
Abstract
Significance:
In vivo molecular and metabolic imaging is an emerging field in biomedical research that aims to perform noninvasive detection of tissue metabolism in disease states and responses to therapeutic agents. The imbalance in tissue oxidation/reduction (Redox) states is related to the onset and progression of several diseases. Tissue redox metabolism provides biomarkers for early diagnosis and drug treatments. Thus, noninvasive imaging of redox metabolism could be a useful, novel diagnostic tool for diagnosis of redox-related disease and drug discovery.
Recent Advances:
In vivo dynamic nuclear polarization magnetic resonance imaging (DNP-MRI) is a technique that enables the imaging of free radicals in living animals. DNP enhances the MRI signal by irradiating the target tissue or solution with the free radical molecule's electron paramagnetic resonance frequency before executing pulse sequence of the MRI. In vivo DNP-MRI with redox-sensitive nitroxyl radicals as the DNP redox contrast agent enables the imaging of the redox metabolism on various diseases. Moreover, nitroxyl radicals show antioxidant effects that suppress oxidative stress.
Critical Issues:
To date, considerable progress has been documented preclinically in the development of animal imaging systems. Here, we review redox imaging of in vivo DNP-MRI with a focus on the recent progress of this system and its uses in patients with redox-related diseases.
Future Directions:
This technique could have broad applications in the study of other redox-related diseases, such as cancer, inflammation, and neurological disorders, and facilitate the evaluation of treatment response as a theranostic tool. Antioxid. Redox Signal. 36, 172–184.
Introduction
I
The dissolution DNP method has been extensively used for metabolic imaging of common biological 13C molecules, such as pyruvate and lactate. In dissolution DNP methods, DNP is induced in a magnetic field with liquid helium, and the hyperpolarized 13C molecules are administered to animals to observe the in vivo metabolism using 13C MRI (4, 49, 56 –59, 62). In contrast, the in vivo DNP method can be performed at room temperature; thus, it is possible to induce the in vivo DNP phenomenon using free radicals (Fig. 1A, B). In this case, these radicals could serve as imaging probes in living organisms. In vivo DNP-MRI, also known as Overhauser MRI or proton electron double resonance imaging is a method for imaging redox metabolism in living organisms with their anatomical structures (2, 40, 47, 82).

Because the imbalance in the tissue oxidation/reduction (redox) state is associated with the onset and progression of various diseases (12, 55, 71, 76, 78), the tissue redox metabolism could be an important parameter to provide biomarkers for early diagnosis and evaluation of drug response. Therefore, noninvasive imaging of the redox metabolism could serve as a useful and novel diagnostic imaging tool for drug discoveries and clinical applications.
Nitroxyl radicals (nitroxide) are stable free radicals with unique redox reactivities, antioxidative properties, and contrast effect in magnetic resonance technologies, such as electron paramagnetic resonance imaging, MRI, and DNP-MRI (Fig. 1C). Therefore, they have been used as spin probes in various biophysical and biochemical experiments (74, 75). Several previous studies have demonstrated that nitroxyl radicals interact with various metabolic processes (14, 16, 27, 36, 51). The free radicals in nitroxide molecules are stabilized by methyl groups at the α position of the five-membered pyrrolidine (carbamoyl-PROXYL) and the six-membered piperidine (Tempol) ring structures (Fig. 1C). The redox transformations among the oxidized form of nitroxyl radical, the reduced form, and the oxoammonium cation are shown in Figure 1D. The oxidized nitroxyl radicals exist as redox pairs and comprise the free radical form and nonparamagnetic hydroxylamine.
