
Abstract
Background:
Autistic individuals might undergo a magnetic resonance imaging (MRI) examination for clinical concerns or research. Increased sensory stimulation, lack of appropriate environmental adjustments, or lack of streamlined communication in the MRI suite may pose challenges to autistic patients and render MRI scans inaccessible. This study aimed at (i) exploring the MRI scan experiences of autistic adults in the United Kingdom; (ii) identifying barriers and enablers toward successful and safe MRI examinations; (iii) assessing autistic individuals' satisfaction with MRI service; and (iv) informing future recommendations for practice improvement.
Methods:
We distributed an online survey to the autistic community on social media, using snowball sampling. Inclusion criteria were: being older than 16, have an autism diagnosis or self-diagnosis, self-reported capacity to consent, and having had an MRI scan in the United Kingdom. We used descriptive statistics for demographics, inferential statistics for group comparisons/correlations, and content analysis for qualitative data.
Results:
We received 112 responses. A total of 29.6% of the respondents reported not being sent any information before the scan. Most participants (68%) confirmed that radiographers provided detailed information on the day of the examination, but only 17.1% reported that radiographers offered some reasonable environmental adjustments. Only 23.2% of them confirmed they disclosed their autistic identity when booking MRI scanning. We found that quality of communication, physical environment, patient emotions, staff training, and confounding societal factors impacted their MRI experiences. Autistic individuals rated their overall MRI experience as neutral and reported high levels of claustrophobia (44.8%).
Conclusion:
This study highlighted a lack of effective communication and coordination of care, either between health care services or between patients and radiographers, and lack of reasonable adjustments as vital for more accessible and person-centered MRI scanning for autistic individuals. Enablers of successful scans included effective communication, adjusted MRI environment, scans tailored to individuals' needs/preferences, and well-trained staff.
Community brief
Why is this an important issue?
Magnetic resonance imaging (MRI) is an examination that shows human anatomy and may explain the causes of symptoms. Autistic people may need MRI scans for various reasons, such as low back pain, headaches, accidents, or epilepsy. They have known sensitivities to sound, light, smell, or touch and increased anxiety, so the narrow, loud, isolating, unfamiliar MRI environment may be overwhelming to them. If MRI scans are, for these reasons, inaccessible, many autistic people will have to live with long-standing conditions, pain, or other symptoms, or have delayed treatment, with impact on their quality of life, and life expectancy.
What was the purpose of this study?
We tried to understand how autistic people perceive MRI examinations, things that work, and the challenges they face. We also asked for their suggestions to improve practice and accessibility.
What did we do?
We distributed an online questionnaire to autistic adults through social media. We analyzed the data using appropriate statistical and text analysis methods.
What were the results of the study?
We received 112 responses. Autistic people rated their overall MRI experience as average. Nearly a third (29.6%) reported they were not sent any information before MRI, and only 17.1% reported that radiographers offered some reasonable environmental adjustments. Most participants (68%) reported that radiographers provided detailed information on the day of the scan. Only 23.2% of them disclosed their autistic identity when booking MRIs. We found that quality of communication, physical environment, patient emotions, staff training, stigma, and timely autism diagnosis impacted their MRI experiences.
What do these findings add to what was already known?
Autistic people MRI scan experiences are at the heart of this project. Our project shows that MRI for common symptoms is often inaccessible by autistic people. We should improve the MRI environment, adjust communication format/content for them, and deliver person-centered care in MRI. Health care professionals should receive relevant training, to understand the challenges autistic people might face and better support them in MRI scanning.
What are potential weaknesses in the study?
The pandemic has impacted participant recruitment; therefore, the results of this sample may not reflect the full impact on the wider autistic population or adequately represent the autistic community, due to small size and including only people who could consent.
These results come from different centers, so there is a lot of variation in the use of MRI equipment.
How will these findings help autistic adults now or in the future?
We outline the main challenges associated with MRI, so autistic adults and their families/carers understand more of what they could expect in future examinations; hopefully, researchers and scanner manufacturers will try to tackle these challenges to make MRI scans truly accessible for autistic people.
We shared this knowledge with stakeholders to develop guidelines and started using it in training. We want to ensure that MRI is person-centered and more accessible for autistic patients.
