
Abstract
Background:
Camouflaging involves the masking of autism traits, potentially creating an outer impression of “non-autisticness.” Although associations of camouflaging with anxiety and depression in autistic adults are widely reported, factors that mediate these associations are unclear. We examined two potential mediators of the association between camouflaging and anxiety/depression: perceived stress and emotion regulation (ER) challenges.
Methods:
Seven hundred eighty-seven autistic adults (18.2–78.2 years) recruited through Simons Powering Autism Research (SPARK) Research Match completed questionnaires, including the Camouflaging Autistic Traits Questionnaire (CAT-Q), and measures of autistic traits, depressive and anxious symptomatology, perceived stress, and ER challenges. Four moderated mediation models were tested. In all models the independent variable was CAT-Q total score, and the moderator variable was sex designated at birth. The dependent variable was depressive or anxious symptomatology, and the mediator variable was perceived stress or ER challenges.
Results:
We found that more camouflaging, increased ER challenges, and higher levels of perceived stress were associated with greater depressive and anxious symptomatology. We also found that perceived stress and ER challenges significantly mediated the associations between camouflaging and both depression and anxiety. In the model with perceived stress and anxiety, sex moderated the mediation, with females showing a stronger mediation. There was no significant moderation in any of the other models.
Conclusion:
We contextualize the findings within the broader literature on camouflaging as a response to stigma and other facets of minority stress. We discuss how the results of this study support the idea that the day-to-day stress of living in a neurotypical world, the cognitively demanding nature of camouflaging, and the constraints that camouflaging place on autistic people's behaviors in social contexts (e.g., contributing to suppressing ER strategies such as stimming), create a cycle that contributes to elevated rates of anxiety and depression in autistic people.
Community brief
Why is this an important issue?
Camouflaging describes behaviors that can mask social differences. Camouflaging includes things such as “copying” other people's hand movements or facial expressions. Some autistic people say camouflaging feels like they are “pretending” to be someone they are not. Camouflaging is associated with depression and anxiety. We do not know exactly what other factors may be related to these associations between camouflaging and depression and anxiety. Autistic adults have high rates of depression and anxiety. It is important to understand factors that might make autistic adults more vulnerable to depression and anxiety.
What was the purpose of this study?
The purpose of this study was to look at possible factors related to associations between camouflaging and anxiety and depression. We looked at two factors: perceived stress and emotion regulation challenges. Perceived stress is how stressed a person feels in their day-to-day life. Emotion regulation is how a person handles their emotions across different situations. We looked at perceived stress and emotion regulation challenges for three main reasons. First, autistic adults report high levels of perceived stress and challenges with emotion regulation. Second, perceived stress and emotion regulation challenges are both associated with depression and anxiety in autistic people. Third, camouflaging is associated with increased stress in autistic people.
What did the researchers do?
We asked 787 autistic adults living in the United States to complete surveys. Participants answered questions about camouflaging. Participants rated their anxiety and depression. Participants reported on how stressed they felt and how they handled their emotions. We looked at associations between camouflaging and depression and anxiety. We also looked at whether different amounts of perceived stress or different challenges handling emotions were associated with camouflaging, depression, and anxiety. We tested whether all of these associations differed for autistic people designated male sex at birth relative to those designated female sex at birth.
What were the results of the study?
We found that more camouflaging, increased emotion regulation challenges, and higher levels of perceived stress were all associated with more depression and anxiety. We also found that perceived stress and emotion regulation challenges each significantly related to the associations between camouflaging and both depression and anxiety. For the most part, these associations did not differ for autistic people who were designated male sex at birth relative to those who were designated female sex at birth.
What do these findings add to what is already known?
These findings support the idea that the day-to-day stress of living in a neurotypical world play a part in elevated rates of anxiety and depression in autistic people.
What are the potential weaknesses in the study?
We collected information from autistic people at one point in time. This limits how we can interpret the associations we found.
How will these findings help autistic adults now or in the future?
These findings may help us to better understand why autistic adults are at risk for depression and anxiety. The findings may show us ways to improve the mental health of autistic adults.
Introduction
Camouflaging in autism refers to behaviors that may modify the presentation of core autism (i.e., social-communication and restricted/repetitive behavioral) traits. 1 Camouflaging involves the masking of autism traits, potentially creating an impression of “non-autisticness.”1–4 The autobiographical writings of autistic people have provided rich descriptions of camouflaging, 5 drawing the attention and interest of autism researchers. Qualitative research has investigated camouflaging by querying the lived experiences of autistic people (e.g., in interviews), 6 whereas cross-sectional quantitative studies have endeavored to operationalize camouflaging and examine its associations with other variables, such as gender identity, sex assigned at birth, and mental health.
The two broad approaches to this operationalization are the self-report7,8 and discrepancy-based9–11 approaches. Self-report approaches ask individuals to reflect on and rate their experiences and behaviors of camouflaging, whereas discrepancy-based approaches quantify camouflaging as a “discrepancy” between external behavioral presentations and internal or lived autistic experiences.
Both conceptual and terminological challenges confront camouflaging research.12,13 These challenges include the wide variety of terms used to refer to camouflaging and other potentially overlapping or related constructs. These terms include “masking,”14–16 “social compensation,”17–19 “adaptive morphing,” 20 and “passing as non-autistic.” 21 (See table 1 in Ai et al., 22 e.g., of autistic camouflaging strategies; see Supplementary Table S1 in Lai et al. 12 for explication of constructs with potential “links” to camouflaging and how these may be similar to and/or different from autistic camouflaging.)
Participant Characteristics and Self-Report Ratings
Gender identity n = 785; race n = 784; ethnicity n = 781; household income n = 785.
AQ-28, 28-item Autism-Spectrum Quotient; BDEFS, Barkley Deficits in Executive Functioning Scale; CAT-Q, Camouflaging Autistic Traits Questionnaire; SD, standard deviation.
In addition, it is currently unclear how camouflaging differs from or is similar to experiences of social anxiety or other psychiatric symptomatology or conditions that include increased fears of negative social evaluation.13,23 To increase rigor in the study of camouflaging, some recommend that researchers adopt a broader framework, 22 conceptualizing camouflaging as a form of impression management, which involves self-monitoring and self-concealment to make favorable impressions on others.
