
Abstract
Background:
The historical focus on autism as a childhood disorder means that evidence regarding autism in adulthood lags significantly behind research in other age groups. Emerging studies on the relationship of age with autism characteristics do not target older adult samples, which presents a barrier to studying the important variability that exists in life span developmental research. This study aims to further our understanding of the relationship between the Autism-Spectrum Quotient Scale and age in a large adult sample.
Methods:
The present study examines the relationship of Autism-Spectrum Quotient Scale (AQ) scores with age in 1139 adults, ages 18–97 years. Participants came from three distinct samples—a sample of primarily students, a sample of MTurk participants, and a sample of primarily community dwelling older adults. The majority of the participants did not self-report an autism diagnosis (91%), were female (67%), and identified as White (81%). Participants completed the AQ primarily via online surveys. Researchers scored the AQ following six common scoring practices.
Results:
Results of preregistered analyses indicate that autism characteristics measured by the AQ are not strongly associated with age (r values from −0.01 to −0.11). Further findings indicate that the measurement of autism characteristics is consistent across age into late life using both multiple groups and local structural equation modeling approaches to measurement invariance (comparative fit indices = 0.82–0.83, root mean square error = 0.06) as well as reliability analysis. Finally, demographic and autism-related variables (sex, race, self-identified autism spectrum disorder diagnosis, and degree of autism characteristics) did not moderate the relationship between age and autism characteristics.
Conclusion:
These results suggest that self-reports of autism characteristics using the AQ do not vary strongly by age in this large age-representative sample. Findings suggest that the AQ can potentially serve as a useful tool for future research on autism across the life span. Important limitations on what we can learn from these findings point toward critical avenues for future research in this area.
Lay summary
Why was this study done?
Self-report questionnaires of autism characteristics are a potentially important resource for studying autism in adulthood. This study sought to provide additional information about one of the most commonly used self-report questionnaires, the Autism-Spectrum Quotient Scale (AQ), across adulthood.
What was the purpose of this study?
This study intended to determine if there is a relationship between scores on the AQ and age. Researchers also worked to identify which of the multiple different ways of scoring the AQ worked best across adulthood.
What did the researchers do?
Researchers collected data from over a thousand participants aged 18–97 years. Participants from three different age groups completed online surveys to self-report their levels of autism characteristics on the AQ. Researchers tested the relationship between AQ scores and age with six different commonly used ways to calculate AQ scores. Researchers used multiple statistical techniques to evaluate various measurement properties of the AQ.
What were the results of the study?
The results indicate that autism characteristics measured by the AQ are not strongly associated with age. Along with that, there is evidence that certain approaches to measuring of autism characteristics are consistent across age into late life and do not vary with demographic and autism-related factors.
What do these findings add to what was already known?
These results add to the growing evidence that self-reports of autism characteristics using the AQ in general samples are not strongly associated with age across adulthood. These findings also provide guidance about ways of scoring the AQ that work well through late life.
What are potential weaknesses in the study?
While the AQ has a degree of relationship with autism diagnoses, this is far from perfect and has not been evaluated in the context of aging research. Therefore, findings from the present research must be carefully interpreted to be about autism characteristics not diagnoses. The sample was also limited in a number of other ways. As in any studies including a broad age range of individuals, the oldest participants are likely quite healthy, engaged individuals. This may particularly be the case given the higher mortality rates and health challenges seen with autism. Similarly, as with any self-report research, this research is limited to those individuals who could answer questions about their autism characteristics. The sample was also predominantly White and nonautistic. Finally, the research was limited to one point in time and so cannot tell us about how autism characteristics may change across adulthood.
How will these findings help autistic adults now or in the future?
These findings support the potential for the AQ to be a useful tool for future research on autism in adulthood. For example, researchers can use measures such as the AQ to study how autism characteristics change over time or are associated with aging-related issues such as changes in physical health and memory. Such research may be able to provide a better understanding of how to support autistic individuals across adulthood.
Introduction
A growing literature recognizes the need for a greater understanding of autism across the life span, including well into late life.1–6 The historic focus on autism in childhood limits evidence to date, to the degree that older adults are referred to as a “lost generation.” 7 A notable barrier to research in adulthood is the lack of validated diagnostic tools for autism particularly for older adults, with those commonly used in children and younger adults8,9 either not calibrated or not feasible to conduct later in adulthood.10–13 This lack of available measures makes self-report questionnaires of autism characteristics an important avenue for studying autism in adulthood.
