
Abstract
Anthracyclines are widely used in anticancer protocols, but can induce cardiotoxicity by mechanisms that mainly involve oxidative damage and mitochondrial dysfunction. Radiotherapy (RT) can also impair cardiac function by promoting myocardial fibrosis, microvascular damage, and decreased density of myocardial capillaries. Hence, we aim at investigating prospectively whether RT impacts heart function in lymphoma patients who had been already treated with anthracyclines. Twenty-nine consecutive patients with Hodgkin or non-Hodgkin lymphomas underwent echocardiography at baseline (before antineoplastic treatments), and then every 2 months, until 6 months after treatment completion. Echo evaluation included standard two-dimensional and speckle tracking. Twenty-two patients treated with anthracycline-based regimens were eligible. Out of the 22 patients, 8 received chemotherapy (CT) only (subgroup 1), while 14 underwent RT after CT [subgroup 2 (S2)]. At the end of CT, ejection fraction was significantly reduced in the whole population. At 6 months after completion of therapies, E/E′ increased and global longitudinal strain was compromised in S2, suggesting additional damage induced by RT after CT. On the basis of the data from our small prospective study, we can hypothesize that in lymphoma patients, anthracyclines can worsen cardiac function, and RT may have an additional unfavorable myocardial impact.
Introduction
A

Our data show that anthracycline impairment of cardiac function is detectable with traditional echocardiography already at the end of chemotherapy, while radiotherapy induces an additional damage that affects mostly the midventricular and apical sections of the heart, detectable by the more sophisticated global longitudinal strain (GLS). At present GLS is not routinely used for cardiac follow-up of cancer patients, but we believe that it can be an important tool for early detection of cardiac impairment due to anticancer treatments, as highlighted by clinical guidelines (1, 2, 9).
Radiotherapy (RT) is used in many anticancer protocols, but unfortunately can also damage the heart [radiation-related heart disease (RRHD)] and induce cardiomyopathy, coronary artery disease, and valvular disease. RRHD can be acute, lasting only a few days after irradiation, or chronic, leading to myocardial fibrosis. Chronic cardiac damage after RT can manifest many years after irradiation, and hence, it is difficult to estimate the real incidence of RRHD (9) (Fig. 2).

At present, LV ejection fraction (EF) measured by two-dimensional (2D)-echocardiography is widely used to detect cardiac dysfunction during and after anticancer treatments (9). However, left ventricular ejection fraction (LVEF) measurements could underestimate cardiac injury, since a reduction in LVEF is detectable by echocardiography when heart dysfunction is already consistent; therefore, this parameter is not really suitable to identify early, subclinical damage. Moreover, intra- and interoperator reproducibility of LVEF measurements is low. New echocardiographic approaches, such as assessment of myocardial deformation with global longitudinal strain (GLS) in speckle tracking echocardiography (STE), allow for detection of early cardiac motion abnormalities (5, 7).
GLS and STE have been investigated mainly in breast cancer, and are nowadays recommended by the American Society of Echocardiography and the European Association of Cardiovascular Imaging (5). It has been recently shown that GLS predicts cardiotoxicity in lymphoma patients in a retrospective study (3). Here, in a small prospective study, we used traditional and STE to detect early anthracycline cardiotoxicity in adult patients with Hodgkin's lymphoma (HL) and non-Hodgkin's lymphoma (NHL), aimed at verifying whether patients who underwent mediastinal irradiation for RT after anthracycline-based chemotherapy (CT) develop further impairment in GLS, and we checked whether the alterations in GLS induced by radiations predominantly affect the midventricular and apical regions of the LV, more exposed to radiations.