The most recent version of the Diagnostic and Statistical Manual for Mental Disorders-Fifth Edition (DSM-5) 24 acknowledged, for the first time, the role that compensatory strategies, such as camouflaging, may play in modifying autism's clinical presentation: “…symptoms must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities or may be masked by learned strategies [emphasis added] in later life).”24(p50)
Camouflaging may modify the presentation of various “autistic” behaviors, with the bulk of research having approached camouflaging primarily from the angle of social communication differences (see review in Cook et al. 25 ). Camouflaging may also modify the presentation of restricted and repetitive behaviors and interests, 26 for instance, autistic individuals may conceal or suppress “stimming” or repetitive motoric movements in social contexts. 27 Importantly, however, regardless of how camouflaging may modify the external observable presentation of autism, camouflaging does not modify the underlying autistic profile and thus the internal lived experience of autism.28–30
Camouflaging may thus create a mismatch between an external presentation that does not suggest autism (and may even appear to argue against autism) and an internal lived experience of autism-related differences. 6 This mismatch may in turn be linked not only to later diagnosis but also to elevated risk for mental health difficulties, 31 including anxiety,17,32 depression,32,33 and suicidality. 34 Indeed, for autistic adults who report camouflaging, emerging evidence indicates that finding it more difficult to camouflage (i.e., subjective report of increased difficulties with camouflaging) is a possible “autism specific depression symptom.”35(p11)
To our knowledge, no study to date has examined potential mediators of the associations between camouflaging and depression/anxiety. Thus, the aim of this article is to address this lacuna by looking at two candidates: emotion regulation (ER) challenges and perceived stress. ER is a component of executive functioning (EF). EF is an umbrella term, designating a suite of self-directed actions engaged in the service of goal acheivement. 36 ER is one component of EF, referring to the contextually appropriate direction and modulation of emotional responsivity to facilitate goal pursuit and achievement. 37
Broadly, emotion (dys)regulation has been implicated in anxious38–40 and depressive39,41,42 disorders, including vulnerability for these disorders. Furthermore, in adults, ER mediates the association between cumulative adverse life experiences and depression 43 and between interpersonal stress and depression, 44 suggesting the potential importance of ER as a factor in depressive symptomatology.
Perceived stress refers to a person's appraisal of how stressful their everyday life is and how equipped they assess themselves to be at handling day-to-day stressors. 45 Within the general population, elevated perceived stress is associated with depressive and anxious disorders, 46 and mediates associations between neuroticism and anxious and depressive symptomatology. 47
More narrowly, research provides suggestive evidence for the roles of ER challenges and perceived stress in depression and anxiety in autistic individuals. Challenges in ER are prominent in autism,48–51 are more prevalent in autism relative to neurotypical populations, 51 and endure throughout the lifespan for some autistic individuals. 52 ER challenges are related to core autism traits, including uncertainty intolerance, 53 difficulties with changes in routine, and sensory overstimulation. 54
In autism, greater emotion dysregulation is associated with increasing expressions of suicidal ideation, which itself is significantly elevated in autistic individuals compared with the general population. 55 Because of these associations and the prevalence of ER challenges in autism, some propose that co-occurring psychiatric conditions in autism may be better understood and addressed as an intersection of emotion dysregulation with autism traits,50,56,57 and ER is identified as a therapeutic target to reduce the burden of mental health conditions in autistic individuals. 58
Another likely contributor to mental health problems in autistic adults is the experience of everyday life as stressful. Indeed, overall, autistic adults report higher levels of perceived stress relative to neurotypical adults.59–62 Although (to our knowledge) no study to date has examined associations between perceived stress and camouflaging, the qualitative literature on camouflaging indicates that camouflaging is linked with elevated experiences of stress in autistic adults. These studies have illuminated the lived experience of camouflaging among autistic adults, who describe camouflaging as effortful, exhausting, and stressful.6,63,64 Indeed, camouflaging is qualitatively linked to “autistic burnout,” characterized in part by overwhelming exhaustion and decreased tolerance for otherwise manageable sensory stimuli and social interactions.31,65
Camouflaging is observed more frequently in autistic girls/women versus autistic boys/men,11,66,67 and may play a role in misdiagnosis of autistic girls/women.3,6,68 Although camouflaging is attested in autistic males and autistic females, studies in child,9,30,67 adolescent,69–71 and adult66,72 samples have reported greater levels of camouflaging in autistic individuals designated female at birth (DFAB) relative to those designated male at birth (DMAB) (although see Cage and Troxell-Whitman 73 for null findings for birth-sex differences in camouflaging in autistic adults). Although autistic individuals DFAB may camouflage more than those DMAB, the association between camouflaging and both anxiety and depression may not be impacted by sex designated at birth and/or gender. Instead, regardless of sex designated at birth/gender, increased camouflaging may be associated with increased anxiety and depression. 32
Depression and anxiety are among the most common co-occurring psychiatric conditions in autistic adults,74,75 and co-occur at significantly elevated rates compared with general population estimates.75–78 Autistic youth and adults DFAB show elevated depressive and anxious symptoms relative to those DMAB.79–81 Further autistic adults DFAB report higher levels of perceived stress than autistic adults DMAB,62,82 and in a study of autistic individuals aged 4–20 years who were psychiatrically hospitalized, autistic females evidenced greater challenges in ER compared with autistic males. 83 As such, sex designated at birth may be a boundary condition on any would-be factors linking camouflaging and depression/anxiety.
Taken together, known associations between (i) ER and both depression and anxiety, (ii) perceived stress and both depression and anxiety, and (iii) camouflaging and both depression and anxiety provide baseline evidence and rationale for exploring more complex modeling of relationships between these constructs. Indeed, it may be that ER and/or perceived stress mediate the association between camouflaging and both depression and anxiety. Thus, this study aimed to examine, for the first time, whether perceived stress and ER challenges play a role in the associations between camouflaging and elevated depression and anxiety in autistic adults.
To probe the potential role of sex designated at birth as a boundary condition, birth-sex was included as a moderator in all models. We hypothesized that (i) higher levels of camouflaging, perceived stress, and emotion dysregulation would each be associated with higher levels of depression and anxiety; (ii) perceived stress and emotion dysregulation would each independently mediate the associations between camouflaging and both anxiety and depression; and (iii) sex designated at birth would moderate the mediations in hypothesis 2, with these relationships showing a stronger effect in those DFAB.
