
Abstract
Background:
The present debate regarding what constitutes “cognitively healthy aging” in people with elevated autistic traits is highly relevant to the diagnosis of age-related conditions such as mild cognitive impairment (MCI) and dementia. Behavioral reaction time (RT) is an important component of cognition and everyday functioning, and it is included in diagnostic testing for such conditions. Autism trait level is not typically considered when including participants in aging-related RT research, and therefore requires examination to address whether those with high levels of autistic traits may show differences in terms of their RT performance, as relevant to testing for MCI and dementia.
Methods:
In the present study, we examined the relationship between RT and levels of autistic traits in 76 community-dwelling older adults (aged 50–78 years). We also investigated whether there were any differences in the relationship between RT and autistic trait level with respect to sex.
Results:
We found that the relationship between an individual’s levels of autistic traits and their RT scores varied depending on the type of task used, and on sex. In particular, for females, higher levels of autistic traits were related to slower RTs on the Trail Making task (Trails A), a task commonly used in clinical practice.
Conclusion:
Our findings indicate that some aspects of age-related cognitive decline may be steeper for older adults with higher levels of autistic traits, but that the impact may be different depending on sex, with higher trait levels in females being indicative of poorer RT performance. These findings may explain some of the outcome variability typical of previous studies, and have important implications for interpreting tests used for dementia diagnosis, particularly for older adults on the autism spectrum.
Community Brief
Why is this an important issue?
Reaction time (RT) refers to the amount of time that passes between when we perceive something and when we respond to it. It is an important part of our thinking and reasoning abilities called cognition, affecting how we function in daily life, and is included in the tests used for diagnosing age-related conditions including mild cognitive impairment (MCI) and dementia. It is important to understand more about the relationship between autistic traits and RT, particularly as we age.
What was the purpose of this study?
A person’s level of autistic traits are not typically taken into account when reaction time data is collected from the general population. This data is then used to compare an individual’s performance with when diagnosing conditions such as MCI and dementia. This means that, for older adults on the autism spectrum, current practice based on such data may be leading to inaccurate interpretation of cognitive ability.
What did the researchers do?
The current study recruited 76 people aged between 50 and 78 years, and investigated the relationship between their reaction time and levels of autistic traits on two different tests. We also analysed whether there were differences between males’ and females’ performances.
What were the results of the study?
We found that the relationship between an individual’s levels of autistic traits and their reaction time scores vary depending on the type of task used, and on sex. For example, for females, higher levels of autistic traits were related to slower reaction times on one task.
What do these findings add to what was already known?
The findings will be important in determining how clinical test results are interpreted, in particular concerning the diagnosis of MCI and dementia in people with higher levels of autistic traits. In addition, this study indicates that reaction time performance may decline to a greater degree for older adults with higher levels of autistic traits, but that this may be more noticeable in females compared to males.
What are potential weaknesses in the study?
This study recruited a higher number of females (N = 51) compared to males (N = 25). This may mean that there are limits to the extent to which conclusions can be drawn regarding the differences between sexes. Further research can aim to address these weaknesses by recruiting larger numbers of male and female older adults.
How will these findings help autistic adults now or in the future?
Our findings have important implications for how clinicians should interpret the results of tests used for dementia diagnosis, particularly for older adults on the autism spectrum.
Future research should aim to determine whether these results can be replicated with different tests of reaction time, and in older people with even higher levels of autistic traits. Finally, it is noted that studies of autistic traits in the general population cannot replace those with diagnosed autistic older adults. Future studies should therefore seek to determine how meaningful such reaction time data are to assessment and diagnosis of MCI and dementia in autistic older adults, and to determine what constitutes ‘cognitively normal ageing’ for autistic people as they age.
Introduction
Despite the fact that autism spectrum disorder (ASD; henceforth autism) is relatively common (1%–2% prevalence), little emphasis has been placed on research examining its relationship with cognitive function in older adulthood.1–9 Such investigation is vital to gain a more complete understanding of the relationship between aging and autism to better address needs in older adulthood, and to distinguish typical aging from disorders such as mild cognitive impairment (MCI; e.g., difficulties with cognitive abilities such as memory and reasoning in older age, which do not meet criteria for dementia diagnosis) and dementia. 1 There is some evidence indicating that aging with an autism diagnosis may be associated with disproportionately greater levels of objective cognitive decline (e.g., for processing speed, working memory, and executive function),2,4,8,10,11 compared with non-autistic older adults. Nevertheless, preservation (in visual and verbal memory, executive function, information processing speed),2,4,12–15 and even enhancement are found for some functions (e.g., visual perception and early sensory processing16,17 [see López Pérez et al. 18 ]). Such findings may indicate partial protection against age-related decline in some aspects of cognitive function,4,19 and that cognitive differences between autistic and non-autistic adults may become less pronounced with increasing age.2,20
However, the diversity of cognitive functions investigated, alongside a paucity of studies for any specific aspect of cognition, likely contributes to such heterogeneity, as does the range of tests used to ostensibly measure the same function. Indeed, subtle variation in test requirements may recruit different aspects of brain function and cognition variously associated with, or influenced by, autism and autistic traits. Studies have also varied widely with respect to the number of participants tested, the size of age groups, and numbers of males and females included (and indeed whether both sexes are included, as several studies include only male participants,1,4,13,15–27 with some recent research indicating that cognitive decline may be more likely in autistic older females than in males). 28 Heterogeneity may also be explained, at least in part, by individual differences in the time course and vulnerability patterns of age-related cognitive change in autistic people, 10 the heterogeneous nature of autism per se, 29 and atypical, but not necessarily dysfunctional, brain processing in autism.1,13,30–33 Further potential contributory factors to outcome variability may include investigation across studies of different age ranges, and whether participants’ autism diagnostic status and/or levels of autistic traits are measured. Such outcome variation highlights further some of the difficulty in determining whether age-related cognitive decline may be steeper for autistic compared with non-autistic adults,4,10,34 or presenting with a similar trajectory,4,35,36 or indeed whether autism may be protective against age-related decline.34,35,37