Results, Discussion, Limitations, and Future Perspectives
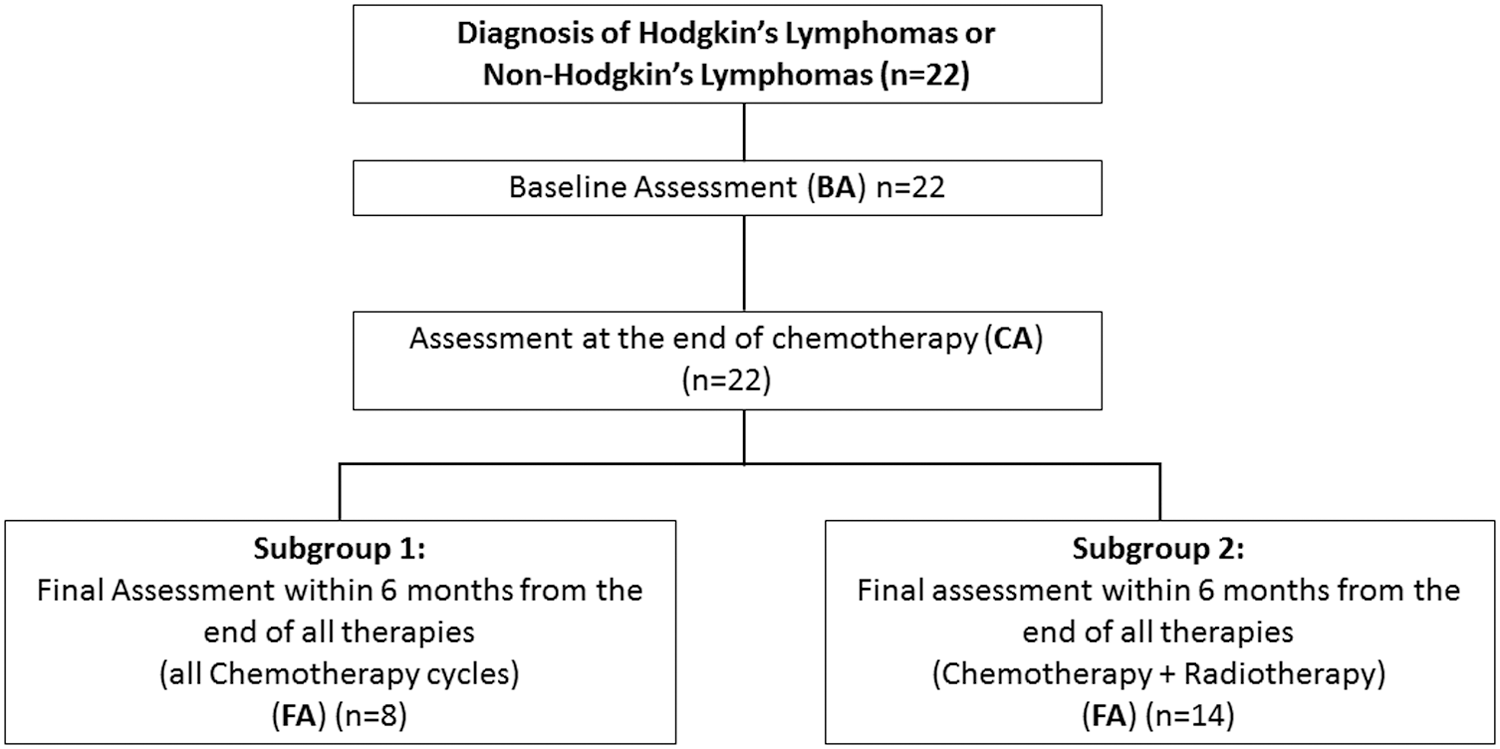
Twenty-nine adult patients (19 females; 66%) newly diagnosed with lymphoma to be treated with anthracycline-based CT (with or without RT) were evaluated from November 2015 to March 2018. One patient did not complete all the CT cycles, one had a diagnosis of relapse and underwent a second-line treatment with rituximab and bendamustine, and five were lacking a baseline cardiac evaluation. Hence, 22 patients met the inclusion criteria and were eligible for the study (see Fig. 3 for study design). Our final cohort consisted of 14 (63.6%) females, with a median age of 41 (20; 88) years; 86.4% had HL. All patients underwent anthracycline-based regimens (Table 1), median cumulative dose was 378.00 (100.00; 600.00) mg/m2. Fourteen out of 22 patients (subgroup S2) were also treated with involved-field RT (IFRT), mostly directed to the anterior mediastinum with a median prescribed dose of 30.00 (30.00; 36.00) Gy, fractionated in 20 sessions, while subgroup 1 (S1) identified patients treated with CT only.
General Characteristics of the Study Cohort at Baseline Assessment
Data are expressed as median (minimum; maximum values) or number (%).
ACEi, angiotensin converting enzyme inhibitors; ARBs, angiotensin receptor blockers; ESC, European Society of Cardiology; GLS, global longitudinal strain; HL, Hodgkin lymphoma; NHL, non-Hodgkin lymphoma; N.S., not significant; N/A, not applicable; S1, subgroup 1; S2, subgroup 2.
Baseline echocardiographic data [baseline assessment (BA)] were compared with echocardiographic data acquired at the end of CT [chemotherapy assessment (CA)], and within 6 months from the end of hematologic treatments [final assessment (FA)]. CA was performed after 4.5 months (2; 8) from BA [5 months (2; 8) for S1, 4 months (2; 7) for subgroup 2 (S2)]. FA was performed after 9.5 (6.0; 13.0) months from BA; in particular, the median follow-up for the S1 was 9 (8; 12) months, while for the S2 was 10 (6; 13) months.
