
Abstract
Background:
Decreased sound tolerance (DST) is an increased sensitivity to sound at levels that would not bother most people. DST is highly prevalent in autistic adults; however, the extent to which DST differs across autistic and non-autistic adults is uncertain. This study explores multiple domains of DST symptoms and the severity of DST symptoms, as well as the behavioral reactions and coping strategies adopted to manage DST in both autistic and non-autistic adults. Lastly relationships between DST, autism characteristics, mental health, and quality of life were explored.
Methods:
This study used online surveys to investigate the characteristics of DST in 77 autistic and 128 non-autistic adults who self-report DST, as well as the relationship between DST and autistic characteristics, mental health, and quality of life.
Results:
The results of this study indicated that clinically relevant misophonia, an aversion to specific sounds, was more prevalent in the sample of autistic adults who self-reported DST. Similarly, clinically relevant hyperacusis, a reduced tolerance to everyday sounds at volumes that would not be distressing to most people, was also more prevalent in the sample of autistic adults who self-reported DST. Across the entire sample, misophonia symptoms were associated with more autistic traits and higher anxiety, whereas hyperacusis symptom severity was associated with more autistic traits, higher anxiety and depression symptoms, and poorer quality of life.
Conclusion:
Although clinical cases of misophonia and hyperacusis were more prevalent in our sample of autistic adults who self-reported DST, these forms of DST may be related in similar ways to mental health and quality of life of both autistic and non-autistic adults. Future work should focus on differentiating the subtypes of DST to facilitate the development of treatments that specifically target the symptoms of each subtype (i.e., misophonia, and hyperacusis) rather than treating DST as a homogeneous problem.
Community Brief
Why is this an important issue?
Many autistic adults find sounds to be distressing. However, we are unsure whether these experiences with sound are similar to the experiences of non-autistic adults. We also don’t know if the distress caused by sound has similar effects on anxiety, depression, and quality of life for autistic and non-autistic adults.
What was the purpose of this study?
The purpose of this study was to better understand how sounds influence autistic and non-autistic adults who report sounds to be distressing. Specifically we were interested in the types of sounds and general features of sounds that are distressing. We also wanted to know how these adults react to sound and what they try to do to reduce negative reactions to sound. We were interested in how the distress created by sound might be related to autism characteristics, anxiety, depression, and quality of life.
What did the researchers do?
We had 77 autistic and 94 non-autistic adults who self-reported a decreased tolerance to sound fill out questionnaires online. These questionnaires asked about experiences with sound, autistic characteristics, anxiety, depression, and quality of life.
What were the results of the study?
The results indicated that misophonia, a dislike of specific trigger sounds, was worse in autistic adults. Hyperacusis, or suffering caused by everyday sounds at a loudness that does not bother most people, was also worse in autistic adults. Misophonia symptoms were related to anxiety in both autistic and non-autistic adults. Hyperacusis symptoms were related to autism characteristics, anxiety, and depression, and a lower quality of life in both autistic and non-autistic adults.
What do these findings add to what was already known?
These findings tell us that the kinds of sounds that are troublesome and the reactions adults have to sound are qualitatively similar for autistic and non-autistic adults, with autistic adults having more severe symptoms. These findings also tell us that decreased sound tolerance may affect mental health and quality of life. However, as we looked at associations between different variables, we cannot say that decreased sound tolerance is causing poor mental health and reduced quality of life; rather these findings just reveal that they are related.
What are potential weaknesses in the study?
Our data were collected online, so we could not make sure that our autistic participants had official diagnoses. Online collection also made us unable to test participants’ hearing. Most of our sample was female. We are unsure if this is because more females find sound distressing, or more females are willing to complete online surveys. Lastly, because participants were describing their trouble with sound, we were not objectively measuring reactions to sound; it is possible that the observed findings might be the result of how people chose to describe their experiences. The instruments used to measure hyperacusis and misophonia have not been validated on autistic samples. Future work using measures validated on autistic samples could reveal different patterns of results.
How will these findings help autistic adults now or in the future?
These findings explain the types and features of sounds that cause the most trouble for autistic people. These findings also suggest that sound may have a big effect on the mental health and quality of life of autistic people. As such, these findings provide important information that can be used to help people to create more sensory-friendly environments that will be of great benefit to autistic people with sound sensitivities.
Background
In our daily lives, we function in rich, complex, and unpredictable sensory environments. For people diagnosed with autism, a neurodevelopmental condition associated with sensory processing differences, these environments can be highly distressing.1,2 In fact, sensory processing differences experienced by autistic individuals have been linked to difficulties with cognitive, social, and occupational functioning, as well as emotional well-being and sleep disturbances.3–7 A reduced tolerance to everyday sounds, or decreased sound tolerance (DST), is the most common sensory challenge experienced by autistic individuals,5,8 with an estimated prevalence of between 38 and 45 percent. 7 These rates are staggeringly higher than self-reported sound intolerance in non-autistic people, which has been estimated between 2 and 6 percent.9,10 Despite the high prevalence and debilitating nature of DST in autism, it is poorly understood.
Some of the confusion regarding DST can be attributed to the fact that DST is a broad term that describes people who show unusual responses to sound without any corresponding differences in hearing thresholds. 11 However, these sounds can vary vastly in their sound properties, as well as in the emotional and behavioral reactions they elicit. For example, one person with DST might experience pain in response to sounds in general, while another may experience high levels of irritation to only specific sounds. 2 Furthermore, given that there are no widely accepted diagnostic criteria, 12 etiology, cure, or treatment plan for DST, it remains unknown if these varied presentations of DST represent the same underlying neurophysiological mechanism.
To parse the heterogeneity in the characteristics of DST, attempts have been made to classify different presentations of DST. For example, loudness hyperacusis, pain hyperacusis, annoyance hyperacusis, and fear hyperacusis have been used to describe the different clinical presentations of DST, with hyperacusis considered synonymous with DST. 13 More recently, the DST subtypes of hyperacusis, misophonia, and phonophobia have been adopted,3,6 where hyperacusis refers specifically to the DST associated with increased perceived loudness, while annoyance and fear hyperacusis are classified as misophonia and phonophobia, respectively. Under this framework, hyperacusis is reduced tolerance to everyday sounds at volumes that would not be distressing to most individuals. 6 Misophonia is an acquired neuropsychiatric condition where specific trigger sounds, such as chewing, sniffing, and tapping, elicit excessive negative reactions14–16 and increased autonomic arousal. 17 Phonophobia is a fear of specific sounds or classes of sounds that often results in preemptive avoidance behaviors to avoid the feared sound.6,18 Given that clear definitions of these subtypes are only beginning to emerge, the behavioral and emotional characteristics of these subtypes of DST need further investigation.
DST was recently investigated in a large sample (n = 88) of parents who reported on the sound intolerances of their autistic children. 2 Loud (or sounds that are perceived as loud), unexpected, high-pitched, and human-produced sounds were endorsed as being distressing for the children. Furthermore, parents reported a variety of behavioral reactions such as yelling and covering of ears, and emotional reactions such as stress, irritation, and anxiety. The description of these trigger sounds and their behavioral and emotional reactions suggests that the sample likely contained autistic children with hyperacusis and/or misophonia, although validated measures assessing symptoms of these conditions were not administered. Parents reported on the strategies their children adopted to cope with distressing sounds, with a high endorsement of behavioral strategies such as taking breaks and avoiding noisy settings. Although parents stressed that these strategies helped manage their child’s reactions to sound, they also indicated that these strategies impacted their child’s participation at home, at school, and in the community. Although this study highlighted the behavioral and emotional characteristics, and the impacts of DST on autistic children, less is known about DST in autistic adults.
