
Abstract
Background:
Autistic people with co-occurring attention deficit/hyperactivity disorder (ADHD) appear to be at heightened risk of suicide. To understand why, we explored two explanatory mechanisms from the interpersonal theory of suicide: first, that co-occurring ADHD might be associated with greater risk through greater thwarted belongingness and perceived burdensomeness and, secondly, that hyperactive/impulsive features might incur additional risk through their association with painful and provocative events, which are suggested to create “capability” for suicide.
Methods:
Autistic adults (n = 314) completed an online survey including measures of thwarted belongingness, perceived burdensomeness, painful and provocative events, acquired capability for suicide, and ADHD features. Creating an overall index of likely ADHD, we examined associations between likely ADHD, suicide ideation, and lifetime suicide attempts through the parallel mediators of thwarted belongingness, perceived burdensomeness, anxiety, and depression. In several models, we then examined hyperactive, impulsive, and inattentive features as predictors of exposure to painful and provocative events and subsequent capability for suicide, and examined whether these two variables, sequentially or individually, mediated an association with lifetime suicide attempts.
Results:
Likely ADHD was associated with past-year suicide ideation through greater depression and perceived burdensomeness, which also mediated its association with more suicide attempts. Hyperactive and impulsive features were associated with exposure to painful and provocative events and through this acquired suicide capability. Both features were associated with more numerous suicide attempts through these two mediators sequentially, and through exposure to painful and provocative events alone.
Conclusions:
These data suggest that suicidality in autistic people with ADHD may be partially related to perceived burdensomeness and to acquired suicide capability after exposure to painful and provocative events. However, as we observed a pathway to suicidality associated with painful and provocative events alone, it is likely that there are also other explanatory mechanisms for the influence of traumatic events on suicide risk.
Community brief
Why is this an important issue?
Suicide is a leading cause of premature death in autistic people, but we still know little about why autistic people are at greater risk and how we can help. Recent findings suggest that autistic people with co-occurring attention deficit/hyperactivity disorder (ADHD) are at even higher risk, but we do not yet understand why.
What was the purpose of this study?
This research examined two potential explanations for higher risk of suicide in autistic people with co-occurring ADHD. First, we expected that because these individuals are often very isolated and struggle with independence and employment, they might be more vulnerable to two risk factors for suicide: “thwarted belongingness,” the feeling of being alienated from other people, and “perceived burdensomeness,” the feeling that one is a burden to others. We also expected that hyperactive/impulsive features associated with ADHD might make people more likely to experience painful and dangerous events. Exposure to events like this is suggested to make people less frightened of dying by suicide and more able to attempt to end their lives. This is called “acquiring capability” for suicide.
What did the researchers do?
We asked 314 autistic adults to complete an online survey including measures of thwarted belongingness, perceived burdensomeness, exposure to painful and dangerous events, and acquired capability for suicide. They also completed a scale measuring ADHD features, and symptoms of depression and anxiety. We then looked at which of these factors, if any, explained suicide risk in autistic people with co-occurring ADHD.
What were the results of the study?
Our data suggest that autistic people with co-occurring ADHD might be at greater risk of suicide ideation and attempts because they are more likely to experience depression and to feel like a burden to others. We also found that people with high degrees of hyperactive/impulsive features were more likely to experience painful and dangerous events, and, therefore, had greater capability for suicide—because of this, they were more likely to have attempted suicide more times in the past. Exposure to these kinds of traumatic events also increased the risk of suicide all by itself.
What do these findings add to what was already known?
Very little is known about why autistic people with co-occurring ADHD might be at even higher risk of suicide than people with either ADHD or autism alone. No studies have examined explanations for suicide in this subgroup.
What are potential weaknesses in the study?
Because this study looked at a snapshot of participants' current states, we cannot be sure of the direction of relationships between variables. For example, it might be that experiences of surviving suicide attempts actually make people feel more depressed and more like a burden afterward, rather than these feelings being the risk factors that contributed to suicide attempts.
How will these findings help autistic adults now or in the future?
These findings indicate feelings and experiences that are relevant to suicide risk in autistic people with co-occurring ADHD, which might thus be important to target in interventions.
Introduction
Suicide is a leading cause of premature mortality in autistic people without intellectual disability, with suicide attempts and deaths considerably higher than those seen in the general population.1–5 One group who appear at particular risk within this demographic are autistic people with co-occurring attention deficit/hyperactivity disorder (ADHD), which has a lifetime prevalence of 40.2% in autistic samples. 6 ADHD is considered by many to be a neurological “cousin” of autism, 7 a developmental condition with shared genetic heritability8,9 and an overlapping neurological profile. 10
Despite some shared features that may challenge differential diagnosis, 11 ADHD possesses its own distinctive behavioral and neurological features that distinguish it from autism, and the appearance of ADHD and autistic features within an individual shows that the two can co-occur.10,12
One study estimated the risk of suicide attempts in these individuals as threefold higher than the fourfold increase already seen within the autistic community 13 ; in the same cohort, suicide deaths were increased fivefold on top of the eightfold increase seen in individuals with autism alone. With similar findings corroborated in ADHD samples, 14 this heightened risk in autistic people with ADHD is importantly independent of psychiatric conditions such as anxiety, depression, and substance abuse, 13 which are also more common in this cohort15,16 and a major correlate and risk factor for suicidality, in and of themselves, in both autistic and ADHD populations.2,17,18
Similarly, a number of studies report an association between ADHD and suicidality14,19–21 that is separate from these confounds and seemingly reflects something about living in the world as an ADHD individual. 22 These concerning findings highlight the need to examine the role of co-occurring ADHD in autistic suicidality and to identify the mechanisms through which these individuals might be at greater risk.
Recent efforts to comprehend suicidality in autistic people have drawn on theoretical frameworks in an attempt to integrate and explain seemingly disparate risk factors. To date, the dominant paradigm in suicidology is the Interpersonal Theory of Suicide (ITS),23–25 which holds that suicide ideation and suicide attempts are distinct phenomena dependent on specific proximal risk factors. The theory suggests that the desire to die by suicide arises from the confluence of “thwarted belongingness” (a state of loneliness and the absence of reciprocal caring relationships) and “perceived burdensomeness” (feelings of self-hate and worthlessness, beliefs that one is a liability to others).
The ITS holds that suicide attempts and deaths occur in people in whom suicide ideation converges with the capability to enact lethal self-injury. Such capability can be “acquired” through exposure to physically painful and emotionally provocative or triggering experiences. Although events of this nature include exposure to traumatic events (e.g., violent victimization, accidents, and combat experience), engagement in nonsuicidal self-injury (NSSI), or intravenous drug use, they also include a range of behaviors associated with thrill seeking or extreme sports (e.g., skydiving, rock climbing, getting a tattoo, and riding a motorbike): essentially, experiences in which individuals are exposed to pain and fear of pain and death, and can become habituated to the same.26,27
The explanatory power of the ITS lies partly in its recognition of overarching psychological constructs that incorporate individual correlates of suicidality (e.g., unemployment and family conflict), with life events and experiences. Many varied factors associated with suicidality in autistic people—for instance, loneliness and unmet support needs,17,28,29 camouflaging, 17 low self-worth, 30 and NSSI17,31—may, if the theory is applicable in this group, be understood in terms of a small number of shared psychological constructs.