Background
Sensory overload and communication barriers remain two of the most important challenges to address when it comes to accessible health care for autistic individuals. 1 These barriers and challenges are significant and have profound impact on health care delivery, patient and service user experience, physical and mental well-being, quality of life, and life expectancy for autistic individuals.2–4 Recent studies have shown that, because of these challenges and lack of reasonable adjustments in health care settings, autistic adults experienced difficulties in making health care appointments by telephone (62%), in feeling heard and understood (56%), difficulty in communicating with their doctor (53%), and experiencing anxiety in the waiting room environment (51%). 3 There is, therefore, great need for person-centered reasonable adjustments to ensure equity of health care provision for all service users.4–7
Magnetic resonance imaging (MRI) is a medical imaging examination used for a wide range of clinical conditions, which allows delineation of fine anatomical details in the human body and therefore enables optimal diagnosis and treatment. However, as we explain later, it remains a lengthy, anxiety-provoking, challenging examination with moderate acceptance from patients, 8 despite some early efforts to optimise its clinical practice for the general population9–11 and for autistic people, in particular.12,13
Autistic people may need to undergo MRI examinations, either as part of a research project studying autism, or for clinical concerns, such as persistent headaches, low back pain, injuries, accidents, or falls. Researchers use MRI of the brain frequently for autism research.12,14–16 Further, we use MRI to assist in the diagnosis and monitoring of autism-related co-occurring conditions, such as epilepsy. 17
Recent research has shown that autistic individuals have higher co-occurrence of conditions such as epilepsy, which require medical attention and often MRI scanning.18,19 However, autistic individuals may face several challenges when accessing health care. These include lack of accessibility of services, lack of coordination or continuity of care, sub-optimal patient-provider communication, stigmatization (including from health care professionals), poor staff awareness of sensory sensitivities that might impact autistic service users, lack of clinical staff understanding of autistic people's needs, and general lack of knowledge regarding autism.20,21
Despite the increase in the number of autism-related research studies, there is still much to learn and understand about the barriers that autistic individuals face when accessing health care, 22 and also about the reasonable adjustments required to ensure they have a positive experience.4,23,24 For all these reasons, autistic service users cannot access health care provisions with the same ease as neurotypical individuals, resulting in unmet needs. This may also explain the lower quality of life, and increased overall mortality among autistic populations.25,26
Despite its clinical usefulness, MRI scanning can feel overwhelming for anyone wishing to undergo this medical examination. This is mainly because of the narrow structure of the MRI scanner, the loud noise during the scan, and the relatively long scan duration, 27 all of which may increase the risk of patient anxiety or claustrophobia.28–30 This might be further exacerbated among autistic individuals, who typically show higher levels of anxiety than the general population. 31
Claustrophobia, which may affect around 10% of neurotypical patients, 32 can adversely affect scan completion rates, increase scan repeats, and impact workflows and patient experience, with such data for autistic individuals still lacking. The need to administer intravenous contrast, to achieve optimal diagnosis in some MRI scans, and to optimally position a patient on the MRI examination table, so they can remain still for longer, may also pose further challenges to autistic individuals, exacerbating their sensory overload.
These issues emphasize the need for an individualized, person-centered approach for autistic individuals undergoing MRI scanning for a safe, accessible, and successful examination. To address these issues, we aimed at gaining an understanding of the main barriers to and enabling features of MRI scanning in the United Kingdom, as autistic adults reported, alongside mapping out their needs, preferences, and experiences during MRI examinations.
This work is part of a wider project that received funding from the Society and College of Radiographers, aiming at improving MRI scanning for autistic individuals. In this wider project, we included a systematic review, which identified all reasonable adjustments currently used when autistic patients undergo MRI examinations. 24 It also included a U.K.-wide survey investigating current practice and knowledge of radiographers, highlighting knowledge gaps of health care practitioners due to insufficient training. 33 The aim of this work was (i) to explore the MRI scan experiences of autistic adults in the United Kingdom, (ii) to identify barriers and enablers toward a successful and safe MRI examination, (iii) to assess autistic individuals' satisfaction with MRI service, and (iv) to inform future recommendations for practice improvement.
Methods
Methodology
We adopted the pragmatic paradigm, in which we employed a combination of quantitative and qualitative data collection methods.
The study aligns with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies, 34 the American Psychological Association guidelines for paper format, 35 and the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) for online surveys. 36
Participants
Participants were autistic individuals older than the age of 16 years. Inclusion criteria were an autism diagnosis or self-diagnosis of autism, self-reported capacity to consent, and a prior MRI scan experience in the United Kingdom. For autism diagnosis, we did not administer any screening questionnaires, or other means to confirm/reject diagnosis of autism. Of an initial sample of 122 survey respondents, we excluded 10 because they only completed demographic information but no other survey questions. The final sample included 112 autistic adults with demographic characteristics as follows (Table 1).
Demographic Data of Autistic Adults (n = 112)
The majority (88.4%) of autistic adults in this study did not report having any perceived or diagnosed disabilities; six reported having dyslexia, four also had attention deficit hyperactivity disorder, two dyspraxia, two dyscalculia, two sensory processing disorders, and one dysgraphia.
Materials
We designed an online survey on Qualtrics (Qualtrics, Provo, UT). We included quantitative Likert scale questions, as well as open-ended questions that prompted a qualitative response. We employed adaptive questioning to reduce number and complexity of the questions. 36
A team of experts in autism research and MRI scanning designed the survey questions with input from autistic consultants and autistic service users on the content and design of the questionnaire. The survey questions built on previous work, which identified the reasonable adjustments required for autistic adults in health care 37 or when scanning autistic individuals with MRI 24 as well as the enablers and challenges of MRI scanning based on practitioners' perspectives. 33 We conducted a pilot survey with the help of autistic individuals (n = 4), who provided detailed written and verbal feedback, that we included in the final survey.