The most well known and well studied of these self-report questionnaires is the Autism-Spectrum Quotient Scale (AQ). 14 Given the contribution of the AQ to understanding autism characteristics, identifying the relationship between the AQ and age is critical for research seeking a better understanding of autism in adulthood. At present, a small number of studies provide evidence on the relationship of the AQ with age in adulthood, and findings vary across these studies. Findings conflict in autistic samples with evidence for both a curvilinear relationship such that AQ scores are lower in later adulthood 15 and a positive relationship between age and AQ scores. 16 In both samples, the relationship between age and autism characteristics is not significant for nonautistic individuals, but a large panel study demonstrates a J-shaped relationship with age such that autism characteristics are highest during late life in the general population. 17 The present study uses a sample of 1139 adults ages 18–97 years to replicate and extend research on the relationship of the AQ with age in three ways.
First, it is not clear that existing evidence on the relationship of AQ with age includes participants older than 79 years, thus restricting our knowledge to the “young-old,” with little insight into what autism characteristics may look like in the “oldest-old.”18,19 While the standard U.S. Census demographic criteria for older adulthood use a threshold of 65 years of age, important variability, heterogeneity, and age-related change exist within this age group.20–23 Autism is associated with important age-related variables such as physical health,24–27 cognitive performance,28,29 and psychological well-being.30–35 In addition to their implications for overall quality of life, these challenges have ancillary impacts on families and caregivers, a significant financial impact, and the potential to create greater risk of acute and chronic disease burden across the life span.36,37 Validating the AQ may particularly be useful in this demographic given the uncertainty about the extent to which autism characteristics are present in the general aging population and the likelihood that autism characteristics may be associated with the need for additional support in later adulthood. 38
Second, we examine the relationship of AQ scores with age across multiple different scoring protocols of the AQ. Prior research used both the original AQ15,16 and the abbreviated 10-item version of the AQ. 17 However, psychometric studies of the AQ suggest that optimal measurement fit may occur with a subset of 28 items. 39 In examining different scoring models, we have the opportunity to identify a well-fitting scoring protocol that is psychometrically consistent across age using tests of measurement invariance. Measurement invariance is a best practice analysis that establishes the extent to which a construct is consistent across different values of a potential moderating variable, in this case, age. For example, it is possible that the meaning of items may drift with generational language differences causing changes in the way individuals respond to a given items or set of items in a questionnaire. The AQ demonstrates invariance across individuals with and without an autism spectrum disorder (ASD) diagnosis. 40 To our knowledge, there are no published studies testing the age invariance of the AQ. Given that much of what we know about the AQ comes from young adult samples,14,41 age measurement invariance is an important psychometric question especially when using the AQ across adulthood. Confirmation that the AQ demonstrates measurement invariance with age will establish best fitting models of the AQ and establish that any observed age differences in the AQ are due to actual age differences and not due to differences in scale function with age.
Finally, the present sample allows us to conduct exploratory analyses investigating potential moderating variables of the relationship of AQ scores with age. Prior work in this area suggests that autism diagnosis may be an important moderator, with two studies showing no relationship in individuals without autism.15,16 In addition, we test the extent to which effects vary for individuals who self-report elevated AQ scores (≥26)42,43 compared with those who self-report lower AQ scores, as well as across gender and race.
Methods
Participants
Participants represent pooled data (N = 1139) from three online samples in which individuals completed the AQ. Sample 1 is primarily undergraduate students and their family members (n = 369, Mage = 23.07, SDage = 8.73, age range = 18–63) who completed the AQ for course credit. Sample 2 is a group of Mechanical Turk participants (n = 391, Mage = 34.01, SDage = 11.26, age range = 18–75) who received $0.15 as part of a larger study. Sample 3 is primarily older adults (n = 379, Mage = 65.42, SDage = 14.91, age range = 18–97) who participated in a study of autism and aging funded by NIH Grant No. R21 AG059051-01. Researchers recruited Sample 3 participants primarily through paid advertisements and mailers. There was a monthly drawing for $100 for participation in Sample 3. Sample 1 and Sample 3 participants also found out about the study from postings on online autism websites and discussion forums, through family members of children participating in intervention studies with our research team, and through outreach with local community partners. In Sample 3, targeted efforts via social media advertisements and paid mailers attempted to recruit more participants of color but with limited success. There were no exclusion criteria for participation in these studies. The only inclusion criterion for the present analyses was completion of the AQ as part of one of the samples described previously. Our institution's institutional review board approved all data collection efforts and the study met the American Psychological Association (APA) ethical guidelines for human research.
