
Abstract
Chronic obstructive pulmonary disease (COPD) and atrial fibrillation (AF) are characterized by increased oxidative stress, but the impact of the coexistence of COPD and AF on systemic oxidative stress is unclear. We performed a cross-sectional study including 157 outpatients to investigate the Nox2-related oxidative stress in patients with AF and COPD. COPD was defined by an FEV1/FVC <0.70. Oxidative stress was measured by sNox2-dp, a marker of Nox2 activation, and urinary isoprostanes. We divided patients into four groups: Group 0: hypertension (n = 49, controls); Group 1: COPD (n = 42); Group 2: AF (n = 33); and Group 3: COPD and AF (n = 33). Mean age was 68.3 ± 11.0 years, and 46.5% were women. Patients with COPD or AF showed increased levels of sNox2-dp as compared with group 0; sNox2-dp further increased in patients with COPD + AF. In these patients, sNox2-dp was higher than in those with COPD (p < 0.001) or AF (p = 0.003). At multivariable logistic regression analysis, chronic kidney disease, COPD, and AF were associated with sNox2-dp above median. Similar results were observed for urinary isoprostanes. We hypothesize that the coexistence of COPD in AF patients may be associated with an increased systemic oxidative stress by the upregulation of Nox2.
Innovation
Patients with atrial fibrillation (AF) and chronic obstructive pulmonary disease (COPD) represent a subgroup of patients at high risk for cardiovascular events. Mechanisms underlying this increased risk are not completely clear and may include atherosclerotic burden and inflammation. Results from our study support the hypothesis that the coexistence of COPD and AF may be associated with an increased systemic oxidative stress, as shown by the upregulation of Nox2 activity and urinary isoprostanes excretion.
Introduction
T
COPD is associated with a cluster of cardiovascular comorbidities, including arterial hypertension (HTN), diabetes, obesity, and ischemic heart disease. The most important risk factors for COPD include environmental (i.e., cigarette smoking, air pollution) and genetic risk factors, causing an increased inflammation and oxidative stress, ultimately leading to airway obstruction and parenchymal destruction. The increase of oxidative stress in COPD patients' airways, in particular related to the activity of nicotinamide adenine dinucleotide phosphate (NADPH) oxidase (Nox2), has a significant role in the amplification of inflammatory response.
Among cardiovascular diseases, COPD is an established risk factor for incident atrial fibrillation (AF), and AF represents the most common arrhythmia in patients with COPD (2). As for COPD, inflammation and oxidative stress play a pathogenetic role in the onset, persistence, and progression of AF. In particular, Nox2 is a significant producer of extracellular reactive oxygen species (ROS) in patients with AF.
Recent evidence suggested that COPD is associated with worse symptom control and quality of life, and it also worsens the prognosis of patients with AF, increasing the rate of cardiovascular events and mortality (3). A recent analysis from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) showed that the rate of events in patients with AF and COPD was not substantially influenced by treatments, including antiarrhythmic drugs and oral anticoagulation (3), suggesting that other elements in addition to cardiovascular risk factors may concur with the increased rate of events in this population (3).
Thus, the mechanisms underlying the association between COPD and outcomes in patients with AF remain substantially unexplored. We hypothesized that oxidative stress may be one factor implicated in this association and that the presence of COPD in AF may result in increased oxidative stress. This aspect has never been explored earlier, and the impact of the coexistence of these two conditions on systemic oxidative stress is unknown.
With this aim, we performed a cross-sectional analysis in patients with spirometry-based diagnosis of COPD, in whom we measured two markers of oxidative stress, namely Nox2 and urinary isoprostanes.