The questions covered: (i) basic participants' demographic data; (ii) information about their MRI scan experience (number of scans, duration, anatomy that was examined, communication with the MRI personnel, provision of vital information on the scan requirements, environmental adjustments before, during, and after the scan, patient satisfaction metrics); (iii) recommendations for improvements addressed to health care practitioners; and (iv) suggestions and advice to other autistic service users.
We offered visual mapping of survey completion rates and workflow adjustments to allow free movement through the questions (both forward and backwards) to make the survey more accessible to the participants. We worded all questions using neurodiversity-friendly, identity-first language. We did not offer any incentives to participants.
Procedures
Data collection
We collected data between February 17, 2021 and April 30, 2021, using the snowball sampling technique 38 to facilitate recruitment of participants who may be hard-to-reach. We distributed the survey electronically through the National Autistic Society, the London Autism Group charity, the researchers' professional networks, and the autistic community on Twitter, LinkedIn and Facebook, with a clear note of the study being only open to autistic participants with experience of an MRI scan in the United Kingdom. We used electronic reminders and regular re-sharing on social media to increase the uptake. 39
Patient, public, and community engagement
We employed patient and public involvement during research planning, survey design, piloting and data collection, data analysis, and drafting of this work, to ensure that we actively involved autistic individuals in this project from start to end as co-producers. A team of seven radiographers and one nurse worked with four autism researchers, two autistic consultants, and three autistic service users to discuss pre-study considerations, co-produce and revise survey items, discuss recruitment of participants, and post-study considerations. Following AASPIRE's guidelines, 7 we strove to use flexible modalities, to provide sufficient processing time, to encourage transparency and power sharing, and to disseminate findings collaboratively. Co-authors include two autistic people who worked closely with the team as research collaborators.
We achieved direct feedback from the autistic community through one-to-one online discussions with service users and autistic consultants, group online discussions, and presentation of the work in two live online events with a strong autistic community representation in the audience. We also placed an announcement on Twitter using the hashtag #actuallyautistic #autismfriendlymri seeking feedback from the autistic community. We used similar hashtags on other social media, including the social media channels by the London Autism Group.
Ethics and governance
We received ethics approval before this study by City, University of London Health Sciences Research Ethics Committee (ETH2021-0950). We obtained electronic informed consent at the beginning of the survey via a dedicated question. Participants had access to an information sheet on the first page of the survey containing all the essential information for the study and had access to an email address for any enquiries. Anonymity of the participants was vital to create a safe environment, enabling the authenticity of the responses. If participants felt secure in the knowledge that their responses could not be traced back to them, we thought that this was more likely to encourage honest feedback and authentic dialogue. Data collection and data storage followed the research institution's protocols.
Quantitative analysis
We used the Statistical Package for the Social Sciences (SPSS), version 26 (IBM; SPSS, Inc., Chicago) for quantitative analyses. We reported descriptive statistics in terms of absolute numbers and/or frequencies of responses for categorical data and means and standard deviations (SDs) for the continuous ratings of patient experience. As survey questions did not force a response and most questions provided an option for participants to indicate that they could not recall relevant details, therefore relevant frequencies do not always sum to the full sample size.
To further characterize the patterns of observation in the descriptive data, we explored associations between variables through non-parametric Spearman's rank-order correlations or chi-square tests. Where appropriate, we used t-tests for sub-group comparisons, and we reported Cohen's d effect sizes to quantify the magnitude of the differences we observed. We set the level of statistical significance at p < 0.05 and generated graphs to highlight any relevant findings.
Qualitative analysis
We employed content analysis to analyze the answers to the open-ended questions of the survey. In particular, we used conceptual content analysis, to determine the occurrence and frequency of concepts in this free text. 40 To achieve this, we used a process of selective reduction of the concepts identified in explicit terms. We moved from initially coding explicit terms into topic categories, which shared a commonality with each other, in a way that was, as possible, exhaustive but not mutually exclusive. We then worked to derive more generic themes, each one of which encompassed interconnected topic categories. 41
These open-ended survey questions related to (i) descriptions of individual MRI scan experiences and (ii) suggestions for future improvement of practice as the autistic service users suggested. Two researchers performed the analysis; one (T.O'R.) employed the NVivo software (QSR International Pty Ltd.) and the other (J.M.H.-L.) used manual analysis, both underpinned by the principles of content analysis.41,42 The two researchers read and re-read data in an inductive approach, which consisted of the researchers familiarizing themselves with the data and noting initial ideas; coding the data according to ideas, interesting features, and consistent patterns; reviewing the codes resulting in consolidation and grouping into categories and then, as the analysis progressed, into comprehensive themes; finally, the researchers re-read data to check for perceived analytical gaps and to validate the themes.