A recent meta-analysis suggests that the lifetime prevalence of hyperacusis in autistic people is 60.58%, with prevalence increasing with age. 7 The results of this recent meta-analysis underscore the high prevalence of DST in autistic adults and emphasize the importance of further research to help understand and classify DST in autistic adults. Thus, the first aim of the current study was to explore multiple domains of DST symptoms in autistic adults. We specifically examined misophonia and hyperacusis symptoms in a sample of autistic adults who report experiencing DST and compared them with a sample of non-autistic adults with DST. The second aim of this study was to explore the relationship between misophonia and hyperacusis symptoms and mental health, quality of life, and autism characteristics. By comparing autistic and non-autistic adults, our aim was to gain a better understanding of whether these different forms of DST are experienced differently across these populations. Ultimately, these data may help to better inform research on the causes, prevention, and treatment of DST.
Methods
This study is part of a larger research program that was developed in consultation with an advisory group that comprised autistic researchers, autistic community members, parents, and nonprofit stakeholders. Although autistic adults were not involved in the specific design of this study or the data collection, analyses, or interpretation of the data reported in this article, this advisory group was integral to obtaining the funding for this research program and shaping the research questions being addressed in this article.
Participants
A total of 77 autistic adults (mean [M] age = 33.00 years, standard deviation [SD] = 11.53) and 128 non-autistic adults from the community (M age = 32.68 years, SD = 12.78) participated in the current study (see Table 1 for participant demographic information). Note, one autistic respondent omitted their age and thus was excluded from any analyses that included age. Autism diagnosis was self-reported. We recruited both autistic and non-autistic participants from the community using online advertisements. Inclusion criteria for the current study required that participants self-report having decreased tolerance of sound, be at least 19 years old, and have access to a device capable of completing an online survey. To probe for DST, we asked participants to indicate “which of the following best describes your negative reaction to sound,” using a 4-point Likert scale, with 0 indicating no negative reactions to sound. We excluded participants who rated their negative reaction to sound as a 0. This resulted in the exclusion of 1 autistic and 35 non-autistic respondents from further analyses to create samples that only included participants who reported negative reactions to sound. We sent participants meeting these criteria an online survey where they read and provided informed consent before proceeding with the study. Upon completion, participants had the option to be entered into a draw for a $100 gift card of their choice. All procedures were approved by the Simon Fraser University Research Ethics Board and were in accordance with the World Medical Association 2013 Declaration of Helsinki.
Demographic Information for Autistic and Non-Autistic Samples
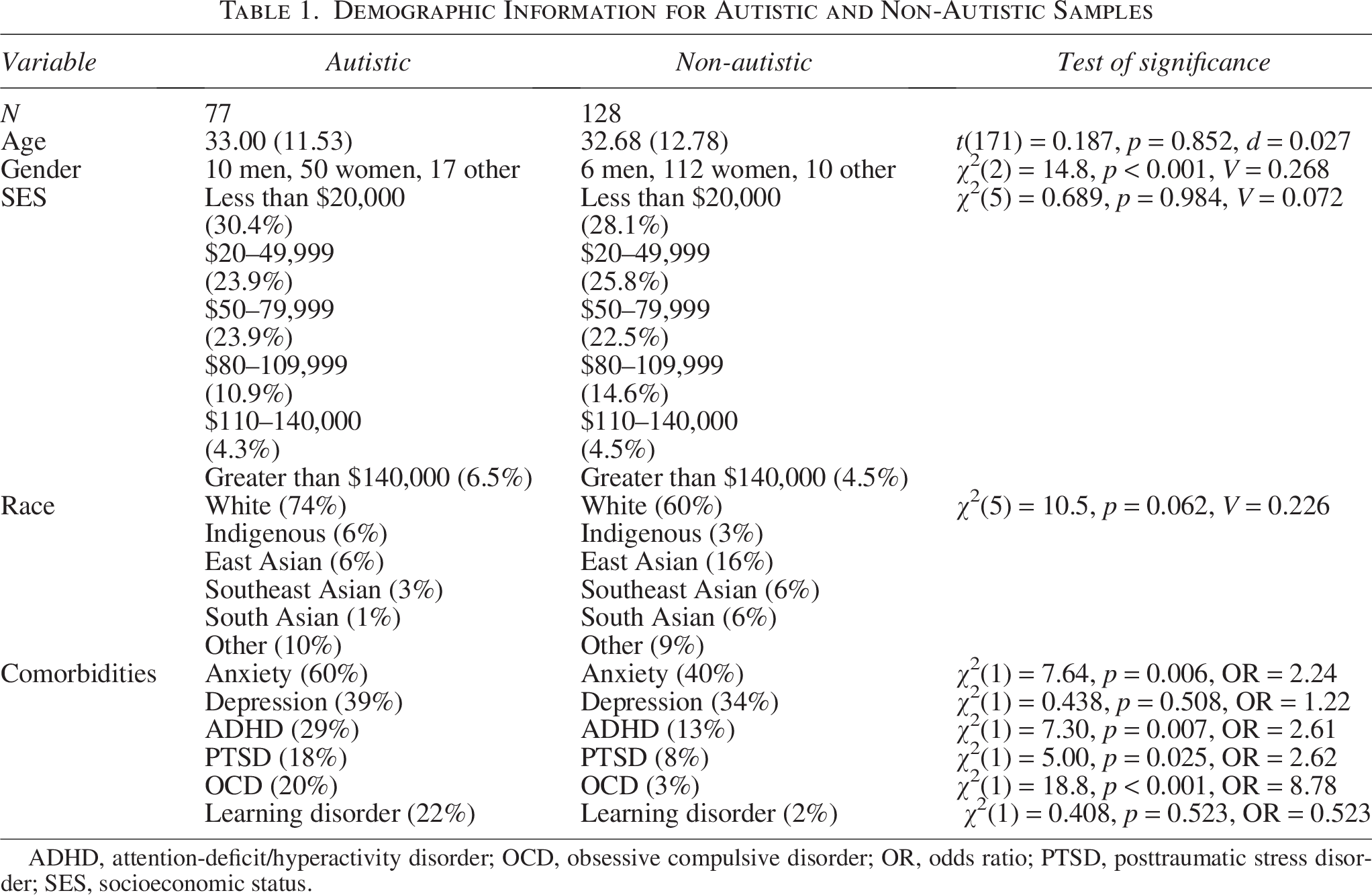
ADHD, attention-deficit/hyperactivity disorder; OCD, obsessive compulsive disorder; OR, odds ratio; PTSD, posttraumatic stress disorder; SES, socioeconomic status.
Measures
See Table 2 for the internal consistency of all measures used in the current study and Supplementary Data S1 for additional details on the psychometric properties of these measures.
Comparison of Study Measures Across Autistic and Non-Autistic Participants

AQ, Autism-Spectrum Quotient; HIS, Inventory of Hyperacusis Symptoms; MQ, Misophonia Questionnaire; PHQ, Patient Health Questionnaire (PHQ); WHOQoL, World Health Organization Quality of Life Questionnaire.
