
Abstract
Background:
Phenotypic similarities exist between autism-related experiences and anxiety (especially social anxiety and obsessive-compulsive disorder [OCD]), making it difficult for autistic people to self-report their experiences using existing measures developed for nonautistic adults. We examined whether clarifications aiming to tease out autism-related experiences from social anxiety or OCD in self-report questionnaires would influence autistic and nonautistic participants' ratings.
Methods:
Two autistic consultants and two experienced clinicians were consulted to develop item clarifications aiming to disentangle autistic from anxiety experiences for two questionnaires: the Social Anxiety Questionnaire (SAQ) and the Padua Inventory (PI) for OCD. Autistic adults (n = 50) and nonautistic university students with higher (n = 81) and lower autistic traits (ATs; n = 104) completed the original questionnaire followed by the clarified questionnaire items online.
Results:
For social anxiety, there were few significant differences between the original and clarified item and total SAQ scores. For OCD, participants reported significantly lower scores for the OCD-clarified PI items than for the original items and the autism-clarified items. Larger original–clarified PI mean item differences were noted in items describing repetitive behaviors, “obsessional” thoughts, and contamination fears. Similar patterns of differences were found in autistic and nonautistic participants with higher and lower ATs, but differences were often larger in the autistic group.
Conclusion:
The SAQ in its original form appears to be an appropriate measure for autistic people to self-report social anxiety. However, autistic people appeared to complete the original PI items to reflect, to some extent, their autism-related experiences, rather than the originally intended OCD symptoms. Thus, the original OCD self-report ratings were inflated using the PI. Professionals should therefore clarify the intended meanings of different items of the PI to ensure more accurate and relevant ratings of OCD symptoms in autistic people.
Lay summary
Why was this study done?
Autistic people and people with higher autistic traits (ATs) often experience higher rates of anxiety. Anxiety measures developed for the general population may not be appropriate or accurate for measuring anxiety in autistic people. We investigated whether clarifying items in existing self-report questionnaires to tease out anxiety from autistic experiences would influence the way autistic adults self-report their social anxiety and obsessive-compulsive disorder (OCD) symptoms, and if so in what ways. We also wanted to know whether providing these item clarifications would affect the ratings of nonautistic individuals with varying rates of ATs to the same extent.
What did the researchers do?
We initially consulted two autistic adults and two clinicians with experience working with autistic adults and co-occurring mental health difficulties. We selected two measures: the Social Anxiety Questionnaire (SAQ) for social anxiety symptoms and the Padua Inventory for OCD symptoms. The consultants identified social anxiety and OCD items that could be interpreted or experienced differently by autistic people and proposed ways to clarify them to make their meaning clearer.
Next, 50 autistic people and 185 nonautistic university students participated in our online study. The nonautistic participants were grouped into those with higher or lower ATs. Participants completed the original social anxiety and OCD questionnaires first, followed by the clarified versions of the two questionnaires.
What were the results of the study?
For social anxiety, we only found small differences in ratings when participants used measures with or without clarifications. This was true in both autistic and nonautistic participants. For OCD symptoms, autistic people's OCD ratings were significantly lower for many items after we provided clarifications, especially for items describing repetitive behaviors, “obsessional” thoughts, and contamination fears. This finding suggests that in the original questionnaire, autistic people may have also been rating their autism-related experiences, not just the OCD experiences or symptoms the questionnaire was trying to measure. We found similar differences between the original and clarified item ratings in nonautistic participants with higher and lower ATs. However, the differences were more common and pronounced with the autistic participants.
What do these findings add to what was already known?
These findings suggest that original self-report measures of anxiety may need to be clarified so that autistic adults can better capture and rate their anxiety, rather than their autism-related experiences.
What are potential weaknesses in the study?
We used only two anxiety questionnaires, so these findings may or may not be applicable to other OCD or social anxiety questionnaires available. Also, the clarifications we provided may not be representative of all autistic people's experiences, and it is possible that there are other and better ways to clarify the items. We also conducted many item comparisons in this study, so there is a possibility that some findings were due to chance.
How will these findings help autistic adults now or in the future?
Our findings can help improve clinical interviews and use of anxiety questionnaires by making them more accurate. They can also help clinicians appreciate the importance of asking clarifying questions to ensure they better capture autistic adults' anxiety experiences.