To emphasize the participants' voices in results, we also read through and highlighted pertinent quotes from the data and added a pictorial representation of the overall themes and categories. Finally, we produced a table with frequencies for each category. Different types of qualitative analyses have employed this approach in the past, to help introduce a “weighting” between different themes and categories, particularly when it comes to amplifying service user experiences and highlighting priorities for practice change43–46 (corresponding to those categories with the highest frequency in the data).
To ensure trustworthiness, intra-coder agreement exercises took place to promote researchers' reflexivity. 47 We facilitated data interpretation using group discussions within the research team, and C.M. and N.S. conducted a credibility check of themes. 42 A final consultation with the whole team followed to discuss specific theme descriptions and select the most relevant quotes.
Convergence of results
We attempted to integrate the qualitative and quantitative results and converge them into the recommendations for the future practice section further below.
Results
MRI scan characteristics
Nearly half of the autistic adults (47.3%) had experienced between two and five MRI examinations, 37.5% had only one, and 15.2% more than five. The number of previous MRI scans did not relate to the overall MRI experience as the adult respondents rated (rs = 0.07; n = 104; p = 0.46). In terms of scan durations, 21.9% of participants reported that their most recent scan was 10–20 minutes long, for 28.9% of them scans lasted 20–30 minutes, and 32% reported scans longer than 30 minutes. Across all participants who could recall scan durations, there was no correlation between the duration and overall MRI experience (rs = 0.11; n = 98; p = 0.91).
Most autistic adults (71.5%) who reported multiple scans said that they had their MRI scans at different hospitals/departments and the majority of scans (58.1%) took place in the past 2 years.
MRI scan referrals
Musculoskeletal concerns, low back pain, headaches, and injuries were the main reasons to refer participants for MRI examinations (Supplementary Material S1).
Communication and flow of information before, during, and after the MRI scan
A minority of autistic adults (23.2%) reported that they (or in one case someone on their behalf) informed the department about their diagnosis when scheduling the MRI examination. Across the entire sample, of those who disclosed their autistic identity, 31% were asked about needs or preferences for the scan, whereas of those who did not disclose their diagnosis only 4% were asked about needs or scan preferences. A significant effect of good communication and attention to the patients' needs and preferences was related to the likelihood of them disclosing their autistic identity, χ 2 (1, n = 105) = 15.22, p < 0.001.
Interestingly, the 28 participants who reported disclosing their diagnosis rated their overall scanning experience as marginally worse (M = 37.89, SD = 28.63) than the 71 participants who did not (M = 49.69, SD = 29.24) (t = 1.82, df = 97, p = 0.072) with a moderate effect size of Cohen's d = 0.41. By contrast, the 11 participants who reported being asked about their needs and preferences reported significantly higher scan satisfaction (M = 65.00, SD = 25.87) than the 88 participants who reported not being asked (M = 44.02, SD = 29.12) (t = 2.28, df = 97, p = 0.025) with a large effect size of Cohen's d = 0.73. Sample sizes were too small to draw definitive conclusions on the interaction between disclosure and being asked about personal preferences.
In terms of type of information before scan, 55.4% of participants reported being sent an information leaflet, 14.9% were offered verbal information over the phone, and a further 1.6% of the respondents were sent a link with an informative video to watch at home. None of them was offered a pre-visit to the MRI department, and nearly a third of the respondents (29.6%) reported they were not sent any information at all.
Most participants (68%) reported that radiographers tried to provide detailed information to them on the day of the examination. Also, most autistic service users (85.8%) reported that they understood what was required of them during the scan.
Regarding communication between the radiographer and the patient during the scan, 41.5% of autistic adults reported that the radiographer tried to maintain regular communication with them. Most of the autistic adults (70.8%) reported that they did not have any way to know how much time was left when inside the MRI scanner, a factor considered vital to manage their anxiety.
After the MRI scan, slightly more than half of autistic individuals (52.5%) reported receiving sufficient information as to what to expect next.
Personalizing the patient's MRI journey
Only 15.2% of autistic adults were asked to bring their favourite music to listen to during the scan. Nearly half of the respondents (48.4%) reported a lack of Special Educational Needs specialists onsite.
Accompanying people were allowed into the MRI room for 30.4% of autistic adults. More than half of the autistic adults in this sample size (51.8%) reported being very independent, therefore they did not request an accompanying person for the scan.
Only 17.1% of respondents reported that radiographers offered some reasonable environmental adjustments, which included (i) allowing more time to ask questions and get explanations (21%), (ii) music played through the headphones (14.8%), (iii) offering a blanket (11%), (iv) making efforts to reduce noises (11%), (v) adjusting lighting in the room (7.8%), (vi) adjusting temperature (6.2%), (vii) offering more pillows (4.6%), (viii) allowing more time for familiarization (3.9%), (ix) trying to reduce number of people in the room (2.3%), and (x) offering a video to watch during the scan (1.6%).