Measures
Demographic variables
Age was a primary variable of interest in this study. The sample represents three U.S. Census demographic age groups 18 —young adults (age 18–44 years), midlife adults (age 45–64 years), and older adults (age 65–97 years). Sex, race, and self-reported ASD diagnostic status are demographic moderators in exploratory analyses. Demographic details of the whole sample and by age group are available in Table 1.
Demographic Characteristics
Note: ASD+/− indicates whether (+) or not (−) a participant self-reported having an ASD diagnosis. AQ+/− indicates whether a participant scored a 26 or higher (+) or below 26 (−) on the AQ-50 using count scoring.
AQ, Autism-Spectrum Quotient Scale; ASD, autism spectrum disorder; SD, standard deviation.
Autism-Spectrum Quotient Scale
The AQ quantifies participants' self-report autism characteristics. 14 The AQ consists of 50 statements such as “I tend to have very strong interests, which I get upset about if I can't pursue” and “I find social situations easy.” Participants respond to each statement from “definitely agree” (1) to “definitely disagree” (4).
Procedure
Data collection and storage for all three samples occurred via the Research Electronic Data Capture (REDCap) electronic data capture tools hosted at Canisius College. REDCap is a secure, web-based application designed to support data capture for research studies, providing (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources. 44 To increase accessibility for older adult participants, participants in Sample 3 had the option to take surveys via a paper-and-pencil format rather than as an online survey.
Analyses
All analyses were preregistered at https://osf.io/ncbgj following guidelines for preregistration of planned secondary analyses. 45 The preregistration for this study provides additional information about the researchers' knowledge of the data before conducting analyses, experience with the data sets, scoring protocols, and information on alternative models considered had the primary planned measurement models failed to achieve adequate fit. Deidentified data, data scoring codes, analysis code, and R Markdown output for this article are available at https://osf.io/evh6f. Because of privacy concerns for our relatively small number of participants self-identifying as having an ASD diagnosis, additional data from this subsample are available by request.
All analyses were conducted in R version 4.0.2. 46 Given the size of the sample, significance values are reported for all analyses, but judgments of effect are based on the effect size estimates themselves using guidelines from Funder and Ozer (e.g., “r = 0.30 is ‘large’ and potentially powerful in the short and long run”) and Cohen.47,48 Post hoc power analyses computed with the pwr package indicate that this sample size allows us to detect small correlation effects of 0.10 with a power of 0.90 and a significance level of 0.05. 49 This pooled sample size is adequately powered to test structural models. 50
Scoring the AQ
Researchers used two common approaches to score the AQ: (1) characteristic count scores with participants receiving 1 point for each statement where they endorsed an autism characteristic and (2) characteristic intensity scores using raw item responses on the 4-point scale. Researchers applied this scoring across the full 50 items and in two shorter versions, the AQ-Short 39 where 28 items form two distinct subscales (social interaction and numbers/patterns), and the 10 item AQ-10.14,51 Count scores on the AQ-50 identified a subset of participants who self-reported AQ scores of 26 or above.42,43 Identification of this group facilitated exploratory analyses comparing study effects at different levels of autism characteristics.
Measurement invariance
We used two different approaches to measurement invariance using structural equation modeling (SEM). Full information maximum likelihood procedures in lavaan imputed indicator-level missing data. 52 Lavaan constrains the first factor loading to unity by default. All models were estimated using maximum likelihood estimation with robust standard errors and fixed-factor scaling standardization. Model fit comparisons for structural measurement models and tests of measurement invariance are evaluated by comparing comparative fit indices (CFI), root mean square error (RMSEA), standardized root mean square residual (SRMR), and sample-size adjusted Bayesian information criterion (SABIC). Acceptable fit thresholds are present when CFI are >0.95 and RMSEA and SRMR are <0.08. A lower SABIC indicates a superior fit when comparing multiple models. 53 Full fit statistics are available at https://osf.io/evh6f.
Tests of measurement invariance begin by identifying a measurement model for the scale of interest that fits well across the sample. For example, in research on the AQ, a response to the first item “I prefer to do things with others rather than on my own” serves as a manifest indicator of the latent AQ subscale, “social skills.” Each latent subscale serves as an indicator of additional higher order latent constructs. In this case, we used item-level responses on the 4-point scale to build two measurement models for the AQ:
One Latent Factor, Five Subscale Indicators. In the first measurement model, items served as manifest indicators to construct the five subscales from the 50-item AQ scoring—social skills, attention switching, attention to details, communication, and imagination, which served as indicators for a single, latent AQ factor.