Recent investigations support the relevance of thwarted belongingness, perceived burdensomeness, and acquired capability to suicidality in autistic people,32,33 although they suggest that factors traditionally associated with suicidal ideation in the ITS might also contribute to suicide attempts in autistic people. Perceived burdensomeness appeared to be a particularly potent predictor of both outcomes, and mediated the higher rates of suicide ideation seen in autistic people who were single. 33 In the same vein, in the general population, perceived burdensomeness and thwarted belongingness mediated the association between camouflaging autistic traits and suicidality. 34
In considering suicide risk associated with ADHD through the lens of the ITS, it may be significant that nonautistic people with ADHD struggle with loneliness, low self-worth, feelings of inferiority and difference from others, and may engage in camouflaging as they “strive to be normal.”35–39 They are more likely to experience academic underachievement and/or exclusion, unemployment, difficulty sustaining employment, and to find themselves in financial arrears or dependent on family. 40 Financial distress, which is suggested by the ITS as a likely antecedent of perceived burdensomeness, 24 has actually been linked to psychological distress and suicide in this population. 19
Although little research has explored ITS constructs as predictors of suicidality in ADHD, recent studies in the general population have indeed suggested a mediating role for perceived burdensomeness and thwarted belongingness in the association between ADHD traits and suicide ideation. 41 With both states (particularly perceived burdensomeness) associated with suicidality in autistic people,32,33 it is possible that the higher risk of suicide ideation in autistic people with ADHD might also be mediated by greater likelihood of experiencing these states.
As children and adolescents, these individuals tend to score more poorly than young people with either condition alone on standardized measures of adaptive and executive function, experience more mental health conditions, and struggle more with the social and academic pressures of school.16,42–45 There are few studies examining the welfare of autistic adults with co-occurring ADHD, but those that exist suggest that with greater degrees of ADHD features, autistic people rate their quality of life as poorer (including in relation to physical and mental health) and may be more isolated, with lower likelihood of employment and independence.46,47
Although we might hypothesize that high states of thwarted belongingness and perceived burdensomeness, if present, would be associated with a strong desire for death, two additional mechanisms may be relevant in explaining the high rates of suicide attempts and deaths in autistic people with ADHD. First, there is some suggestion that mental rehearsal of suicide plans, a behavior associated with suicide ideation and subsequent attempts, is a unique facet of the acquired capability construct that both reinforces suicide ideation and contributes to the erosion of fear of death. 48
In this way, prolonged periods of intense suicide ideation with mental rehearsal of suicide plans, which are suggested by heightened rates of suicide ideation in neurodivergent people,4,49–51 may habituate individuals to the thought of suicide and actually enable them to act on suicidal thoughts. Second, an additional pathway to suicidality in ADHD is indicated by one of its core feature domains,* that of hyperactive/impulsive features.
Although trait impulsivity is not a reliable predictor of suicide attempts, 52 impulsivity is considered an indirect and distal risk factor because it increases the likelihood that an individual will be drawn and/or exposed to the painful and provocative events that increase suicide capability.53,54 Unfortunately, although a number of studies report associations between ADHD and suicidality,19,21,55 NSSI, 56 and violent and traumatic events,57–59 few examined these associations in relation to specific features.
Several studies implicate hyperactive/impulsive features in self-injurious behavior,60,61 but neither examined the specificity of this association to hyperactive/impulsive features or looked at subsequent effects on acquired capability and later suicidality. Although one study did support a link between ADHD and suicidality in relation to victimization trauma, 62 these authors did not examine whether acquired capability mediated an association between exposure to this type of provocative event and suicide attempts, or consider differential effects of ADHD features.
In light of the apparent greater risk of suicidality suggested in autistic people with ADHD,13,14 this study aimed to examine associations between co-occurring ADHD, suicide ideation, and suicide attempts in light of two hypothesized pathways based on the ITS and previous autism literature. Our first analyses focused on thwarted belongingness and perceived burdensomeness, which we hypothesized might occur at higher levels in autistic people with ADHD due to the deleterious academic, occupational, social, and emotional correlates of co-occurring autism and ADHD.46,63,64
In the general public, the association between these constructs and ADHD features mediated their association with suicide ideation, 41 consistent with the assertions of the ITS. We hypothesized a similar mediating role of these constructs between co-occurring ADHD and suicide ideation in our autistic sample, but given that thwarted belongingness and perceived burdensomeness may be relevant to suicide attempts in autistic people, 32 we also examined their role in the association between co-occurring ADHD and suicide attempts.
Our second analyses focused on acquired capability, which is understood to accrue from exposure to painful and provocative events. 26 We hypothesized that hyperactive/impulsive features, in particular, would be associated with higher incidence of painful and provocative events and henceforth greater acquired capability for suicide, and that these two variables would mediate an association between this specific feature domain and suicide attempts.
Methods
Participants
These analyses were performed using data from the same autistic sample (n = 314) described in Moseley et al. 33 These volunteers responded to online advertisements on social media and to adverts distributed to the Autistica Research Network and the Cambridge Research Database. The majority (95.8%) lived in the United Kingdom, with 1.3% living in the United States and the remainder within South America and the European Union. Fifty-four of the sample (11 of those who reported their sex as male, 43 who reported their sex as female) had been formally diagnosed as having ADHD (unfortunately, we did not enquire when these diagnoses were made). Further demographic information about the sample is displayed in Table 1, along with their scores to major study variables.
Sample Demographic Information and Scores in Major Study Variables
Note: Demographic information and average sample scores on scales used in this analysis. ADHD variables are derived from the CAARS-S:S; thwarted belongingness and perceived burdensomeness from the INQ-15; acquired capability from the ACWRSS; painful and provocative events from the PPES; and depression and anxiety from the PHQ-9 and GAD-7, respectively. Internal consistency is provided for those scales assessing reflective constructs (whose items indicate one or more latent variables).
ACWRSS, Acquired Capability with Rehearsal for Suicide Scale; ADHD, attention deficit/hyperactivity disorder; CAARS-S:S, Connors Adult ADHD Rating Scale self-report short version; GAD-7, generalized anxiety disorder-7; GCSEs, General Certificate of Secondary Education; INQ-15, Interpersonal Needs Questionnaire-15; PHQ-9, Patient Health Questionnaire-9; PPES, Painful and Provocative Events Scale; SD, standard deviation.
Materials and procedure
The science and technology faculty ethics panel at Bournemouth University reviewed and approved this study; measures taken for the safety and comfort of participants are listed in full in a previous publication. 33 Participants completed an online survey (hosted on Qualtrics) that included measures of co-occurring ADHD, ITS constructs, suicide ideation, and attempts, along with depressive and anxious symptoms. Internal consistency was high for each measure in this sample (Table 1).