The in vivo redox reaction is modulated by these nitroxyl radicals as redox probes for DNP-MRI. The reduction rate of the nitroxyl radicals depends on the tissue redox environment and is affected by other factors, such as the overgeneration of reactive oxygen species (ROS); redox reactions, such as electron transfer in the mitochondria; and decreased antioxidant defenses. Recently, it was found that one nitroxyl radical, carbamoyl-PROXYL, is useful for monitoring the mitochondrial redox metabolism in mouse livers (54). Therefore, in vivo DNP-MRI with the nitroxyl radical method has been previously used for obtaining valuable data regarding the tissue redox status in various redox-related diseases (17, 21, 22, 28, 35, 54, 70, 87 –89). Here, we present a review of the redox imaging using in vivo DNP-MRI with a focus on the recent progress in this imaging system and its application in patients with redox-related diseases. Furthermore, the therapeutic effects of nitroxyl radicals that were used as contrast agents for DNP-MRI have been described to have potential application in theranostics. This technique could have broad applications in the study of other redox-related diseases, such as cancer, inflammation, and neurological disorders.
Application of In Vivo DNP-MRI for Animal Disease Models
Local muscle inflammation
Muscle tissue is a major source and user of energy in the body. The abundance of mitochondria in this muscle results in the generation of adenosine triphosphate through the electron transfer mechanism, which represents a substantial source of free radicals (52). Therefore, oxidative stress can be linked to the formation and development of skeletal muscle diseases. The infiltration of macrophages, neutrophils, and lymphocytes into the muscle is a characteristic feature of some incurable types of myositis, such as polymyositis and muscular dystrophy. (37, 79, 83). Acute neutrophil-mediated inflammation is a normal immunological response in which white blood cells infiltrate affected tissues and create ROS such as superoxide and hydrogen peroxide within minutes to hours of damage (66). Although widely used, the local anesthetic bupivacaine (BPVC) damages fibers of skeletal muscles and causes significant inflammatory response at the injection site (6, 68). Within hours of BPVC injection, damage of muscle fibers occurs, inflammatory cells infiltrate the treated tissues, and within weeks, muscle cell regeneration is proven (6). Therefore, the BPVC treatment has been used as an animal model of muscle inflammation and regeneration (42).