17
Two-Factor. The second measurement model followed the model identified in work with the AQ-Short.
39
In this model, 28 of the original 50 AQ items are used as manifest indicators for five subscales (social skills, routine, switching, imagination, and numbers/patterns), four of which (social skills, routine, switching, and imagination) are used as indicators of a higher order latent factor representing social interaction that is distinct from but nonorthogonal to the remaining number/pattern construct.
Multiple group tests of measurement invariance proceed by establishing configural invariance comparing groups on the basic structure of the measurement model without any specified constraints. Effectively, configural invariance shows that the same indicators contribute to the same higher order latent construct for each group. Next, constraints are added forcing indicator loadings on latent constructs to be equivalent across groups to test metric invariance. This means that the indicator is contributing to the higher order construct in the same way for each group. Finally, scalar invariance constrains the estimation of the intercept of each indicator to be equivalent across groups. Scalar invariance means that individuals from different groups who have the same score on the higher order construct will also have the same pattern of values on the indicators. Here, multiple group measurement invariance tests the configural, metric, and scalar invariance of the AQ across three distinct age groups (young adult, midlife adults, and older adults).
This traditional approach to measurement invariance is necessarily limited because it relies on testing age invariance through binning the continuous variable of age into artificial age groups. New techniques using local SEM allow analysis of age as a continuous variable. 54 Local SEM does this by using age weighting to provide estimates of the measurement model for each age point. For example, an estimate for 50-year-old participants weights 49- and 51-year-old participants more than 30- and 60-year-old participants who are weighted more than 20- and 70-year-old participants. This allows each participant to be used in estimating the model at any given age point increasing power for the estimation of the model at each age point. Thus, rather than limiting models by age groups, model estimation occurs at each age point and age-graded trends in fit and model parameters can be identified. Following recommendations for samples of this size, we set the bandwidth parameter for these analyses to h = 2 prioritizing the weighting of ages within two standard deviations of the focal age. 54 This provided an effective N for the total sample of 24,794 ranging from 37 effective participants at age 97, to 593 effective participants at age 24.
Results
Table 2 presents the zero-order correlations of age with the different common scoring approaches to the AQ, as well as the reliability and descriptive statistics for each scoring approach. A weak negative association was present for age and intensity scores on the full 50-item AQ. No other methods of calculating AQ scores were meaningfully associated with age.
Descriptive Statistics and Zero-Order Correlations with Age for Autism-Spectrum Quotient Scale Scores Across Multiple Scoring Approaches
CI, confidence interval.
An important assumption underlying each of these correlation analyses is the assumption of measurement invariance—that the AQ functions equivalently across age. The large sample size of our sample allows us to test this previously untested assumption for some of these scoring protocols. Replicating prior research on the measurement model of the AQ, the two-factor AQ-Short measurement model showed superior fit [χ 2 (344) = 1592.58, CFI = 0.85, RMSEA = 0.06, SRMR = 0.06, SABIC = 78,001.90] to the single-factor AQ-50 solution [χ 2 (1170) = 6808.06, CFI = 0.66, RMSEA = 0.07, SRMR = 0.07, SABIC = 139,438.60], which, at times, failed to converge. Although the CFI for the AQ-Short measurement model were lower than normal acceptable thresholds, the other fit indices were acceptable and superior to the single-factor AQ-50. These fit statistics are quite similar to those in prior work. 39 The lower CFI seen with the AQ-Short are likely due to the low correlations of some of the items expected in a higher order model. 55 As such, we used the two-factor AQ-Short model for tests of measurement invariance.
Multiple group tests of configural invariance confirm that the AQ-Short measurement model had acceptable fit across the three age groups (CFI = 0.83, RMSEA = 0.06). This suggests that the same items contribute to the same higher order construct in each group. As shown in Table 3, chi-square metrics suggest there was a slight decrease in chi-square fit but not in CFI nor RMSEA when constraining loadings (metric invariance) and intercepts (scalar invariance). 56 Local SEM confirms that the measurement model of the AQ-Short identified in prior work appears to be consistent across age (MCFI = 0.86, SDCFI = 0.04; MRMSEA = 0.06, SDRMSEA = 0.01). 39 Materials available at https://osf.io/evh6f provide details on specific parameter estimates across the measurement model and visualizations of fit statistics and parameters at each age. In addition to measurement invariance across age, exploratory analyses indicate that the AQ-Short has good reliability across age groups with alpha reliability of 0.87 (young adults), 0.91 (midlife), and 0.83 (older adults) for the social behavior subscale, and 0.78 (young adults), 0.83 (midlife), and 0.72 (older adults) for the number/pattern subscale.