Methods
Participants
Study investigators recruited autistic adult participants through Simons Powering Autism Research (SPARK) 84 Research Match (Project Nos. RM0045Wallace1839 and RM0045Wallace4090). SPARK is part of the Simons Foundation Autism Research Initiative. SPARK maintains an active registry of more than 100,000 autistic persons residing in the United States. Upon enrollment in the registry, SPARK participants complete a questionnaire battery, and they consent to have their de-identified data shared with qualified researchers. SPARK registry participants also consent to receive email communications about studies for which they are eligible.
SPARK's Research Match service connects registry participants with researchers. 85 A qualified researcher with a study protocol that their institution's ethics board has approved can submit an application to recruit participants through Research Match. A committee comprising community and scientific advisors will review their application. 86 If approved, SPARK emails registry participants with information about the study, and registry participants can indicate their interest to learn more about the study and decide whether or not to participate.
SPARK participants included in the analyses reported in this study were part of a broader online study of autistic adult outcomes. After completing the survey battery, participants received $25 USD in the form of an electronic gift card. Study investigators collected these data between December 4, 2019 and January 16, 2020, before the first laboratory-confirmed case of COVID in the United States.
To be included in the broader online study, participants must have been ≥18 years of age, and must have been “independent adults,” defined by SPARK as adults who do not have a court-appointed legal guardian and are thus able to consent for themselves. Based on SPARK's determination of “independent adult,” these participants are unlikely to have a co-occurring intellectual disability. Furthermore, as part of a medical history collected in this study, no participant reported a diagnosis of an intellectual disability.
To be included in the analyses reported in this study, participants must have self-disclosed a community-based professional autism diagnosis, consistent with their inclusion in the SPARK registry. SPARK does not independently confirm self-disclosed professional autism diagnosis. However, SPARK partners with and recruits from expert autism clinical sites, in part, to increase the likelihood that participants have a professional autism diagnosis. 84 A separate validation study examining the electronic medical records for 254 SPARK participants, including “independent” adults, confirmed an autism spectrum diagnosis in 98.8% of the sample. 87 Furthermore, to characterize the current sample, autistic traits were queried using the 28-item Autism-Spectrum Quotient (AQ-28), 88 and consistent with the report of a community-based autism diagnosis by all included participants, 95.2% of participants scored above the AQ-28 cutoff (>65) (Table 1).
Finally, to be included in analyses reported in this study, participants must have completed all of the relevant study measures and have <20% of data missing on each measure. No inclusionary criteria considered self-disclosed history of any psychiatric or medical conditions. Rather, given elevated rates of co-occurring psychiatric and medical conditions74,89–92 among autistic adults, we determined not to exclude participants based on health history to ensure the representativeness of the sample.
The final sample included in this study consisted of 787 autistic adults (59.8% DFAB) aged 18.2–78.2 years.
The study was approved by The George Washington University Institutional Review Board and followed all procedures in accordance with the Declaration of Helsinki.
Measures
In addition to the measures described hereunder, sociodemographic data were collected, including age and sex designated at birth. For the purposes of sample characterization, age of diagnosis, gender identity, ethno-racial identity, and total annual household income are summarized in Table 1.
Camouflaging
Camouflaging was queried using the Camouflaging Autistic Traits Questionnaire (CAT-Q). 7 The CAT-Q is a 25-item survey that quantifies self-reported camouflaging during social interactions (e.g., “In social situations, I feel like I'm ‘performing’ rather than being myself,” “I have spent time learning social skills from television shows and films, and try to use these in my interactions”; “I monitor my body language or facial expressions so that I appear interested by the person I am interacting with.”). 7
Questions are answered on a 7-point Likert scale (from 1 = Strongly disagree to 7 = Strongly agree), and seven items are reverse-scored. Total CAT-Q scores range from 25 to 175, with higher scores indicating more self-reported camouflaging. The CAT-Q has demonstrated good internal consistency and convergent validity as well as acceptable test–retest reliability. 7 Cronbach's alpha for the CAT-Q in the current sample was 0.91. The mean CAT-Q item score served as the independent variable in all analyses.
Depressive symptoms
The 9-item Patient Health Questionnaire (PHQ-9) 93 was used to assess depressive symptomatology and its severity. Participants reported on the presence/frequency of depressive symptoms over the preceding 2-week period using a 4-point Likert scale (0 = Not at all; 1 = Several days; 2 = More than half the days; 3 = Nearly every day). Responses are summed to generate a total score ranging from 0 to 27. Higher scores are indicative of more severe depressive symptomatology.
The PHQ-9 demonstrates criterion and construct validity and high internal consistency (Cronbach's alpha = 0.86–0.89), and test–retest reliability (intraclass correlation = 0.84). 93 Of particular relevance to this study, the PHQ-9 has shown excellent internal consistency (Cronbach's alpha = 0.91) and good convergent validity in autistic adults, metrics that were comparable with those of a nonautistic sample, supporting its utility in samples of autistic adults. 94 Cronbach's alpha for the PHQ-9 in the current sample was 0.90. Mean PHQ-9 item score served as a dependent variable in analyses. See Supplementary Table S1 for further details on mental health-related characteristics of the sample.
Anxiety symptoms
The 7-item Generalized Anxiety Disorder questionnaire (GAD-7) 95 was used to assess anxiety. Using a 4-point Likert scale (0 = Not at all; 1 = Several days; 2 = More than half the days; 3 = Nearly every day), participants reported on the presence/frequency of anxiety during the preceding 2 weeks. A total score is generated by summing responses. Scores range from 0 to 21. Higher scores suggest greater anxious symptomatology. The GAD-7 has demonstrated strong criterion and construct validity, high internal consistency (Cronbach's alpha = 0.92) and good test–retest reliability (intraclass correlation = 0.83). 95 Cronbach's alpha for the GAD-7 in the current sample was 0.92. Mean GAD-7 item score served as a dependent variable in analyses.