Autistic traits
The Autism-Spectrum Quotient (AQ) 19 is a 50-item questionnaire assessing self-reported autistic traits. Higher scores represent higher levels of self-reported autistic traits. A score of 29 and higher has been suggested to differentiate autistic adults from non-autistic adults. 20
DST questionnaire
Participants completed an in-house questionnaire, adapted, in part, from Law et al. (2016) 21 , designed to assess aspects of their DST (see Supplementary Data S1). This questionnaire probed participants about their emotional reactions to sounds, the types of sounds (both specific and broad) that cause them to react negatively, how their DST impacts their lives, and solutions they wish existed to help them cope with their DST.
Misophonia symptoms
The Misophonia Questionnaire (MQ) 22 , 23 assessed the presence of misophonia symptoms, associated emotions and behaviors arising from experiences with the sounds the respondent is sensitive to, and an overall self-report rating of sound sensitivity severity. In the first section of the MQ, the Misophonia Symptom Scale, respondents rate the extent to which they are sensitive to seven specific sounds, such as throat sounds, nasal sounds, and people eating. If the participants endorse sensitivity to one or more of the sounds in the first section of the MQ, they are asked to complete the second section. The second section, named the Misophonia Emotions and Behaviors Scale, asks participants about their associated emotional and behavioral reactions to the sounds endorsed in the first section. These sections yield an MQ total score out of 68, where higher scores correspond to greater severity of misophonia symptoms. The third section of the MQ, the Misophonia Severity Scale, asks participants to self-select the severity of their sound sensitivities, ranging from 1 (minimal) to 15 (very severe). Respondents who select a 7 or higher on the Misophonia Severity Scale and have an average item score of 2 or higher on the MQ Emotions and Behaviors Scale are identified as having clinically significant misophonia symptoms. 24
Hyperacusis symptoms
The Inventory of Hyperacusis Symptoms (IHS) 25 is a 25-item questionnaire assessing the extent to which participants endorse hyperacusis symptoms, namely loudness, annoyance, fear, and pain arising from their experiences with sounds. The IHS yields a total score out of 100, where higher total scores correspond to greater severity of hyperacusis symptoms. A total score of 75 is considered a cutoff for the clinical presence of hyperacusis.
Anxiety and depression
The Patient Health Questionnaire for Depression and Anxiety (PHQ-4) 26 was administered to all participants. The PHQ-4 contains four questions in total: two measuring anxiety and two measuring depression symptoms. Respondents rate how often they have been bothered by specific problems over the past two weeks. The PHQ-4 not only yields a total score out of 12 but also yields an anxiety subscale and a depression subscale.
Quality of life
The quality of life of all participants was assessed using the World Health Organization Brief Quality of Life Scale (WHOQoL-BREF). The WHOQoL-BREF contains 26 questions and yields four domain scores representing various areas of well-being: physical health, psychological, social relationships, and environment. In addition, individual questions probe the respondents’ overall quality of life and quality of health. An average quality-of-life score was also calculated by taking an average across the four domains.
Data analysis
Before conducting any data analyses, we screened the dataset for careless, invalid, and/or duplicate responses. First, we confirmed there were no duplicate IP addresses, and next we looked for respondents who had survey completion times that were more than ±2 standard deviations from the mean of the sample. Lastly, we reviewed short answer responses in attempt to find instances where participants exclusively answered multiple-choice questions or provided answers that were not relevant to the question being asked. All respondents passed these checks; thus, we did not eliminate any respondents.
For continuous variables measured in this study, we conducted Welch’s independent samples t-tests because of unequal variances across the samples. We report effect sizes using Cohen’s d. We analyzed categorical variables with chi-square independent samples tests of association, with odds ratios or Cramer’s V used to report effect sizes for variables with 2 or 3 or more levels, respectively. We used Wilcoxon rank-sum test to analyze ordinal variables, with correlation coefficients reported to demonstrate the effect size. An alpha of 0.05 was used to evaluate significance. In instances of multiple comparisons, we controlled for family-wise error by adjusting the p-value using “adjusted alpha = alpha/number of comparisons.” To examine associations between variables, correlations were conducted with significant relations further explored with linear regression. For all tests, we assessed appropriate assumptions, including no outliers (standardized residuals were examined to ensure values fell between ±3) or influential points (Cook’s distance values were examined to ensure values were under 1), normality (the Q-Q plot of residuals was inspected), homoscedasticity (the residuals vs. fitted values plot was inspected), and multicollinearity (variance inflation factor values were examined to ensure values <5), and corrected for them when necessary. In a few instances, we identified standardized residual values between ±3 and 5 (statistical outliers). In these cases, we reran the analyses without these participants. Given that the new analyses did not affect the outcome of the statistical analyses, we retained these outliers, and report on the full sample.
Results
Autistic traits
As expected, we identified higher autistic traits in the autistic sample than in the non-autistic sample (see Fig. 1 and Table 2).

Descriptive information for autistic (n = 77) and non-autistic (n = 128) respondents, including age, autism spectrum quotient (AQ) total score, Misophonia Questionnaire Severity score (MQSev), Misophonia Questionnaire Symptom score (MQSym), Inventory of Hyperacusis Symptoms total score (IHS), Patient Health Questionnaire (PHQ) of depression and anxiety total score, PHQ of depression and anxiety scale anxiety subscale score (Anxiety), PHQ of depression and anxiety scale depression subscale score (Depression), and the World Health Organization quality-of-life (QoL) averaged score. Note: One autistic participant withheld the age.
Measures of sound tolerance
We identified significantly higher clinical levels of misophonia and hyperacusis in the autistic sample of adults reporting DST than in the non-autistic sample of adults reporting DST. Thirty percent (30%) of these autistic adults reported clinically significant misophonia symptoms, compared with 13% of the non-autistic adults. Fifty-six percent (56%) of the autistic adults reported clinically significant hyperacusis symptoms, compared with 17% of the non-autistic adults. Twenty-six percent (26%) of the autistic adults reported both clinically significant misophonia symptoms and hyperacusis symptoms, compared with 9% of the non-autistic adults. Overall, we observed a higher prevalence of clinical misophonia symptoms, clinical hyperacusis symptoms, or both clinical misophonia and hyperacusis symptoms in the autistic sample of adults reporting DST than in the non-autistic sample of adults reporting DST (see Table 2).
Overall, the autistic sample had higher misophonia severity scores and a higher mean IHS score. However, given that many of the non-autistic respondents did not reach the clinical threshold for misophonia or hyperacusis, the increased number of nonclinical cases may have diluted the severity scores in the non-autistic group. For this reason, we conducted independent samples t-tests to compare misophonia severity and IHS total scores across only the autistic and non-autistic respondents who reached the clinical cutoffs for each of the respective questionnaires. After restricting the sample to only clinical cases, misophonia severity scores, t(29.3) = 0.013, p = 0.990, d = 0.004, and IHS total scores, t(41.5) = 1.54, p = 0.131, d = 0.405, did not differ across the autistic and non-autistic respondents.