Although the majority of research has focused on individuals diagnosed with autism, non-autistic individuals also show varying levels of autistic traits, and provide a fruitful avenue for research in older adults.11,15,38,39 In addition, evidence from individuals who meet the criteria for the Broader Autism Phenotype (BAP; a phenotype in relatives of autistic people who show similarities to the defining features of autism, including social and communication difficulties, and restricted interests and behaviors)40–42 indicates that although they may experience more subjective cognitive decline with age (SCD; perceived decline in cognitive abilities with aging, which are not found on objective tests of function), rates of memory decline or clinical progression to MCI appear to be similar. 20 However, evidence also indicates that aging with elevated autistic traits (i.e., high, but below clinical cut-off for diagnostic purposes) is associated with poorer performance on measures of executive function and episodic memory.15,39 It is possible therefore that some older adults present within control groups in autism research may have, often unmeasured, high levels of autistic traits, which may affect task performance, further blurring group differences.15,20,43
The lack of evidence regarding what constitutes “typical or cognitively healthy aging” for autistic people and those with elevated autistic traits is particularly relevant to the diagnosis of age-related conditions such as SCD, MCI, and dementia.8,12,20,44,45 For some individuals, SCD and MCI represent very early or prodromal (preclinical) stages of dementia such as Alzheimer’s disease. For others, SCD and MCI may reflect a range of other conditions, some of which may not progress any further, or in some cases may be reversible. Early and differential diagnosis can be challenging, often requiring repeated testing and follow-up, but this is imperative to ensure timely and appropriate intervention, treatment, and care. An important diagnostic component is the administration of a battery of neuropsychological tests designed to determine the integrity of a wide range of cognitive functions (such as memory, executive function, language, and information processing speed). The performance of an individual is then compared to the “norms” of performance for that test (often taking into account factors such as age and educational level), with certain performance levels indicative of probable dementia or MCI. However, these diagnostic processes incorporate tests with normative data sets, which may not be sufficiently representative of cognitive function in older adults on the autism spectrum. This is particularly pertinent considering recent evidence indicating that autistic adults younger than 65 are more than twice as likely to be diagnosed with dementia compared with the general population, 46 and because autistic older adults may be at higher risk for SCD. 20 A recent study examined a large cohort of older adults with MCI or dementia (without formal autism diagnoses), who were assessed on a yearly basis using cognitive and clinical examinations. The findings indicate a significant association between the behavioral and psychiatric symptoms of dementia and autism-related behaviors, as well as a relationship between a greater degree of dementia severity and higher levels of autism-related behaviors. 5 Furthermore, those classed as being likely/possible to have autism had a longer duration of cognitive impairment, and poorer global cognition. 5
A more complete understanding of the relationships between aging, cognitive function, and interactions with other factors such as the autistic trait level is therefore necessary, to ensure that cognitive testing is adjusted for those on the autism spectrum, thus ensuring the same level of early and appropriate MCI and dementia diagnosis as in non-autistic people. As repeated cognitive testing plays a key role in the management of MCI and dementia, it is important therefore to also take into account any autism-related differences in age-related cognitive change over time, and the implications for potential adjustments to management and care. This aligns with the movement toward the adoption of an approach that emphasizes the importance of individual differences and characteristics in health care, moving away from the “one-size-fits-all” concept toward greater consideration of individual differences. This approach is increasingly adopted with respect to cognitive aging and dementia,47,48 and appears particularly relevant to autistic individuals and those with elevated autistic traits.
In this article, we focus on the relationship between autistic trait level and behavioral reaction time (RT); an important component of information processing, cognition, and everyday functionality that is characteristically impacted in typical aging, as well as in MCI and dementia, and is measured as part of diagnostic test batteries for such conditions. RT tasks engage multiple, distributed neural systems, 49 and can therefore be indicative of the integrity of many aspects of brain function. RT is closely linked with white matter integrity, 50 revealing disproportionate slowing in RT for older adults living with conditions associated with detrimental changes in white matter such as vascular cognitive impairment49,51–54 and Alzheimer’s disease. 55 Slowed RT is also associated with negative outcomes, including head injury, increased risk of mortality, morbidity, and falls, as well as reduced participation in exercise, work, poorer driving ability, mobility, quality of life, well-being, and social communication, as well as decreased independence in daily function.1,13,49,56–69 The intraindividual variability of RT (IIV; the manner in which an individual’s RTs will vary across trials within a given task) is also an important behavioral marker of functional integrity, particularly with respect to dementia and cognitive impairment,53,55,70–72 with evidence indicating that increased variability in RT may be associated with amyloid beta pathology (which is associated with some types of dementia) at age 70. 73
As there is evidence in the autistic population of reduced structural and functional integrity of white matter,1,74,75 and of a higher rate of comorbidity and increased risk for chronic disease, 76 one might predict slower and more variable RT in older adults on the autism spectrum, and therefore, a correlation between levels of autistic traits and both RT and IIV. However, research examining IIV in autism is scarce, and where studies have been conducted, they appear to have focused only on autistic children also diagnosed with ADHD. 31 Although some studies have indeed revealed significant RT slowing in autism across the life span, there is also evidence for preserved RT function.12,13,15,20,31,33,62,74,75,77–83 Previous studies may have failed to take into account the inherent heterogeneity in RT, which may have contributed to outcome variability seen in studies of RT in autism. This may also be related to factors such as sample size, test type, complexity, sensitivity, age, educational level, general cognition, subjective cognition, depression, or anxiety,4,9,10,13,20,71,82,84 as well as sex stratification with respect to some RT tests, 58 which in turn can be mediated by the task type and resource demands. 85 Furthermore, and of particular relevance to both clinical practice and research, considerable variation in RT within groups of individuals of a similar age with ostensibly the same diagnosis of dementia/MCI can occur.71,84 We argue that such factors should therefore be considered when analyzing and interpreting autism RT research, when measuring RT as part of a diagnostic process for MCI/dementia, and in producing normative data for tests of RT. This may be particularly important with respect to autism trait level, which is not typically considered an exclusion criterion in aging-related RT research, meaning that individual variation in levels of autistic traits may contribute to variability within and between groups and studies.15,20,43
Present study
There is little information available about the relationship between autistic trait level in older adults and cognitive function. Therefore, the overarching aim of this study was to improve our understanding of RT and its IIV in relation to autism trait level and thus its research and clinical applications.