Multiple Group Measurement Invariance of Autism-Spectrum Quotient Scale by Age Groups
CFI, comparative fit indices; RMSEA, root mean square error.
Figure 1 (social behavior subscale) and Figure 2 (number/pattern subscale) visualize the relationship between the AQ-Short and age. Exploratory analyses indicate a small nonlinear, cubic relationship between age and both the social behavior (age 3 β = 0.15, p < 0.001) and number/pattern (age 3 β = 0.12, p = 0.005) subscales of the AQ-Short, visible in these figures.
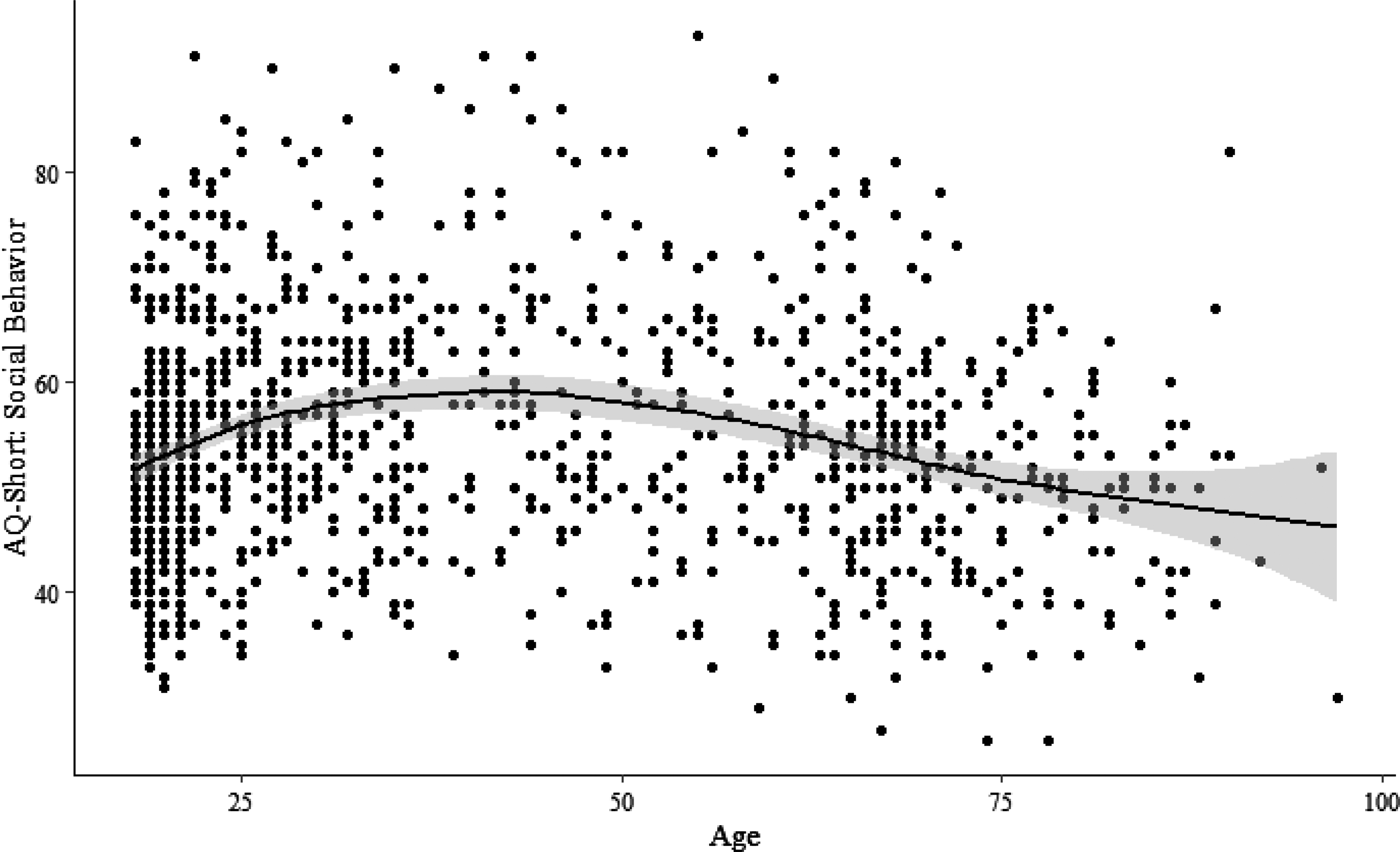
AQ-Short subscale of social interaction by age. The line shows mean at each age with the shaded area representing the 95% confidence interval of the estimate. AQ, Autism-Spectrum Quotient Scale.