Descriptions of sound intolerance
We asked participants to describe how long they have been sensitive to noise. Eighty-three percent of autistic adults indicated that they have been sensitive to noise since childhood, 9% indicated that their sensitivity developed in adulthood, and 8% were unsure. Sixty-three percent of non-autistic adults indicated they have been sensitive to noise since childhood, whereas 29% indicated that their sensitivity developed in adulthood, and 9% were unsure. These reported ages of onset were significantly different across groups, χ2(2) = 11.7, p = 0.003, V = 0.292. We also asked participants to indicate whether their sound sensitivities had been evaluated by a professional. Twenty-one percent of the autistic adults indicated that they had been assessed by a professional, whereas only 9% of the non-autistic adults indicated they had. Seventy percent and 89% of the autistic and non-autistic adults, respectively, indicated that they had not been evaluated by a professional, whereas 9% and 2% indicated they could not recall. This pattern of results was significant across groups, χ2(2) = 12.0, p = 0.002, V = 0.242.
In the absence of established measures of phonophobia, to assess whether this condition may also be present in our sample, we asked participants to indicate whether the anticipation of hearing a sound causes a negative reaction (see Fig. 2a). Although autistic (40.3%) participants most commonly reported that the anticipation of sound “sometimes” causes them to have a negative reaction, for non-autistic participants, both “rarely” and “sometimes” were equally most frequently endorsed (30.7% each). Autistic participants endorsed “frequently” or “always” 32.5% of the time, compared with 18.9% of non-autistic participants. Comparatively, non-autistic participants endorsed “never” 19.7% of the time, relative to 5.2% of autistic participants. This pattern of responses was significantly different between the autistic and non-autistic respondents, W = 3549.5 p < 0.001 r = −0.24, suggesting that phonophobia-like negative reactions to the anticipation of sound may occur more frequently for autistic people.
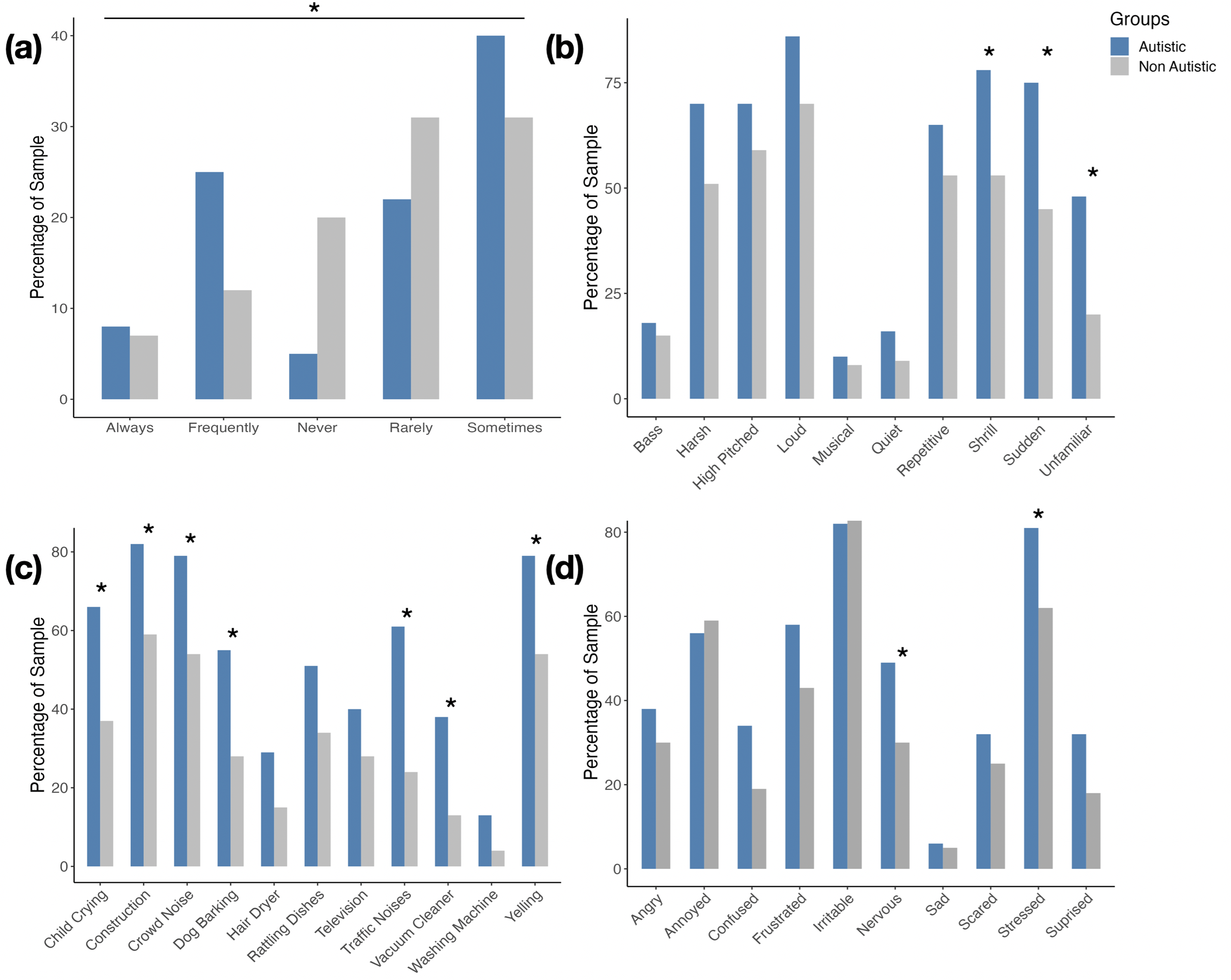
Percentage of autistic (blue) and non-autistic (gray) respondents who endorsed
Properties of aversive sounds
We asked participants to report whether their negative reactions to sound(s) are caused by specific, general, or both specific and general sounds. Within the autistic sample, 85.7% of respondents indicated they were sensitive to both very specific and general sounds and noises, whereas 14.3% indicated they were sensitive to only very specific sounds and noises, and no respondent indicated they only react to general noise. In the non-autistic sample, 59.4% of respondents endorsed both general and specific sounds and noises, whereas 35.9% indicated they only react to very specific sounds and noises, and 4.7% indicated reactions only occur to general noises. The distribution of responses was significantly different across the samples, χ2(2)=16.5, p < 0.001, V = 0.284.
We assessed the general features of sounds eliciting negative reactions in participants (see Fig. 2b). We conduced chi-square analyses to determine whether the general features of sounds that elicit negative reactions differed across autistic and non-autistic respondents. To correct for multiple comparisons, we used an alpha value of 0.005 to evaluate significance. Autistic respondents endorsed shrill (p < 0.001; odds ratio [OR] = 3.11), sudden (p < 0.001; OR = 3.68), and unfamiliar (p < 0.001; OR = 3.81) sounds as eliciting negative reactions significantly more often than did non-autistic respondents (see Supplementary Data S1 for detailed statistics).
We gave participants a list of specific sounds and asked them to endorse whether these sounds elicited negative reactions (see Fig. 2c). Chi-square analyses compared responses across autistic and non-autistic respondents. To correct for multiple comparisons, we used an alpha value of 0.005 to evaluate significance. Traffic noise (p < 0.001; OR = 4.90), dogs barking (p < 0.001; OR = 3.07), child(ren) crying (p < 0.001; OR = 3.38), construction (p < 0.001; OR = 3.18), someone yelling (p < 0.001; OR = 3.26), crowd noise (p < 0.001; OR = 3.26), and vacuum cleaners (p < 0.001; OR = 3.94) were all endorsed proportionally more by autistic respondents (see Supplementary Data S1 for detailed statistics).