Introduction
Autistic people often experience anxiety across their life span at rates much higher1–5 than the general population,6,7 with obsessive-compulsive disorder (OCD) and social anxiety some of the most commonly reported. 8 Higher anxiety rates are also consistently observed in individuals with higher autistic traits (ATs; i.e., elevated but subclinical social, communication, and behavioral characteristics similar to those observed in autistic people).9–11
While autistic people experience anxiety that often meets Diagnostic and Statistical Manual 12 (DSM-5) criteria (hereafter termed “common anxiety”), there is also evidence of anxiety presentations or experiences that do not fit neatly into the DSM-5, and which are more closely related to autistic experiences (hereafter termed “autism-related anxiety”). These may include (1) worries, fears, or anxieties about sensory experiences such as loud or high-pitched sounds; (2) worries about unexpected or sudden changes to environment, routines, or schedules; and (3) specific phobias that are much less common in the general population (such as fears of men with beards or mechanical things).13,14
Considerable overlap also exists between several “common” and autism-related anxiety experiences, but the same behavioral expressions are likely qualitatively different. 15 For example, reduced social interaction and eye contact could be due to (1) reduced or limited social motivation; (2) worries relating to autism-related social differences or difficulties; or (3) anxious anticipation and fear of social- or performance-related negative evaluations, which could be related to more “common” social anxiety. Furthermore, repetitive behaviors may be autism-syntonic (i.e., consistent with the individual's preferred/pleasurable or anxiety-reducing activities or interests) 16 or could be DSM-defined OCD-related compulsive behaviors performed in response to unwanted intrusive thoughts aiming to reduce anxiety. 17
To date, most existing anxiety measures used with autistic people have been developed for and validated in the general population; they may not adequately differentiate “common”/DSM-related from autism-related anxiety presentations or experiences. To the best of our knowledge, only two studies to date have attempted to tease out overlapping anxiety and autistic behaviors and explore autism-related anxiety experiences. One study developed an addendum to an existing semi-structured clinical interview—the Anxiety Disorders Interview Schedule (ADIS) 18 —with the researchers performing further systematic questioning to tease out “common” anxiety from potentially phenotypically similar autism-related experiences/anxieties in young autistic people. 19 Another study modified original item wordings from the Revised Children's Anxiety and Depression Scale 20 developed for nonautistic children and also included additional autism-relevant items, following review of the existing literature and interviews and consultations with caregivers, to develop the Anxiety Scale for Children–Autism Spectrum Disorder (ASC-ASD). 21 Both adapted measures demonstrated good psychometric properties and may be appropriate to capture autism-related anxieties in young autistic people.19,21
However, very little is known about whether existing anxiety measures are accurate and relevant for autistic adults to report their anxiety-related experiences. A recent meta-analysis 4 provided preliminary evidence that studies using structured interviews with clinicians resulted in lower adult prevalence estimates of OCD and social anxiety (19% and 26%, respectively) than studies using informant-completed questionnaires (43% and 51%, respectively) primarily developed for nonautistic adults, suggesting that it is important to improve reporting, screening, and assessing anxiety experiences by autistic people when using questionnaires.
The aim of this study was therefore to explore whether, and to what extent, clarifying items in existing self-report questionnaires for adults influence autistic people's social anxiety and OCD ratings. As nonautistic people with higher ATs also report higher levels of anxiety, this study included nonautistic participants (grouped into “higher AT” and “lower AT” subgroups); the aim of including nonautistic participants was not to compare them directly with the autistic group, but rather to explore if the pattern of within-group rating differences before and after clarifications in autistic people was also present, and to what extent, in nonautistic people with varying rates of ATs.
Methods
Study design
This online study employed a quantitative repeated-measures cross-sectional design.
Participants
We recruited (1) 52 autistic adults able to independently self-report and (2) 186 nonautistic university students from the National University of Singapore (NUS). We excluded two autistic participants and one nonautistic participant due to missing data (final nautistic = 50; nnonautistic = 185; see the Data Analytic Plan section).
Autistic participants self-reported their autism diagnosis (see Table 1 for all participant characteristics) and provided details of when, where, and by whom they received their diagnosis. None of the nonautistic participants reported being given an autism diagnosis. Eighty-eight percent of the autistic group scored above the cutoff i for the Broad Autism Phenotype Questionnaire 22 (BAPQ; see the Measures section; Table 2). Nonautistic participants were organized into “higher AT” (n = 81 ii ) and “lower AT” (n = 104) according to whether they scored above or below the BAPQ cutoff raw score of 3.15. 22
Demographic Characteristics of Autistic and Nonautistic (Higher and Lower Autistic Trait) Participants
All the participants in the autistic group without a formal ASD diagnosis scored above the BAPQ cutoff. Given that some individuals may experience barriers to formal diagnosis and that the patterns and strengths of results were unchanged when data from these participants were excluded, analyses were conducted on the data from all 50 autistic participants.
Total percentage exceeds 64%, 7.4%, and 6.7% who selected “Yes,” respectively, in autistic and in higher and lower AT groups, as participants were allowed to select more than one additional condition in their responses.