A total of 36.8% of adult autistic service users reported that they were offered headphones for use during the scan, only 34% of them were offered music, and 6.4% said they had the option to watch a movie during scanning.
Patients' ratings of their MRI experience
We also asked autistic adults (n = 112) to rate their experience (from 0 to 100, where 0 = poor experience, 50 = moderate 100 = excellent) in relation to the MRI unit environment (Fig. 1). Overall, autistic adults highly rated the cleanliness and tidiness in the MRI room; however, experiences in relation to acoustic noise levels in the scanning area, comfort when lying down on the scanner examination table, and availability of quiet areas to relax were rated as very poor by most autistic adults.
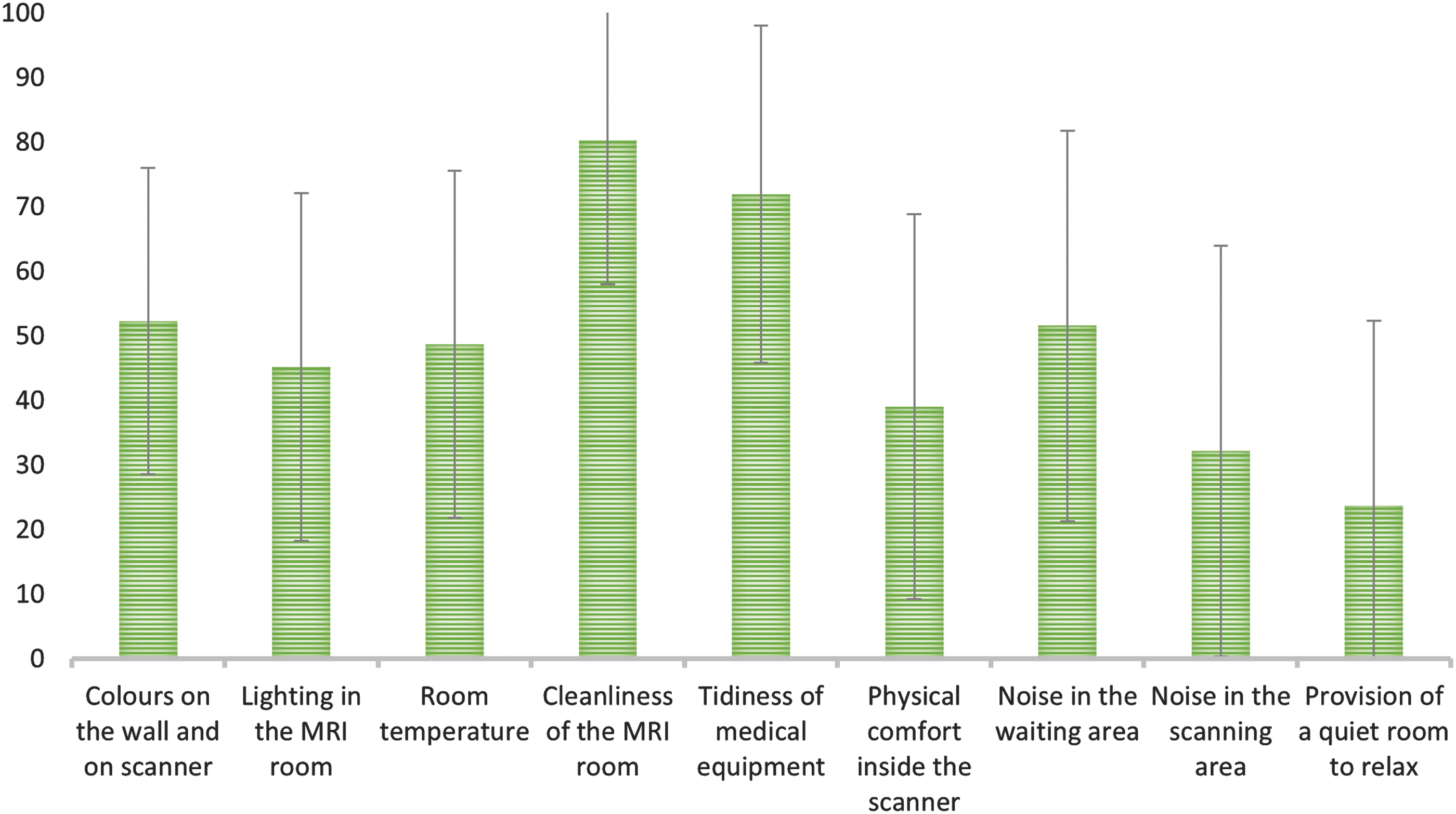
Mean experience ratings on a 1–100 point scale (1 = very poor, 100 = excellent) and SD related to the MRI unit environment, as rated by autistic adults. The y-axis relates to mean experience ratings and the x-axis presents different physical environment characteristics, that participants were asked to rate in the MRI unit. MRI, magnetic resonance imaging; SD, standard deviation.
