able to improve IR in animal models and humans (2).
Interestingly, we found that the IR parameters (fasting insulin and HOMA-IR) positively correlated with the levels of vitamin E and PCOs. The association between changes in IR and PCOs is not a new concept. Indeed, it has been reported that serum protein carbonylation may serve as biomarker in patients with type 2 diabetes, and increased protein carbonylation is a sign of severe oxidative damage and disease-related protein dysfunctions (7).
Interestingly, the treatment with HXT and vitamin E also reduced liver triglycerides content, which exhibited a significant positive correlation with the GSH/GSSG ratio and AOPP levels, even if there are no significant changes in the levels of AOPPs during the treatment. This implies that the amelioration of triglycerides could be associated, as previously suggested by Witko-Sarsat et al. (9), with oxidative modification of low-density lipoproteins (LDLs), even the mechanism remains to be explored.
Our data also demonstrated that the treatment with HXT and vitamin E caused a statistically significant increase of GSH and GSSG levels and a decrease of the levels of PCOs, SNOPs, and AGEs.
Considering the biochemistry of vitamin E and HXT, we can certainly speculate that its significant improvement of oxidative stress biomarkers may be due to the antioxidant effect of the two bioactive compounds administered. Vitamin E, in fact, is widely known as one of the most potent antioxidants in nature (2), and several studies demonstrated the potential antioxidant activity of HXT in stress-related disorders (3).
According to the data we acquired here following 4 months of treatment with vitamin E and HXT, we observed improvement of steatosis, as evaluated by ultrasound.
The beneficial effect of the combination of the two molecules on steatosis could result from either direct or indirect consequences of oxidative stress parameters' ameliorations. However, our data showed that the improvement of steatosis positively correlated with HXT, AGEs, and PCOs levels, suggesting that the correction of oxidative parameters by the antioxidant therapy is one of the promising targets for pediatric NASH.
The main limitation of this proof-of-concept study is the use of ultrasound to quantify liver steatosis, although we plan to perform liver biopsies after a longer follow-up time, even if these will be performed for clinical reasons and not for trial evaluation. The second limitation is that we did not evaluate the possible contribution of the single treatment because of lack of HXT and vitamin E arm alone. The third limitation is that 4 months are not enough to judge the long-term efficacy of a treatment for liver steatosis.
In conclusion, 4 months of treatment with HXT and vitamin E is enough to improve the main oxidative stress parameters, IR, and steatosis in children with NAFLD.
The effect of long-term treatment with HXT and vitamin E with respect to reversal of hepatic injury in NASH, as well as the analysis of the other oxidative stress parameters with respect to histologic pattern, remain to be defined in a possible extension of this trial.
Notes
Study population and design
Eighty-one white European patients (aged 4–16 years) with NAFLD, referred to the Hepato-Metabolic Department of “Bambino Gesù” Children's Hospital (Rome, Italy) between March 2017 and April 2018, were enrolled in the present study (Supplementary Fig. S1). The diagnosis of NAFLD was performed according to the guidelines of the European Society of Pediatric Gastroenterology, Hepatology and Nutrition. The children were eligible for the study if they were between 4 and 16 years of age, had a liver steatosis, alanine aminotransferase (ALT) levels <10 upper limit of normal, and no laboratory and/or clinical signs of liver decompensation. Moreover, in all children, other causes of liver disease (i.e., viral liver disease, autoimmune hepatitis, Wilson's disease, and α-1-antitrypsin deficiency), celiac disease, alcohol consumption, use of drugs known to induce fatty liver were excluded.
The RCT was undertaken to examine the efficacy and safety of a mixture of HXT and vitamin E orally versus identical placebo for 16 weeks on hepatic steatosis and metabolic parameters in children and adolescents with biopsy-proven NAFLD.
The pharmaceutical formulation was composed of a hard gelatin enteric-coated (Eudraguard® natural; Evonik Industries AG, Essen, Germany) capsule (Fenolia™; P&P Farma Srl, Turin, Italy) containing 3.75 mg of HXT from a standardized olive extract (elaVida™; DSM, Heerlen, The Netherlands) and 5 mg of DL-α-tocopheryl acetate, conveyed in extra virgin organic olive oil. Placebo capsule formulation was the same of what described above but without the elaVida extract.