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; AT, autistic trait; N/A, not applicable; OCD, obsessive-compulsive disorder; PDD-NOS, pervasive developmental disorder–not otherwise specified.
Broad Autism Phenotype Questionnaire Scores and Number of Participants Meeting the Broad Autism Phenotype Questionnaire Cutoff per Group
Significant results with medium or large ES are in bold.
The BAPQ scores for four autistic participants were not calculated as they had more than 20% missing data, but all four had a professional clinical ASD diagnosis.
The relatively high percentage of nonautistic participants scoring above BAPQ cutoff (n = 81, 43.8% of nonautistic sample) is likely due to applying a cutoff from a Western sample to our Asian student sample, as Asian participants consistently report higher ATs than Western participants.23,24
The Cronbach's alpha were in the poor range for the higher AT participants (α = 0.47) and the borderline range for lower AT participants (α = 0.64). It has been previously suggested that Cronbach's alpha is likely to be underestimated and less accurate in nonnormal data (such as the BAPQ scores for the two subgroups) due to the presence of additional error or bias in estimating internal consistency. 33
BAPQ, Broad Autism Phenotype Questionnaire; ES, effect sizes.
Measures
All original and clarified versions of the self-report measures had excellent internal consistencies for all the three groups, with the exception of the BAPQ for the nonautistic groups (Tables 2 and 5).
The BAPQ
The BAPQ 22 is a 36-item questionnaire measuring ATs in the general population. The BAPQ cutoff score indicates higher ATs but was not designed to specifically screen for autism. Each item is rated on a 6-point Likert scale, ranging from 1 (very rarely) to 6 (very often). The total score was calculated by summing all BAPQ item raw scores and averaging across all 36 items (total score range 1–6; higher scores = more ATs). The BAPQ demonstrated better psychometric properties in a nonclinical sample than two other ATs measures. 25
The Social Anxiety Questionnaire
The 30-item Social Anxiety Questionnaire 26 (SAQ) assesses the level of unease, stress, or nervousness in different social situations. Rated on a 5-point Likert scale ranging from 1 (not at all or very slight) to 5 (very high or extremely high; total score range 0–150; higher score = more anxiety), the SAQ demonstrated good internal consistency, reliability, and validity with nonautistic participants.27,28
The Padua Inventory
The 60-item Padua Inventory 29 (PI) measures the degree of disturbance associated with obsessive-compulsive symptoms. Each item is rated on a 5-point Likert scale ranging from 0 (not at all) to 4 (very much; total score range 0–240; higher scores = more OCD symptoms). It has good internal consistency and validity in Western and Asian student samples30–32 and was used in a study to investigate the overlap between ATs and OCD in the general population. 11
Procedure
Development of clarifications to the original questionnaire items iii
Two autistic consultants/advocates with postgraduate educational qualifications (K.M.K. and D.-J.L.) and two psychiatrists with extensive experience working with autistic adults with co-occurring mental health difficulties (G.M.Y.T. and K.-C.W.) were our consultants. The researchers (X.Y.C. and I.M.) presented the original SAQ and PI items individually to the consultants, who identified items that could be interpreted or experienced differently from the original “common”/DSM-related social anxiety or OCD meanings by autistic people and could therefore potentially be ambiguous for autistic people. iv
The consultants identified 5 of the 30 SAQ items (17%) and 40 of the 60 PI items (67%) as potentially ambiguous in meaning. They then discussed and proposed ways to clarify the items, so as to better disentangle anxiety from overlapping autism-related anxieties/experiences. The research team considered together and synthesized the comments and suggestions from all consultants to propose initial clarifications. The consultants were then invited to further comment and edit the proposed clarifications through e-mail consultations before item clarifications were finalized.
To achieve the study's aims, the finalized item clarifications reflected either “common” anxiety or autism-related experiences (see Table 3 for examples v ). Some items were determined by consultants to have more than one relevant autism-related experience, hence resulting in three clarified options. Each original item could therefore have one, two, or three clarified options, depending on the consultants' input.
Examples of Original Questionnaire Items and Their Corresponding Clarified Items Following the Consultation Process
Full list of the items can be requested from the authors.
PI, Padua Inventory; SAQ, Social Anxiety Questionnaire.
Ethics
The NUS Psychology Department Ethics Review Committee approved the study (reference code: 2018-August-63). All participants gave written informed consent. All data were anonymously submitted.
Recruitment
We recruited autistic adults within Singapore and internationally via social media, word of mouth, the researchers' professional contacts, and mailing lists of the NUS Disability Support Office and a Singapore-based employability and employment support center for autistic adults. Nonautistic Singapore-based university students were recruited through a research-participant pool or through posters placed around the university.