A total of 44.8% of respondents reported experiencing claustrophobia during the MRI scan. Although only 17% of the 17 adults who had undergone more than 5 scans reported claustrophobia compared with the 38.3% of the 42 who had only one scan, overall, the relation between number of scans and reports of claustrophobia was not statistically significant (rs = 0.007, n = 72, p = 0.95).
Finally, we asked the respondents to rate their overall MRI experience from 0 to 100, and on average they rated their experience as neutral (mean = 48.54 ± 30.14).
Qualitative results
Figure 2 demonstrates the themes and categories of the content analysis.

Themes (in blue background) and respective categories (in white background) emerging from content analysis.
The categories that emerged from the content analysis of the open-ended questions can also be viewed in Supplementary Material S2 in descending order of frequency based on their occurrence in the data. The data related to (i) descriptions of MRI scan experiences and (ii) suggestions for improvement of these experiences to other autistic service users and to health care practitioners. Further, Table 2 given next depicts some representative quotes on the five more frequently discussed categories.
Representative Quotes for the Top 5 Emerging Categories as Derived from Content Analysis (See Also Fig. 2)
ASD, autism spectrum disorder.
Discussion
Although many studies use MRI to study the neurological correlates of autism, to our knowledge, this study is the first of its kind that directly highlights the experiences of autistic service users when undergoing MRI examinations. The results of this study point to a range of interesting, although concerning, findings with clear implications for future practice.
Communication and flow of information between health care practitioners and autistic service users
From the combined results of this work and previous literature,24,33 communication between health care services and autistic service users scheduled for MRI examinations is vital and it needs further improvements. This observation relates not only to the lack of information to the service users beforehand, but also lack of communication between health care services (e.g., referring consultants and radiology practitioners) and suboptimal information exchanges before and on the day of the examination.
Recent research corroborates this, as autistic service users have been found to largely report communication challenges alongside other barriers when accessing health care.3,21,48 Poor patient-health care provider communication leads to lower satisfaction for autistic patients because of more unmet needs during their care compared to non-autistic users. 21 If a radiographer is not aware of all the required information before the patient attending for MRI scanning, they have very limited options and time to customize the MRI scan for the patient on the day of the examination. Also, and perhaps most importantly, providing a lot of new information to autistic individuals on the day of the MRI scan, and not before, could further increase their anxiety and make the whole experience overwhelming. Therefore, it is essential to provide them with accurate and meaningful information in a timely manner.
The MRI departments should engage with autistic service users by employing a personalized communication approach during pre-visits, such as obtaining critical information about the autistic patient's needs and preferences before the examination.12,13,48 Effective communication should also include clear and detailed information provided to autistic individuals well before the examination in an inclusive way: We must also consider the timing and format (orally, in writing, with the use of flashcards, and/or with the facilitation of a specialist), since customization of the experience correlates with improved health care outcomes.49,50 It is useful to note that many autistic individuals prefer other ways to communicate than the phone, due to social anxiety and other reasons. 51
Impact of masking
Most of the adults in our study (53.6%) did not disclose their autistic identity when booking the examination with the MRI department. This may be because of concerns about being stigmatized, lack of adequate information provided from health care services, and masking. 52 Some respondents explained that they felt embarrassed to disclose they were autistic before the MRI scan, because of fear of how this could affect their care. Our results substantiate that, when prompted by health care practitioners, autistic services users in our study were at least twice as likely to disclose their identity before the MRI scan compared with those who were not prompted by a health care professional.
Social camouflaging, often with masking behaviors, is used by many autistic individuals to hide their autistic identity during social interactions. 52 Very importantly, camouflaging or masking may limit the availability or range of provisions and adjustments and, subsequently, impact service user experience. Interestingly, disclosing a diagnosis and individualized needs and preferences may lead to a worse scanning experience than not disclosing at all, as this study has shown. This may be because the expectations for service provision increase when an autistic person discloses their identity and preferences; however, the link between expectations and satisfaction in health care remains weak and not sufficiently studied. 53
We must still do a lot of work to support and empower autistic patients to disclose their identity when using health care services, to ensure their individual needs and preferences are met and their experience is humanized. 54 Finally, we can also attribute the lack of customized communication approaches or reasonable environmental adjustments to the lack of a formal autism diagnosis at the time of MRI scanning that might impact overall experience.