The ability to image inflammation in vivo gives us great advantages for understanding the pathophysiology and early evaluation of diseases. Imaging of tissue inflammation using computed tomography (CT) and MRI provides information based on tissue structural changes (24). In addition, several novel imaging methods and tools have been developed for that purpose (13, 45, 64, 84, 85, 90). For example, Chandrasekharan et al. reported that magnetic particle imaging using antibody-conjugated safe superparamagnetic iron oxide nanoparticles as tracers specific to neutrophils could be efficiently utilized in vivo as a noninvasive and radiation-free tracking method of inflammatory cells (13).
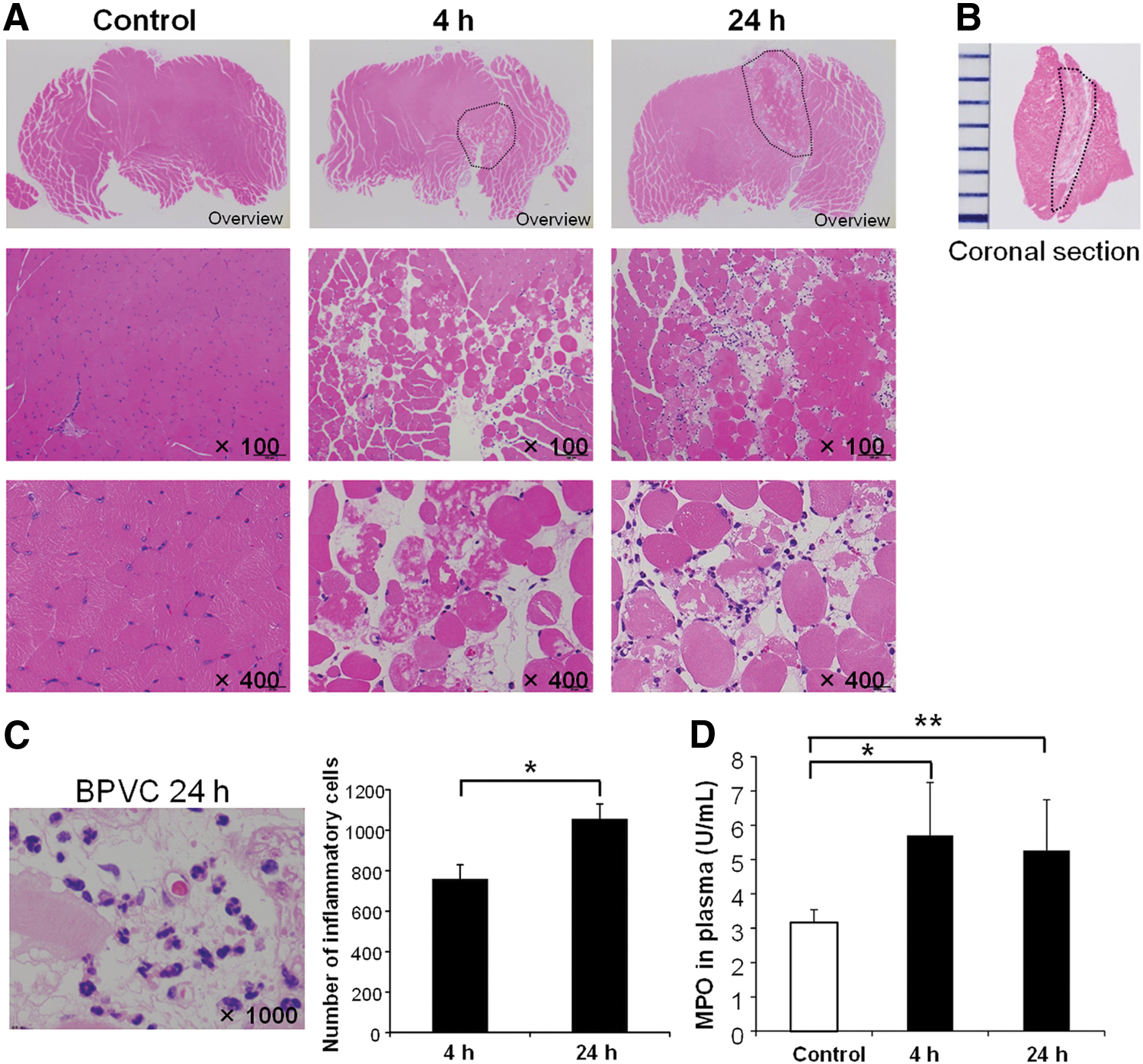
Another method for imaging of local inflammation in the skeletal muscle using the in vivo DNP-MRI was also developed and applied to an animal model (20). Female C57/BL6 mice were administered 0.5% BPVC into the gastrocnemius muscles of their right hind limb to create focal myositis, and their left hind limbs were left untreated as a normal control (20). On histopathological assessment, all the control muscle samples showed normal histological appearance of the muscular tissue with a normal fiber structure and peripheral nuclei (Fig. 2A). At 4 h after BPVC therapy, however, there was a localized muscular lesion at the core of the gastrocnemius muscle, with hyaline degenerative changes of muscle fibers, muscle necrosis, and inflammatory cell infiltration. The muscle damage ranged roughly 8–10 mm from a distal to proximal direction (Fig. 2B). After 24 h of BPVC administration, significant leukocytic infiltration was detected with notable changes at 4 h. Numbers of inflammatory cells at the damaged area at 24 h were significantly higher than those at 4 h postadministration (Fig. 2C). The degree of neutrophil infiltration in myositis was measured using plasma myeloperoxidase (MPO) enzyme activity, which was significantly higher at 4 and 24 h after BPVC administration compared with controls (Fig. 2D).