Results
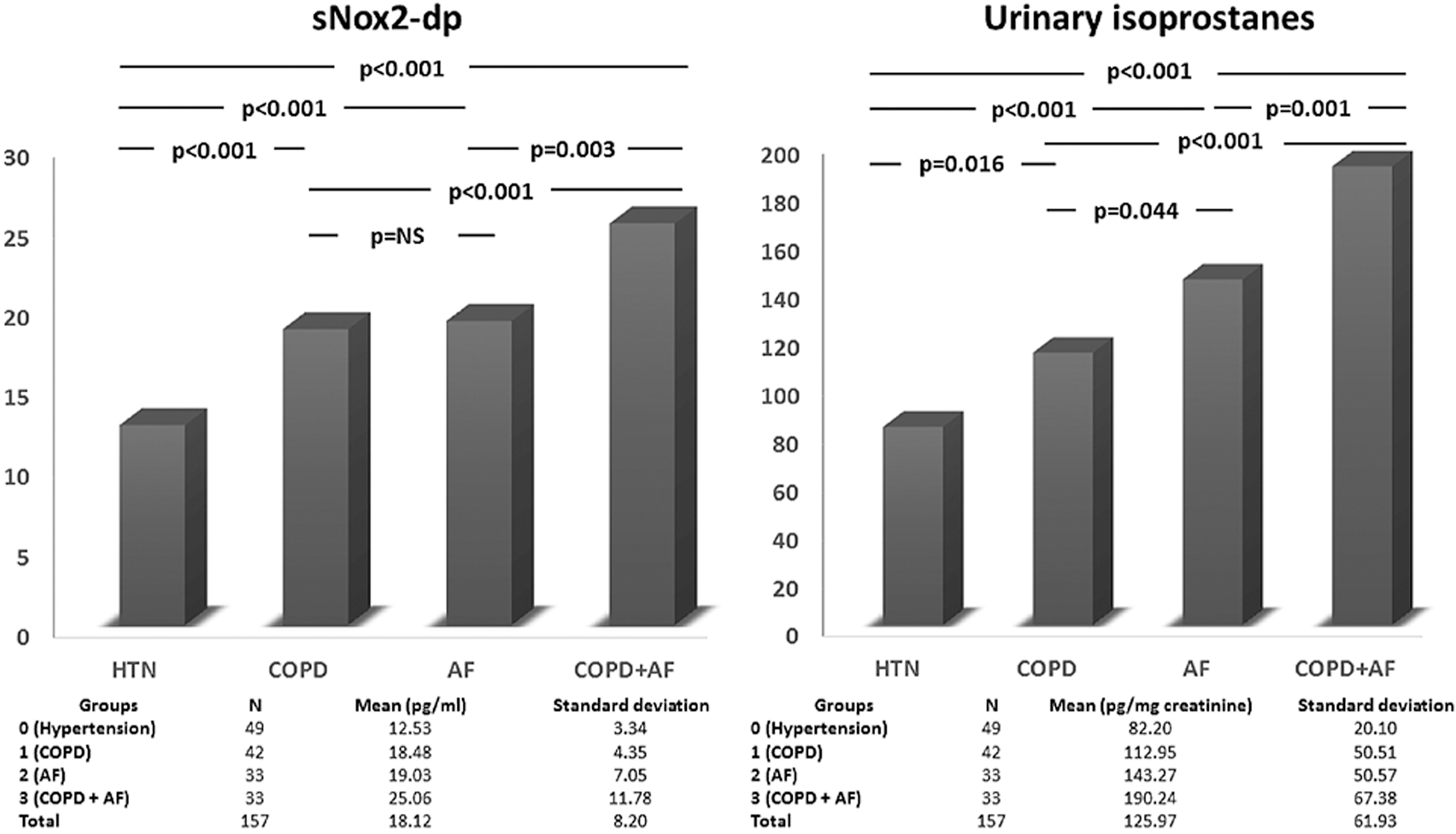
The characteristics of the study population are shown in Table 1. Mean age was 68.3 ± 11.0 years, and 46.5% were women. We found a significant difference among groups regarding sNox2-dp levels and urinary isoprostanes (analysis of variance [ANOVA], p < 0.001 for each marker). In particular, we found a similar increase of sNox2-dp in patients with COPD (difference between mean 5946, standard error [SE] 1457, p < 0.001) or AF (difference between mean 6500, SE 1560, p < 0.001) as compared with those with HTN (group 0, Fig. 1A). Patients with both COPD and AF (group 3) showed a further increase of Nox2 activity compared with group 0 (Fig. 1A, difference between means 12,530, SE 1560, p < 0.001). Levels of sNox2-dp of this group were significantly higher compared with those in patients from group 1 (p < 0.001) and group 2 (p = 0.003).
Characteristics of the Study Population
ANOVA.
χ2 test.