Independent variables: co-occurring ADHD and feature domains
As it has only recently become possible for individuals to be diagnosed with both autism and ADHD and women are particularly under-recognised,12,65 we deemed it highly likely that more participants might exhibit ADHD features than just those who had received official ADHD diagnoses. The Connors Adult ADHD Rating Scale self-report short version (CAARS-S:S 66 ) includes 26 items that correspond to subscales inattention/memory problems, hyperactivity/restlessness, impulsivity/emotional lability, and problems with self-concept.
We transformed these raw scores for each subscale into t-scores for comparison with standardized age-appropriate norms for males and females, and used the t-scores for inattention/memory, hyperactivity/restlessness, and impulsivity/emotional lability as continuous measures in our analysis.
An additional subscale of the CAARS-S:S, the ADHD index, constitutes 12 items that are most strongly indicative of likely ADHD. In the general population, t-scores of 70 in the ADHD index are highly indicative of likely ADHD. Standardized scores do not, to our knowledge, exist for autistic adults, but in our sample, 142 participants (45.2%) scored above 70 on the ADHD index (108 females and 34 males, a subset that included the 54 participants with official ADHD diagnoses). Using this, we created a binary index indicative of likely ADHD (participants coded 1 if their ADHD index t-score was 70 or above).
Mediators: ITS constructs
The Interpersonal Needs Questionnaire-15
The Interpersonal Needs Questionnaire-15 (INQ-15) 67 includes nine statements related to thwarted belongingness and six to perceived burdensomeness. Participants responded to items on a scale from 1 to 7, with higher scores indicating greater thwarted belongingness and perceived burdensomeness.
The Acquired Capability with Rehearsal for Suicide Scale
The Acquired Capability with Rehearsal for Suicide Scale (ACWRSS) 48 is a brief 7-item measure wherein higher scores reflect greater acquired capability. Although the scale comprises items assessing fear of death, pain tolerance, and mental rehearsal, only the total score was used here.
Painful and Provocative Events Scale
The 26-item version of the Painful and Provocative Events Scale (PPES) 26 includes a list of experiences (e.g., “have you gone skydiving” and “did you get a tattoo?”). Participants responded to each item with “never” (scored 1), “once” (2), “2–3 times” (3), “4–20 times” (4), or “more than 20 times” (5).
Dependent variables: suicide ideation and attempts
We created a continuous composite item reflecting the frequency and intensity of suicide ideation over the past 12 months, based on the sum of scores to two correlated items (r = 0.55, p < 0.001) in the Self-Injurious Thoughts and Behaviours Interview short form (SITBI 68 ). More details were originally reported in Moseley et al. 33 The composite score ranged between 0 (no suicide ideation within the past year) and an integer between 2 and 12: low scores reflected rare or brief incidents of suicide ideation, whereas higher scores indicated the presence of suicide ideation that was frequent and/or intense.
For an ordinal index of lifetime suicide attempts, we used the SITBI item, “How many times in your lifetime have you made an actual attempt to kill yourself, in which you had at least some intent to die?” Participants could respond with “never” (scored 0), “once” (1), “twice” (2), “three or four times” (3), or “five or more times” (4). Frequency of participant responses to the two SITBI items, the suicide ideation composite, and number of lifetime suicide attempts are shown in Figure 1.
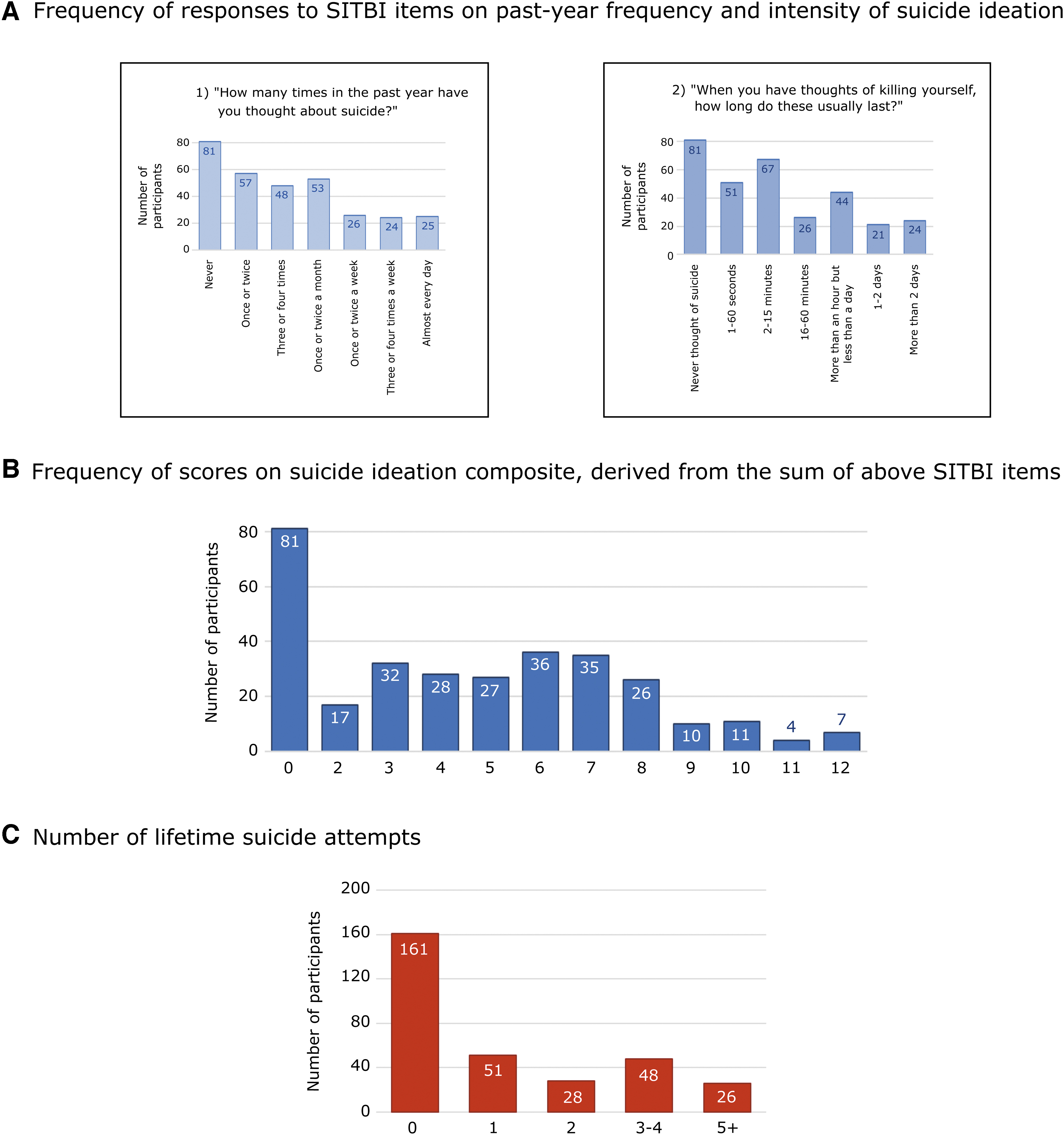
Past-year suicide ideation and lifetime suicide attempts in the sample. Note: Figure reproduced with permission from Moseley et al.