In vivo DNP-MRI was conducted at 4 and 24 h after administration of BPVC using the cell-permeable (carbamoyl-PROXYL) and the cell-impermeable (carboxy-PROXYL) as probes. DNP probe was injected into the BPVC-treated and untreated contralateral gastrocnemius muscle, and DNP-MRI images were captured over time. Analysis of the image strength was performed to compare the decay rate of the DNP probe between the injured and normal gastrocnemius. For BPVC injection, the decay rates were faster at 4 and 24 h than on their contralateral muscles. Moreover, the average decay rate observed in the BPVC-treated legs of eight mice was significantly higher at 24 h but not at 4 h using either of the probes, carboxy-PROXYL or carbamoyl-PROXYL (Fig. 3A, B). The changes in probe decay rates between the control and BPVC-treated muscles were clearly identifiable in the redox metabolic maps. The differences in the decay rates of BPVC-treated and its contralateral (nontreated) legs in each individual mouse were then calculated (Fig. 3A, B, right panels). In these panels, a symbol above the line marked “even” indicated that the decay rate of redox metabolism in the BPVC-treated leg was faster than that in the control leg. It is noteworthy that even at 4 h, there was a tendency toward a higher rate of decay with BPVC administration, which was compatible with the averaged results at 24 h. Although the administered probe tended to be distributed in the region of interest of the muscular tissue, the degree of correlation between the distribution of the probe and the area of inflammation may lead to variations in the rates of in vivo decay. These data indicate that the in vivo DNP-MRI system can detect variations that occur in the redox state during various stages of the inflammatory processes in myositis. Moreover, it shows that these variations occur in the interstitial space of the muscular tissue rather than inside the myocytes.

Atopic dermatitis
Several novel imaging methods are being developed for that purpose of noninvasive in vivo diagnostics and therapy control in dermatology, which will help to better understand the pathomechanisms of skin diseases and to characterize the effects of therapies. As a noninvasive diagnostic method for skin diseases, dermoscopy is mainly used in assessing various general dermatological disorders based on microscopic observation (18, 19). Other noninvasive technologies such as high frequency ultrasonography, hyperspectral imaging, and confocal microscopy have also been developed for evaluation of skin diseases (15, 25, 67). For example, Kroger et al. has reported an in vivo noninvasive imaging technique to visualize dermal mast cells in skin diseases using two-photon excited fluorescence lifetime imaging signatures (41).
Atopic dermatitis (AD) is a long-lasting and common form of skin inflammation (dermatitis) that comes from a combination of hereditary, environmental, and immunological factors (8). Interstitial and perivascular inflammatory cells such as mast cells and plasma cells, eosinophils, B lymphocytes, and T lymphocytes are infiltered into the dermis of patients with AD (30). Recent research showed that oxidative stress can play a role in a wide range of skin disorders, such as AD and aging (30, 65, 72). During normal metabolic activities, oxidants such as free radicals, oxygen radicals, and nitric oxide species are formed. Biological antioxidant protection mechanisms, including enzyme-based (glutathione peroxidase, peroxiredoxins, and superoxide dismutase) and nonenzyme-based (vitamins A, C, and E, glutathione, polyphenols, and coenzyme Q10) systems, are also developed in living beings to counteract these oxidative substances (23, 30). Increased lipid peroxidation and reduced antioxidant levels are thought to trigger severe oxidative stress in the patients (72, 81), implying that reducing oxidative stress is a successful approach in the treatment of the disease (34, 69, 81). Furthermore, oxidative stress has been proven to enhance inflammation by upregulating genes that encode the inflammatory cytokines in normal keratinocytes (80), and inflammatory cells (30). Overall, these findings suggest that redox instability triggered by multiple inflammatory responses and excessive oxidative stress is a key factor in the pathophysiology of the disease. Therefore, imaging the redox state of the skin may be a useful tool for monitoring disease progression and therapeutic effect in skin disorders, potentially leading to the development of a new plan for management of AD based on the skin's altered redox status.