AF, atrial fibrillation; ANOVA, analysis of variance; BMI, body mass index; COPD, chronic obstructive pulmonary disease; eGFR, estimated glomerular filtration rate; HTN, hypertension; LABA, long-acting beta-agonists; OR, odds ratio.
The levels of sNox2-dp were correlated with estimated glomerular filtration rate (eGFR) (r: −0.223, p = 0.005), FEV1% (r: −0.210, p = 0.025), FEV1/FVC (r: −0.168, p = 0.035), and age (r: 0.245, p = 0.002).
Mean value of urinary 8-iso-Prostaglandin F2α (8-iso-PGF2α) was 125.97 ± 61.93 pg/mg creatinine. As compared with patients with HTN, a higher urinary excretion of 8-iso-PGF2α was present in the groups of patients with COPD or AF (p < 0.001 for each, Fig. 1B), with the latter showing a slightly higher value than the COPD group (p = 0.044). Patients with coexistent AF and COPD had significantly higher values of urinary 8-iso-PGF2α compared with patients with single conditions (Fig. 1B).
Multivariable logistic regression analysis (Table 2A) showed that chronic kidney disease (odds ratio [OR] 2.678, 95% confidence interval [CI] 1.028–6.977, p = 0.044), COPD (OR 4.080, 95% CI 1.816–9.166, p = 0.001), and AF (OR 8.026, 95% CI 3.074–20.956, p < 0.001) were independently associated with sNox2-dp above the median.
Logistic Regression Analysis of Factors Associated with sNox2-dp Above the Median (Panel A) and Urinary Isoprostanes Above Median (Panel B)
CI, confidence interval.
Similar results were found by using urinary isoprostanes above median as dependent variables (Table 2B).
Discussion
In this observational study, we found that COPD and AF are associated with an increased Nox2-related oxidative stress. A novel finding is that patients presenting with both COPD and AF disclosed a further increase of sNox2-dp and urinary isoprostanes in comparison to patients who had only one of the two conditions.
To corroborate our findings, we measured a second marker of oxidative stress, such as urinary excretion of isoprostanes, which derived from the nonenzymatic oxidation of arachidonic acid, a phenomenon involving Nox2-derived ROS. We found an increased excretion of urinary isoprostanes in patients with COPD and AF, as compared with single conditions. Our results are in keeping with a previous study showing that patients with COPD had an increased urinary isoprostane F2 alpha-III, which is a stable marker of systemic oxidative stress (7).
These findings reinforce the role of oxidative stress in the pathogenesis of COPD and AF, suggesting Nox2 as a key player linking these two conditions.
Our results have prognostic implications as we have previously shown that an increase of Nox2 activity and urinary isoprostanes excretion are associated with a higher rate of cardiovascular events in patients with AF (6). Future observational prospective studies will investigate the prognostic value of Nox2 also in the setting of COPD, with or without AF.
Altogether, these data suggest that in addition to the well-known risk factors such as hypoxia, hypercapnia, and pulmonary arterial and right ventricular HTN, oxidative stress may contribute to the increased incidence of AF in patients with COPD, and lead us to hypothesize that increased Nox2 activity may be involved in the onset of cardiovascular complications in patients with COPD and AF.
We also found that reduced kidney function was an independent determinant of increased Nox2 activity. This finding is in keeping with previous reports showing that NADPH oxidase isoforms, which are localized at different sites in the kidney, are important contributors in the development of kidney damage.
Our study has also potential therapeutic implications. Patients with COPD and AF represent a subgroup of patients characterized by a particularly increased oxidative stress. These patients may benefit from an antioxidant therapy aimed at reducing both lung inflammation and COPD exacerbations, and AF progression and its complications (9). However, interventional studies with nonspecific antioxidants have provided inconclusive results so far, mostly due to methodology pitfalls and inadequate selection of patients (8). The identification of a specific enzyme, such as Nox2, may allow planning strategies aimed at inhibiting a specific pro-oxidant pathway, potentially representing a valid complementary strategy for the management of patients at high cardiovascular risk, such as those with concomitant COPD and AF.