33
Part
Covariates and additional mediators: depressive and anxious symptoms
As additional variables relevant to suicidality, we included depression and anxiety as covariates and extra mediators in our analyses. These were measured with the Patient Health Questionnaire-9 69 and the generalized anxiety disorder-7 70 , respectively.
Analysis
First, we examined the data for each variable and outcome measure for outliers, normality, autocorrelations, and homoscedasticity, and normal distribution of residuals. We then performed mediation analyses using PROCESS for SPSS (version 3), 71 a macro based on ordinary least squares regression with bootstrapping (5000 samples). In each instance, we set confidence intervals (CIs) at 95%, and controlled for age and sex as covariates.
Data were standardized for all analyses with PROCESS, though CIs are generated in unstandardized form; as such, we present both standardized and unstandardized coefficients for each model. Our first set of analyses focused on thwarted belongingness and perceived burdensomeness. We used our binary measure of likely ADHD in two mediation analyses (adjusting alpha levels, p = 0.025): in these, we examined indirect effects of this binary predictor on past-year suicide ideation and then lifetime suicide attempts.
Thwarted belongingness, perceived burdensomeness, depression, and anxiety were included as parallel mediators in this model (Model 4 in PROCESS). Indirect effects and their CIs are presented in unstandardized and in partially standardized form (full standardization is not possible or indeed recommended for dichotomous predictors). 71
Our second set of analyses, focusing on pathways to acquired capability through painful and provocative events, used the sequential mediation model (Model 6). Controlling for all the variables in the previous analyses (anxiety, depression, thwarted belongingness, and perceived burdensomeness) in addition to age and sex, we examined distinct pathways between ADHD feature domains and lifetime suicide attempts through exposure to painful and provocative events (first mediator) and then acquired capability total score (second mediator).
We hypothesized that this pathway would be specific for hyperactivity/restlessness and impulsivity/emotional lability (henceforth hyperactivity and impulsivity) features, but to confirm this specificity, the analysis was also performed for the inattention/memory domain (henceforth inattention). Alpha levels for these three analyses were corrected to p = 0.017. Indirect effects and their CIs are presented in unstandardized and standardized form, along with the upsilon statistic as a reflection of effect size. 72
Results
Co-occurring ADHD, thwarted belongingness, and perceived burdensomeness
Our binary index of likely ADHD was associated with greater anxiety (b = 4.60 [β = 0.78], p < 0.001, CI: 3.38 to 5.82), depression (b = 5.47 [β = 0.76], p < 0.001, CI: 3.98 to 6.96), and perceived burdensomeness (b = 4.58 [β = 0.48], p < 0.001, CI: 2.50 to 6.30), though not thwarted belongingness (b = 1.37 [β = 0.15], p = 0.1920, CI: −0.69 to 3.43). Perceived burdensomeness (b = 0.13 [β = 0.37], p < 0.001, CI: 0.09 to 0.17), depression (b = 0.19 [β = 0.41], p < 0.001, CI: 0.13 to 0.25), and sex (with being female associated with greater likelihood of suicide ideation: b = −0.82 [β = −0.11], p = 0.0128, CI: −1.47 to −0.18) all contributed to the model for past-year suicide ideation (R 2 = 0.46, F [7, 306] = 37.71, p < 0.001), though anxiety (b = −0.04 [β = −0.06], p = 0.3011, CI: −0.11 to 0.03) and thwarted belongingness (b = 0.01 [β = 0.03], p = 0.5302, CI: −0.02 to 0.04) did not.
Likely ADHD did not directly predict greater suicide ideation (b = 0.15 [β = 0.04], p = 0.6399, CI: −0.47 to 0.76), but a significant total effect (b = 1.62 [β = 0.48], p < 0.001, CI: 0.89 to 2.35) reflected that mediation was occurring. In this way, likely ADHD was associated with suicide ideation through greater depression (unstandardized effect b = 1.04 [bootSE = 0.24], bootstrapped CI: 0.60 to 1.54; when partially standardized, b = 0.31 [bootSE = 0.07], bootstrapped CI: 0.18 to 0.45) and stronger feelings of burdensomeness (unstandardized effect b = 0.60 [bootSE = 0.17], bootstrapped CI: 0.29 to 0.95; when partially standardized, b = 0.18 [bootSE = 0.05], bootstrapped CI: 0.09 to 0.28). Relationships between variables (unstandardized) are depicted in Figure 2, part A.
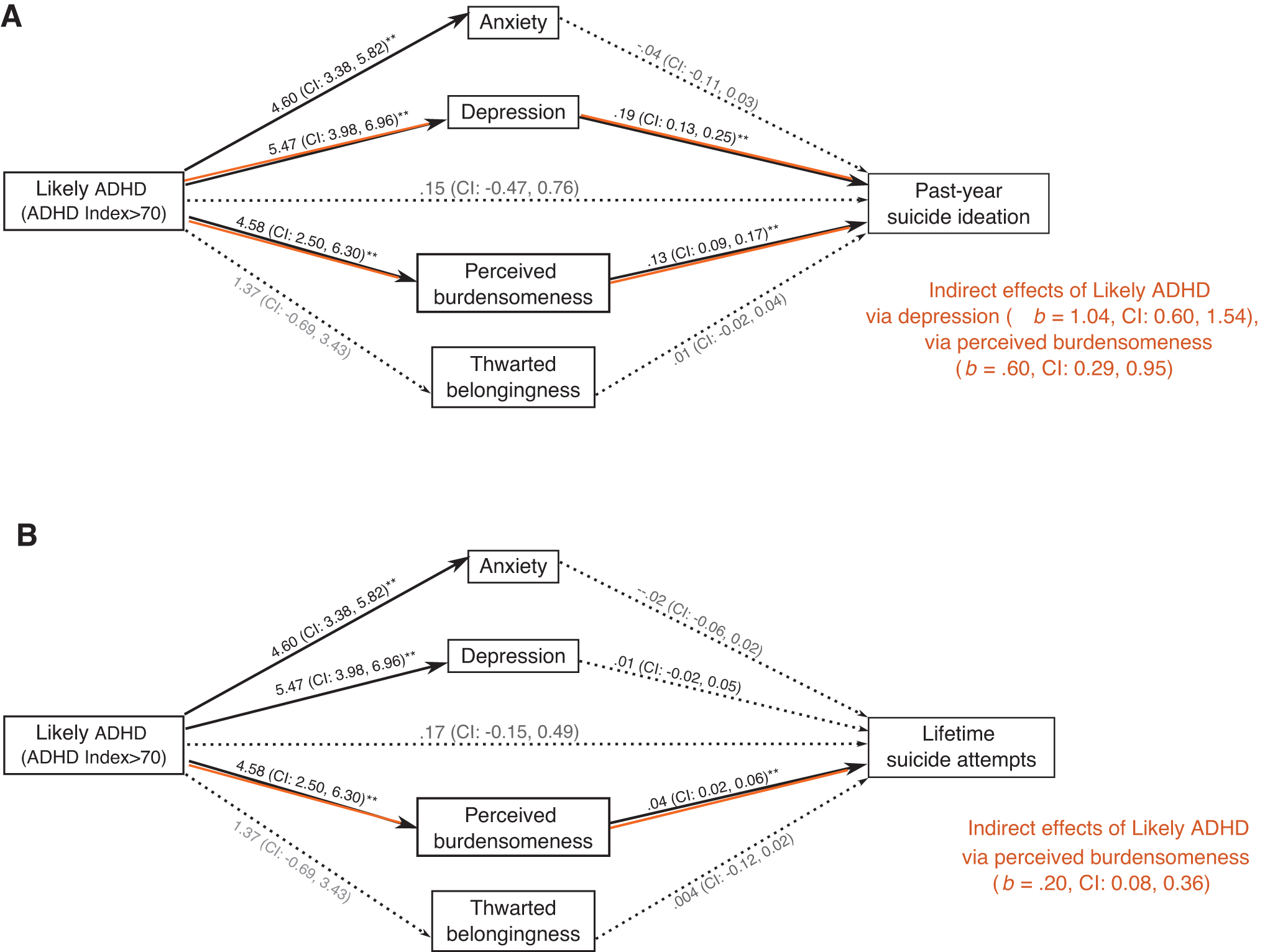
Associations between co-occurring ADHD, thwarted belongingness, burdensomeness, and suicidality. Note: Part
Only perceived burdensomeness (b = 0.04 [β = 0.31], p < 0.001, CI: 0.02 to 0.06) and female sex (b = −0.50 [β = −0.16], p = 0.0041, CI: −0.84 to −0.16) were directly predictive of lifetime suicide attempts (R 2 = 0.15, F [7, 296] = 7.44, p < 0.001), when this outcome was modeled as the dependent variable.