This study was conducted to address the following three main research questions: (1) what is the relationship between RT and autism trait level (AQ); (2) would a relationship between RT and AQ differ depending on RT task type; and (3) which other factors may contribute to any relationship between RT and AQ? The first research question, and main objective of this study, was to determine the potential relationship between RT and autism trait level (as measured by the Autism Spectrum Quotient; AQ-50), 86 in older adults (aged 50+). Second, to determine whether any relationship between RT and AQ differs depending on the type of RT test used, we used two different, but clinical- and research-typical tests; the Trail Making test (TMT) 87 and a Visual Search test. 88 The TMT is typically used to assess executive function and executive function-related RT, and is commonly included in test batteries used in the diagnosis of dementia and its initial stages. Visual Search tests are used to assess attention-related RT (e.g., attentional shifting). Using a multi-trial Visual Search test also allowed us to measure IIV. Both the TMT and the Visual Search tests are typically used in RT-related research, and have two levels of difficulty (which vary in resource load and information processing requirement, as well as in functional network recruitment), thus allowing the determination of whether such factors may influence study outcome. Finally, to determine which other factors might contribute to any relationship between RT and levels of autistic traits, we also measured subjective and objective cognitive function using the Cognitive Change Index (CCI 89 ) and the Montreal Cognitive Assessment (MoCA 90 ), respectively. As previous RT studies have shown that RT can vary significantly with respect to sex, type of task, and sex by task interactions,58,71 we analyzed the data separately for males and females to determine any specific relationship between sex, RT, and levels of autistic traits. As autistic people disproportionately experience anxiety and depression compared with their non-autistic counterparts,23,38,76,91 we also administered the Beck Depression and the Beck Anxiety Inventories (BDI and BAI).92,93
Methods
Participants
We recruited community-dwelling older adults (n = 76, males = 25, females = 51; mean age = 65.0 years; range = 50–78) using opportunistic sampling from the Older Adults Research Participant Database at Swansea University, university-wide emails, and various community outreach events to increase the diversity of our sample (e.g., those who do not have access to/use the internet). Inclusion criteria included self-reported fair general health, fluency in English language, normal or corrected-to-normal vision and hearing, and the physical ability to perform the tasks. Exclusion criteria included past visits to their general practitioner or memory services regarding concerns about memory, clinically significant neurological, psychiatric, or medical conditions, psychoactive/neuroleptic drug use, history of serious head injury, and present or previous substance or alcohol dependency. We did not control for the use of prescribed and non-prescribed medication. We invited participants by email or letter to attend the Department of Psychology at Swansea University, Wales, UK for an appointment of around 2.5 hours, which included frequent breaks. Data were collected as part of a larger research project assessing cognitive abilities and autistic traits in a large cohort of older adults, with male and female participants matched where possible with respect to age, educational level, and general cognition (MoCA score; see below) before analysis. All inclusion and exclusion criteria for the larger project were as above.
Materials
Autism spectrum quotient
The Autism Spectrum Quotient (AQ-50 86 ) is a paper-based questionnaire providing a self-reported measure of levels of autistic traits, including 50 questions assessing social skill, attention switching, attention to detail, communication, and imagination. Participants were asked to rate their level of agreement with items such as “I prefer to do things with others rather than on my own” on a 4-point scale from “definitely agree” to “definitely disagree.” Participants were scored with one point for each item when they endorsed a behavior associated with autism either mildly or strongly (e.g., “strongly disagree” or “disagree” in response to the item “I can easily keep track of several different people’s conversations”). Test–retest reliability for the AQ-50 is reported at r = 0.7. 86
The Trail Making test (TMT)
The Trails A and B 87 test was administered as a measure of executive function-related speed of processing, attention, and cognitive flexibility.94,95 Trails A is a one-trial, paper-based task commonly described as probing information processing speed in relation to attention, visual scanning/search, number recognition, numeric sequencing, and motor speed. Trails B, another one-trial task, is typically described as exploring the efficiency of set-shifting, mental flexibility, executive function, divided attention, attention switching and shifting, visual search set shifting, simultaneous maintenance of two sequences, working memory, and cognitive flexibility. For Trails A, participants were asked to draw one continuous line joining a series of circled numbers in ascending order as quickly but as accurately as possible. The circled numbers were printed at random locations on an A4 sheet of paper, such that participants had to search for the next number in the sequence to join them. For Trails B, participants were asked to draw one continuous line joining a series of alternating circled numbers and letters in an ascending and alphabetical order (A -> 1 -> B -> 2, etc.) as quickly but as accurately as possible. Again, the circled numbers and letters were printed at random locations. For each trial, the experimenter immediately indicated to the participant if they made a mistake, asking the participant to rectify the mistake before continuing. Brief practice trials were provided for both Trails A and B. The dependent variable was time taken in seconds to complete each trial (note that this included any time taken to rectify errors). Test–retest reliability of the TMT A and B have been reported at 0.81 and 0.86, respectively. 96
Visual search
A computer-based visual search task was used. 88 Participants were seated ∼60 cm away from the computer screen. All trials included either a left- or right-pointing white target arrow on a black background (see Fig. 1).