ER challenges
The Barkley Deficits in Executive Functioning Scale (BDEFS) 96 is a self-rating questionnaire used to evaluate different aspects of EF in the daily lives of adults. Participants were asked to complete the Self-Regulation of Emotions subscale of the BDEFS (BDEFS-SRE) to measure their ability to manage and control their emotions in everyday life. The BDEFS-SRE approaches emotion (dys)regulation from a two-stage model of emotional self-control, including items that probe both the inhibition of emotional responses and the subsequent regulation of emotional responses. 96
BDEFS-SRE subscale items capture the inhibition of strong emotional responses (e.g., “Quick to get angry or become upset,” “Easily excitable”). Grounded in the model of emotion self-regulation developed by Gross,37,97,98 the subscale also includes items that probe challenges in deploying ER strategies, such as attention deployment (or attentional shifting, e.g., “Cannot seem to distract myself away from whatever is upsetting me emotionally to help calm me down. I can't refocus my mind to a more positive framework”) and cognitive change (or cognitive reappraisal, e.g., “I cannot redefine negative events into more positive viewpoints when I feel strong emotions”; “I am not able to evaluate an emotionally upsetting event more objectively”). 96
The BDEFS-SRE subscale is composed of 13 items and participants respond to each item using a 4-point Likert scale (ranging from 1 = Never or Rarely to 4 = Very Often). The BDEFS-SRE subscale score is calculated by summing responses to the 13 items. Total BDEFS-SRE scores range from 13 to 52, with higher scores reflecting greater challenges in the inhibition and self-regulation of emotion.
The BDEFS was developed and validated for use with adults with ADHD36,96; however, it has been used with autistic adults. 99 Nevertheless, the BDEFS (including the BDEFS-SRE subscale) has not been specifically validated for use with autistic adult samples. In addition, in the development of the BDEFS, to ensure that norms were based on a general population sample of adults, neither persons with “psychiatric, developmental, learning, or medical disorders” nor those using “psychotropic medications” were excluded from the sample.36(p252)
The BDEFS-SRE demonstrates strong internal consistency (Cronbach's alpha = 0.95) and test–retest (r = 0.78) reliabilities. 96 Concurrent validity of the BDEFS has been demonstrated with metrics of adult outcome (e.g., educational history, occupational measures [e.g., self- and employer-rated job performance, duration of employment]). 96 In the current sample, Cronbach's alpha for the BDEFS-SRE was 0.94. The mean BDEFS-SRE item score was used as a mediator variable in analyses.
Perceived stress
The Perceived Stress Scale (PSS)45,100 is one of the most commonly used instruments for the measurement of perceived stress, and has been implemented in samples of autistic adults.61,101,102 The 10-item version of the PSS 100 was used in this study (e.g., “In the last month, how often have you felt difficulties were piling up so high that you could not overcome them,” “In the last month, how often have you felt that you were unable to control the important things in your life,” “In the last month, how often have you felt confident about your ability to handle your personal problems”). The PSS forms a unidimensional scale of global perceived stress. Four of the 10 items are reverse-scored.
Participants respond to each item based on a 5-point Likert scale (ranging from 0 = Never to 4 = Very Often). Total scores range from 0 to 40, with higher scores indicating greater levels of perceived stress. The 10-item PSS has shown good psychometric properties comparable with the longer, 14-item version of the PSS. 103 Broadly, the 10-item PSS shows good internal consistency reliability (Cronbach's alpha = 0.78–0.98).100,104 Furthermore, and of particular relevance to this study, within a sample of autistic adults without co-occurring intellectual disability, the PSS has demonstrated good internal consistency reliability (Cronbach's alpha = 0.87). 61 Cronbach's alpha for the PSS in the current sample was 0.89. The mean PSS item score was used as a mediator variable in analyses.
Autistic traits
Participants completed the AQ-28, which queries autistic traits using a 4-point Likert scale (1 = definitely agree, 4 = definitely disagree). 88 Total scores range from 28 to 112, with higher scores reflecting greater autistic traits. The AQ-28 total score has shown acceptable to good internal consistency, and good validity and reliability within clinical samples. 88 To further characterize the current sample, we also determined the number of participants scoring above the AQ-28 cutoff (>65), as described in the Participants section earlier. Cronbach's alpha for the AQ-28 total score in the current sample was 0.85. The mean AQ-28 item score was used as a covariate in all models.
Statistical approach
Statistical analyses were conducted in R (v.3.6.3), and moderated mediation analyses were implemented using the PROCESS package. 105 Moderated mediation modeling is an appropriate statistical approach for various types of data, including data that are cross-sectional and/or correlational.105(pp.16–19) Specifically, we follow expert consensus in the use of mediation in cross-sectional data, including Hayes and Rockwood, 106 Hayes, 105 and others.
These statisticians contend that mediation as a statistical modeling approach is agnostic with respect to the nature of data analyzed, including whether data are correlational versus experimental or cross-sectional versus longitudinal. Methods such as mediation can be used in cross-sectional data sets without concern about implementing the statistical method itself; however, as with all statistical modeling, care must be taken in appropriately framing the interpretation of such results, a point we return to in the Discussion section.
Four conditional process models (or moderated mediation models) were tested (PROCESS Model 59; Fig. 1). In all models, the mean CAT-Q item score was the independent variable, and the moderator variable was sex designated as birth. Sex was dummy coded as “0, 1” with male coded as the reference level (i.e., male coded as “0”). Following previous studies, 66 age at survey completion and mean AQ-28 item score were used as covariates in all models. The dependent variable was PHQ-9 or GAD-7 total score, and the mediator variable was the BDEFS-SRE or PSS score. Modeling implemented bootstrap confidence intervals (CIs) using 10,000 bootstrap samples. CIs that did not include zero were considered significant.