Although not predicting lifetime suicide attempts directly (b = 0.17 [β = 0.12], p = 0.2988, CI: −0.15 to 0.49), a significant total effect of likely ADHD (b = 0.36 [β = 0.26], p = 0.0206, CI: 0.06 to 0.67) reflected an indirect relationship where likely ADHD was associated with more numerous suicide attempts through its association with greater feelings of burdensomeness (unstandardized effect b = 0.20 [bootSE = 0.07], bootstrapped CI: 0.08 to 0.36; when partially standardized, b = 0.15 [bootSE = 0.05], bootstrapped CI: 0.06 to 0.26) (Fig. 2, part B).
ADHD feature domains, painful and provocative events, and acquired capability
With three analyses, we then examined effects of hyperactivity, impulsivity, and inattention as predictors of painful and provocative events, acquired capability and lifetime suicide attempts sequentially (Fig. 3 depict unstandardized coefficients reflecting relationships between variables). Hyperactivity was significantly associated with painful and provocative events as the first mediator (b = 0.31 [β = 0.34], p < 0.001, CI: 0.21 to 0.42; R2 = 0.23, F [7, 304] = 12.71, p < 0.001). It was not directly associated with acquired capability (b = −0.07 [β = −0.07], p = 0.2596, CI: −0.21 to 0.06), which was predicted by PPES scores (b = 0.42 [β = 0.34], p < 0.001, CI: 0.29 to 0.55; R2 = 0.29, F (8, 303) = 15.20, p < 0.001).
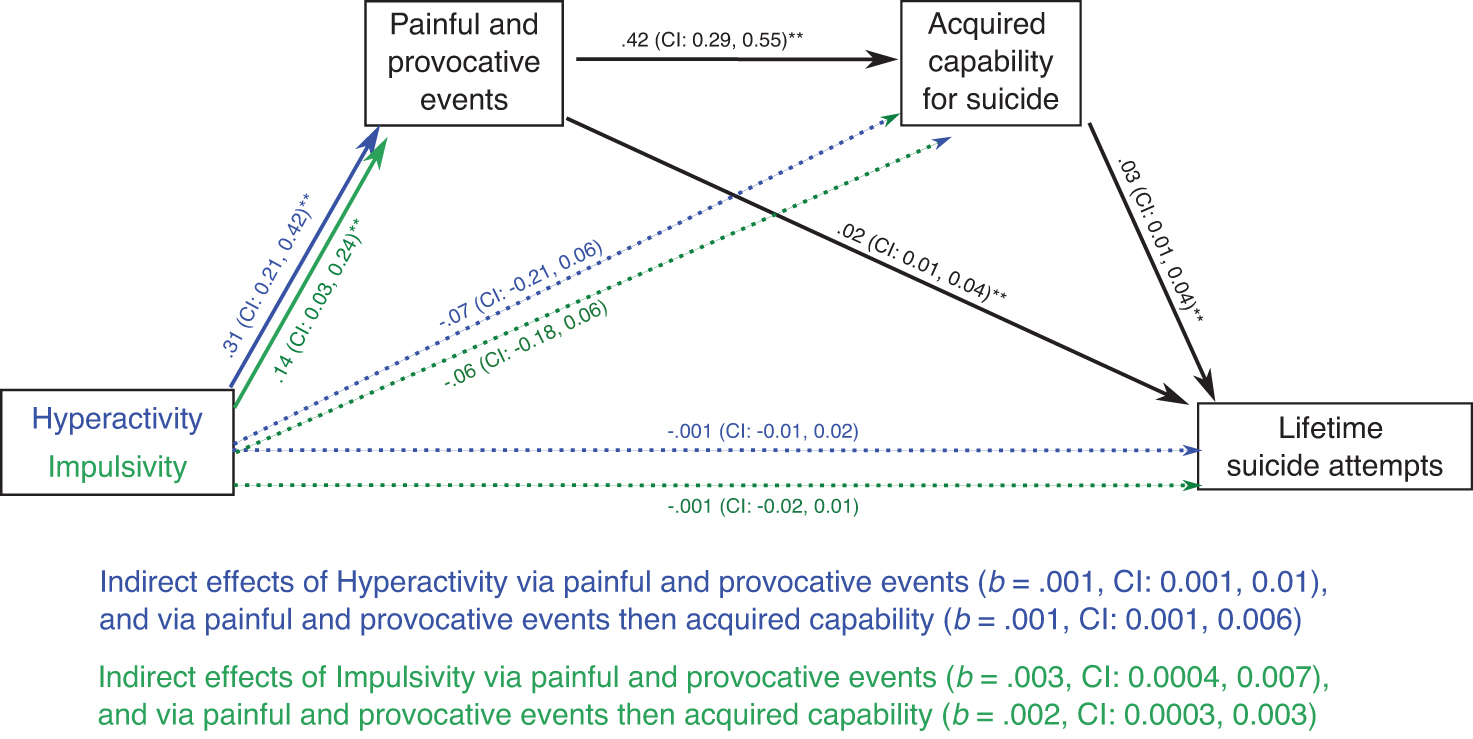
Associations between ADHD feature domains and lifetime suicide attempts. Note: Figure 2 depicts two separate mediation analyses, one with hyperactivity (blue) as the predictor, the other with impulsivity (green) as the predictor. Lines in black reflect relationships between painful and provocative events, acquired capability, and lifetime suicide attempts with coefficients from the hyperactivity analysis. Double asterisks (**) represent unstandardized coefficients significant at p < 0.001. Indirect effects (coefficients and CIs) are unstandardized.