Patients were randomized to receive two capsules combining 7.5 mg of HXT and 10 mg of vitamin E (treatment arm) or identical capsules as placebo (placebo arm) per day. The dosage of the HXT and vitamin E intervention was determined based on the available evidence in obese patients with NAFLD.
The computer-generated randomization sequence assigned the participants in a 1:1 ratio to treatment arm or placebo arm. A statistician, who was blinded to participants' clinical data and did not participate in patients' clinical care, generated the allocation sequence and assigned participants to their group. Only the statistician had access to the treatment codes, and participants and investigators were blinded to the treatment for the duration of the study.
Additionally, all patients were included in a lifestyle intervention program consisting of a hypocaloric diet [25–30 kcal/(kg·d)] and regular physical exercise (twice-weekly 2-h physical activity).
The compliance with treatment was monitored at each visit by counting the returned capsules. Moreover, adverse effects were recorded by the principal investigator. Anthropometric measurements and laboratory data were collected at baseline and 4 months. We defined changes in oxidative stress parameters and “marker” of the evolution of NAFLD as the primary outcome of the present proof-of-concept trial. The secondary outcomes were the improvement of hepatic steatosis.
This study was registered on July 26, 2016, in
Anthropometrical and biochemical measurements
Anthropometric measurements and laboratory tests including liver enzymes and glucoinsulinemic and lipids profiles with liver echography were performed at baseline and repeated at 4 months.
The body weight and height were measured with the patients wearing underwear. BMI (kg/m2) and waist circumference were calculated as described previously.
Serum glucose, lipid profile (triglycerides, cholesterol-total, high-density lipoprotein cholesterol, and LDL), liver function tests (aspartate aminotransferase and ALT, gamma-glutamyl transpeptidase [GGT], albumin, and international normalized ratio), fasting plasma glucose, and insulin were measured in all patients after an overnight 12-h fasting. IR was assessed by the HOMA: HOMA-IR = [insulin0 (μIU/mL) × glucose0 (mM)]/22.5. A cutoff value of >2.5 was considered as an index of IR.
Hepatic ultrasound
Liver steatosis was identified by abdominal ultrasound evaluation by the same experienced radiologist, who was blinded to the health conditions of the patients, using an Acuson Sequoia C512 scanner equipped with a 15L8 transducer (Universal Diagnostic Solutions, Oceanside, CA). Liver steatosis was defined according to the criteria (mild = 0, moderate = 1, and severe = 2), a bright hepatic echo pattern compared with echo response of the right kidney.
Chemicals
Physiological saline solution (NaCl 0.9%), trichoroacetic acid (TCA), 2,4-dinitro-phenylhydrazine (DNPH), guanidine, potassium phosphate monobasic (KH2PO4), Bradford reagent, ammonium sulfamate, mercuric chloride (HgCl2), sulfanilamide, N-1-naphthylethylendiamine, S-nitrosoglutathione, phosphate-buffered saline (PBS), potassium iodide, chloramine-T, GSH, GSSG, HXT, gallic acid, α-tocopherol, and tocopheryl acetate were purchased from Sigma–Aldrich (Saint Louis, MI). Chloridric acid (HCl), sulfuric acid (H2SO4), meta-phosphoric acid, phosphoric acid (H3PO4), glacial acetic acid, ethyl acetate, and ethanol were purchased from Merck (Darmstadt, Germany). Trifluoroacetic acid (TFA), acetonitrile, n-heptane, tetrahydrofuran, and glacial acetic acid were high-performance liquid chromatography (HPLC) grade and were purchased from Merck. Other reagents and solvents were of analytical grade.
Analysis of protein carbonyl groups
Briefly, 100 μL of serum diluted 1:10 with physiological saline solution was added with 20% TCA and centrifuged at 13,000 g for 2 min at 4°C. The protein pellet was incubated with 100 μL of 10 mM DNPH (HCl 2 N) for 60 min at room temperature (RT) vortex mixing every 15 min. Then, the proteins were precipitated by adding 20% TCA solution, vortex mixed, and centrifuged as described previously. The protein pellet was washed three times with 200 μL of ethyl acetate/ethanol solution (1:1, v/v); then, it was resuspended in 120 μL of guanidine solution 6 M (KH2PO4 20 mM, pH 2.3 by TFA) at 37°C for 15 min.