Computer-based visual search task depicting a distracter-present trial on the left
Participants were instructed to fixate on the center cross before each trial, and then to respond as quickly and as accurately as possible to whether the target was pointing to the right or left using a QWERTY keyboard (right hand on key L to answer “right,” or left hand on key A to answer “left”). A clock-face configuration was used to position the target, both when it appeared alone (see (b) in FIG. 1) and when surrounded by distractors (see (a) FIG. 1; seven white arrows that pointed up or down), in a counterbalanced arrangement to eliminate differences in processing between the right, left, upper, and lower visual fields. Sixty-four trials were presented, with the target appearing eight times at each of the possible “clock-face” locations. Distractors were present with the target in the other clock-face locations for the distracter-present trials, and for the other half of the trials, no distracters were present (i.e., target only). For each trial, the central fixation cross appeared for 1000 ms, followed by the target (with or without distracters), which remained on screen until the participant responded. Ten practice trials were completed before the test began. Responses were eliminated if they were incorrect, or obviously due to a disturbance/lapse of concentration (e.g., responses with an RT below 150 ms, i.e., faster than natural RT, representing the pre-empting of the stimulus). For each participant, the median time (information processing speed) taken to respond to the target alone and the target plus distracter trials was determined, and group mean data produced. Individual and group mean errors were also calculated.
Montreal Cognitive Assessment (MoCA)
The paper-based MoCA 90 provided an index of general cognitive functioning. The MoCA is a 30-item experimenter-administered cognitive screening tool measuring short-term and working memory, visuospatial ability, executive function, language, attention, concentration, abstract reasoning, and orientation to time and place. Typical cognitive function is indicated by a raw score of at least 26/30. The MoCA has also been found to be a more sensitive screening tool for cognitive abilities in autistic older adults, compared with other measures such as the Mini-Mental State Exam (MMSE). 97 Internal consistency for the MoCA has been reported to be α = 0.84. 98
Cognitive Change Index (CCI)
The CCI (self-report 89 ) is an paper-based questionnaire consisting of 20 questions about perceptions of one’s own memory, executive function, and language abilities. Participants were asked to consider their cognitive function recently compared with the previous five years when rating each item on a 1–5 Likert scale (1 = no change or typical ability, 5 = much worse or severe problem) for items such as “recalling information when I really try,” “focusing on goals and carrying out a plan”, and “understanding conversations”. A higher total score indicates greater feelings of SCD compared with five years ago (reliability at α = 0.94). 99
Beck Anxiety Inventory
The Beck Anxiety Inventory (BAI 93 ) is a measure of self-reported symptoms of anxiety over the past week. The BAI is a paper-based questionnaire consisting of 21 items regarding physical and cognitive symptoms of anxiety (e.g., heart pounding; fear of the worst), which participants rate on a four-point scale ranging from 0 (not at all) to 3 (severely, I could barely stand it) in relation to how much they were bothered by each symptom. A higher score indicates greater symptoms of anxiety (internal consistency α = 0.92; test–retest reliability = 0.75). 100
Beck Depression Inventory
The Beck Depression Inventory (BDI 92 ) is a measure of self-reported symptoms of depression over the past week. The BDI is a paper-based questionnaire consisting of 21 items regarding cognitive, behavioral, affective, and somatic symptoms of depression, which participants rate on a four-point scale ranging from 0 to 3. For example, for the topic of sadness, choices range from 0 “I do not feel sad” to 3 “I am so sad and unhappy that I can’t stand it”. A higher score indicates higher levels of depression symptoms (internal consistency α = 0.85). 92
Procedure
We collected demographic data using questionnaires sent to participants by post before the study, including date of birth, sex1, present and/or previous occupation/s, formal qualifications, and the AQ. The remainder of the measures were assessed during the study appointment. Tasks were administered in a fixed order alongside other tasks not described here as part of a larger research project (including the Empathizing and Systemizing Quotients, a task measuring visual and spatial abilities, Wide Range Achievement Test (WRAT) math task, block design task, and a measure of intuitive physics). In total, participants completed a neuropsychological test battery consisting of 14 tasks lasting approximately 2 hours, intersected by a break. The measures reported in this article were administered in the following order: MoCA, Trails A & B, Visual Search, BAI, BDI, CCI, with a minimum of one break in the middle of the appointment (more if requested by the participant). All participants were tested individually. At the end of the session, individuals were fully debriefed with respect to their participation.
Statistical analysis
Statistical analysis was conducted using IBM SPSS Statistics Version 28.0.1.1. For Trails B, one participant’s score was removed as an extreme outlier as identified by the Shapiro–Wilk analysis. Pearson product-moment correlation was used to determine the strength and direction of a linear relationship between variables (AQ, TMT: A, TMT: B, Visual Search: Target alone, Visual Search: Target plus distracter, MoCA, CCI, BAI, and BDI). Linear regression analysis was used to (a) determine whether the linear regression between two variables was statistically significant; (b) determine how much of the variation in the dependent variable was explained by the independent variable; (c) understand the direction and magnitude of any relationship; and (d) predict values of the dependent variables based on different values of the independent variable. Independent-samples t-tests were used to determine if a significant difference existed between the means of two independent groups (males and females).