Both PPES scores (b = 0.02 [β = 0.16], p = 0.0087, CI: 0.01 to 0.04) and acquired capability (b = 0.03 [β = 0.26], p < 0.001, CI: 0.01 to 0.04) contributed to the model for lifetime suicide attempts (R 2 = 0.24, F (9, 302) = 10.62, p < 0.001). Hyperactivity did not directly predict lifetime suicide attempts (b = 0.001 [β = 0.001], p = 0.8777, CI: −0.01 to 0.02), but was associated with this outcome through two indirect pathways. First, hyperactivity was associated with increased exposure to painful and provocative events, which in itself predicted more numerous suicide attempts (unstandardized b = 0.001 [bootSE = 0.003], bootstrapped CI: 0.001 to 0.01; standardized β = 0.05 [bootSE = 0.03], bootstrapped CI: 0.01 to 0.11; υ = 0.003).
Second, in a sequential mediation effect, hyperactivity was associated with increased exposure to provocative events, with greater acquired capability, and through these with more numerous suicide attempts (unstandardized b = 0.001 [bootSE = 0.001], bootstrapped CI: 0.001 to 0.006; standardized β = 0.03 [bootSE = 0.01], bootstrapped CI: 0.01 to 0.05; υ = 0.001).
Impulsivity functioned entirely similarly to hyperactivity, being associated with painful and provocative events directly and being indirectly associated with lifetime suicide attempts through the same two indirect pathways (see Supplementary Data for statistical notations and for covariate effects that were not the focus of this analysis). Inattention was not associated with painful and provocative events (b = 0.05 [β = 0.07], p = 0.2287) or acquired capability (b = −0.06 [β = −0.07], p = 0.2107), and was not directly or indirectly associated with lifetime suicide attempts.
Our analyses focusing on relationships between suicidality, co-occurring ADHD, and ADHD feature domains are summarized in Figure 4.
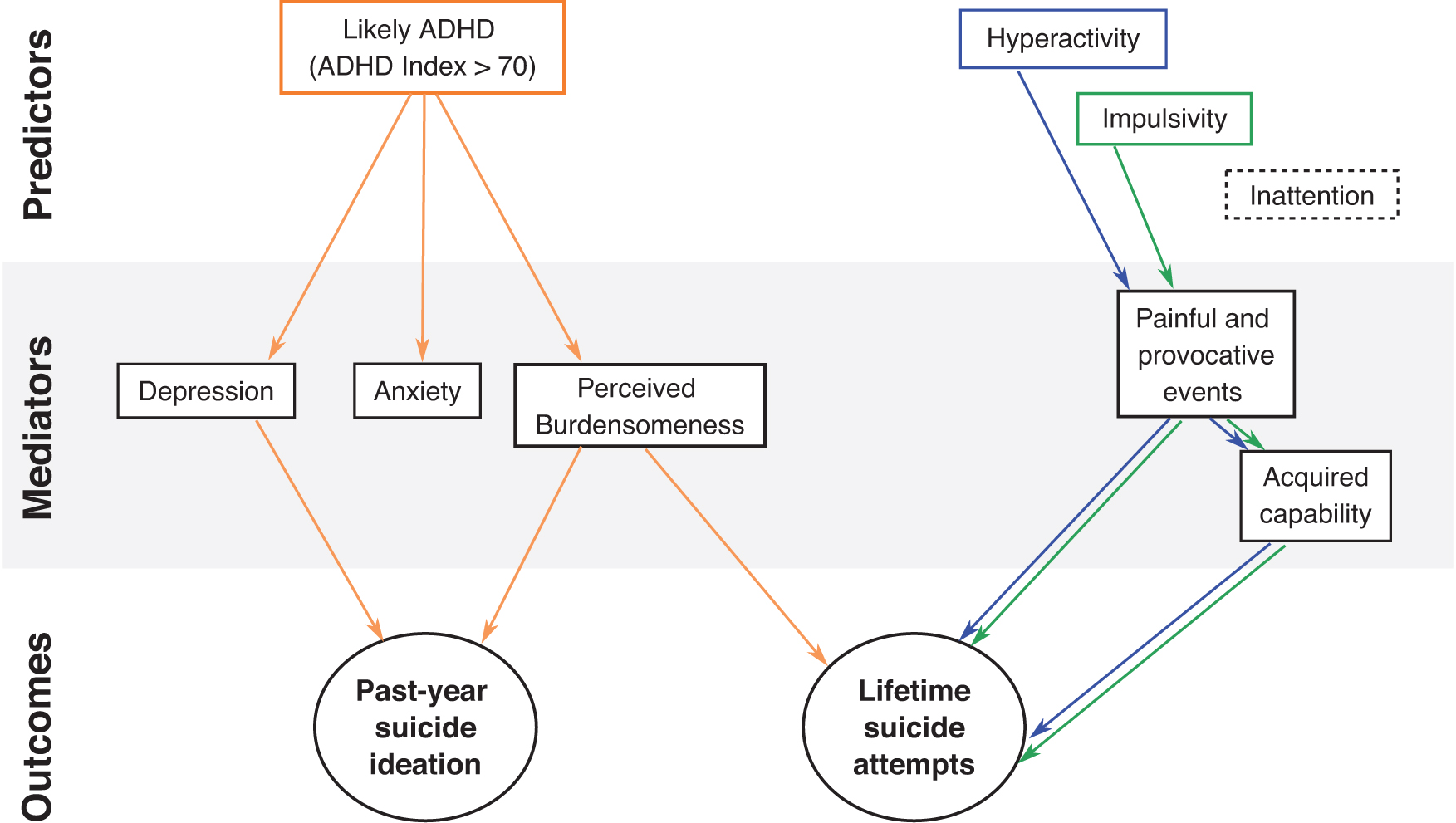
Summarized analyses of relationships between ADHD and suicidality. Note: Relationships between variables are summarized in Figure 3. Likely ADHD was positively associated with suicide ideation through perceived burdensomeness and depression; perceived burdensomeness also connected ADHD co-occurrence to lifetime suicide attempts. Finally, hyperactivity and impulsivity were associated with lifetime suicide attempts through increased exposure to painful and provocative events, and through this exposure and increased capability for suicide.
Discussion
Suicide is devastating for individuals and their families and community. There is a critical need for psychological theory to identify a parsimonious set of explanatory principles with clear implications for prevention and intervention. 73 In line with previous efforts to test the relevance of ITS constructs to autistic suicidality,32,33 this study considered theory-derived hypotheses in relation to the heightened risk observed in autistic people with ADHD.13,14 We primarily hypothesized a mediating role for thwarted belongingness and perceived burdensomeness in associations between likely co-occurring ADHD, suicide ideation, and suicide attempts. Second, we considered an effect of hyperactive/impulsive features on painful and provocative events, acquired capability, and through these, lifetime suicide attempts.