Sample solution was brought to RT, centrifuged at 13,000 g for 5 min at 4°C, and the supernatant read at 375 nm by a Multiskan™ GO reader plate (Thermo Fisher Scientific, Waltham, MA) against a blank (physiological saline solution instead of sample) as control. The serum concentration of carbonyl groups was quantified by the following equation:
where A is the absorbance of sample at 375 nm, 6.364 is the mM extinction coefficient (ɛmM = 22 mM −1 cm−1) considering the optical path length (0.2893 cm), and V is the volume of sample within the well.
Results were normalized to the total protein amount determined by the Bradford reagent and expressed in nanomoles (nmol) of carbonyl groups per milligram of protein by the following equation:
where C is the nanomoles per well, P is the total protein amount, and D is the sample dilution factor.
Analysis of SNOPs
Serum sample (60 μL) was pipetted directly into a multiwell plate and 50 μL of ammonium sulfamate solution 0.5% was added. After incubation time (3 min), 40 μL of HgCl2/sulfanilamide solution (0.25% and 2.55% v/v, respectively) and 40 μL of N-1-naphthylethylendiamine 0.38% in HCl 0.4 N were added. The absorbance was read at 540 nm by a Multiskan GO reader plate (Thermo Fisher Scientific) after an incubation time of 5 min.
SNOPs were quantified by using a standard calibration curve of S-nitrosoglutathione solubilized in H2SO4 0.2 N (12.5–100 μM). Results were normalized to the total protein amount determined by the Bradford reagent and expressed in nanomoles of carbonyl groups per milligram of protein.
Analysis of AGEs and AOPPs
Determination of AGE and AOPP was carried out by spectrofluorimetric detection.
AGE determination was carried out on serum diluted 1:5 with PBS (pH 7.4). The fluorescence intensity was recorded (λem 440 nm, λex 350 nm), and results are expressed in arbitrary units per gram of protein (AU/g protein).
For AOPP determination, 10 μL of KI (1.16 M) and 20 μL of glacial acetic acid were added to 200 μL of serum diluted 1:5 with PBS 20 mM. The absorbance was read immediately at 340 nm. Chloramine-T (12.5–100 μM) was used as reference compound while PBS was used, instead of sample, as negative control. AOPP concentration was expressed in nanomoles of Chloramine-T per milligram of protein.
Analysis of GSH and GSSG
The GSH and GSSG simultaneous quantification in plasma samples was carried out by solid-phase extraction (SPE) followed by HPLC-DAD (HPLC with diode array detection). Briefly, 400 μL of meta-phosphoric acid was added to 200 μL of plasma sample and incubated at RT for 15 min. Sample was then centrifuged at 10,000 g for 5 min at 4°C and the supernatant processed by SPE using a BOND Elut C18 cartridge 50 mg/3 mL (Agilent Technologies, Santa Clara, CA) pre-conditioned with methanol (2 mL). The elution was carried out with TFA 0.1% (1 mL). Sample was filtered using a 0.22 μm nylon syringe filter and injected into an Agilent 1100 series HPLC system (Santa Clara, CA). The separation was achieved on Prodigy™ 5 μm ODS-3 100 Å, LC Column 250 × 4.6 mm (Phenomenex, Torrance, CA) by isocratic elution (30 min) using TFA 0.1%/acetonitrile (95:5, v/v) as mobile phase. The flow rate was 1 mL/min, and the detection wavelength was set at 215 nm. The column oven was kept at RT while the auto-sampler temperature was maintained at 4°C. The quali-quantitative analysis of glutathione derivatives was carried out by comparing retention times and UV-visible spectra (UV-VIS) (range 190–400 nm) and using external standard calibration curves (5–40 μg/mL) of the commercial available reference compounds (GSH and GSSG) solubilized in mobile phase.