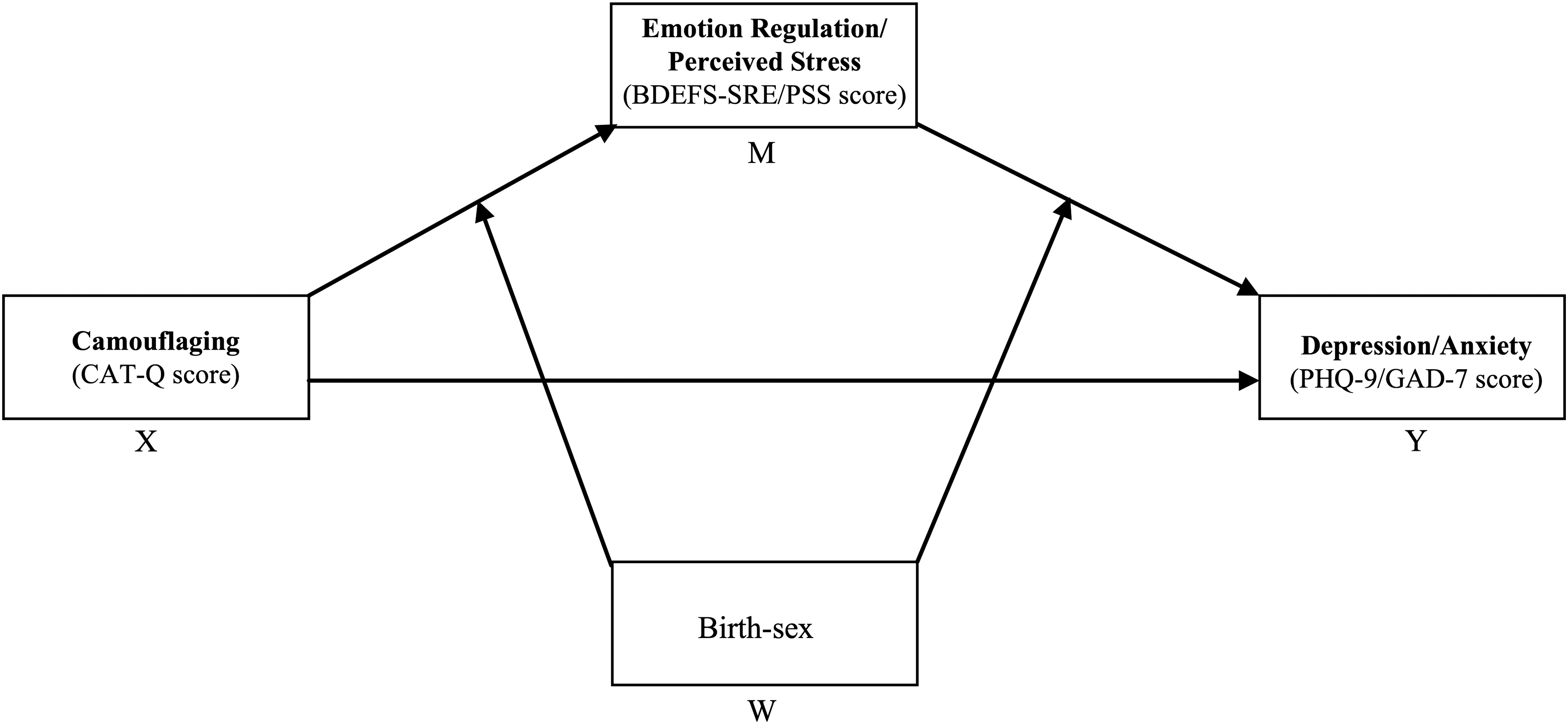
Conceptual diagram representing models tested (simple mediation model with all three paths moderated by birth-sex).
For each model, items from each measure were compared with items from other measures included within that same model (e.g., for a model including CAT-Q, GAD-7, and BDEFS-SRE, items from the GAD-7 were compared with items from the CAT-Q and BDEFS-SRE) to determine whether items between any two measures substantively overlapped in content and/or wording. A single item from the BDEFS-SRE (“Quick to get angry or become upset.”) was determined to substantively overlap with a single item from the GAD-7 (“Becoming easily annoyed or irritable.”); and a single item from the PSS (“In the last month, how often have you felt nervous and stressed.”) was determined to substantively overlap with an item from the GAD-7 (“Feeling nervous, anxious or on edge.”).
Mean items scores for the BDEFS-SRE and PSS were thus recomputed without the relevant item from each survey. In models for which GAD-7 was the dependent variable and BDEFS-SRE or PSS was the mediator variable, the recomputed mean item score was used. For the sake of completeness, models run with the overlapping items as indicated earlier are reported in the Supplementary Materials (see Supplementary Tables S3 and S4, and Supplementary Fig. S1).
Results
Results from all four moderated mediation models are presented in Tables 2 and 3 and Figure 2.
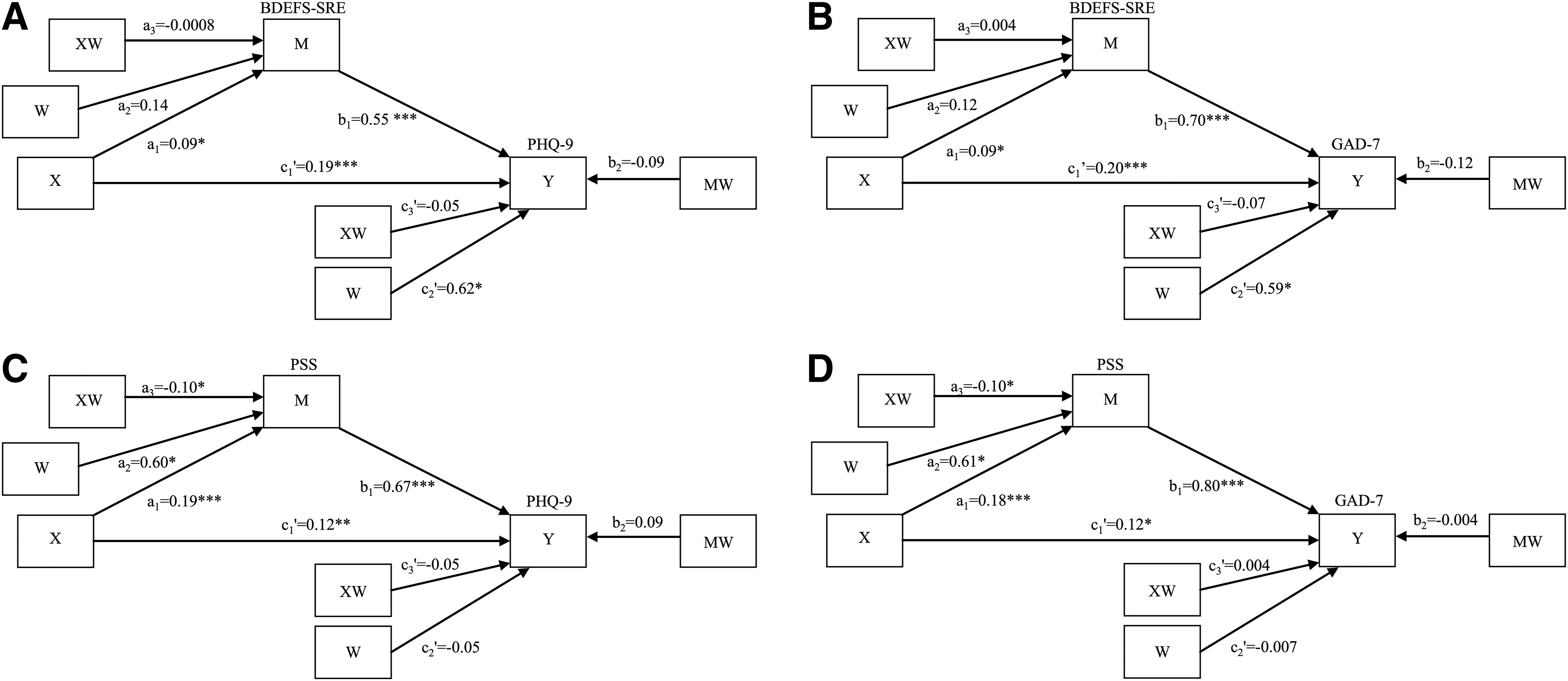
Statistical diagrams of four moderated mediation models of the association between camouflaging and depression
Model Coefficients for the Four Moderated Mediation Models with Two Covariates
Birth-sex was coded as male = 0, female = 1. Regression coefficients are unstandardized; standardized coefficients are not produced in conditional process models.