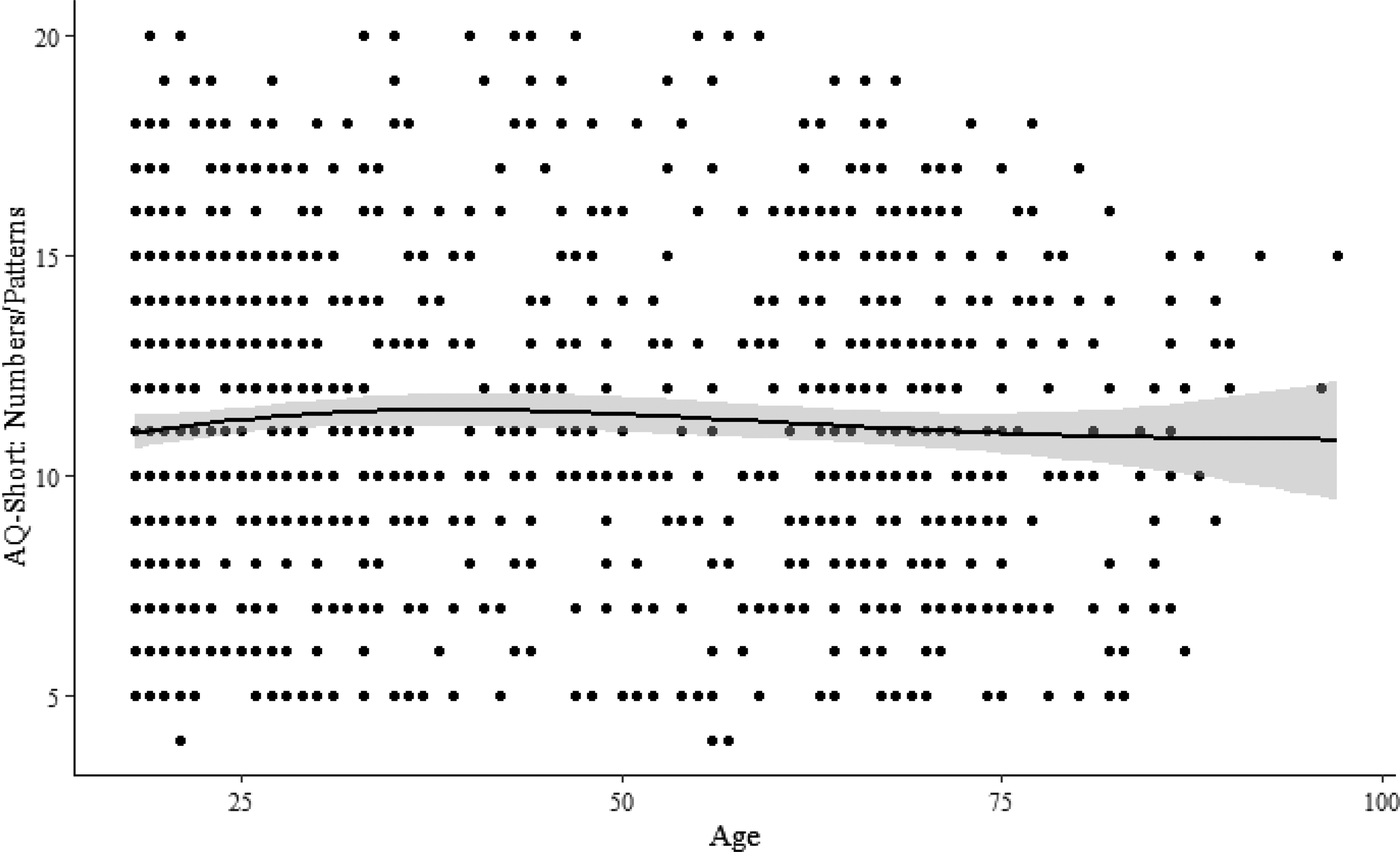
AQ-Short subscale of numbers/patterns by age. The line shows mean at each age with the shaded area representing the 95% confidence interval of the estimate.