Our first hypothesis was partially supported in so far as our binary index of likely ADHD was associated with greater anxiety, depression, and perceived burdensomeness; it was indirectly associated with greater likelihood of suicide ideation through its effects on depression and perceived burdensomeness, and indirectly associated with more numerous lifetime suicide attempts through perceived burdensomeness. The relationship between likely ADHD, anxiety, depression, and perceived burdensomeness corroborates extant literature purporting poorer mental health, social, and occupational outcomes in autistic people with ADHD.16,46
In relation to suicidality, studies in nonautistic people with ADHD suggested that the deleterious outcomes associated with ADHD might give rise to negative affect, and through this, suicide ideation. 74 A single study in the general population examined this association in relation to the ITS, showing that the association between ADHD traits and suicide ideation was indeed mediated by higher scores in thwarted belongingness and perceived burdensomeness. 41
Although this study supports a mediating role for perceived burdensomeness, the apparent irrelevance of thwarted belongingness stands in contrast to these previous findings and those of Pelton et al., 32 who previously found associations between these constructs and both suicide ideation and attempts. Notedly, as those authors did not control for depression, the effect of thwarted belongingness they observed could have been confounded by depression.
They do note, however, that autistic and nonautistic people differ in the way they interpret a couple of items from the INQ, such that the test may not work entirely similarly in these two groups; furthermore, apparently pathological scores in thwarted belongingness may be sadly less remarkable in autistic people, 75 given their typically smaller social networks. This may explain why thwarted belongingness was not especially associated with suicidality in the sample reflected herein and in Moseley et al., 33 and highlights the importance of developing adapted tools for testing hypotheses around suicidality in neurodivergent groups.
Our second hypothesis concerned with likely ADHD pertained to the association between impulsivity and painful and provocative events,53,54 which are suggested to play an important role in the development of acquired suicide capability. This expectation was borne out, as both hyperactive and impulsive features were associated with acquired capability only through painful and provocative experiences; part of their indirect association with lifetime suicide attempts was realized through this sequential pathway.
Though previous research is scarce in relation to the mechanisms that might underpin an association between ADHD feature domains and suicidality, these findings corroborate the relationship between hyperactive/impulsive features and a range of behaviors and outcomes that might serve to desensitize individuals to pain and fear of death, including NSSI,57–59 abusing substances and other risky behaviors, 76 getting accidentally injured or involved in accidents.77,78
Although we did not predict significant associations between inattentive features and our mediators, it is important to note that these features are, in fact, also associated with risky behavior, accident and injury, and suicide itself in people with ADHD.20,78,79 It is likely that this association is underpinned by different mechanisms, such as difficulties with cognitive control as opposed to sensation seeking. In that that the PPES includes many events that are “actively approached rather than passively experienced” and that these items are associated with sensation seeking, 80 it is possible that hyperactive/impulsive features of ADHD were more likely to correlate with this instrument, despite rates of real-life accidents and injuries associated with inattentive features.
It is possible that the different means through which autistic and nonautistic people with ADHD experience painful and provocative events also bear relevance to the impact of the same on acquired capability for suicide, but this query requires further more extensive investigation.
Interestingly, although hyperactivity and impulsivity were associated with lifetime suicide attempts through painful and provocative events and acquired capability sequentially, they also exerted an indirect effect on lifetime suicide attempts through exposure to painful and provocative events alone. An intriguing parallel with this finding comes from Pelton et al., 32 who observed an indirect effect of lifetime trauma on lifetime suicidality through acquired capability and a direct effect of lifetime trauma on suicidality. The consistency of this association across measurement tools—Pelton et al. 32 used the vulnerability experience quotient, 81 which is validated in autistic people—highlights the significance of this association, the mechanisms of which are still unknown.
In this analysis, depression and anxiety were controlled for as covariates, but exposure to painful and provocative events might plausibly be associated with lifetime suicide attempts through their impact on psychiatric health. Recent studies have examined the apparent elevation of PTSD or complex PTSD in autistic people, finding that post-trauma symptoms are associated with a wider range of events than those traditionally associated with PTSD.82–84 Indeed, autistic and nonautistic authors are increasingly recognizing the damage incurred by aspects of “simply” living in the world as a neurodivergent person, including the chronic stress associated with victimization, social marginalization, and sensory discomfort and/or pain.85,86
Trauma and rumination have indeed been purported as the mediators of relationships between autistic traits and mood disorder in the general population 87 ; the same research group reported an association between lifetime suicidality, depression, and rumination. 88 The autistic community has highlighted research around the impact of stressful and traumatic life events as a priority, 89 and this is corroborated by the association between painful and provocative events and lifetime suicide attempts in our data, over and above effects through acquired capability.
As this finding cannot be clearly understood in light of the ITS, it is important to recognize that this is but one theoretical approach to suicidality, and future studies may benefit from consideration of a wider constellation of dynamic and stable factors.90,91 One alternative, for instance, places greater emphasis on the balance between factors that “push” individuals toward suicide, chiefly pain (psychological and otherwise) and hopelessness, and factors that “pull” or anchor individuals to life, chiefly connections to friends and family, communities, and other valued things, roles, or purposes. 92
This and other approaches provide testable hypotheses that, compared, could shed light on mechanisms underpinning suicidality in autistic people; more broadly, though, this kind of consideration of factors that make life unbearable and their relationship and relative weighting against the factors that make life worth living for autistic people may be of great clinical value. It is however important, as noted by Mitchell et al., 93 to recognize the tendency of such models to focus principally on intrapersonal factors, which could divert attention from the very real damage incurred on the individual by systemic disadvantages and societal prejudices toward neurodivergent people.
In that sense, interventions with such goals of supporting connectedness and reducing feelings of thwarted belongingness and perceived burdensomeness in the individual may be ineffectual without commitment to meaningful change at a societal level.
Limitations and future directions
The primary limitation on conclusions drawn from these data rests on their cross-sectional nature, which disallows directional relationships to be inferred between our variables of interest. Mediation models are by nature suggestive of causality and the hypotheses derived from the ITS likewise assume directional relationships between variables, but cross-sectional designs do not allow us to affirm causal relationships between any of the variables as modeled herein. 94 This is particularly notable in light of the fact that nonfatal suicide attempts, themselves, are recognized as a potent means of accruing capability for future attempts.24,95
As such, although associations between hyperactive/impulsive features, painful and provocative events, and acquired capability appear compatible with ITS hypotheses, we cannot ascertain when suicide attempts occurred during the lifetime, and how these affected scores in these variables. Likewise, we cannot ascertain that thwarted belongingness and perceived burdensomeness preceded suicide ideation; sadly, experiences of suicide ideation and nonfatal attempts themselves affect social relationships, with some individuals experiencing alienation and shame,96,97 which could, themselves, contribute to these apparently suicidogenic states.
Although cross-sectional studies can assist with preliminary hypothesis testing and highlighting areas of potential relevance, longitudinal designs are imperative to understand the development of these cognitive-affective states and their relationship with suicidality, and the development of suicide capability in response to real-life events.
The present findings come from the same sample described in Moseley et al., 33 and the same limitations of our sample are true. In that the sample was mainly British and largely Caucasian, the findings cannot be presumed to generalize to autistic people from other cultures and racial/ethnic groups. Similarly, as the sample primarily comprised cisgender autistic women with only a small proportion of autistic men (a smaller proportion of whom scored above cutoff on the CAARS-S:S), effects of sex in this study may be spurious and further research is needed to generalize findings to cisgender men more broadly.