Data collection
Participants completed a 30-minute online survey in this order: (1) demographic questionnaire; (2) original SAQ and PI questionnaires (in randomly counterbalanced order across participants); (3) BAPQ; (4) a 3- to 5-minute Spot-The-Difference distraction task to reduce recency effects on participants' subsequent ratings; and (5) clarified SAQ and PI (also randomly counterbalanced), using the same rating scale as the original questionnaires.
Data analytic plan
Missing data
Missing data ranged from 1.6% to 5.5% in the different questionnaires/versions for the autistic group, and from 0.03% to 0.4% for the nonautistic group. vi No instructions on the handling of missing data were specified in the original measures. We excluded participants from further analyses if more than 20% of the main questionnaire items were missing (nautistic = 2; nnonautistic = 1 vii ). For subsequent analyses, if fewer than 20% of items in any given measure were missing for a participant, they were substituted using the participants' mean item score respectively from the original or clarified questionnaires.
Data analyses
All analyses were conducted using SPSS 20.0. Original total scores were calculated according to the measures' instructions.22,26,29 Social anxiety- or OCD-clarified total scores were calculated as follows: all ratings of clarified items reflecting “common”/DSM-related social anxiety or OCD interpretations + all original ratings of items that did not require clarification + ratings of items with only minor wording changes. Autism-clarified total scores were calculated similarly but included the autism-clarified instead of anxiety-clarified item ratings.
The Friedman test compared original with their corresponding clarified item scores. Post-hoc Wilcoxon signed rank test examined differences between original and clarified items, and between anxiety- and autism-clarified items. Data were checked for normality using the Shapiro–Wilk test. Normality assumptions were met for the autistic group's data, but not for all the measures in the nonautistic groups (p < 0.05). Paired samples t-tests or the Wilcoxon signed rank test were used accordingly for data that met or did not meet normality assumptions.
Bonferroni corrections were not applied to the multiple comparisons performed, as they are conservative and may result in increased type II errors, especially within correlated measures (i.e., the original and clarified measures in this study).35–37 However, effect sizes (ES) were calculated and reported, and emphasis was placed on p < 0.01 and medium (r = 0.30) and large ES (r = 0.50) 38 in the interpretation of results.
Post hoc power analysis was conducted using G*Power. 39 With nautistic = 50, nhigherAT = 81, and nlowerAT = 104, and alpha level of 0.05, the power to detect a medium effect in the within-participants' differences between original and clarified ratings was 0.93 for the autistic group and 0.99 for the higher and lower AT groups.
Results
Social anxiety: differences between original and clarified SAQ ratings
SAQ differences at item level
Table 4 presents statistically significant item differences only; all other nonreported comparisons were of small ES (−0.29 < r < −0.01) and/or were not significant. viii
Statistically Significant Social Anxiety Questionnaire Item Contrasts Between Original, Social Anxiety-, and Autism-Clarified Item Ratings
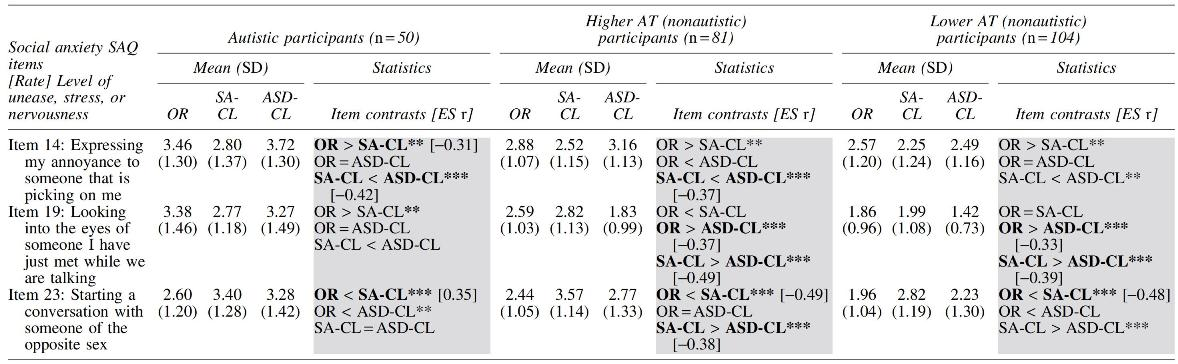
Significant differences with medium or large ES (i.e., >0.3) are in bold; only ES >0.3 values are presented in full, all other ES were small (<0.3) and are not presented in the table.
“ = ” Denotes nonsignificant rating differences; “<” denotes significantly less than; “>” denotes significantly greater than.
p ≤ 0.01, ***p ≤ 0.001. Full statistics (including results that were statistically nonsignificant) can be requested from the authors.