Exploratory analyses also tested the impact of potential moderators on the relationship between age and AQ-Short scores. Table 4 provides the correlations between age and AQ-Short scores within each of the following groups: gender, race, individuals who self-identify as having an autism diagnosis, and individuals who self-reported elevated autism characteristics. As indicated by the z-score comparisons of the age-AQ correlations within groups, AQ-Short scores do not vary by these variables.
Correlation Between Age and Autism-Spectrum Quotient Scale-Short by Gender, Race, Self-Reported Diagnostic Status, and Autism-Spectrum Quotient Scale Elevation
Note: ASD+/− indicates whether (+) or not (−) a participant self-reported having an autism diagnosis. AQ+/− indicates whether a participant scored a 26 or higher (+) or below 26 (−) on the AQ-50 using count scoring.
Discussion
The present study examines the relationship of the AQ with age in 1139 adults ages 18–97 years. Results indicate that self-reports of autism characteristics using a variety of distinct approaches to scoring the AQ do not appear to be highly age graded in this large age-representative sample but, instead, appear to vary consistently across age with some indication that AQ scores may be highest in late young adulthood in this sample. The lack of relationship between age and AQ scores is consistent with some prior work in nonautistic subsamples,15,16 but in contrast to other findings indicating a J-shaped relationship between age and AQ-10 scores, where scores were highest in late life. 17
It is critical to note that finding that age is relatively unrelated to AQ scores does not mean that age is unimportant to understanding autism or that we should not examine autism in adulthood. Instead, the results should give added confidence to researchers who want to study autism characteristics throughout the life span. The use of self-report tools such as the AQ-Short can be a central part of building the growing field of understanding autism in adulthood, particularly given the challenges created by the historic focus on autism in childhood. Without a history of confirmed diagnoses or validated tools for diagnosis particularly for those in late life, continuous self-report measures of autism characteristics provide an effective and efficient way of assessing both elevated and subclinical autism characteristics.
The finding of measurement invariance and reliability across age can help researchers investigate age-related questions with a degree of confidence in the consistency of the AQ-Short across a wide range of adults. In general, both multiple groups and local SEM approaches to measurement invariance, as well as reliability analyses, indicate that the AQ-Short 39 may be a useful research tool through adulthood and into late life. As researchers move forward in understanding autism in adulthood, they should whenever possible, conduct tests of measurement invariance and reliability to ensure that the present findings replicate in other samples. Many past studies had the potential to test the relationship between AQ and age and test for measurement invariance of the AQ across multiple demographic variables. Making this a common practice will go a long way to advancing the knowledge about autism in adulthood. Further work should also investigate other psychometric properties of the AQ and other measures of autism characteristics across age such as test/retest reliability and further identification of the nomological net of autism characteristics.
In conducting these tests in future research, it is important to note that the fit of the AQ-Short continues to be at just acceptable thresholds and there was some degradation in fit by chi-square metrics when constraining parameters for measurement invariance. However, given the sample size, lack of change in CFI and RMSEA when setting measurement invariance restrictions, known lower CFI when items may not be highly correlated such as is the case for the two-factor model of the AQ-Short, and the consistency of parameter estimates across groups at each level of invariance, we can reasonably begin to conclude that the AQ-Short is a consistent measure across age. 56 In interpreting local SEM findings, lower sample size at the age margins of the sample may limit the conclusions that can be drawn from either end of the age range, and so, further work is needed to confirm findings in emerging adults and the oldest old.
Researchers are encouraged to not just replicate but extend the analyses reported here as findings may vary across samples, cultures, the diagnostic status of participants, and other self-report measures of autism characteristics. In prior work, the AQ-Short demonstrated configural and metric invariance, but not scalar invariance when comparing between ASD diagnostic status. 40 This suggests that “the AQ-S can be used to investigate possible causes and consequences of autistic traits in both groups separately, but caution is due when combining or comparing levels of autistic traits across the two groups” (p. 55). Given sample size limitations, we were not able to test age invariance of the AQ-Short within the group who reported ASD diagnoses.
Moderation analyses of the relationship of the AQ-Short with age did not suggest that the relationship of autism characteristics with age varies by self-report diagnostic status. Gender, race, and degree of autism characteristics also did not moderate this relationship. This suggests that the lack of relationship between the AQ-Short and age is consistent across the moderator variables in this sample. This is in contrast to two prior studies that show a relationship between age and AQ scores in autistic individuals, but not in nonautistic individuals.15,16 As these two studies had conflicting results, with one finding a positive relationship and one finding a negative relationship between age and AQ scores, further work replicating these findings in more demographically diverse samples and in clinician-confirmed autistic participants will be crucial as will identifying additional potential moderators of the relationship between age and autism characteristics.