We also asked participants to indicate what “other” sounds or noises cause them to react negatively. Broadly characterizing these “other” noises, we report frequencies across six generally similar categories.
Human-produced sounds were described by 43% (n = 33) and 42% (n = 54; OR = 1.05) of the autistic and non-autistic samples, respectively, including chewing/eating (autistic [A]: 12%, n = 9; non-autistic [NA]: 19%, n = 24; OR = 0.58), talking (A: 31%, n = 24; NA: 17%, n = 22; OR = 2.19), snoring/loud breathing (A: 1%, n = 1; NA: 5%, n = 7; OR = 0.19), arguing/talking in a negative tone (A: 1%, n = 1; NA: 5%, n = 6; OR = 0.19), “s” noises while talking (A: 3%, n = 2; NA: 2%, n = 2; OR = 1.52), spitting (NA: 2%, n = 2), sniffing (NA: 3%, n = 4), coughing (A: 3%, n = 2; NA: 1%, n = 1; OR = 3.06), and laughing/cackling (A: 1%, n = 1; NA: 1%, n = 1; OR = 1.00).
Autistic (12%; n = 9) and non-autistic (6%; n = 8; OR = 2.14) participants described animal/insect sounds, including cat/bird noises (A: 4%, n = 3; NA: 5%, n = 6; OR = 0.79), dogs breathing/panting (A: 1%, n = 1; NA: 2%, n = 3; OR = 0.49), and insects buzzing (A: 8%, n = 6).
Autistic (51%; n = 39) and non-autistic (37%; n = 48; OR = 1.77) participants described loud and/or sudden noises, including alarms/sirens (A: 34%, n = 26; NA: 14%, n = 18; OR = 3.16), musical instruments (NA: 8%, n = 8), leaf blowers/lawnmowers (A: 8%, n = 6; NA: 4%, n = 5; OR = 2.09), crashing/smashing sounds (A: 5%, n = 4; NA: 12%, n = 15; OR = 0.39), motorcycles/trains (A: 16%, n = 12; NA: 8%, n = 10; OR = 2.19), washroom hand dryers (A: 3%, n = 2; NA: 2%, n = 3; OR = 1.52), toilets flushing (A: 4%, n = 3; NA: 2%, n = 2; OR = 2.04), balloons popping (A: 5%, n = 4; NA: 1%, n = 1; OR = 5.21), thunder (A: 1%, n = 1), and fireworks (A: 6%, n = 5).
Autistic (53%; n = 41) and non-autistic (30%; n = 39; OR = 2.63) participants described constant noises, including background music/radio (A: 31%, n = 24; A: 17%, n = 22; OR = 2.19), competing/multiple noises at once (A: 22%, n = 17; NA: 11%, n = 14; OR = 2.28), air conditioner/fan (A: 8%, n = 6; NA: 6%, n = 8; OR = 1.36), and the hum of electricity in the walls or from lights (A: 13%, n = 10; NA: 3%, n = 4; OR = 4.83).
Autistic (16%; n = 12) and non-autistic (15%; n = 20; OR = 1.08) participants described repetitive sounds, including clocks ticking (A: 3%, n = 2; NA: 9%, n = 11; OR = 0.31), tapping (A: 8%, n = 6; NA: 5%, n = 6; OR = 1.65), and beeping (A: 8%, n = 6; NA: 4%, n = 5; OR = 2.09).
We grouped the last category of sounds based on their unique sound properties. Autistic (23%; n = 18) and non-autistic (16%; n = 21; OR = 1.57) endorsed these unique sounds. These include metal rubbing (A: 17%, n = 13; NA: 5%, n = 7; OR = 3.89), nails on a chalkboard (NA: 5%, n = 7), Styrofoam (A: 4%, n = 3; NA: 3%, n = 4; OR = 1.35), muffled noises (A: 1%, n = 1; NA: 3%, n = 4; OR = 0.33), crinkling bags like chip or cereal bags (NA: 3%, n = 4), creaking (A: 1%, n = 1), and the crunching of snow (A: 1%, n = 1; NA: 1%, n = 1; OR = 1.00).
Following the collection of these data, the Duke Misophonia Questionnaire 24 was published, including a list of common misophonia triggers. As such, we also coded the “other” responses according to this list (see Supplementary Data S1).
Responses to aversive sounds
Participants endorsed a list of emotional responses they felt when they were exposed to an aversive sound (see Fig. 2d). We used Chi-square analyses to compare the frequency with which autistic versus non-autistic respondents endorsed each emotional response. To correct for multiple comparisons, we used an alpha value of 0.005 to evaluate significance. Autistic respondents more frequently endorsed nervous (p = 0.005; OR = 2.31) and stressed (p = 0.005; OR = 2.56) feelings than non-autistic respondents (see Supplementary Data S1 for detailed statistics).
Given the concept of “pain hyperacusis,” we also looked more specifically at how often sound caused our participants pain by analyzing the question, “Sound can cause me pain and/or physical discomfort,” on the IHS. Autistic participants (54.6%) most commonly reported that sound “very much so” causes them pain and/or physical discomfort, whereas “a little” was most frequently endorsed (31.5%) by non-autistic respondents; see Supplementary Data S1 for more details. Accordingly, this pattern of responses was significantly different between autistic and non-autistic respondents, W = 2993.5 p < 0.001 r = −0.39, suggesting that autistic participants were more likely to experience pain and/or physical discomfort from sound.
Participants were then asked to describe how these negative reactions to sound impact their life. Based on the responses recorded, categories were established to summarize the open-ended responses across participants. The autistic and non-autistic samples reported that these sounds put them in a bad mood, making them annoyed and/or irritated (A: 19%, n = 15; NA: 22%, n = 28; OR = 0.83). Sounds were also reported to be distracting/disruptive (A: 23%, n = 18; NA: 18%, n = 23; OR = 1.36), cause stress/anxiety/or the feeling of being overwhelmed (A: 25%, n = 19; NA: 16%; n = 21; OR = 1.75), produce avoidance (A: 32%, n = 25; NA: 19%, n = 24; OR = 2.01), fleeing (A: 18%, n = 14; NA: 7%; n = 9; OR: 2.92), cause interpersonal issues (A: 3%, n = 2; NA: 10%; n = 13; OR = 0.28), fatigue (A: 8%, n = 6; NA: 5%; n = 7; OR = 1.65), pain (A: 13%; n = 10; NA: 5%; n = 12; OR = 2.84), fear (A: 1%, n = 1; NA: 3%; n = 4; OR = 0.33), outbursts (A: 1%, n = 1; NA: 2%, n = 3; OR = 0.50), depression (A: 5%, n = 4; NA: 1%, n = 1; OR = 5.21), embarrassment (A: 4%, n = 3; NA: 1%, n = 1; OR = 4.13), confusion (A: 1%; n = 1), and bullying/abuse/discrimination (A: 3%, n = 2; NA: 1%, n = 1; OR = 3.06). Finally, the sample indicated they have been able to reduce the effects of sound on their life through coping strategies such as noise-canceling headphones or earplugs (A: 21%, n = 16; NA: 12%; n = 15; OR = 1.95).