C, covariate; Coeff., regression coefficient; ER, emotion regulation; M, mediator variable; SE, standard error; W, moderator variable; X, independent variable; Y, dependent variable.
Conditional Direct and Indirect Effects for the Conditional Process Models in Figure 1
Equations show the computation of model regression coefficients for the relevant indirect and direct effects. “0” and “1” correspond to birth-sex (W), coded as 0 = male, 1 = female. Covariates for all models were AQ-28 and age.
Direct and indirect effects of camouflaging on depression: ER challenges as mediator
In models with ER challenges as mediator, camouflaging showed a significant direct effect on depressive symptomatology [males: t(779) = 5.11, p < 0.0001, 95% CI = 0.12 to 0.27; females: t(779) = 3.30, p = 0.001, 95% CI = 0.04 to 0.16]; this direct effect was not significantly moderated by birth-sex [t(779) = −1.95, p = 0.052, 95% CI = −0.19 to 0.001].
Mediation of the association between camouflaging and depression by ER challenges was significant (bootstrap 95% CIs between 0.003 and 0.098 for males, and between 0.009 and 0.074 for females); however, there was no significant moderated mediation, as bootstrap CIs included zero (−0.07 to 0.05), reflecting no significant impact of birth-sex on the direction or strength of the indirect effect.
Direct and indirect effects of camouflaging on anxiety: ER challenges as mediator
In models with ER challenges as mediator, camouflaging showed a significant direct effect on anxious symptomatology [males: t(779) = 5.00, p < 0.00001, 95% CI = 0.12 to 0.28; females: t(779) = 4.07, p = 0.0001, 95% CI = 0.07 to 0.19]; this direct effect was not significantly moderated by birth-sex [t(779) = −1.37, p = 0.17, 95% CI = −0.17 to 0.03].
Mediation of the association between camouflaging and anxiety by ER challenges was significant (bootstrap 95% CIs between 0.005 and 0.13 for males and 0.02 and 0.10 for females); there was no significant moderated mediation, however, as bootstrap CIs included zero (−0.08 to 0.063), indicative of no significant impact of birth-sex on the strength or direction of the indirect effect.
Direct and indirect effects of camouflaging on depression: perceived stress as mediator
In models with perceived stress as mediator, camouflaging showed a significant direct effect on depressive symptomatology [males: t(779) = 3.52, p = 0.0005, 95% CI = 0.05 to 0.18; females: t(779) = 2.61, p = 0.009, 95% CI = 0.02 to 0.12]; this direct effect was not significantly moderated by birth-sex [t(779) = −1.19, p = 0.24, 95% CI = −0.13 to 0.03].
Mediation of the association between camouflaging and depression by perceived stress was significant (bootstrap 95% CIs between 0.08 and 0.18 for males, and 0.02 and 0.11 for females); however, there was no significant moderation of this mediation, as bootstrap CIs included zero (−0.13 to 0.01), indicating that the direction and strength of the indirect effect were not significantly impacted by birth-sex.
Direct and indirect effects of camouflaging on anxiety: perceived stress as mediator
In models with perceived stress as mediator, camouflaging showed a significant direct effect on anxious symptomatology [males: t(779) = 3.2250, p = 0.0013, 95% CI = 0.05 to 0.19; females: t(779) = 4.1413, p < 0.0001, 95% CI = 0.06 to 0.18]; this direct effect was not significantly moderated by birth-sex [t(779) = 0.0084, p = 0.99, 95% CI = −0.09 to 0.09]. Mediation of the association between camouflaging and anxiety by perceived stress was significant (bootstrap 95% CIs between 0.08 and 0.21 for males, and between 0.02 and 0.11 for females); and this mediation was moderated by birth-sex with the effect entirely below zero (95% bootstrap CI = −0.16 to −0.01), suggesting male sex at birth is associated with a weaker indirect effect.
Discussion
In a large sample of autistic adults, this cross-sectional study examined two potential mediators of the associations of camouflaging with depression and anxiety: ER challenges and perceived stress. To our knowledge, this is the first study to illuminate potential mediators of the associations between self-reported camouflaging and poorer mental health. As hypothesized, we found that more camouflaging, increased ER challenges, and higher levels of perceived stress were each associated with both greater depressive and anxious symptomatology.
Specifically, significant direct effects of camouflaging on depressive and anxious symptomatology were observed in all models, and the path from each of the mediator variables (ER challenges and perceived stress) to the dependent variables (depression and anxiety) was significant in all models. These effects are consistent with separate threads of quantitative research pointing to associations between (i) camouflaging and anxiety/depression,17,32,71,73 (ii) ER challenges and anxiety/depression,49,56,58 and elevated perceived stress and poorer psychological quality of life 62 in autistic individuals.