First, we assessed cardiac function by analyzing echocardiographic differences from BA to CA in the whole population. Importantly, at the end of CT, we observed a significant reduction in LVEF, from 60% (54; 65) at BA to 55% (53; 65) at CA. No other conventional echocardiographic parameter changed, as shown in Table 2. These results were confirmed when we excluded 4 patients older than 65 years: EF declined from 60% (55; 63) to 57% (53; 65), p = 0.033.
Echocardiographic and Global Longitudinal Strain Parameters of the Whole Population
Bold values indicate p < 0.05.
Data are expressed as median (minimum; maximum).
BA, baseline assessment; CA, chemotherapy assessment; FA, final assessment; LAVi, left atrial volume indexed; LV-EDVi, left ventricular end diastolic volume indexed; LV, left ventricle; LVEF, left ventricular ejection fraction; TAPSE, tricuspid annular plane systolic excursion.
We then divided our population according to whether patients underwent RT or not. The subgroup analysis revealed that in S1 no conventional parameter changed from CA to FA (final assessment), while in group S2, we found a significant increase in E/E’ from CA [6.2 (4.2; 14.2)] to FA [6.9 (5.5; 15.2), p < 0.05] (Table 3), suggesting an increase in LV diastolic pressures due to RT after CT. The same was true when we excluded the three elderly patients: E/E′ increased from CA [6.0 (4.2; 13.0)] to FA [6.8 (5.5; 13.6), p = 0.01].
Subgroup 1 and Subgroup 2: Standard Echocardiographic Parameters
Bold values indicate p < 0.05.
Data are expressed as median (minimum; maximum).
We then aimed at further assessing heart function by using the more sophisticated STE. We found that in the whole population, GLS significantly worsened from BA to CA [from −17.17 (−23.33; −11.33) to −16.17 (−19.61; −11.94), p < 0.01], and the same was true when we excluded the four elderly patients [from −17.58 (−20.44; -13.50) to −16.19 (−19.61; −11.94), p < 0.01]. Such impairment persisted at FA, with no significant differences between CA and FA (Table 2). At subgroup analysis, GLS in S1 had the same behavior (Table 4).
Global Longitudinal Strain and Mean Segment Values of Subgroup 2
Bold values indicate p < 0.05.
Data are expressed as median (minimum; maximum).
Interestingly when we analyzed group S2, GLS worsened, although not significantly, from BA to CA, while the change from BA to FA was significant (Table 4), also when we excluded the three elderly patients. In particular, the entity of worsening in GLS from CA to FA was significantly more relevant in S2 than in S1, suggesting that RT after CT significantly adds on an impairment in cardiac function (Table 5). In S2, the impairment in GLS at FA was more evident in the midventricular and apical regions of the LV (Table 4).
Differences in % Change in Global Longitudinal Strain Between S1 and S2
Bold value indicates p < 0.05.
Data are expressed as median (minimum; maximum).
Recent studies have shown that baseline GLS predicts long-term LV dysfunction after anthracycline CT and HF hospitalization in lymphoma patients (3). In our work, we observed a slight but significant reduction of EF right after CT in our population (Table 2), even though no patient had a decrease in EF sufficient to meet the diagnostic criteria for cardiotoxicity (1, 5, 9). In addition, we checked for differences between patients treated with CT only (S1) and patients treated with RT after CT (S2). In S1 patients, GLS analysis detected a decrease in myocardial deformation after CT compared with baseline (CA vs. BA). No further changes in GLS were found at FA versus CA, suggesting that the subclinical damage induced by anthracyclines has an early onset right after CT and does not revert, at least during the time of observation (Table 2). A longer follow-up will reveal whether such alterations in GLS will recover or whether they are predictive of overt cardiac deterioration, with adverse remodeling and further decrease in EF.