We also asked participants to describe what coping mechanism they wish existed to mediate their sound sensitivities. Based on the responses recorded, we establishedcategories to summarize the open-ended responses across participants. Both autistic (40%, n = 31) and non-autistic samples (25%, n = 32; OR = 2.00) mentioned better noise-canceling devices such as headphones, earplugs, or equipment to block noise. Furthermore, they specifically mentioned the need for devices that could selectively filter frequencies (A: 14%, n = 11; NA: 9%; n = 12; OR = 1.65) and devices that do not have to go on or in the ear (A: 4%, n = 3; NA: 1%; n = 1; OR = 4.13). In addition, respondents mentioned they wished for more social acceptance and/or socially acceptable devices for blocking or filtering noise (A: 10%, n = 8; NA: 9%; n = 12; OR = 1.12), as well as greater awareness of the distress that noise can cause individuals (A: 10%, n = 8; NA: 8%; n = 10; OR = 1.28). Participants also mentioned elimination of unnecessary loud noises (A: 12%, n = 9; NA: 10%; n = 13; OR = 1.23), as well as more quiet spaces or quiet hours in spaces (A: 18%, n = 14; NA: 5%; n = 6; OR = 4.17). Warning before loud sounds (A: 4%, n = 3; NA: 2%; n = 3; OR = 2.04) and better laws or policies to keep environments quiet (A: 5%, n = 4; NA: 2%; n = 3; OR = 2.58) were also mentioned. Lastly, the sample wished for desensitization methods to make them less sensitive (A: 5%, n = 4; NA: 5%; n = 6; OR = 1.00), meditation techniques to eliminate their sensitivity (NA: 2%, n = 2), medication to alleviate their sensitivity (NA: 1%, n = 1), wished for a cure (NA: 1%, n = 1), or simply said “I don’t know” (A: 5%, n = 4).
Associations between DST and mental health and quality of life
We conducted regression analyses to determine whether DST (MQ total scores, MQ severity scores, and IHS total scores) was differentially associated with anxiety, depression, and quality of life, across the autistic and non-autistic groups. The interaction between group (autistic, non-autistic) and the DST predictor (MQ total scores, MQ severity scores, and IHS total scores) did not account for significant variance in anxiety, depression, or quality of life (see Supplementary Data S1); thus, the samples were combined for further analysis. Correlational analyses were conducted to investigate relationships between measures of DST and age, autistic traits, mental health, and quality of life (see Table 3). Overall, results indicate that increased MQ total and severity scores were associated with more autistic traits and higher levels of anxiety, whereas greater IHS severity scores were associated with higher levels of autistic traits, anxiety, and depression and lower average quality of life (see Supplementary Data S1 for additional exploratory correlations).
Associations Between Decreased Sound Tolerance and Age, Autistic Traits, Mental Health, and Quality of Life

To correct for multiple comparisons, an alpha of 0.003 was set to assess significance (0.05/15 comparisons). Bolded values indicate statistical significance at p < 0.003.
One participant omitted their age; thus, N = 204 for age analyses.
AQ, Autism-Spectrum Quotient; MQ, Misophonia Questionnaire; IHS, Inventory of Hyperacusis Symptoms; PHQ, Patient Health Questionnaire; WHO QoL, World Health Organization Quality of Life Questionnaire.
Next, we conducted partial correlations between DST predictors (MQ total scores, MQ severity scores, and IHS total scores) and anxiety, depression, and quality-of-life total scores while controlling for age, gender, and autistic traits (AQ scores). Anxiety was significantly associated with MQ total scores [r(202) = 0.250, p < 0.001] and IHS scores [r(202) = 0.332, p < 0.001], whereas depression and quality of life were only associated with IHS scores [r(202) = 0.195, p = 0.005, r(202) = −0.228, p = 0.001, respectively]; see Supplementary Data S1 for full statistics.
To explore these relations further, we conducted additional regression analyses. First, we examined whether misophonia (total score) and/or hyperacusis symptoms (IHS total scores) accounted for unique variance in quality of life, after controlling for age, gender, and autistic traits (AQ scores). Overall 14% of the variance in quality of life was accounted for by the model [F(5,198) = 6.45, p < 0.001], with age (B = 0.13, p = 0.03) and hyperacusis symptoms (B = −0.27, p < 0.001) as the only significant predictors; see Supplementary Data S1 for detailed statistics.
We also conducted a regression analysis to examine whether misophonia (total score) and/or hyperacusis symptoms (IHS total scores) accounted for unique variance in anxiety scores, after controlling for depression, age, gender, and autistic traits (AQ scores). Overall 52% of the variance in anxiety scores was accounted for by the model [F(6,197) = 35.8, p < 0.001], with depression (B = 0.58, p < 0.001) and hyperacusis symptoms (B = 0.03, p = 0.005) as the only significant predictors; see Supplementary Data S1 for detailed statistics.
Discussion
We examined the characteristics of DST, specifically misophonia and hyperacusis symptoms, in autistic and non-autistic adults who self-reported DST. Furthermore, we explored the relationships between misophonia and hyperacusis symptoms/severity and mental health, quality of life, and autism characteristics. These results provide the foundation for understanding the characteristics of DST in autistic and non-autistic adults, as well as how DST influences everyday life in these populations. As DST is the most common sensory challenge experienced by autistic individuals,5,8 understanding whether the DST experienced by autistic adults is simply more severe, or whether it is qualitatively different from the DST experienced by non-autistic adults, is a crucial step in advancing research on the etiology, diagnosis, supports for, and treatment of DST.
Misophonia and hyperacusis rates in the current sample
To classify the DST experienced by our sample, we had participants complete misophonia and hyperacusis questionnaires. Thirty percent (30%) of autistic adults and 13% of non-autistic adults reported clinically significant misophonia symptoms. Interestingly, although 42% of the non-autistic sample reported human-produced sounds (a common class of misophonia triggers) as distressing, only 13% of the non-autistic sample had clinically significant misophonia symptoms. On the contrary, 43% of the autistic sample reported human-produced sounds as distressing, whereas 30% had clinically significant misophonia symptoms. To better understand how misophonia severity might differ across these samples, we compared misophonia severity ratings across only the respondents who were classified as having clinically significant levels of misophonia and/or hyperacusis. In these “clinical” samples, we did not find differences in misophonia severity across groups. This suggests that both clinical and subclinical misophonia symptoms may be more prevalent in autistic people reporting DST, but misophonia is experienced at similar levels of severity in both autistic and non-autistic people with clinical levels of misophonia symptoms. When considering hyperacusis, 56% of autistic adults and 17% of non-autistic adults reported clinically significant hyperacusis symptoms. Together these results suggest that among autistic and non-autistic people who report DST, clinical levels of misophonia and/or hyperacusis symptoms may be more prevalent in autistic people. However, given this research was not designed to assess prevalence, this finding should be interpreted with caution.