Communication and coordination between health care services
The examples of poor communication before, during, and after the scan from this study also indicate a lack of coordinated care, and lack of effective communication between health care services. Previous research has similarly reported a lack of support from general practitioners toward autistic individuals, 55 and this highlighted the need for cross-disciplinary coordination for continuity of care of autistic patients. 20
The lack of early vital information reaching health care practitioners makes it more challenging for booking staff, receptionists, and radiographers to co-ordinate a plan and prepare personalized strategies for communication and reasonable environment adjustments. The lack of appropriate staff training in autism further accentuates these challenges. 33
Despite the lack of sufficient information before MRI scanning, most of the respondents received adequate information during scanning (e.g., on how to use the MRI call button in case they felt unwell), in line with current MRI safety requirements before MRI scan. 56 Although most of the autistic participants reported not having regular communication with the radiographer during the scan, some explained it was their choice as they preferred to minimize distractions during the examination.
Personalizing the autistic patient's MRI journey
Customizing the patient's journey is vital for their experience in MRI; we can achieve this in different ways, 24 including audiovisual material, pre-visits, and other familiarization techniques, distraction techniques, and in-scan optimization, including noise reduction and faster scanning techniques.57,58
In the present study, most MRI radiographers did not adjust the MRI unit environment for autistic individuals, and we can attribute this either to lack of knowledge of the patient's needs, lack of training, lack of resources, or lack of time during the busy clinical MRI slots. 33 These adjustments are, however, vital for a successful examination, given sensory processing sensitivities of autistic people, 59 atypical visual behavior, auditory sensory processing sensitivities, and potential difficulties in processing simultaneous visual, auditory, and tactile inputs. 60
Based on this evidence, MRI departments should invest in staff training, patient preparation/communication, equipment, for example, adjustable lighting and temperature systems, spaces, for example, quiet areas, and finally develop strategies and make use of available hardware/software to reduce the noise. Moreover, visual timers could help alleviate some of the anxiety as they could offer some indication of the remaining time in the scanner for those who wish to know.
The literature reports hearing loss as an MRI-related complication. 61 The reduced use of headphones during MRI scanning, as autistic service users reported in this study, raises serious concerns regarding the lack of basic provisions of essential MRI safety equipment. However, this may be due to the use of earplugs instead or other noise canceling techniques during scanning or of inherently quieter MRI sequences.62,63 This could also be due to inability to fit the headphones in the head coil due to coil design. This concerning finding is something that warrants further investigation in future studies.
Our results indicate that nearly half of the patients were not offered music, despite its known benefits to minimize anxiety and offer some distraction.13,64,65 However, resourcing allocations or equipment functionality may limit the use of audio or visual hardware and software, so we must interpret the results under this lens.
Most patients in this study did not require the use of sedation or general anesthesia (GA) before their examination. Sedation or GA have been used when scanning autistic individuals (mainly children) in the MRI environment.66,67 However, these strategies carry their own potential risks, 68 and we should reserve them only for patients not able to undergo the examination fully awake, after a careful risk-benefit analysis on a case-by-case basis and in discussion with the service user and their carer, where appropriate. 69
Patient satisfaction and ratings of MRI scan experience
Research has indicated that patients undergoing MRI examinations can be influenced by prior personal experience or by the experiences of others. 70 The MRI-related anxiety is higher during the first MRI scan. 71 We should take all these into account when customizing the patient's MRI scan.
Autistic service users also reported a positive experience regarding the cleanliness and tidiness of the MRI room. Previous research findings highlight the impact of clean health care environments on reducing health care-associated infections 72 and improving patient satisfaction with the health care service. 73 Our study might include more MRI scans taking place around the COVID-19 pandemic, so our participants might have experienced an environment where enhanced universal cleaning and disinfection techniques were applying.
Autistic individuals rated excessive noise and the lack of quiet rooms as the most negative aspects of their MRI experience. Noise during MRI scans can reach above 100 db 74 and it is a major factor of patient anxiety in hospital settings in general. 70 Autistic individuals are known to present more frequently than the general population with different levels of hearing loss, hyperacusis, or other hearing conditions and sensitivities, 75 so efforts should be focused on improving these aspects during their MRI scans.
In addition, ensuring the patient's physical comfort when lying down inside the scanner is vital for an improved patient experience, for high-quality scans without motion artefacts, elimination of scan repeats, and recalls. 76 Hence, we could employ lightweight and flexible coils, softer examination table mattresses, better and more customizable patient positioning provisions, or wider magnet bores, including open-MRI and upright MRI solutions, to improve patient comfort.77,78
Autistic participants rated their overall MRI experience as moderate. This was attributed mainly to the lack of reasonable adjustments during the scan. Patient satisfaction with MRI examinations varies, as previous studies in the general population have reported, vastly related to individual patient experiences and environments.79,80
We noted a larger incidence of claustrophobia (44.8%) among autistic service users in our study compared with studies in the neurotypical population (10%). 30 We can attribute this to the complex sensory sensitivities and higher levels of anxiety experienced by autistic service users, which might increase prevalence of claustrophobia, but it may also be that this survey was completed predominantly by people who wanted to raise a concern in relation to their MRI scan experience, so we should interpret it with caution.