Results
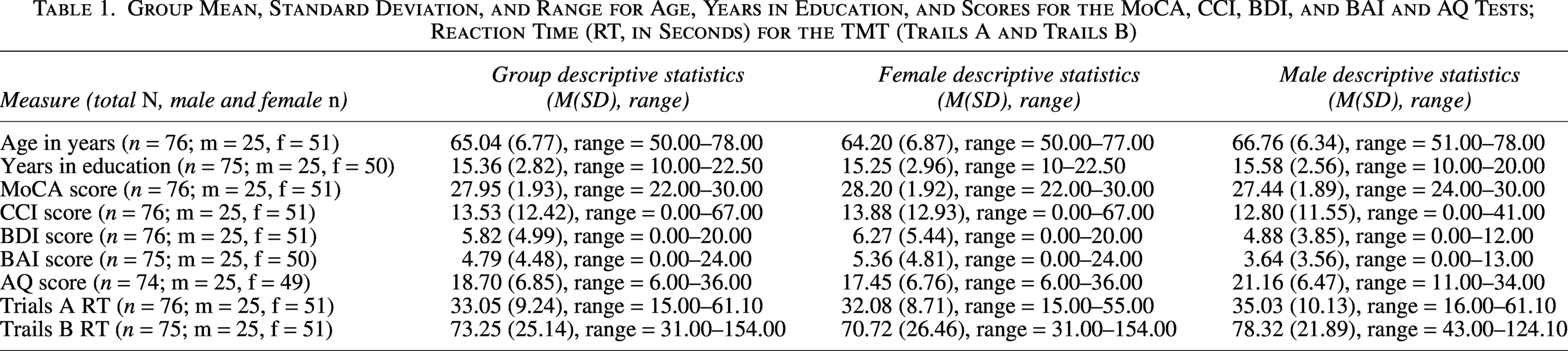
During recruitment, we ensured that male and female participants were matched at the group level where possible with respect to age, educational level, and general cognition. Despite our efforts,2 more females than males were recruited. Nevertheless, independent t-test analyses confirmed that there were no significant differences between men and women for mean age (p = 0.121), years in education (p = 0.636), MoCA (p = 0.109), CCI (p = 0.724), BDI (p = 0.255), or BAI (p = 0.118; see Table 1). However, AQ score was significantly greater for males than females (p = 0.026).
Group Mean, Standard Deviation, and Range for Age, Years in Education, and Scores for the MoCA, CCI, BDI, and BAI and AQ Tests; Reaction Time (RT, in Seconds) for the TMT (Trails A and Trails B)
Autism Spectrum Quotient (AQ) correlations
AQ score was not correlated with age, years in education, MoCA, CCI, BDI, or BAI scores across the entire sample (see Table 2), nor when analyzing the data separately between the sexes (all ps > 0.05, see Table 3).
Correlations Between Demographic Factors and All Measures
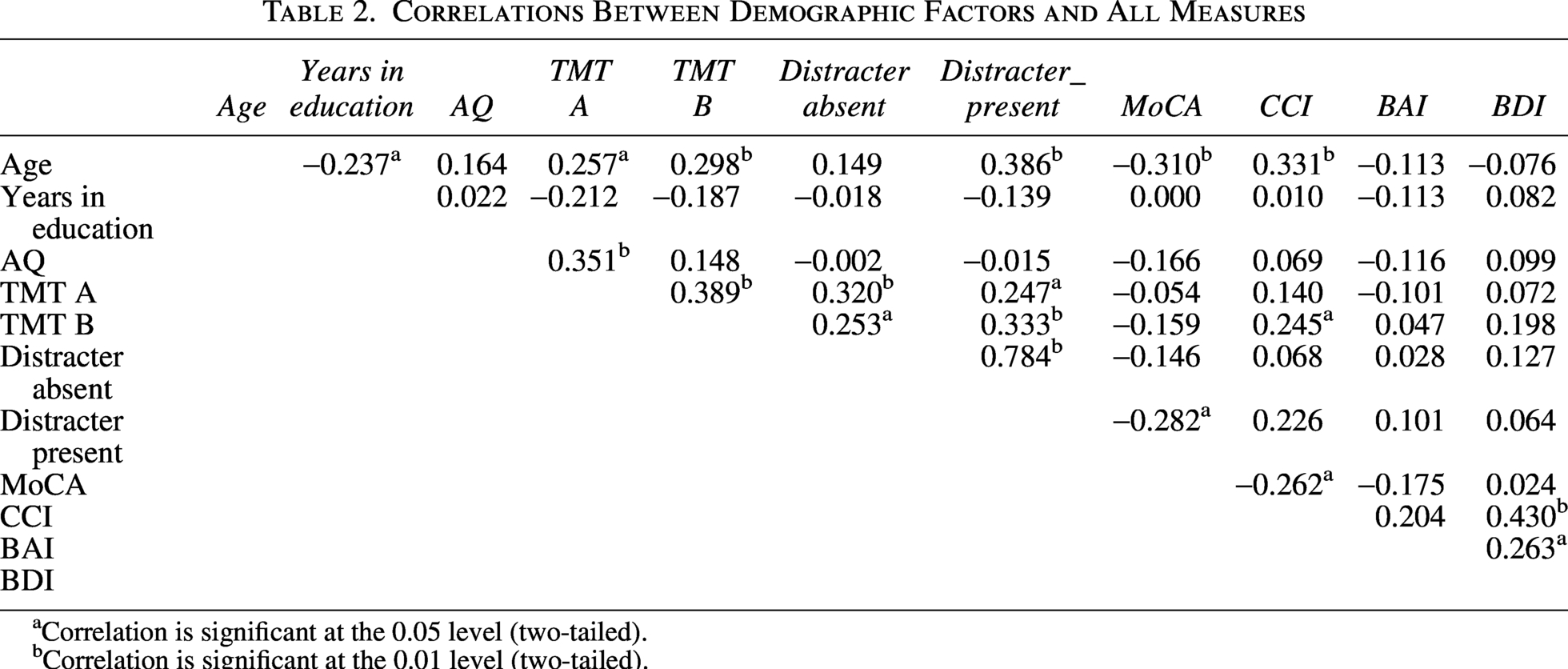
Correlation is significant at the 0.05 level (two-tailed).
Correlation is significant at the 0.01 level (two-tailed).