Properties of aversive sounds
Although autistic adults commonly report DST, few studies have focused on the specific types of distressing sounds. When we asked to describe whether their DST is associated with specific sounds, or sounds more generally, 86% of the autistic sample indicated they react negatively to both specific and general sounds and noises, and 14% indicated they were sensitive to only very specific sounds and noises. This contrasts with the non-autistic sample, where only 59% of respondents endorsed both general and specific sounds, whereas 36% indicated that they only respond negatively to specific sounds and noises. This pattern of results suggests that non-autistic adults’ DST may more often be linked to specific “trigger” sounds, whereas autistic adults’ DST may be linked to sounds in general, with specific noises being especially triggering. When asked to report the general features of sounds that they react negatively to, the majority (>50%) of autistic and non-autistic respondents indicated that loud, high-pitched, and repetitive sounds were distressing. Loud sounds are reported as extremely distressing for individuals with hyperacusis report.6,18 Most autistic adults also endorsed sudden, unfamiliar, and harsh sounds as distressing. The distressing nature of sudden sounds is consistent with the autobiographical accounts of “Loud sounds, sudden sounds. Worse yet, loud and sudden sounds I don’t expect”27 being distressing to autistic adults. Overall, the larger number of different types of sounds that were endorsed as distressing to the autistic relative to the non-autistic respondents is consistent with the earlier reported finding that both general and specific sounds are less tolerable to a larger number of autistic respondents.
Autistic adults reported on specific sounds that they react negatively to, of the 11 options provided, most autistic respondents endorsed 7 categories as distressing (traffic noises, dogs barking, rattling dishes, children crying, construction, yelling, and crowd noises), whereas non-autistic respondents only reported construction noises were distressing. This may again speak to the more generalized nature of DST in autistic adults. Participants were also asked to provide a list of “other” sounds or noises that cause them to react negatively. These responses were largely consistent across autistic and non-autistic respondents and broadly fell into six categories: human-produced sounds (e.g., chewing, talking), animal/insect sounds (e.g., birds chirping, dogs panting), loud and/or sudden noises (e.g., alarms, sirens), constant noises (e.g., background music/radio), repetitive noises (e.g., clocks ticking, beeping), and noises with unique sound properties (e.g., Styrofoam, metal rubbing). Although these “other” sounds were more frequently mentioned by autistic adults, the examples provided were largely similar across the two groups of respondents. Overall, although the types of noises reported as distressing did not show obvious qualitative differences across groups, quantitatively across the features (e.g., loud, high-pitched), specific categories (e.g., child crying, dog barking), and self-reported aversive sounds, a higher proportion of autistic respondents consistently endorsed DST. This is consistent with the higher proportion of the autistic sample that met the threshold for clinically significant misophonia and hyperacusis symptoms. Furthermore, these findings align with recent reports 28 that misophonia is more prevalent in autistic adults but not qualitatively different than what is experienced by non-autistic adults.
Reactions to sound or the anticipation of sound
To assess whether phonophobia may also describe some of the DST in these samples, we asked participants whether they have negative reactions to the anticipation of sound. Autistic people reported being more often negatively affected by the anticipation of sounds, with 73% of autistic respondents indicating they are “frequently,” “always,” or “sometimes” negatively affected by the anticipation of sounds, whereas in contrast, 50% of non-autistic respondents indicated they are “rarely” or “never” negatively affected by the anticipation of sounds. To our knowledge, at the time of data collection, researchers had no validated measurement tools available to assess phonophobia (however, see Williams et al., 29 Aazh et al., 30 Allusoglu and Aksoy, 31 and American Psychiatric Association 32 for recent contributions), but given these reports, it appears that participants in this sample (particularly the autistic sample) may also experience symptoms of phonophobia, possibly reflecting a learned fear response as a result of experiencing misophonia or hyperacusis.6,11 Although widely held diagnostic criteria for phonophobia have not yet been established, recent operational definitions of phonophobia (adapted from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [DSM-5] criteria for specific phobia of sounds 33 ) specify that the fear or avoidance of situations/sounds must be excessive relative to what would be expected for an individual with the same level of hyperacusis/misophonia symptoms. 34 Given that in our study we did not examine the intensity of respondents’ negative reactions during the anticipation of sound, we cannot be sure that respondents meet this operational definition of phonophobia. Rather, respondents may have been reporting on fear/avoidance reactions that were proportionate to their level of hyperacusis/misophonia symptoms. 34 Given the high rates of hyperacusis and misophonia in our autistic sample, we conjecture that phonophobia symptoms developed secondarily to these other forms of DST. 35 Importantly, the type of DST experienced by individuals (e.g., pure hyperacusis; pure misophonia; hyperacusis + secondary phonophobia; misophonia + secondary phonophobia; pure phonophobia) likely has implications for treatment best practices. 35
Considering the emotional responses reported by both autistic and non-autistic respondents when exposed to aversive sounds, DST appears to create a high level of distress. Across both groups, over half of the sample endorsed feelings of stress, irritability, annoyance, and frustration. Given the concept of “pain hyperacusis,” 35 we also looked more specifically at how often our respondents experienced pain in response to sound. Unlike previous reports, 36 autistic respondents more frequently endorsed sound causing higher levels of pain. Experiencing these negative emotions in response to everyday sounds is likely to create difficulties with everyday functioning. Accordingly, respondents most frequently reported that these negative reactions produced avoidance behaviors, created distractions or disruptions, and created anxiety or the feeling of being overwhelmed. Given these reports, it is likely that DST influences mental health and quality of life.
Relationship between DST and mental health and quality of life
We used correlational analyses to investigate the relationship between DST and mental health and quality of life more. Autistic and non-autistic samples were not found to differ in the strength of these relations, suggesting that DST has a similar impact on both groups. Consistent with earlier research, 36 83% of autistic respondents, relative to 63% of non-autistic respondents, indicated that they had been sensitive to noise since childhood. It is possible that this earlier onset in the autistic sample allowed individuals more time to develop compensatory strategies or coping mechanisms to mediate the effects of DST. Nonetheless, given that the strength of these relations did not differ, the samples were combined to examine the relationship between DST and mental health and quality of life. In line with the qualitative descriptions of negative reactions to sounds provided by the sample, after controlling for age, gender, and autistic traits, we found that increases in both MQ and IHS total scores were associated with higher levels of anxiety. That being said, when we then used MQ and IHS scores to predict anxiety in the same model, again after controlling for age, gender, and autistic traits, we only found that IHS scores accounted for unique variance in anxiety scores. Similarly, after controlling for age, gender, and autistic traits, we found that only hyperacusis severity scores were associated with increased depression and lower overall quality of life.
Given that hyperacusis is related to the perceived loudness of sounds, although misophonia is restricted to more specific sounds, the more generalized nature of hyperacusis may mean that it exerts a larger effect on people's everyday lives. For example, while most people spend a large amount of time each day interacting with other people, human-produced noises (often the triggers in misophonia) are only a subset of the noises we are exposed to each day. Furthermore, avoiding, predicting, and coping with human-produced noises may be easier than with noises in general. For example, if chewing noises particularly trigger someone with misophonia, they may avoid environments where these noises are commonly encountered, such as restaurants and kitchens (although some argue that misophonia triggers may be too unpredictable to avoid successfully 37 ). On the contrary, if someone with hyperacusis attempts to avoid environments with distressing sounds, they would need to avoid most public spaces and dramatically modify private spaces to remove noise sources. Overall, this would necessitate more avoidance, isolation, and accommodation. We suggest that in the case of hyperacusis, the decision between avoidance, isolation, and accommodation, or enduring high levels of distress because of the noise exposure, may promote more depressed feelings and have a greater impact on these individuals’ quality of life. Given that avoiding misophonia triggers may involve limiting participation in social activities (e.g., avoiding family gatherings, work socials),14,38,39 misophonia has the potential to degrade social relationships. Further research should focus on the impact of misophonia on the quality of interpersonal relationships.