The results of the present study constitute valuable pilot data for larger-scale prospective studies to optimize radiography practice, communication, software, and hardware capabilities to better serve not only the autistic community, but also the general population.
Importantly, there are yet no data that report the numbers of autistic individuals who cannot undergo MRI scanning because of lack of accessibility. Autistic individuals living with chronic pain and various undiagnosed conditions, who have not been able to have any MRI examinations and therefore not eligible to participate in this study, have contacted us via social media to voice their concerns for the lack of accessibility of MRI examinations and the challenges they faced.
We hope that this and future studies will raise awareness of the poor experiences of autistic individuals undertaking MRI scanning and the lack of accessibility of MRI provisions and inform recommendations for MRI practice improvement.
Recommendations for practice
Table 3 summarizes some key recommendations for practice highlighted by our qualitative and quantitative data and supported by other literature as well. Although many of these recommendations relate directly to better and more resourcing, their deployment may allow for more efficient and effective use of MRI scan time.
Key Recommendations for Practice
GP, general practitioner; MRI, magnetic resonance imaging.
Limitations
Sampling
This study used convenience sampling and numbers of respondents do not represent the large U.K. autistic population, so we should interpret the results with caution. Also lack of access to social media, through which we distributed the study, might have prevented the participation of some individuals. Finally, as this study only included autistic people with the capacity to self-consent, the results cannot be confidently generalized beyond autistic people whose intellectual disability prevents them from possessing the capacity to self-consent.
Demographics
The predominance of female autistic adults over male respondents in this study (three females to one male) is not consistent with population estimates (three autistic males to one female), although the latter are based largely on formal diagnoses and not self-identification, so they may underestimate true numbers of autistic female individuals.81,82 Previous studies suggest that females are frequently undiagnosed and under-represented in various research settings, such as clinical trials, and that some gender-related discrepancies in recruitment still exist.83,84 For the current study, we are unsure whether this occurred because women are more likely to participate in research than men, 85 or whether it is because more autistic women undertake MRI scanning as part of their care.
Impact of COVID-19 pandemic on this study
We designed and conducted this study during the third lockdown of the COVID-19 pandemic in the United Kingdom, which inevitably affected participant recruitment, research design, and methodology. The research team had to adjust to social distancing and other health, safety, and infection control restrictions. Moreover, during that challenging time, the autistic community was disproportionately affected by the pandemic86,87 and priority has shifted to mental and physical health, social distancing and face mask use, employment, and home-schooling. Inevitably workflow and some practices for MRI scans may have changed during that period; we do not have enough data to study the effect of this change on our study.
Retrospective study design
This retrospective study sample is highly heterogeneous, as the respondents have been scanned by different MRI teams, in different MRI scanners, at different hospitals, and for different medical conditions or anatomical areas, all factors that can impact patient experience. Given this heterogeneity, it is difficult to identify the specific combination of factors that are of most importance in determining a positive patient experience. Hence, there is a need to prospectively examine the usefulness of different adjustments in a standardized clinical environment in future studies.
Conclusion
The findings of this study have highlighted the need for coordinated, customized, person-centered care and communication, availability of provisions and of reasonable adjustments during MRI scanning for autistic individuals, as central to service users' experience. We should encourage and empower service users to disclose their preferences and needs early before the scan, to ensure adequate provisions are available for them, as required. The MRI departments should be equipped with all the necessary software and hardware for MRI scan facilitation and offer specific training to relevant staff to meet the needs of every patient, including autistic patients.
Time spent in the preparation and customization of a scan is time well invested toward improving patient experiences and outcome of MRI examinations. Such adjustments to improve accessibility for autistic individuals can also serve a wider population with anxiety when attending for an MRI scan, helping to universally optimize patient experience.
Footnotes
Acknowledgments
The authors would like to thank the Society and College of Radiographers for funding, the London Autism Group Charity, the National Autistic Society, and the autistic community on all social media for kindly and very generously distributing their survey, to increase its scope and reach. Finally, they would like to wholeheartedly thank all autistic participants for kindly sharing their experiences of MRI scanning with us at a time that many of them were severely impacted by the implications of COVID-19 societal restrictions and lack of provisions during the pandemic. They owe them so much and this work is dedicated to them, with the hope it will make a difference to their future experiences of MRI scanning and to those of other autistic individuals, in the United Kingdom and beyond.
Authorship Contribution Statement
Conceptualization of the study and study ethics and design was performed by C.M. The manuscript was drafted by N.S and C.M. Qualitative data were analyzed by J.M.H.-L. and T.O. and reviewed by G.P., and all quantitative analyses were performed by N.S. and S.B.G. Community involvement was through the autistic community on twitter, but also facilitated by K.M. and S.P. as coauthors of this work. All authors edited and approved the final manuscript.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Society and College of Radiographers CORIPS grant scheme [Grant No. SCoR 155-50011HY]. Dissemination and training costs were provided by the City Radiography Research Fund.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.