A burgeoning literature shows increased experiences of stress and the detrimental impacts of this increased stress on the mental health of autistic adults. These experiences of stress include greater risk for lifetime trauma as well as elevated everyday experiences of stress. Autistic individuals experience more traumatic life events relative to neurotypical individuals. These traumatic events include adverse childhood experiences (e.g., bullying, physical abuse, sexual abuse, and other forms of maltreatment),107–110 experiences of interpersonal trauma in adulthood, such as bullying and harassment,111–113 and physical and sexual victimization.113–115
In addition to increased exposure to trauma, autistic adults show overall greater responsivity to major stressors, relative to neurotypical adults, and they specifically report greater perceived severity of stress in response to stressors characterized by change, humiliation, and physical danger. 116 Autistic adults also report elevated levels of perceived stress relative to neurotypical adults.59–62 Among autistic adults, perceived stress is associated with poorer subjective quality of life,62,101 decreased social functioning, 101 and decreased independence in the performance of activities of daily living. 62
Increased mental health problems in autistic people may, in part, be explained by experiences of minority stress, or the exposure to excess social stressors, such as stigma, associated with a minority (i.e., neurominority) identity. 117 Although we did not measure minority stress in this study, perceived stress (which assesses a person's experiences of everyday stress) may nevertheless be indexing facets of minority stress, alongside other stressors (e.g., financial stress, which may be related to elevated rates of under- and unemployment in autistic adults).118–120
Camouflaging or concealing one's neurominority identity is one way in which autistic people may cope with stigma 121 ; however, not disclosing prevents autistic people from accessing legally protected supports and accommodations within academic, workplace, and health care settings.122–125 Some autistic people report that in weighing whether to conceal or disclose their autistic identity, they face a double bind: either decision brings with it possible experiences of negative stereotypes, stigma, social exclusion, and victimization. 126 This described double bind underscores that camouflaging, as the concealment of a minority identity, occurs within the context of a neurotypical-majority society and pressures exerted by that society. 14
Setting aside any potential burdens of camouflaging, the contexts that elicit camouflaging may themselves be stressful and overtaxing because of core autism traits and the challenges these traits can present in certain settings. For example, a job interview, a professional conference, or a party involves social demands, may include novel locations and people, and may occur in overwhelming sensory environs (e.g., in brightly lit, crowded, or noisy settings).
These contexts may thus be overwhelming and stressful for an autistic person whether that person camouflages or not. Suppressing “autistic” behaviors that may be evaluated negatively by others including stimming (which autistic people describe as beneficial and as serving an emotion regulatory function, particularly in environments that are sensorily overstimulating 127 ), in these contexts may constrain autistic people's ability to upregulate positive emotions and downregulate negative emotions, making such settings still more stressful.
The overall stress of social situations and difficulties engaging ER strategies while camouflaging in these settings may be further exacerbated by challenges in EF, including difficulties with working memory, attention shifting, and inhibitory control.128,129 Broadly, better EF predicts more camouflaging in autistic persons, suggesting that EF skills are needed and afford for camouflaging. 70 Based on autistic people's descriptions of their everyday experiences, camouflaging is resource-greedy, taxing top-down EF capabilities.6,63,64
Camouflaging may, therefore, draw down resources that are already relatively limited, particularly if there is insufficient time to recover from settings in which one camouflages, as suggested by autobiographical accounts and qualitative studies of “autistic burnout.”31,65 The resulting cycle of everyday stress and emotion dysregulation, catalyzed by the nexus of core autism traits, EF challenges and camouflaging, may contribute to elevated rates of anxiety and depression in autistic people.
Clinical implications
The results reported in this study, indicating that perceived stress and ER challenges each mediate associations of camouflaging with both depression and anxiety, have clinical implications. In particular, considering that autistic (vs. neurotypical) people face increased minority stress, as well as lifetime trauma exposure, and higher levels of day-to-day stress, these results indicate that clinicians should consider the role of the person–environment fit in autistic adults presenting with depression and/or anxiety. Elevated levels of camouflaging alongside depressive and/or anxious symptomatology may identify risk for poor person–environment fit and may recommend the improvement of this fit, or interventions that reduce stress or improve ER (or some combination of all of these).
For autistic adults, consideration of transactions with potentially invalidating environments, 130 which may drive camouflaging, 14 may be of particular importance in reducing depressive and anxious symptomatology. Understanding the frequency with which autistic adults camouflage and the contexts in which they camouflage in their day-to-day lives may help inform ways to improve the person–environment fit. 73 For autistic adults who report camouflaging to avoid bullying or discrimination, 73 or who are employed in a setting in which social demands are high and are considered necessary for career success and/or advancement, improving the person–environment fit may decrease external pressures to camouflage 131 and thereby improve mental health.
Helping these autistic people to seek out legally protected accommodations or even to seek out employment settings in which neurodivergence is desired rather than merely accommodated could improve the person–environment fit. Nevertheless, it is essential to recognize each person should have autonomy and choice in disclosing their autism or seeking a different employment setting. In addition, not all persons will have access to resources (e.g., financial) that allow for these changes in their environment.
Complex dynamics exist among camouflaging, autistic identity, and disclosure 132 ; however, both autistic individuals' greater awareness of autism-related stigma and higher self-reported camouflaging are associated with poorer psychological well-being. Both less autism acceptance from others (family, friends, and society) and less self-acceptance of autism predict higher levels of depressive symptomatology. 33 Conversely, a positive sense of autism identity and affiliation with the broader community of autistic people are associated with greater psychological well-being. 133 Increasing acceptance by others will help autistic adults decrease self-stigma and foster a positive sense of identity.
At the level of the individual, both perceived stress and ER may also serve as potential therapeutic targets for interventions in autistic adults. Reductions in perceived stress are associated with improved quality of life and lower levels of mental health problems in autistic adults.134–136 The use of mindfulness-based therapies, cognitive-behavior therapy, and dialectical behavior therapy may help moderate ER challenges in autistic individuals.137,138
As hypothesized, the significant mediation of the association between camouflaging and anxiety by perceived stress was significantly moderated by birth-sex. Contrary to our hypotheses, sex designated at birth did not moderate any of the other mediations tested. This was somewhat unexpected given studies showing that relative to autistic persons DMAB, those DFAB report higher levels of camouflaging, perceived stress, depression, and anxiety. These literatures, however, have largely examined designated sex and its associations with the constructs of camouflaging, ER challenges, perceived stress, depression, and anxiety separately.
In this study, DFAB do report more camouflaging, higher levels of perceived stress, greater challenges with ER, and higher anxious and depressive symptomology relative to those DMAB (see Supplementary Table S2 for correlations between designated sex and each of these variables). Notably, however, and in contrast to previous research, this study sought to model the relationships among these variables and to specifically interrogate the role of designated sex as a variable that interacts with these possible relationships.