Correlations Between Demographic Factors and All Measures. Results for Females Are Presented Above the Diagonal; Results for Males Are Presented Below the Diagonal
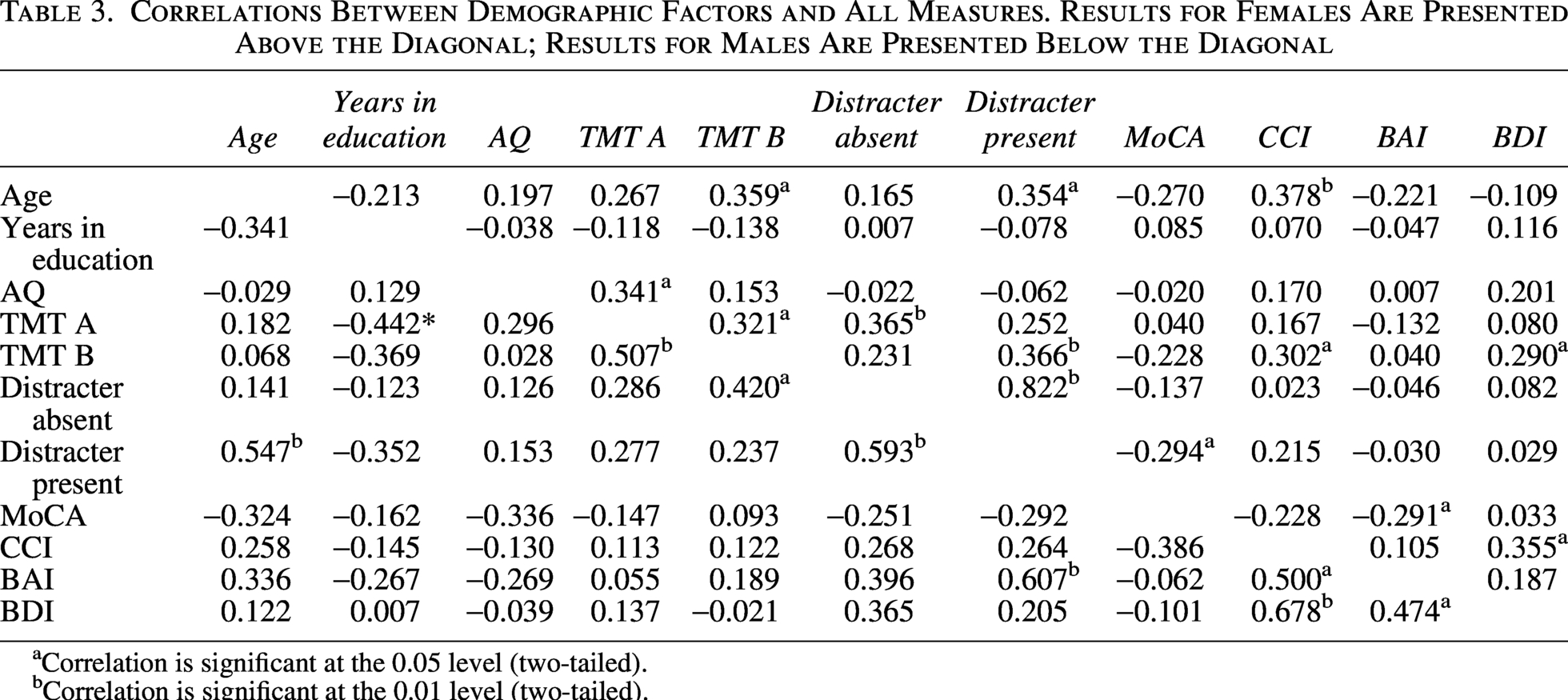
Correlation is significant at the 0.05 level (two-tailed).
Correlation is significant at the 0.01 level (two-tailed).
The Trail Making test
Trails A
Slower Trails A RT was significantly correlated with a higher AQ score, with AQ accounting for 12.3% of the variation in RT [F(1,72) = 10.09, p = 0.002, R2 = 0.123, adjusted R2 = 11.1% (medium effect size)101–103]. Slower Trails A RT was also significantly correlated with older age, with age accounting for 6.6% of the variation in RT [F(1,74) = 5.25, p = 0.025, R2 = 0.066, adjusted R2 = 5.4%], but was not significantly correlated with any other factors (see Table 2, and see Supplementary Table S1 for all box plots).
Males
For males, Trails A RT did not significantly correlate with AQ, age, MoCA, CCI, BDI, or BAI, but faster RTs on Trails A were related to having more years of education, accounting for 19.5% of the variation in RT [F(1, 23) = 5.58, p = 0.027, R2 = 0.195, adjusted R2 = 16% (medium effect size); see Table 3].
Females
Slower Trails A RT was significantly related to higher AQ scores, accounting for 11.6% variation in RT (Trails A) [F(1,47) = 6.18, p = 0.01, R2 = 0.116, adjusted R2 = 0.097]. Trails A was not significantly correlated with any other factors (see Table 3).
Trails B
Trails B RT was not significantly correlated with AQ, but slower responses were associated with older age (as for Trails A), with age accounting for 8.9% of the variation in RT [F(1,74) = 7.14, p = 0.009, R2 = 0.089, adjusted R2 = 7.7%]. A higher CCI score (i.e., greater degree of SCD) was also significantly related to slower Trails B RT, with CCI accounting for 2.6% of the variation in Trails B RT [F(1,73) = 1.91, p = 0.171, R2 = 0.026, adjusted R2 =1.2%]. None of the correlations between Trails B RT and other factors was significant (see Table 2).
Males
Trails B RT was not significantly correlated with any other variable (see Table 3).