Coping strategies for DST
One of the main goals of this research is to improve the quality of life of individuals who experience DST. As such, we asked our participants to describe coping mechanisms they wished existed to mediate their sound sensitivities. By far the most frequent request was for better noise-canceling devices such as headphones and earplugs. Elaborating on that, participants also mentioned devices that could selectively filter out certain frequencies so only the distressing frequencies were eliminated. Participants also discussed devices that do not go on the ear or that are more discrete or aesthetically pleasing. Given that many autistic people have more generalized sensory sensitivities, 40 the former may be related to the tactile sensations created by the devices, while the latter request is likely related to the reports of autism stigma (including stigma for autism-related sensory behaviors) causing bullying, abuse, and discrimination. For example, one respondent commented, “Wearing earplugs in situations that might be loud makes people ask questions,” whereas another commented, “Attempts to use accommodations such as headphones usually results in being bullied and/or abused.” People suggested ways to support those with DST, including greater social acceptance, understanding, compassion, awareness of the distress that noise can cause, the elimination of unnecessary loud noises, and more quiet spaces and quiet hours. Given these relatively easy changes could potentially have dramatic effects, this research speaks to the importance of educating the public on the prevalence of, and burden created by, DST.
Implications, limitations, and future directions
The current study provides strong evidence that autistic and non-autistic adults experience distress from DST and DST is associated with poorer mental health and quality of life. We need to better understand the nuances of DST before strides can be made in the development of treatments and interventions to support adults with DST, including how to differentiate subtypes of DST. One obstacle to this is the lack of validated measures of DST for autistic samples. Although the MQ and IHS have not been validated on autistic samples, a limitation of this study, since the completion of this data collection, the Duke–Vanderbilt Misophonia Screening Questionnaire has been developed and validated on autistic samples. 41
Differentiating subtypes of DST is particularly important to ensure treatments are beneficial, not distressing. Researchers have suggested that hyperacusis results from the amplification of low-level sensory information, leading to an increase in subjective loudness. 6 One treatment option for DST involves promoting desensitization through exposure therapy. 42 This often involves gradual and controlled exposure to sound stimuli, combined with cognitive behavioral techniques.43,44 Therapists originally developed exposure therapy to treat specific phobias (e.g., needle phobia), and it has shown some promise, as gradual exposure has allowed some individuals to adapt and become less reactive to sounds. 45 Given that exposure therapy occurs in a controlled environment, typically a therapist’s office, the therapist can carefully control the sounds. Exposure therapy can in theory be easily tailored to the specific triggers of the patient; however, this is less helpful in cases where the trigger is not a specific sound. Exposure therapy also carries risks. At the beginning of exposure therapy, individuals may experience discomfort and heightened sensitivity to sounds, which can be challenging to tolerate. Furthermore, therapeutic gains from exposure therapy require consistent and regular sessions, often accompanied by cognitive behavioral therapy, which can be very time-consuming. Although exposure therapy can be effective for some individuals, the degree of improvement varies widely 46 and its success may depend on the subtype of DST (e.g., being more appropriate for pure phonophobia without hyperacusis or misophonia). It is important to recognize that research demonstrating the utility of exposure therapy for treating DST in autism, specifically, is lacking. Importantly, the ethical basis of exposure therapy for treating DST has received harsh criticism from some autistic advocates. 47 Future research on intervention approaches must occur in collaboration with autistic advocates and those with lived experience of both autism and DST.
The current findings provide insight into the specific auditory stimuli that are less tolerable to autistic and non-autistic adults with DST, the reactions produced to these sounds, as well as the impact of DST on anxiety, depression, and quality of life. However, there are limitations to this study. Given that data collection occurred online, we could not confirm formal autism diagnosis. The online collection also limited our ability to conduct a formal hearing assessment, and thus, we cannot confirm whether differences in hearing thresholds were present. Some forms of DST (e.g., hyperacusis) are more likely to occur in individuals with hearing loss, but hearing impairment does not account for all cases of DST.38,47 Another potential limitation is that we largely sampled women. Although this may be the result of convenience sampling and the higher rates of women completing online studies, recent reports suggest that clinically significant misophonia is more prevalent in both autistic and non-autistic women, relative to men. 41 Future work should specifically explore the relationship between DST and mental health and quality of life in men versus women. Assessment of some particular DST conditions, particularly phonophobia, was very limited in our study, and future work should attempt to replicate our findings with established protocols as they emerge.29–32 Furthermore, this study was self-report in nature, leading to two additional limitations. First, the sample as a whole was limited to individuals capable of self-report and may thus not generalize to the broader population of autistic individuals. Second, given the potential for bias in subjective reports, future studies should aim to replicate these findings using more objective measures such as physiological responses to potentially triggering sounds. Our study was correlational in nature, limiting our ability to elucidate the direction of causation. As well, when building our regression models, we included some variables based on their past association with the dependent variables (DVs) rather than their correlation with the DVs. It is possible that this decision resulted in reduced power. However, choosing not to control for these variables may have artificially inflated our reported significance, so we opted to take the former more conservative approach. Furthermore, given this study was largely exploratory in nature, statistical analyses were only corrected at the family-wise level, and thus, these preliminary findings need to be validated with future research that applies a more rigorous statistical design. Lastly, we focused solely on negative reactions to sound. Given that many autistic people show both sensory avoidance and seeking behaviors, 2 it would be interesting to explore whether auditory seeking behaviors also occur in autistic people with DST.
Conclusion
These findings highlight the wide variety of sounds that are distressing to both autistic and non-autistic individuals with DST. Importantly, while these findings demonstrate that autistic people may be more likely to experience clinical levels of DST, the experience appears to be qualitatively similar for autistic and non-autistic people. Furthermore, these findings highlight the negative impact that DST has on mental health and quality of life. Future work would benefit from objective measures of sound intolerance, as well as focusing on differentiating the subtypes of DST to facilitate the development of treatments that specifically target the symptoms of each subtype (i.e., misophonia, hyperacusis, and phonophobia) rather than treating DST as a homogeneous problem.
Footnotes
Acknowledgments
The authors would like to thank the individuals who participated in this research. They would also like to thank Natalia Van Esch for her assistance with article revisions and formatting. The authors would also like to acknowledge and thank the reviewers and editors of this article for their valuable insight and suggestions.
Author Disclosure Statement
The authors have no conflicts of interest to declare, financial or otherwise.
Funding Information
This research was supported by the Wilfrid Laurier University Research Support Fund and a research grant from the Kid's Brain Health Network [Intelligent Solutions for Atypical Auditory Processing in Children with Neurodevelopmental Disorders].
Authorship Confirmation Statement
The authors confirm contributions to the article as follows: study conception and design: N.E.S., T.Q.B., G.I., and E.B.; data collection: T.Q.B.; analysis and interpretation of results: N.E.S., E.B., and T.Q.B.; draft article preparation: N.E.S.; article revisions and feedback: T.Q.B., S.A., G.I., and E.B. All authors reviewed the results and approved the final version of the article. The article has been submitted solely to Autism in Adulthood.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.