The gray shadings indicate columns for item contrasts.
ASD-CL, autism-clarified item; OR, original item; SA-CL, social anxiety-clarified item.
Original versus anxiety-clarified items
For autistic participants, original item ratings were significantly higher than the anxiety-clarified items for one (item 14) and significantly lower for another one (item 23) of the five SAQ items that were clarified with medium ES. For the nonautistic participants, only original item 23 was significantly lower than the corresponding anxiety-clarified item, and ES was also medium, similar to the autistic group (Table 4).
Original versus autism-clarified items
For autistic participants, original vs. autism-clarified item differences were small and/or nonsignificant. Both the higher and lower AT groups reported significantly higher ratings in one original item (item 19) compared with the corresponding autism-clarified item, with medium ES (Table 4).
Anxiety- versus autism-clarified items
Autistic participants reported significantly lower anxiety-clarified than autism-clarified ratings in one of the five clarified items (item 14), with medium ES, and the same was found in the higher AT participants. The higher AT group also reported significantly higher ratings on two anxiety-clarified items compared with the corresponding autism-clarified ones, with medium ES (items 19 and 23); the same pattern was found for item 19 only for lower AT participants (Table 4).
Differences in SAQ original–clarified total scores
The only significant difference was that autistic participants reported significantly lower, whereas the higher and lower AT participants reported significantly higher, anxiety-clarified compared with autism-clarified total scores with medium ES (Table 5); there were no significant differences between the original compared with both clarified total SAQ scores in any of the three groups.
Social Anxiety Questionnaire and Padua Inventory Original and Anxiety-Clarified/Autism-Clarified Total Score Differences
Significant differences with medium or large ES (i.e., >0.3) are in bold.
Full statistics can be requested from the authors.
n = 49 for PI for the autistic sample.