In S2 patients, when comparing CA and FA, by means of standard 2D echocardiography, we found an increase in E/E′ (Table 3), showing that the addition of RT upon previous CT administration can worsen diastolic heart function. Further studies are warranted to assess this observation on a longer time period. Moreover, STE analysis in S2 patients revealed that GLS worsened at FA compared with BA (Table 4). These alterations were mainly due to the addition of RT on CT, since there was no significant change of GLS at CA versus BA, while the percentage of drop in GLS between CA and FA was significantly more pronounced in S2 than in S1 (p = 0.04, Table 5). These alterations were mainly localized at the apical and midventricular regions of the LV. We hypothesize that this happens because these are the heart portions more exposed to mediastinal irradiations for lymphoma (Table 4). On the contrary, the reduction in LS observed in S1 is more uniform and does not show patterns of regionality. Seven out of the 22 patients (31.82% of the whole sample) had a reduction of GLS ≥15% from BA to FA (Table 1) (1, 5, 9). Among these seven patients, six belonged to S2, and this seems to confirm our hypothesis that RT after CT can further worsen cardiac damage already induced by CT alone.
There are some limitations to our study. First, this is a single-center study with a small sample size. We plan to keep on enrolling additional patients prospectively, in a multicenter study, to expand our sample and have a better understanding of the echocardiographic changes, and whether such changes are predictive of future clinical events. Second, some patients were already being treated with β-blockers and angiotensin converting enzyme (ACE)-inhibitors, which may have protected from further cardiac deterioration after CT and/or RT, thus masking the real impact of these anticancer treatments. Indeed, β-blockers can reduce oxidative stress and calcium overload in myocardial cells (8). In particular, carvedilol demonstrated a preventive role against LV dysfunction in patients treated with anthracyclines, reducing reactive oxygen species (ROS) production, apoptosis of cardiomyocytes, and mitochondrial alterations (8). The renin/angiotensin/aldosterone system also plays a key role (8). In patients treated with anthracyclines, enalapril reduced the incidence of LV dysfunction, while candesartan ameliorated in vitro anthracycline cardiotoxicity and telmisartan reduced acute LV dysfunction induced by doxorubicin in rats. Coadministration of ACE-Is and carvedilol can reduce cardiac damage induced by anthracyclines (8).
Correlating serum biomarkers to our imaging markers would sure help in the assessment of cardiotoxicity (1, 8, 9), but unfortunately, for most patients we were not able to collect NT-proBNP or troponin values. Importantly, in the setting of oxidative damage, such as the one from anthracyclines and RT, markers of oxidative stress could play a key role in early detection of cardiac damage (8). Unfortunately, ROS are very unstable and their detection in patients treated with anticancer therapies is almost impossible to use in clinical practice (8). Metabolomics may play an important role, with the quantification of succinate that could be used as an alternative biomarker of oxidative or nitrosative cardiotoxicity (8). Furthermore, the decrease in NAD(P)H:quinone oxidoreductase 1 activity and the increase of ROS produced by the activity of NAD(P)H oxidase have also been proposed as early markers of cardiac damage in patients treated with anthracyclines (8).
Another limitation concerns the echocardiographic technique, since STE depends on 2D image quality; nevertheless, none of the patients was excluded from the analysis because of poor quality of echocardiographic images. Furthermore, there is vendor-specific variability in strain measures that may affect reproducibility of GLS findings.
All things considered, with the abovementioned limitations, the data we have obtained from our small prospective study seem to suggest that in adult lymphoma patients, EF declines right after CT. Also, RT seems to have an impact on cardiac function that is additional to CT alone, and this further damage can be detected by STE. Further high-volume studies and longitudinal observations are needed to reveal whether these subclinical changes induced by anthracyclines combined with RT are reversible or will translate into overt cardiotoxicity.
Notes
Study design
In this single-center prospective cohort study, we recruited patients newly diagnosed with HL or NHL from the Division of Hematology of Federico II University, Naples, Italy. The protocol was approved by the local ethics committee, all patients signed a written informed consent, and the study was conducted following the Helsinki Declaration principles.
Inclusion criteria were as follows: new diagnosis of HL and NHL requiring anthracyclines with or without RT; and age >18 years. Patients with previously treated HL or NHL; patients without baseline cardiovascular assessment; patients who did not receive the scheduled regimens or RT for noncardiac-related toxicity; pregnant patients; patients affected by major arrhythmias; and patients whose echocardiographic quality images were not optimal for GLS analysis or did not have adequate thoracic window were excluded.
All patients underwent a full cardiologic examination, 2D-echocardiography, and STE at baseline, at the end of CT, and within 6 months from the end of all antineoplastic treatments.
Cardiologic evaluation
Every echocardiographic examination was preceded by ECG recording, blood pressure measurement, a full clinical evaluation and a full history that included life style (diet, activity, and smoking habits), family history of cardiac disease, coexistent illnesses, and ongoing therapies, and previous diseases and therapies.