This need for future work is likely particularly important for the older adult sample who had a very low rate of self-identified autism in this study. While the present sample is unique in its age representativeness, given they are part of the “lost generation” cohort, 7 extra caution should be taken in interpreting the present findings and extra effort should be given to extending this work in the hard-to-reach sample of autistic older adults in future research. In encouraging researchers to move forward with using the AQ-Short across adulthood, it is essential to highlight limitations of the present work and the existing literature on autism characteristics and age in general. In general, while the present research is one of the first to study autism characteristics in a large age-representative sample, it remains skewed toward more young adult participants. Future work with larger midlife and older adult samples is critical to replicating and extending our current understanding of autism characteristics across the life span.
Importantly, all of the published work to date is cross-sectional. While cross-sectional data can provide valuable insights into the age-graded nature of a variable or the measurement consistency of a variable, they cannot provide information on the development of a variable. Developmental research would provide important information on the extent to which autism characteristics demonstrate rank-order stability or mean-level change over time. Longitudinal research could also investigate the mechanisms associated with developmental patterns such as the impact clinical interventions, social engagement, or distinct life events may have on the changes in autism characteristics across the life span. Relatedly, autism characteristics could show both state- and trait-like characteristics if future research assessed autism characteristics using momentary assessment experience sampling methodologies. Finally, longitudinal research must also investigate the extent to which developmental patterns in autism characteristics may influence age-related changes and vice versa. For example, it is possible given cross-sectional evidence that autism characteristics may put individuals at heightened risk for poor trajectories of aging and, at the same time, that normative age-related changes, particularly role changes and cognitive decline, may increase the expression and impact of autism characteristics over time. However, only longitudinal research on autism characteristics can begin to answer these questions.
In interpreting the present findings and in moving forward with studies of autism and adulthood, researchers must be cognizant of the limitations of selection bias in general and survival bias in particular. Participants in any research must be able to engage with the tools of the research, limiting the generalizability of this research to individuals without cognitive or language limitations (a substantial portion of autistic individuals in the overall population). As with all self-report research within the context of autism, findings are limited to those individuals who can respond to questions about their autism characteristics. 57 Furthermore, participants must be willing to engage with research, and researchers must attend to important factors for recruiting and retaining participants on the autism spectrum. 58 Likewise, as with any studies including a broad age range of individuals, the oldest old are often uniquely healthy and engaged individuals. Given the additionally high mortality rates of individuals on the autism spectrum relative to the general population and the history of autism diagnosis and support, even more selection bias may be at play in older autistic samples or older individuals who self-report elevated autism characteristics.25–27
Finally, while the AQ has support from prior research on its sensitivity and specificity in relation to autism diagnoses, research still needs to evaluate this in the context of aging research.42,43 This limits the generalizability of the current results to autism characteristics in the general population and may not reflect aging in autistic individuals identified in younger generations.
The present research represents one of the first steps to understanding autism characteristics across adulthood. However, given the historical lack of awareness of the diagnosis and continued lack of available validated tools for diagnosis in older adults, readers must interpret findings from the present research in the context of autism characteristics and should not generalize to diagnosed individuals. Future work must continue to expand our understanding of autism and autism characteristics across diverse life span samples.
Footnotes
Authorship Confirmation Statement
J.L.-S., J.D.R., V.M.L., S.K., and C.J.L. prepared the primary drafts of the preregistration and article. J.L.-S., J.D.R., and V.M.L. conducted the analyses. K.F.K., J.P.D., C.L., and M.L.T. provided substantial input into the study design, preregistration, subsequent drafts, and final article. All authors reviewed and approved the final preregistration and submission.
Acknowledgments
The authors thank Bill Chopik, Brigit Reilly, Ted Schwaba, and Seth Spain for their input on the preparation of this article and Mary Ann Langlois for her substantial support of this program of research. The authors also thank the participants of the studies included here and the community partners for their sustained engagement in the growing understanding of autism in adulthood. The preregistration for this project is available at https://osf.io/ncbgj. The data, code, and output for this article are available at ![]() .
.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This article was prepared with support from a National Institutes of Aging at the National Institutes of Health grant (No. 1R21AG059051-01).