ASD-CL, autism-clarified; OCD-CL, OCD-clarified; OR, original; SA-CL, social anxiety-clarified.
OCD: differences between original and clarified PI ratings
PI differences at item level
Table 6 presents statistically significant item differences only; all other nonreported comparisons were of small ES (−0.29 < r < 0) and/or were not significant. ix
Statistically Significant Padua Inventory Items Contrasts Between Original and Clarified (Obsessive-Compulsive Disorder- and Autism-Clarified) Item Scores

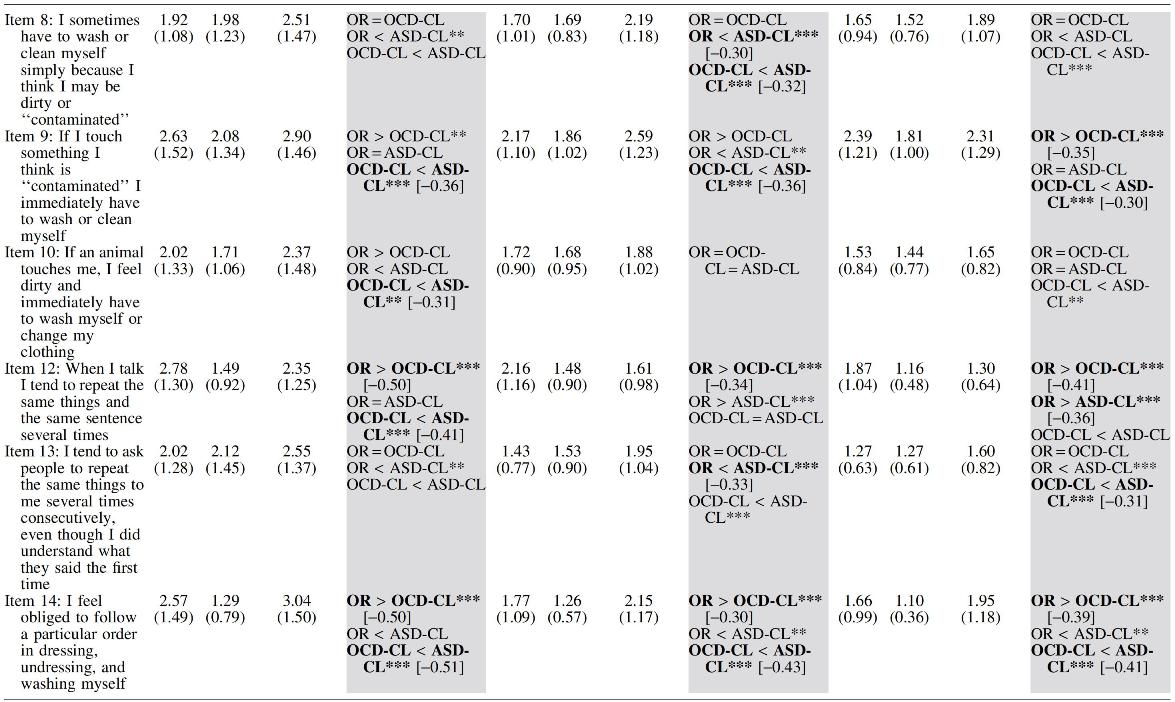

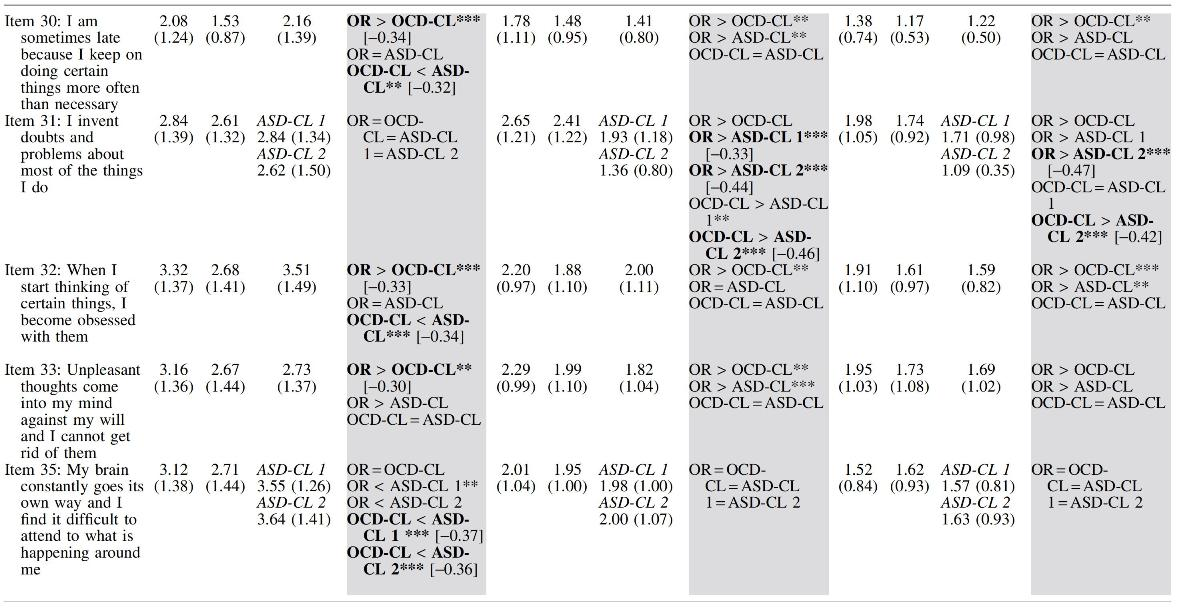
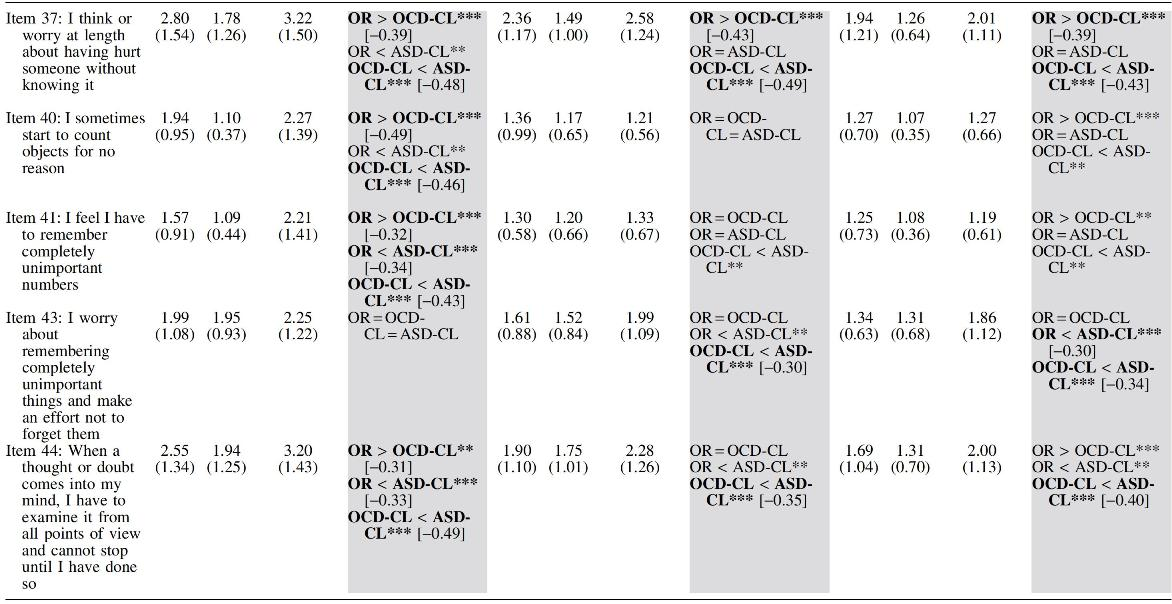
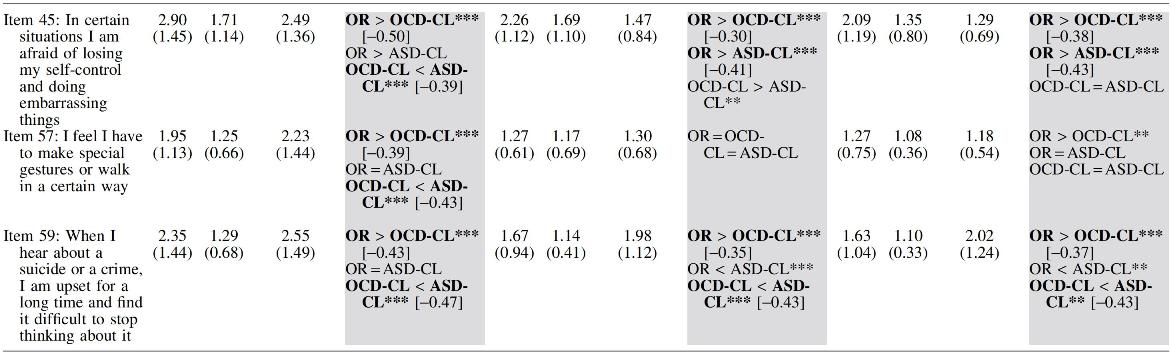
Significant differences with medium or large ES (i.e., >0.3) are in bold; only ES >0.3 values are presented in full, all other ES were small (<0.3) and are not presented in the table.
“ = ” denotes nonsignificant rating differences; “<” denotes significantly less than; “>” denotes significantly greater than.
p ≤ 0.01, ***p ≤ 0.001. Full statistics (including results that were statistically nonsignificant) can be requested from the authors.
The gray shadings indicate columns for item contrasts.
ASD-CL, autism-clarified item; OCD-CL, OCD-clarified item; OR, original item.
Original versus OCD-clarified items
Autistic participants reported significantly higher ratings for 16 of the 40 original items, compared with the corresponding OCD-clarified items, with medium-to-large ES. The same pattern was found in both higher and lower AT participants but only for 7/40 items, with medium ES (Table 6).
Original versus autism-clarified items
The autistic participants' original item ratings were significantly lower than the corresponding autism-clarified ones in 3/40 and higher in 1/40 items, all with medium ES. The same patterns and ES were found in the higher AT group (6/40 and 3/40 items, respectively) and in the lower AT group (3/40 and 5/40 items, respectively; Table 6).
OCD-clarified versus autism-clarified items
Autistic participants' OCD-clarified item ratings were significantly lower than the autism-clarified ones in 22/40 and higher in 1/40 items, with mostly medium ES. The same patterns and ES were found in the higher AT group (11/40 and 2/40, respectively) and in the lower AT group (10/40 and 3/40 items, respectively; Table 6).