Females
Slower Trails B RT was significantly related to older age, accounting for 12.9% of the variation in Trails B RT [F(1,48) = 7.09, p = 0.010, R2 = 0.129, adjusted R2 = 11.1% (moderate effect size)]. In addition, slower RTs were related to higher CCI scores, accounting for 9.1% of the variation in Trails B RT [F(1,48) = 4.81, p = 0.033, R2 = 0.091, adjusted R2 = 7.2% (small effect size)]. Finally, higher BDI scores (i.e., greater degree of depression symptomology) were related to slower RTs, accounting for 8.4% of the variation in Trails B RT [F(1,48) = 4.41, p = 0.041, R2 = 0.084, adjusted R2 = 6.5% (small to medium effect size)]. None of the other correlations was significant (see Table 3).
Independent t-test analyses revealed that overall, there were no significant differences between males and females for Trails A RT [t(74) = 1.31, p = 0.193, 95% CI: lower = −1.52, upper = 7.42] or for Trails B [t(73) = 1.24, p = 0.219, 95% CI: lower = −4.62, upper = 19.14].
Visual search RT
The visual search RT data were examined for the target-alone condition and the target-plus-distractor condition.
Target-alone condition
Target-alone RTs, and the IIV of RT, were not related to any factors for the entire sample (see Table 2), nor for males and females when analyzed separately (see Table 3).
Target-plus-distracter condition
A slower RT for the target-plus-distracter condition was significantly related to older age, accounting for 14.9% of the variation in RT [F(1, 74) = 13.00, p < 0.001, R2 = 0.149, adjusted R2 = 13.8%], with a higher MoCA score (i.e., poorer objective cognitive functioning), accounting for 7.9% of the variation in RT [F(1, 74) = 6.38, p = 0.014, R2 = 0.079, adjusted R2 = 6.7%], and with a higher CCI score, accounting for 5.4% of the variation in RT [F(1, 73) = 4.14, p = 0.046, R2 = 0.054, adjusted R2 = 4.1%]. IIV was not significantly correlated with any factors (see Table 2).
Males
Slower target-plus-distracter RT was significantly correlated with older age, accounting for 29.9% of the variation in RT [F(1, 23) = 9.80, p = 0.005, R2 = 0.299, adjusted R2 = 26.8%], and with higher BAI scores (i.e., greater degree of anxiety symptomology), accounting for 36.9% of the variation in RT [F(1, 23) = 13.44, p = 0.001, R2 = 0.369, adjusted R2 = 34.1%]. None of the other correlations was significant (see Table 3).
Females
Slower target-plus-distracter RT was significantly correlated with age, accounting for 12.5% of the variation in RT [F(1, 49) = 7.00, p = 0.011, R2 = 0.125, adjusted R2 = 10.7% variation]. In addition, slower RTs were related to lower scores on the MoCA, accounting for 8.6% of the variation in RT [F(1,49) = 0.62, p = 0.037, R2 = 0.609, adjusted R2 = 6.7% variation].
Independent t-test analyses revealed no significant differences between males and females for target-alone RT [t(74) = −0.26, p = 0.796, 95% CI: lower = −0.09, upper = 0.07] or for target-plus-distracter RT [t(74) = −0.13, p = 0.897, 95% CI: lower = −0.18, upper = 0.15]. Finally, there were no significant differences between males and females for the number of errors for either the target alone [t(74) = −0.87, p = 0.386, 95% CI: lower = −0.81, upper = 0.32] or the target-plus-distractor [t(74) = 0.00, p = 1.0, 95% CI: lower = −0.92, upper = 0.92] conditions.
Discussion
To date, there has been little investigation into the relationship between autistic trait level and behavioral RT in older adults. Studies conducted so far indicate significant outcome heterogeneity, rendering it difficult to determine the trajectories of age-related stability or decline in relation to levels of autistic traits. This is particularly relevant in relation to the RT measures used in diagnostic test batteries for conditions such as MCI and dementia, as well as for the production of normative data sets for such tests. In this study, we therefore examined the relationship between older adults’ RTs (using Trail Making and Visual Search tests to examine the effect task type may have on RT performance in tests typically used in clinical practice) and levels of autistic traits. Furthermore, to investigate the potential influence of other factors on RT, we also examined RT and autistic traits in relation to age, sex, educational level, cognition (MoCA score), perceived cognitive change (CCI), anxiety (BAI), and depression (BDI).
Our results indicate one confirmatory and two main findings. First, we replicated the well-established finding that males score significantly higher than females on the AQ. 86 Second, the AQ score was significantly correlated with Trails A RT, although once the group was split by sex, this correlation only remained for the females. Third, there was no significant correlation between visual search RTs and AQ, although RTs on the different tasks were related to other demographic and mental health factors, depending on sex. These main findings are discussed in turn below.
First, slower responses on Trails A were associated with both older age and higher AQ. However, when split by sex, slower Trails A RTs were related to lower levels of education in men, whereas in females, the relationship with higher AQ remained. In addition, poorer performance on Trails B was related to older age and higher levels of SCD, but these correlations only remained for the females when analyzing separately by sex.
These findings suggest that the impact of autistic traits on RT in aging may be different depending on sex, as well as task. These results highlight the importance of considering sex when analyzing the impact of autism and/or levels of autistic traits on typical aging, as well as aging with cognitive impairment such as dementia. 104 This is particularly relevant to aging research, where the extent to which autistic traits influence age-related cognitive change is under-researched. Therefore, different conclusions about the role of autistic traits in RT performance could be drawn based on the distribution of participant sex and the RT tasks used, contributing to study outcome heterogeneity.
The findings may also indicate some evidence for the Female Protective Effect theory (FPE 105 ), through which it is proposed that females can withstand a larger etiological load compared with males before they will necessarily meet the threshold for an autism diagnosis (see also Cauvet et al., 104 Craig et al., 106 , and Deng et al. 107 ). The FPE posits that autistic females will generally have a higher degree of brain changes compared with their male counterparts before exhibiting a similar level of autism-related behavioral features. In terms of the present findings, it could be the case that the older males with higher levels of autistic traits are not disadvantaged in terms of their performance on cognitive tasks measuring RT (i.e., Trails A), whereas older females with higher levels of autistic traits may be at a disadvantage on such tasks.