A model of AD was created by applying Biostir AD ointment repeatedly after giving sodium dodecyl sulfate solution to NC/Nga Tnd mice (86). Since there has been some debate about how well this model represents the manifestations of human AD clinical signs at various phases of the disease (38), two groups of mice were made, one for acute AD (2 weeks of treatment) and the other for chronic AD (4 weeks of treatment). The clinical scores of the mice rose as the times of Biostir AD administrations increased, and the clinical scores for acute and chronic AD animals ranged from 7.1 ± 2.3 to 14.2 ± 1.8 (standard deviation, n = 13), respectively (Fig. 4A). The scalps of acute AD mice formed erythema followed by scale formation, while the scalps and ears of chronic AD mice formed erythema, scales, and erosion, followed by formation of crusts.
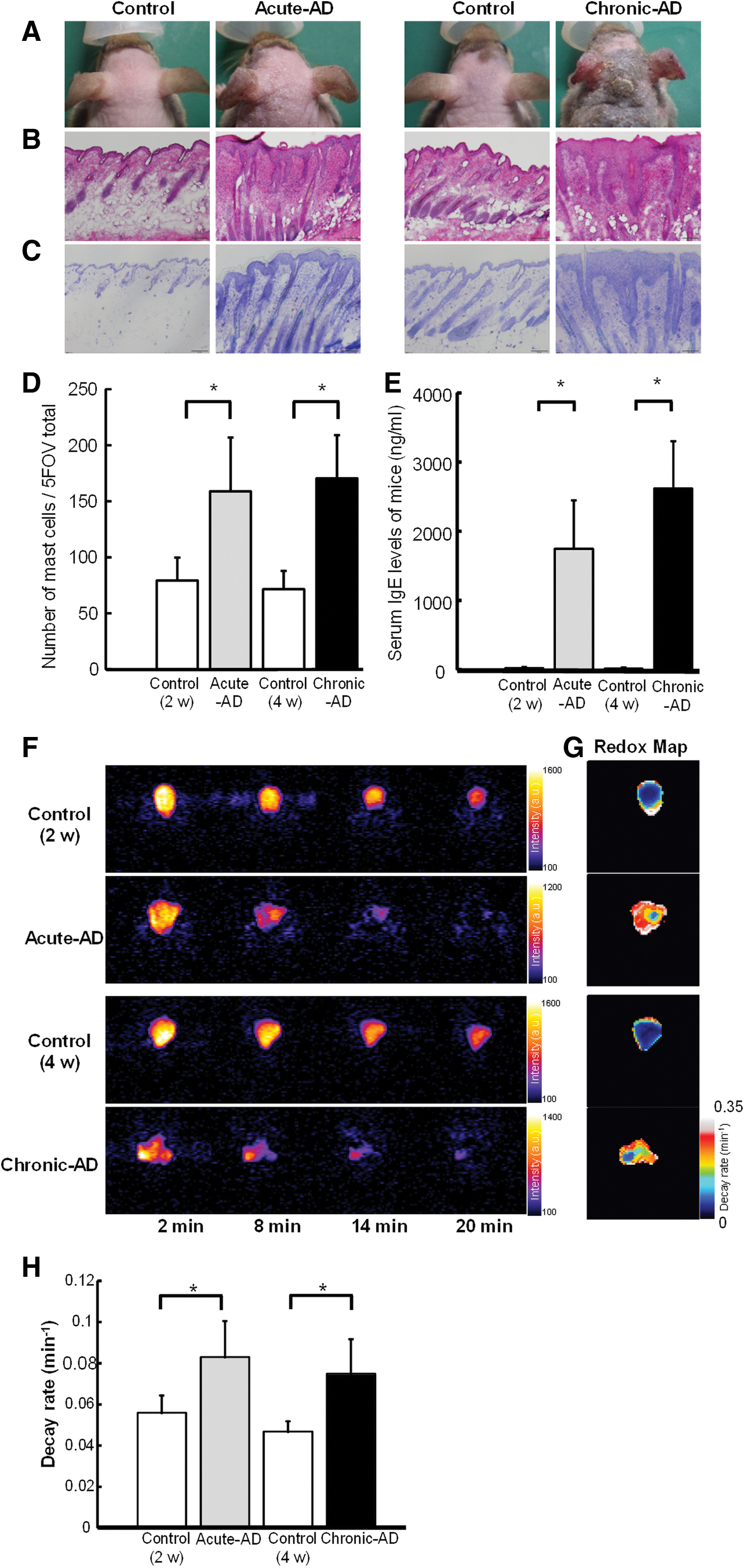
To verify uniformity in the symptoms of AD in each model, skin samples of the mice were histopathologically examined with toluidine blue (TB) or hematoxylin and eosin staining following the in vivo DNP-MRI (Fig. 4B, C). The epidermis of the acute AD animals showed perivascular inflammatory cell infiltration, acanthosis, and spongiosis. Moreover, the dermis of the chronic AD animals also showed similar legions but at more extensive levels. Upon TB staining, both animal groups showed a significantly higher number of mast cells than controls (Fig. 4D). Furthermore, in acute AD mice, serum levels of the blood inflammatory marker immunoglobulin E (IgE) were raised to about 90 times (1700 ng/mL) than those in the controls (Fig. 4E). Chronic AD animals had even higher levels (2600 ng/mL), which was about 160 times higher than those of the controls. Previous findings of AD-like signs in this animal model match these clinical characteristics (33, 77, 86).
Using in vivo DNP-MRI, the redox condition in the dermal tissue from AD mice with acute and chronic disease was assessed. It verified that the nitroxyl radical Tempol was distributed in a similar localization pattern in both mice groups as well as in control animals. When the in vivo DNP probe, Tempol, was used, it caused an increase in image intensity that eventually faded over time (Fig. 4F). The image intensity of AD mice had slightly faster decay rates than control mice, despite no significant variations between mice