Notably, the significant differences were mostly in items describing repetitive behaviors, “obsessional” thoughts, and contamination fears, in which the OCD-clarified ratings were consistently lower than the autism-clarified and original item ratings.
Differences in PI original–clarified total scores
All the groups reported significantly higher original total PI score compared with the OCD-clarified total score, with at least medium ES. There were no statistically significant differences between the original and autism-clarified total scores for any of the groups, and ES were small. All the groups reported significantly lower OCD-clarified than autism-clarified total scores, with at least medium ES (Table 5).
Discussion
Social anxiety self-report ratings using the SAQ
Our findings suggest that the original SAQ measure, a relatively new and freely available self-report measure, is sufficiently clear and specific to assess social anxiety in autistic people and in people with higher ATs and to distinguish social anxiety from autism-related experiences; it can therefore probably be used in its existing form with autistic people and/or people with higher ATs. The SAQ explicitly invites respondents to rate their anxiety in specific social situations, instead of rating more general symptoms of social avoidance or social interaction difficulties (as with other measures that overlap with autistic experiences), the nature and function of which are much more difficult to assess via screening measures.15,40 Indeed, a previous study 41 found that autistic participants with co-occurring social anxiety reported greater social anxiety than nonautistic participants with social anxiety diagnoses on a questionnaire containing multiple overlapping and ambiguous experiences, 42 compared with questionnaires that mainly require participants to rate their fear or worry, 43 or ones that include fewer overlapping experiences. 44 It is therefore possible that other social anxiety screening measures that were not explored in our study may have greater symptom ambiguity or overlap that will likely require clarification for a more accurate self-report.