Eight patients (32.4% of the sample) had hypertension that was well managed by common antihypertensive therapies; two patients (9.1%) had type 2 diabetes; four patients (18.2%) had dyslipidemia; and six patients were active smokers (27.3%); while seven were former smokers (31.8%). No patient had ischemic heart disease. Baseline patients' characteristics are shown in Table 1.
Conventional echocardiography
Standard transthoracic 2D-echocardiographic examinations were performed using a Philips iE33 ultrasound machine (Philips Healthcare, Andover, MA). Images were obtained using a 3.4 MHz transducer with patients in left lateral decubitus position. Following the American Society of Echocardiography guidelines (4), standard subxiphoid, apical, and parasternal windows were visualized to acquire 2D images of the cardiac chambers, color, and pulsed- and continuous-wave Doppler measurements.
Speckle tracking echocardiography
Additional 2D-echocardiographic cine loops, using frame rates between 50 and 70 fps, from four-, two-, and three-chamber views were acquired for subsequent offline speckle tracking-derived analysis using a commercially available vendor-independent strain software (Epsilon, Echolnsight, Milwaukee, WI). The analysis was based on an 18-segment model and GLS was obtained from the mean of the values of the 18 segments. Regional strain values from the six basal, six midventricular, and six apical segments of the LV were averaged to obtain three regional longitudinal strain (LS) values (basal, midventricular, and apical, respectively). LS analysis allows for evaluation of shortening of a specific portion of the heart obtained by tracking the endocardial border of the LV, compared with its original length, and is expressed as a negative percentage (6). This evaluation is important to estimate myocardial deformation, defined as peak longitudinal systolic strain and expressed as percentage of the longitudinal shortening of systole compared with diastole. A worsening in strain is defined by a less negative number or a smaller deformation in the longitudinal axis, while an improvement is defined by a higher negative number (in its absolute value) or a greater deformation in the same axis, referred to a given segment (Fig. 4).

A clinical cardiologist expert in echocardiography (V.M.) blinded to patient status analyzed each study for standard echocardiography and strain measurements. To assess for intraobserver variability, eight studies with adequate image quality were randomized for reanalysis 1 week after initial analysis by the same physician, and, to assess interobserver variability, by a second independent clinical cardiologist expert in echocardiography (D.C.), again blinded to patient status.
Intra- and interobserver variability
Intra- and interobserver variability for GLS was excellent [intraclass coefficient correlation (ICC) of 0.95 and 0.92, respectively].
CT and radiation therapy
All patients affected by HL were treated with the combination of adriamycin, bleomycin, vinblastine, and dacarbazine (ABVD) regimen in standard doses (ABVD: adriamycin 25 mg/m2 was administered intravenously on day 1 and 15, bleomycin 10 mg/m2 was administered intravenously on day 1 and 15, vinblastine 6 mg/m2 was administered intravenously on day 1 and 15, and dacarbazine 375 mg/m2 was administered intravenously on day 1 and 15, every 4 weeks) for up to 2–6 cycles (treatment was modulated according to the stage). Patients with NHL received rituximab, cyclophosphamide, doxorubicin, vincristine, prednisolone (cyclophosphamide 750 mg/m2, doxorubicin 50 mg/m2, vincristine 1.4 mg/m2 with a maximum dose of 2 mg, and rituximab 375 mg/m2, all administered intravenously on day 1, and oral prednisolone 40 mg/m2 on days 1–5, every 21 days) for a total of six cycles.
At the end of CT treatment, 14 patients underwent IFRT (radiation dose ≤30 Gy).
Statistical analysis
Data are presented as median (minimum; maximum) for continuous variables, and as absolute numbers or percentage for discrete variables. Patients were analyzed as a whole cohort and then divided into two subgroups: S1 identified patients treated with CT only; S2 included patients who were treated also with RT. Baseline echocardiographic data (BA) were compared with echocardiographic data acquired at the end of CT (CA), and within 6 months from the end of hematologic treatments (FA) using the Friedman test for continuous variables. Bonferroni correction was applied, when appropriate. The chi-squared test was used to compare discrete variables, and the Mann–Whitney U test was used for comparison between the two subgroups.
The ICC was used to calculate the intra- and interobserver variability.
A p value <0.05 was considered statistically significant. Statistical analysis was performed using SPSS Statistics version 24 (IBM, Armonk, NY).
Footnotes
Author Disclosure Statement
C.G.T. received speaking fees from Alere. The remaining authors have nothing to disclose.
Funding Information
C.G.T. is funded by a “Federico II University Ricerca di Ateneo” grant, G.M. was supported, in part, by grants from Regione Campania CISI-Lab, CREME Project, TIMING Project, and Federico II University.