of acute and chronic AD groups (Fig. 4H). The redox maps of the control mice revealed reliably low values. Those with AD lesions, on the contrary, displayed elevated values with higher inhomogeneity (Fig. 4G). These findings imply that the radical reduction reaction of Tempol in mice with AD improved before the onset of a visible skin rash and is exacerbated by oxidative stress elevation.
To investigate the therapeutic effect of the Tempol used as a contrast agent, Tempol was administered through free drinking water in AD-induced NC/NgaTndCrlj mice, and the pathological changes and blood IgE concentration as a blood inflammation marker were monitored. The gross observation showed the pathophysiology of AD in AD mice, whereas a clear suppression effect of pathological progression was observed in Tempol-treated mice (Fig. 5A). In the pathological analysis, we observed improvement in the disease score and decrease in skin thickness (Fig. 5B). Moreover, there was a significant reduction in the serum IgE antibody level, showing that Tempol treatment has an alleviating effect on AD (Fig. 5C).

Nonalcoholic steatohepatitis
Nonalcoholic steatohepatitis (NASH) is known to develop from nonalcoholic fatty liver disease (NAFLD) that results from lifestyle factors other than alcohol consumption, such as eating habits, lack of exercise, and obesity (3, 7, 53). An estimated 1 million individuals in Japan have NASH, and this number may increase to 10 million if NAFLD patients are also included. Approximately 80% of NAFLD cases are nonprogressive and have a benign course, whereas the remaining 20% progress to NASH that advances to cirrhosis and liver cancer via fibrosis (9). However, it is difficult to distinguish NASH liver from NAFLD using current diagnostic imaging methods. Oxidative stress is an important factor in the progression of NAFLD to NASH (26, 31, 48, 53). In particular, the mitochondria contribute to ROS generation and free fatty acid β-oxidation, promoting lipid accumulation. Thus, mitochondria dysfunction increases ROS production and lipid peroxidation (61). In fact, ultrastructural defects and mitochondrial malfunctions were detected in the NASH liver of humans and animals (5, 10). Therefore, the redox metabolism in NASH has been demonstrated in the mitochondria of the NASH liver as a main source of ROS generation (11, 29, 43, 73).