Transgender men, transgender women, and people with nonbinary and broader identities were likewise under-represented, and notably our survey (based on our limited awareness at the time of design) did not adequately differentiate between different transgender identities, such that the numbers presented do not adequately reflect different transgender identities—this is especially important to attend to in future studies, given that suicide risk may be even higher in neurodivergent trans and nonbinary communities. 98 Other potentially marginalized aspects of identity, such as sexual orientation, are also important to measure and examine in future research.
Other groups un- or under-represented here include autistic people with severe intellectual disability, as the study was accessible only to those able to respond to an online advertisement and complete an hour-long (approximately) online survey; for the same reason, those with lower literacy and computer literacy skills were less likely to participate. Self-reported diagnoses were not validated by the researchers. Furthermore, although our advertisement did not mention ADHD specifically, the study may have been especially salient to individuals with experience of mental ill-health and suicidality, such that there may be a self-selection bias at play.
Limitations of our measures include our use of normative assessment tools for ITS constructs. Unfortunately, autism-adapted versions of these measures do not exist, so we cannot be sure that the present measures used in autistic populations actually capture the constructs intended by the original authors. 75 Even in the general population, there is a broader conceptual confusion around the nature and optimal assessment of certain constructs, such as acquired capability.99,100 Although we employed total ACWRSS scores as indicative of suicide capability in our sample, it is highly possible that the scope of this construct differs in neurodivergent people.
The deeper meaning of constructs such as perceived burdensomeness, thwarted belongingness, and acquired capability as perceived and experienced by autistic adults, and whether autistic people themselves perceive these concepts as relevant and important to suicidality, is an important target for future research.
Our investigation operationalized “likely ADHD” by way of CAARS-S:S scores, but this tool was likewise not designed for use in autistic people, or to differentiate between the cognitive and emotional profiles associated with ADHD and autism. Other studies suggest that autistic people (without ADHD) tend to score more highly than neurotypical people on the CAARS-S:S family of tests, though their scores are still significantly lower than those of nonautistic individuals with ADHD.101,102 Nevertheless, the suggested ADHD index cutoff was based on general population norms and has not been ratified for use in autistic people.
Although it is highly likely that some participants had undiagnosed ADHD, we cannot ascertain whether participants above ADHD index cutoffs would actually have met diagnostic criteria for ADHD. Future investigations should validate this co-occurrence with formal diagnostic tools, but if using screening tools, might consider those whose items map directly onto DSM criteria, 103 such that “likely ADHD” could be classified on the basis of meeting a sufficient number of diagnostic criteria. In addition, future research would benefit from including a comparison group of nonautistic people with ADHD to examine shared mechanisms for suicidality alongside additive effects of co-occurring ADHD and autism.
Future research would also benefit from greater scrutiny of variables common to both people with ADHD and autistic people—such as broader psychopathology and substance abuse,2,17,18 socioeconomic, and educational disadvantage104,105—all of which have relevance to everyday difficulties faced by autistic and nonautistic people with ADHD,106–109 to suicidality and interpersonal and intrapersonal constructs fundamental to the ITS.110–112 As we lacked control groups and more extensive consideration of such extraneous variables, we cannot confirm that the associations we observed are indeed particular to co-occurring ADHD within the autistic population, or delineate whether these effects are associated with intrapersonal features or other consequences of living as an autistic person with ADHD.
Finally, although our analysis focused mainly on mechanisms associated with hyperactive/impulsive feature domains, future investigations should explore the explanatory pathways between inattentive features and suicidality in autistic and nonautistic people with ADHD. There is a potential intersection of interest here in relation to sex and late diagnosis, both variables of significance to suicidality (see, e.g., recent literature1,13,113). In nonautistic people with ADHD, cisgender women and girls are more likely to present with primarily inattentive features, 114 a profile that, aside from sex, is associated with longer duration of ADHD going unrecognized, 115 often to the detriment of the individual.35,116,117
There is some suggestion that autistic people are more likely to show a combination of hyperactive/impulsive and inattentive features,118,119 though it is entirely possible that inattentive features are likewise under-recognized in autistic girls, women, and people assigned female at birth (AFAB). In relation to suicidality, we know that the girls, women, and people AFAB who receive a diagnosis of autism or ADHD are more likely to exhibit psychiatric conditions and visibly severe difficulties.120–122
As we controlled for sex and used CAARS-S:S scores as indicative of co-occurring ADHD, this study cannot speak of this issue, but as other studies have reported that suicide attempts are higher in autistic women with ADHD than any other group, 13 the intersectionality of age at diagnosis, feature profile, and sex and gender may be important for future study.
Conclusion
Our findings suggest that constructs from the ITS may bear partial relevance to heightened suicidality in autistic people with co-occurring ADHD. Most particularly, we found that perceived burdensomeness mediated the association between suicide ideation, suicide attempts, and our binary indication of co-occurring ADHD. Furthermore, a relationship between hyperactive/impulsive features and lifetime suicide attempts was mediated by greater exposure to painful and provocative events and acquired capability sequentially.
In that ITS constructs appear relevant to suicide in autistic people, future investigations should validate how these constructs are experienced and how they can be accurately assessed within longitudinal designs. However, the nature of a relationship between hyperactive/impulsive features through painful and provocative events alone also supports the importance of investigating other theoretical approaches, and pathways between traumatic events and suicidality.
Footnotes
Acknowledgments
Our deep gratitude is first and foremost to our participants for their generous participation in our research. We remember those who have died by suicide, and extend our deepest condolences to their families and loved ones. Our thanks go to the ACORN panel at Bournemouth University for funding this research; to colleagues at Bournemouth University and the Autism Research Centre for supporting our recruitment efforts, study design, and safeguarding measures; to staff at Autistica for allowing us to advertise to their research network; and to moderators and owners of Facebook groups who were willing to let us advertise our study.
Authors' Contributions
Quantitative data were collected and analyzed by Dr. Moseley, the primary author of the article, with support for recruitment from Ms. Smith, Dr. Allison, and Professor Baron-Cohen through the Cambridge Autism Research Database (CARD). All authors contributed to analysis decisions and preparing the article for submission.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
R.L.M. and N.J.G. are salaried staff of Bournemouth University; this project received internal funding (£3454) awarded to R.L.M. S.B.C. received funding from the Wellcome Trust 214322\Z\18\Z. For the purpose of open access, the author has applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission. In addition, S.B.C. received funding from Innovative Medicines Initiative 2 Joint Undertaking (JU) under grant agreement No 777394. The JU receives support from the European Union's Horizon 2020 research and innovation program and EFPIA and AUTISM SPEAKS, Autistica, SFARI.
S.B.C. also received funding from the Autism Research Trust, the Templeton World Charitable Fund, the MRC, SFARI, and the NIHR Cambridge Biomedical Research Centre. The research was supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care East of England at Cambridgeshire and Peterborough NHS Foundation Trust. The views expressed are those of the author(s) and not necessarily those of the HS, NIHR, or Department of Health and Social Care.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.