Previous research has shown that men are twice as likely to report SCD than women. 108 In contrast, Klein et al. 28 found that SCD may be more likely in autistic females (although this finding was not statistically significant), and also found an association between higher levels of autistic traits and greater likelihood of SCD. Our findings may somewhat support this, in that older females with higher levels of autistic traits showed poorer performance on an RT task (although it should be noted that sex-group differences were not found), and poorer objective cognitive function (Trails B) was related to higher SCD, indicating that the females in the present study may have been more aware of their own cognitive challenges. Future research should endeavor to further examine the present findings, which indicate that the impact of sex on SCD in the general population (more common in males) may be reversed in those with higher levels of autistic traits. 28
For the visual search RT task, no sex-group differences were found for RTs, nor their IIV, across any of the conditions. In addition, RTs when the target was presented without distracters were not related to any other variables. However, when the target was presented alongside distracters, faster RTs were related to younger age, better objective cognitive ability (as measured by the MoCA), and lower SCD. Faster RTs were associated with younger age for both males and females, while for men, faster RTs were also related to lower anxiety scores, and for females, only the relationship between faster RTs and objective cognitive ability (MoCA) remained. This pattern of results is in line with previous findings of specific interactions between RT, demographic factors, sex, and RT task in general populations. 109
Some evidence indicates that older autistic adults may have a specific deficit in processing speed (e.g., Tse et al. 8 and Spek et al., 110 but see Geurts et al. 10 ) However, such findings are limited and mixed. Indeed, although Davids et al. 12 found that although autistic adults aged >50 displayed generally reduced processing speed during complex executive functioning tasks, this was not associated with executive performance (flexibility, fluency, planning, etc). Our findings do not indicate a clear relationship between levels of autistic traits in an older adult sample and RTs, although they do indicate varied relationships dependent on sex and task. Such outcome variation could also be explained, at least in part, by the association between Trails A and B performance and different aspects of brain processing, 111 which may also, depending upon task, be variably associated with levels of autistic traits.
Limitations and future directions
Giving instructions to answer “as quickly but as accurately as possible” may influence the outcome (i.e., it is unclear to what extent there may be individual differences in the relative weights that participants allocate to their speed vs. their accuracy on a given task). 112 In addition, it has been suggested that socially-provided task instructions can impair autistic adults’ ability to monitor and respond to their own performance on some cognitive tasks.113,114 It is worth considering that autistic people may perform more optimally under non-socially delivered instruction, such as online. Future studies could investigate this further in autistic and non-autistic older adults, delivering clinically relevant cognitive functioning tasks with traditional, clinician-delivered methods versus delivered using technology.
It is also possible that the apparent interaction between RTs and autistic trait level may be related, at least in part, to responses to the test situation (e.g., which test is used and which is administered first), procedure, and environment, and the cognitive processing resources involved in the test, which may be variably affected by levels of autistic traits. Clearly, further research is necessary to determine whether these results can be replicated, especially with different RT tests, and in populations specifically selected for having high levels of autistic traits. Further clinical studies are also needed to determine how meaningful such RT data and other aspects of cognitive function are in terms of clinical assessment and diagnosis, and what constitutes “cognitively normal aging” for older adults on the autism spectrum. Finally, longitudinal studies are required to determine whether SCD is indicative of dementia or has some other etiology, particuarly within older adults on the autism spectrum.
Conclusions
Our findings therefore contribute to the presently mixed results regarding the impact of aging on older adults on the autism spectrum, or with higher levels of autistic traits, on RT,12,13,15,20,31,33,62,75,81–83 but are novel in that they provide some suggestions as to why RT study outcomes in normal and atypical aging are so heterogenous, and the implications of this for those aging with autism or high levels of autistic traits. Indeed, any significant relationship between the level of autistic traits and RT may have implications for the interpretation of test results used in a clinical setting (e.g., dementia diagnosis). Our findings partially support the suggestion that some aspects of cognitive decline in aging may be steeper for older adults with higher levels of autistic traits,4,10,28,34 but also highlight that the impact may be different depending on sex, with poorer RT performance on some tasks for females in particular. The findings therefore have important implications for the autism community, in that they show how testing for cognitive decline in older age may need to take autism diagnostic status and levels of autistic traits into consideration when making a judgment regarding the diagnosis of conditions such as MCI and dementia.
Our results may also be of relevance to the use of normative data (for the Trails A test in particular), for which the potential influence of autistic trait level may not have been taken into account. The results also have implications for the use of the Trails A in studies of RT, the output of which could vary between studies involving different numbers of female participants and their autistic trait level. As anxiety, depression, and cognitive ability are already being taken into account when measuring RT, autistic traits should also be considered.
Footnotes
Acknowledgments
The authors thank all the study participants for their time.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This work was supported by the Realising Potential Trust (B1760) and BRACE Dementia Research (Registered Charity Number: 297965).
Ethics statement
The study was ethically approved by the Department of Psychology Ethics Committee at Swansea University. All participants provided written informed consent, were free to withdraw at will and at any time, and were fully debriefed after participation.
Authorship Confirmation Statement
J.E.N.: Conceptualization, data curation, formal analysis, investigation, methodology, resources, software, supervision, writing—original draft, and writing—review and editing. A.T.: Conceptualization, data curation, formal analysis, investigation, methodology, resources, software, supervision, funding acquisition, writing—original draft, and writing—review and editing. J.R.B.: Conceptualization, data curation, formal analysis, methodology, resources, software, funding acquisition, writing—original draft, and writing—review and editing. A.L.C.: Data curation, formal analysis, investigation, methodology, resources, software, writing—original draft, and writing—review and editing. E.R.: Data curation, formal analysis, investigation, methodology, resources, software, writing—original draft, and writing—review and editing.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.