Currently, liver biopsy is the gold standard for diagnosing and staging NASH. However, it is an invasive procedure that may cause bleeding or infectious complications. In addition, the inspection costs, sampling errors, and differences in diagnostic classification among pathologists make it at a lower value. Therefore, noninvasive imaging technology such as regular MRI, CT, MR elastography, and ultrasound elastography has been developing to differentiate NASH from NAFLD, based on the imaging information of liver fat and fibrosis. This is because the imaging-based evaluation of the liver is more advantageous over the biopsy and serum biomarkers such as its noninvasiveness, the ability to diagnose all the liver regions, and quantitative analysis with localization (1, 32, 44, 46, 91). However, those imaging techniques that are based on the morphological or functional observation after the occurrence of liver fibrosis might not be suitable for distinguishing the early changes of NASH from NAFLD.
The feasibility of using in vivo DNP-MRI for NASH diagnosis based on redox status in the liver was assessed in a methionine-choline-deficient (MCD) mouse as an NASH model. For noninvasive tracking of the redox condition of the liver, in vivo DNP-MRI was conducted after oral administration of MCD (54). The distribution of the enhanced signal area was detected in the entire liver and kidney during 1–13 min after injection of carbamoyl-PROXYL probe (Fig. 6A). Using pharmacokinetic in vivo DNP-MRI, the decay rate of DNP enhancement was estimated (Fig. 6B). It is noteworthy that the reduction rate significantly decreased compared with that in control mice even at 1 week after initiating MCD treatment. Redox metabolism further decreased after longer feeding periods (Fig. 6B). Furthermore, the concentration of the oxidized form of carbamoyl-PROXYL in a liver homogenate solution of the control group was significantly lower than that in the 2-week MCD group (Fig. 6C). In contrast, after reoxidation with potassium ferricyanide, total carbamoyl-PROXYL levels in controls and MCD liver homogenates were not significantly different. These results indicate that the in vivo DNP-MRI reduction rate did not provide information on variations in liver absorption and excretion; however, the radical loss of the carbamoyl-PROXYL is based on the redox reaction. Moreover, the redox metabolic maps revealed that local redox changes were depending on the period of the MCD diet (Fig. 6E). To demonstrate the redox mechanisms, the redox reaction between carbamoyl-PROXYL and liver homogenates was directly investigated using X-band EPR. The EPR signal was significantly lower in the MCD groups than in the controls at 5 min after the addition of MCD. Interestingly, the addition of potassium cyanide (KCN), a complex IV inhibitor in the mitochondrial electron transfer chain (ETC), entirely inhibited these differences. Moreover, the EPR signal of carbamoyl-PROXYL remained unchanged with cytosol. These data indicate that the difference between the control and MCD groups in carbamoyl-PROXYL redox metabolism was abolished by the inhibition of the mitochondrial ETC in liver homogenate solutions.

The precise and noninvasive detection of NASH liver based on the monitoring of in vivo mitochondrial redox reactions with DNP-MRI could be demonstrated. These results also showed that the in vivo assessment of the mitochondrial redox metabolism is an imaging biomarker for NASH and may enable the distinction between NASH and NAFLD patients in clinical practice. Moreover, DNP-MRI with the nitroxyl probe method has potential value in accelerating drug discovery based on the early detection of NASH.
Conclusion
In this review, the applications of in vivo DNP-MRI with the nitroxyl radical method have been described for the detection of redox metabolism in animal models of oxidative diseases. The nitroxyl radical probes are not only used as DNP probes for monitoring tissue redox status but also show antioxidant activity. Therefore, this technique may be a powerful tool for theranostics of various oxidative diseases via monitoring of the tissue redox metabolism.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Medical Research and Development Programs Focused on Technology Transfer, Development of Advanced Measurement, and Analysis Systems (SENTAN) from the Japan Agency for Medical Research and Development, Grant Number 162128. This work was also supported by Japan Society for the Promotion of Science KAKENHI (Grant Numbers 18H02765 and 19H03358) and MEXT Quantum Leap Flagship Program (MEXT Q-LEAP) Grant Number JPMXS0120330644.