Analysis of bioactive compounds HXT and α-tocopherol
The SPE and analytical evaluation of HXT in plasma samples was carried out according to Colica et al. (1) with some modifications. Briefly, 10 μL of 8.5% H3PO4 and 10 μL of gallic acid methanol solution 1 mg/mL (internal standard) were added to 100 μL of plasma sample, which was passed through a Strata™-X 33 μm Polymeric Reversed Phase, 30 mg/mL (Phenomenex), previously activated with 1 mL of methanol followed by 1 mL of deionized water. After a washing step with 500 μL of deionized water, the HXT was eluted with 1.5 mL of 5% methanol solution, filtered using a 0.22 μm nylon syringe filter, and injected into the HPLC system.
The chromatographic separation was carried out by Eclipse plus C18 column (150 × 4.6 mm, 5 μm) (Agilent Technologies) using (A) CH3COOH 0.2% (pH 3.1) and (B) methanol, as mobile phase, according to the following gradient elution: 0–2 min 90% B, 2–10 min 60% B, 10–13 min 90% B, 13–15 min 90% B. The injection volume was 20 μL, the flow rate was set at 1.5 mL/min, and the auto-sampler temperature was maintained at 4°C.
HXT was recognized by comparing the retention time and relative UV-VIS (range 200–400 nm) with that of the commercial available standard and quantified at 280 nm by an external calibration curve (3.125–50 μg/mL). Results are expressed in milligrams of HXT per milliliter of plasma sample.
The α-tocopherol determination was carried out by liquid–liquid extraction followed by HPLC with fluorescence detection analysis. Briefly, 10 μL of α-tocopheryl acetate 0.4 mg/mL in ethanol (internal standard) was added to 200 μL of plasma sample, vortex mixing for 10 min. After that, 200 μL of cold ethanol was added, vortex mixing for 1 min, and the sample extracted with 500 μL of cold hexane solution containing butylated hydroxytoluene 1 mg/mL. The sample was then vortex mixed for 5 min and centrifuged at 12,000 g for 5 min at 4°C. The above extraction procedure was repeated two times and the combined hexane layers were brought to dryness by nitrogen. Sample was resuspended with 200 μL of cold ethanol, vortex mixed for 1 min, filtered using a 0.22 μm nylon syringe filter, and injected into HPLC system.
The chromatographic elution was performed on a LiChrosorb® 5 μm Si 60 Å, LC Column 250 × 4 mm (Phenomenex) maintained at 25°C, using a mobile phase consisting of n-heptane/tetrahydrofuran mixture (96.15/3.85, v/v). The injection volume was 10 μL, the flow rate was set at 1.0 mL/min, and the auto-sampler temperature was maintained at 4°C. The acquisition was set at λem 330 nm and λex 295 nm.
The quantification was carried out by external calibration curve of the commercially available standard (0.5–8.0 μg/mL), and results are expressed in micromoles of α-tocopherol per liter of plasma sample.
All sample preparation steps for both bioactive compounds were carried out in the dark, using burnished glass vials, and maintaining a temperature of ≤4°C to avoid any analytes degradation.
Statistical analyses
Statistical analyses were undertaken using STATISTICA software (version 2010, Chicago, IL). The Kolmogorov–Smirnov test was used to determine whether variables were normally distributed. Normally distributed data are expressed in means ± standard deviations, and nonnormally distributed data are expressed in medians and interquartile ranges. Data were analyzed using the intention-to-treat principle, and the values recorded at baseline were compared with values recorded at 4 months in all patients, regardless of treatment duration. Baseline and follow-up characteristics were tested for differences by Student's t-test (p < 0.05). The change of anthropometrical and laboratory values, between placebo and treatment groups, was evaluated using analysis of variance with repeated measures. Difference between proportions was tested using the chi-square test. Pearson's correlation test was used to evaluate a possible correlation between biochemical variables and histological patterns in NAFLD patients.
Footnotes
Acknowledgment
This work was supported by Italian Ministry of Health funds (Ricerca Corrente 2018) to V.N. and A.A.
Author Disclosure Statement
The authors declare no competing financial interests.
Supplementary Material
Supplementary Figure S1
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.