In this context, statins may represent an interesting therapeutic option, considering that patients taking these drugs have a reduced risk of COPD exacerbation and of myocardial infarction (1). Further, experimental evidence suggested that statins possess pleiotropic properties, including antioxidant activity, by directly inhibiting Nox2 activity. Randomized interventional trials exploring the beneficial effect of statins in patients with COPD and AF are warranted.
Another approach is represented by lifestyle interventions, including diet modifications. A high adherence to Mediterranean diet was associated with an in vivo reduced Nox2 activity in AF patients (5), but data on patients with COPD are lacking.
Limitations include the cross-sectional study design with a relatively low sample size. Despite the presence of COPD being objectively assessed by spirometry in all groups and Nox2 activity being measured by a validated method, we cannot establish a cause
In conclusion, patients with coexistent COPD and AF show increased Nox2-related oxidative stress. This pro-oxidant pathway may represent a target for planning future specific antioxidant interventional strategies.
Materials and Methods
We performed a cross-sectional study including 157 consecutive outpatients who were referred to the outpatient clinic of Predictive Medicine and Atherothrombosis Center in the Department of Internal Medicine and Medical Specialties of I Clinica Medica between January 2015 and September 2016.
Exclusion criteria included the presence of active malignancy, autoimmune disease, chronic inflammatory diseases, and refusal of informed consent signature.
At study entry, all patients underwent a complete clinical laboratory and instrumental work-up. Cardiovascular risk factors were defined as previously described (6). Kidney function was assessed by the eGFR calculated by the simplified MDRD formula. During the visit, anthropometric data and body mass index (BMI, kg/m2) were registered, as well as concomitant drug therapies and smoking habit.
Patients were divided into four groups according to the presence or not of COPD and AF: Group 0: patients with HTN (control group, n = 49); Group 1: patients with COPD (n = 42); Group 2: patients with AF (n = 33); and Group 3: patients with COPD and AF (n = 33).
Markers of oxidative stress
Extracellular levels of soluble peptide Nox2-derived (sNox2-dp), a marker of NADPH oxidase activation, were detected with ELISA test. The peptide was recognized through a specific monoclonal antibody directed against the aminoacidic sequence (224–268) of the extracellular portion of the Nox2 membrane, which is released on the activation of the enzyme. Levels of Nox2 were expressed as pg/mL. Inter-assay and intra-assay coefficients of variation were 5.2% and 6.0%, respectively.
Urinary samples were added with the antioxidant butylated hydroxytoluene at a final concentration of 20 μmol/L and immediately stored at −80°C until use. Urinary 8-iso-Prostaglandin F2α (8-iso-PGF2α) was measured in triplicate for each sample by a validate EIA assay method (6). 8-iso-PGF2α concentration was corrected for recovery and creatinine excretion, and it was expressed as pg/mg of urinary creatinine. Intra-assay and inter-assay coefficients of variation were 2.1% and 4.5%, respectively.
Diagnosis of COPD
At baseline, all patients underwent post-bronchodilator spirometry that was performed by a trained physician. The persistent airflow limitation was defined by an FEV1/FVC <0.70 according to GOLD (Global Initiative for Lung Obstructive Disease) guidelines.
Statistical analysis
Categorical variables were reported as counts and percentages. The independence of categorical variables was tested by χ2 test. Continuous variables were expressed as means ± standard deviation. Group comparison was performed with ANOVA and post hoc analysis with Bonferroni correction. Bivariate analysis was performed with Pearson's linear correlation.
We performed a multivariable logistic regression analysis to investigate factors associated with sNox2-dp levels above the median. Covariates were categorized as follows: female sex (y/n), HTN (y/n), diabetes (y/n), smoking (y/n), chronic kidney disease (eGFR <60 mL/min/m2), statin use (y/n), age ≥75 years, obesity (BMI >30 kg/m2), COPD, and AF. The same model was built with urinary isoprostanes above median as dependent variables. Only p values <0.05 were regarded as statistically significant. All tests were two-tailed, and analyses were performed by using computer software packages (SPSS-22.0; IBM, NY).
Sample size calculation
We computed the minimum sample size with respect to a two-tailed one-sample Student's t-test, considering as (1) relevant a difference in Nox2 of 5 pg/mL (2) standard deviation of the paired differences of 6 pg/mL, (3) type I error probability α = 0.05, and power 1 − β = 0.90. This resulted in n = 31 per group.