Prior research has shown that, although autistic females report more camouflaging than autistic males, predictors (e.g., loneliness) and “outcomes” of camouflaging (e.g., psychological quality of life) do not differ based on designated-sex. 139 Thus, camouflaging does not appear to differentially impact well-being based on birth-sex; rather, for both autistic females and autistic males, greater camouflaging is associated with elevated depression and anxiety. These findings underscore the importance of not equating camouflaging with any particular “presentation” of autism (e.g., the so-called “female autism phenotype”).12,14
Strengths and limitations
Strengths of this study include a large sample of autistic adults (N = 787) that spans younger, middle, and older adulthood. Although this study did not examine age as a variable of interest, the inclusion of autistic adults from younger to older adulthood is important, given the relative paucity of research on autism in adulthood and the critical dearth of such research that includes autistic adults aged ≥50 years.140,141 In the current sample 48.4% (n = 381) of autistic adults were aged ≥40 years, and 24.3% (n = 191) were aged ≥50 years.
This study had limitations. The sample of autistic adults was predominantly White (∼83%), non-Hispanic/Latinx (∼90%). This lack of ethnoracial representativeness limits the generalizability of this study's findings and underscores the need for the recruitment of persons from groups that have been historically underrepresented in autism research.142,143
Camouflaging in this study was operationalized using a self-report measure. However, camouflaging has been operationalized in other ways. For example, discrepancy-based approaches operationalize camouflaging as a difference between an “external” presentation of autistic traits and the “internal” experience or “intrinsic” status of these traits.11,144 In addition, the self-report camouflaging measure used in this study, although widely implemented in the literature, likely does not probe all facets of camouflaging (e.g., seeking autism-friendly environments, as described in Ai et al. 22 ).
Importantly, self-report measures are unlikely to capture aspects of camouflaging that are below the level of conscious awareness 14 and potentially unavailable for self-report, including subtleties of linguistic production, 145 and differences in pragmatic communication, such as gesture use, 9 the synchronization of nonverbal and verbal communicative behaviors, 146 and use of pragmatic markers, 30 which may “hide” autistic traits in some individuals. Thus, there may be other components of camouflaging that are relevant and that would help further expand our knowledge of associations of camouflaging with anxiety and depression.
The data analyzed in this study are cross-sectional. As indicated in the Methods section, the statistical analyses using conditional process modeling implemented in this study are appropriate for these cross-sectional data.105(pp.16–19) However, and as with all studies that examine cross-sectional and/or correlational data (regardless of statistical approach), care is necessary in the interpretation of the results reported in this study. We cannot make claims regarding causality or the directionally of observed associations. For instance, we cannot claim that increased ER challenges are a causal factor in the association between camouflaging and mental health problems; however, we can make claims based on the mediation results reported in this study that nevertheless advance our understanding of associations among the variables examined.
It is important to note that limitations around causal interpretations are not restricted to mediation analyses; rather these apply to many types of analyses, including regression modeling. Thus, in discussing the results from the direct or c′ path (i.e., the path from X to Y), which are results from an ordinary least squares regression model (Table 2 and Fig. 2), we similarly cannot claim that camouflaging causes depression or anxiety. Future work with longitudinal data sets will help to overcome some of these limitations on the interpretation of associations between camouflaging and mental health and illuminate the potential roles of the mediators identified in this study.
Understanding factors that contribute to elevated rates of co-occurring anxious and depressive disorders and symptomatology in autistic adults is essential to improving mental health and overall quality of life. Statistical modeling that incorporates other potential variables associated with camouflaging (e.g., stigma), as well as their mediators and moderators, is needed to provide a comprehensive picture of this complex phenomenon and its associations with mental health. Such modeling may also help us to identify specific roles that a neurotypical-majority society can play in ameliorating some of these negative impacts.130,147
Future studies should also examine cultural contexts of camouflaging and characterize such contexts within statistical modeling. Such cultural contexts as these may relate to different community identities, including race and ethnicity. In addition, future work should examine how co-occurring conditions, including psychiatric conditions, and multiple disability status may impact camouflaging, perceived stress, and emotional health.
This study included sex designated at birth in all models; however, future studies should probe the potential role of gender identity. Gender-diverse identities may be more common among autistic relative to neurotypical persons, and autistic persons are proportionally overrepresented within gender-diverse populations.148,149 Thus, given the independent streams of evidence indicating (i) increased prevalence of anxiety and depression among autistic adults,74,75 (ii) overall increased prevalence of anxiety and depression among gender-diverse relative to cisgender people,150–152 and elevated rates of mental health challenges including depression and anxiety in gender-diverse autistic people,153,154 the examination of gender identity in the contexts of camouflaging and mental health is key.
Finally, and as also noted earlier, to better understand camouflaging and its associations with mental health, longitudinal studies are needed. These studies will inform temporal precedence and may also help to reveal potential developmental and/or age-graded effects of camouflaging, which could in turn inform ways to promote resilience and decrease stress during key developmental periods (e.g., adolescence) when risk for the onset of mental health problems may be particularly high.
Footnotes
Acknowledgments
We are grateful to the autistic adults who participated through SPARK. We also wish to express our gratitude to the SPARK clinical sites, and SPARK staff. We appreciate obtaining access to recruit participants through SPARK Research Match on SFARI Base.
Authorship Confirmation Statement
All authors contributed to the conception of this study. G.L.W. and N.L.R. contributed data for analysis. G.A.M. conducted data analysis. G.A.M., L.Y.S., N.L.R., and G.L.W. conducted interpretation of results. All authors revised the article and approved of the final version for publication. The article has been submitted solely to this journal and is not published, in press, or submitted elsewhere.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by an Autism Speaks Postdoctoral Fellowship (Grant ID 11808) to Goldie A. McQuaid, and by start-up funds from The George Washington University to Gregory L. Wallace. Additional support was provided by the National Institutes of Health to Goldie A. McQuaid (under Grants R01MH100028 and K01MH129622), Nancy Raitano Lee (under Grants R21HD100997 and R21HD106164), and Gregory L. Wallace (under Grants R01MH100028, R21HD106164, R21MH129777, P50HD111142, and R01MH133838).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.