OCD self-report ratings using the PI
Our findings suggest that autistic people in our study were possibly rating, at least to some extent, their autism-related experiences rather than the originally intended OCD experiences in the original PI measure, largely due to limited specificity in the item descriptions, thereby resulting in significantly higher reported ratings for many original PI items. Independent administration of this OCD measure in its original form with autistic people, and to a lesser extent, people with higher ATs, may therefore be less helpful or appropriate—careful revision of the items similar to the clarifications made in our study to enhance specificity and relevance is likely required to better disentangle OCD from autism-related self-ratings. This is consistent with a meta-analysis showing that rates of current OCD were lower when autistic people were assessed using clinical interviews instead of questionnaire measures, 4 suggesting that opportunities to further clarify particular behavioral expressions of OCD-related experiences are important to disentangle “common” anxiety from potentially overlapping autistic experiences.19,21 In agreement with findings from the previous literature that restricted, repetitive behaviors are less discriminating,45,46 our findings also suggest that repetitive behaviors likely represent significant areas of overlap between autism and OCD, which will require specific attention and clarification during assessment.
Additionally, it appears that teasing out autistic from OCD-related experiences in self-report measures, as demonstrated empirically in this study, had similar patterns of effects on both autistic and nonautistic participants with varying rates of ATs, but the ES of the differences appeared to be larger in the autistic participants' rating differences and more items were significantly different in the autistic compared with the nonautistic groups.
Strengths, limitations, and future directions
First, the internal consistency of the BAPQ was suboptimal in the nonautistic groups. Second, the item clarifications were generated in collaboration with autistic people and clinicians with extensive experience working with autistic people. However, our autistic consultants had postgraduate qualifications and high reading and education levels.47–50 Similarly, 34% of our autistic sample were university/college students or graduates, whereas 28% were in full-time employment. Hence, the clarifications provided may not be representative of the experiences of autistic people across the spectrum. Our findings therefore require replication with a larger and more diverse autistic sample. Finally, while the clarifications provided were intended to clarify the experiences rated by our participants, the specificity of these clarifications may have also influenced the ratings: some clarified items could have been too specific for some of the participants. x
As research on the prevalence of anxiety-related problems in autistic people has often used self- or informant-based anxiety measures for the general population, future studies should clarify ambiguous items with multiple alternative interpretations, especially for OCD, to establish more reliable and accurate rates, and should use a combination of informant- and clinician-based measures to obtain clinical information on anxiety in autistic adults. Future research on informant-based measures could provide participants with open-ended questions after they have rated an item to allow them to comment and provide feedback on the clarity and relevance of the items/clarifications made. Finally, other commonly employed self-report anxiety measures should also be investigated in this way, leading to the development and validation of autism-relevant versions of existing anxiety measures, especially OCD ones. Other anxiety experiences, including generalized anxiety, panic, and trauma-related anxiety, need to be explored in a similar way so that autistic people can use informant-based measures that are more valid, specific, and relevant to their own experiences.
Footnotes
Authorship Confirmation Statement
X.Y.C. and I.M. conceptualized and designed the study, with input from all co-authors. All authors contributed to the development of the clarified questionnaire items. X.Y.C. collected the data and conducted the statistical analyses. All authors contributed to data interpretation. X.Y.C. and I.M. led to the development of the article, and all authors contributed to drafts of the article and revised the article critically. All authors have approved the final article submitted. This article has been submitted solely to this journal and is not published, in press, or submitted elsewhere.
Acknowledgments
The research team is grateful to the authors of the SAQ and PI measures employed in this study (Dr. Vincente E. Caballo, Dr. Isabel C. Salazar, Dr. María Jesús Irurtia, Dr. Benito Arias, Dr. Stefan G. Hofmann, and Dr. Ezio Sanavio) for allowing us to develop and study clarifications of the original items for the purposes of this study. We also thank Dr. Sarah Cassidy of the University of Nottingham for sharing her interview protocol for obtaining feedback on existing assessment tools relating to mental health problems, self-injury, and thoughts of ending life from autistic people, which helped shape our consultation for item clarifications in this study. We are grateful to the Autism Resource Centre (Singapore), the NUS Disability Support Office, and Ms. Brenda Tan for facilitating dissemination of information about the study and the recruitment invitations/posters. We also thank Mr. Truman Teo for his assistance with setting up the online survey. Finally, we thank all participants for sharing their experiences and participating in the study.
Author Disclosure Statement
All authors report no competing financial interests.
Funding Information
This study was supported by an internal fund for Thesis Support to the first author, from the Department of Psychology, National University of Singapore.