
Abstract
Background:
Previous literature indicates a proportional overrepresentation of both autism and autistic traits within gender-diverse populations (individuals who experience their gender identity as different from their sex assigned at birth). Emerging but limited evidence also suggests a proportional overrepresentation of gender-diverse identities in autism. To our knowledge, this is the first study to report gender diversity prevalence in autistic adults in the United States.
Methods:
We report the prevalence of gender diversity within two well-characterized samples of autistic adults recruited from SPARK (Simons Foundation Powering Autism Research for Knowledge), the largest online research database of autistic individuals to date. This study includes both an original sample (Dataset 1, n = 205) and a replication sample (Dataset 2, n = 243). In addition, we looked at the co-occurrence of anxiety and/or mood disorders with gender-diverse identities.
Results:
We found that 16.1% of autistic adults in Dataset 1 and 19.8% of autistic adults in Dataset 2 were gender diverse. This compares with prior findings of 0.5% to 4.5% in the general adult population. Autistic participants who were gender diverse, compared with those who were not, were up to six times more likely to report diagnosed anxiety and/or mood disorder(s). The finding of proportional overrepresentation of gender diversity in autistic individuals is consistent with reports from other countries, and higher than some previous estimates (e.g., 15%).
Conclusion:
These findings point to the necessity for autism research to take gender identity into account in addition to sex assigned at birth, and to pay particular attention to the mental health challenges that gender-diverse autistic individuals may face. These important steps will lead toward increased understanding of the needs of gender-diverse autistic individuals and ways to improve care.
Community Brief
Why is this an important issue?
People who are gender diverse (i.e., individuals who experience their gender identity as different from their sex assigned at birth) are more likely to be autistic or to have autistic traits than those who are cisgender (individuals who experience their gender identity as the same as their sex assigned at birth). Some research also suggests that autistic individuals are more likely to be gender diverse than those who are not autistic. However, as far as we know, no studies have looked at the proportion of autistic adults in the United States who are gender diverse.
What was the purpose of this study?
We looked at the rates of gender diversity in autistic adults in the United States. We also examined the rates of anxiety and mood disorders in these adults to see whether there was a difference in rates in the gender-diverse compared with the cisgender autistic adults.
What did the researchers do?
We looked retrospectively at the data from two online studies, which asked autistic and nonautistic adults about their gender identity and their sex assigned at birth. The researchers also asked whether they had received a diagnosis of an anxiety and/or mood disorder and compared these numbers in the cisgender and gender-diverse individuals.
What were the results of the study?
We found that a larger percentage of autistic adults were gender diverse compared to percentages reported in nonautistic individuals in the general adult population. We also found that autistic gender-diverse individuals were more likely to report diagnosed anxiety and/or mood disorders than autistic cisgender adults.
What do these findings add to what was already known?
This work adds to existing knowledge about the rates of gender-diverse identities in autistic adults in the United States. The results also add further information about the different rates of anxiety and mood disorders among gender-diverse and cisgender autistic adults.
What are potential weaknesses in the study?
First, we did not formally compare the nonautistic adults with the autistic samples since not all individuals in the nonautistic samples resided in the United States. Second, some wording on the survey questions does not align with current practices in the field. Third, we recognize the importance of engaging autistic and gender-diverse collaborators throughout the research process. We acknowledge that not having a diverse array of perspectives is a limitation of the study.
How will these findings help autistic adults now or in the future?
These findings will encourage autism researchers to study gender identity in addition to sex assigned at birth since many autism research studies group participants using only “sex” or “gender” and do not report on both. This would allow for improved understanding of gender-diverse autistic individuals and their unique experiences. Our findings also highlight the need for future research to find out more about the needs and challenges experienced by gender-diverse autistic individuals as well as strategies for improving care.
Introduction
Despite increasing interest in “sex differences” in autism research, few autism studies have reported both sex assigned at birth and gender identity. Therefore, it is often unclear in studies of autism-related “sex differences” whether the authors are referring to sex assigned at birth, gender, or a combination. 1 Furthermore, studies often do not account for, or characterize, gender-diverse identities, defined as incongruence between sex assigned at birth and gender. This lack of clarity is especially problematic because previous findings indicate a common intersection between gender diversity and autism, and that neurodevelopmental and mental health phenotypes may differentially relate to gender identity versus sex assigned at birth, highlighting the importance of studying gender identity specifically as it relates to autism.2–6 As such, it is important to advance understanding of the prevalence of gender diversity in autistic individuals, and the mental health challenges that they may experience. To our knowledge, no studies to date examine the prevalence of gender diversity in US-based autistic adults.
Definitions and background
Scientific research has begun to reflect the understanding that sex assigned at birth and gender identity may be different, following decades of misuse and conflation of these terms.7–9 Sex assigned at birth is sometimes problematically called “biological sex.” Throughout this article, we use the phrase “sex assigned at birth” instead of “biological sex” as recommended by the Endocrine Society Clinical Practice Guidelines. 10 The phrase “biological sex” is imprecise and problematic, particularly because “sex assigned at birth may or may not correspond, within a person and over time, with chromosomes, hormones, secondary sex characteristics, genitalia and/or reproductive organs, and not all components of our biology are included in what we describe as sex.” 11 (p765) Sex assigned at birth is generally classified as male, female, or intersex (sometimes referred to as variations in sex traits or intersex variations), based on external genitalia, which often represent various biological features (e.g., genes, hormones, secondary sex characteristics). Importantly, however, these characteristics may change over time, without a clear boundary between male and female. Thus, sex is to some degree a “socially constructed classification based on expectations of ‘biological normalcy.’”(11, p764) Gender identity, on the contrary, is an “overarching category that refers to the components of gender that correspond to a person’s sense of self in relation to their felt and inner sense of gender.”(11, p766)
Cisgender individuals experience their gender as congruent to their sex assigned at birth. Gender-diverse individuals experience their gender identity as different from their sex assigned at birth, including, for example, those who are transgender and/or nonbinary. Some gender-diverse individuals have gender identities that both overlap with and extend beyond their sex assigned at birth (e.g., someone assigned female at birth [AFAB] who identifies as both female and gender neutral). Gender diversity is distinct from gender dysphoria (referred to as gender identity disorder [GID] before 2013), which is defined in the Diagnostic and Statistical Manual of Mental Disorders as a diagnostic category characterized by clinically significant distress related to incongruence between one’s sex assigned at birth and one’s internal gender identity. 12 Some, but not all of those who are gender diverse, experience gender dysphoria.
Prevalence of gender diversity in the general population
Prevalence estimates of gender diversity in the general population vary across studies, time, and geographic location due to differing methods, definitions (e.g., gender diversity vs. gender dysphoria), and cultural contexts. 13 In a review of national surveys of transgender identity from a US sample between 2007 and 2015, Meerwijk and Sevelius estimated a transgender population of 390 out of 100,000 (0.39%) adults. 14 Another US report estimated the proportion of transgender individuals to be 0.5% of adults and 1.4% of youth ages 13–17 years. 15 This is in contrast to a Pew Center Survey, which found that 1.6% of adults in the United States reported being transgender or nonbinary. 16 It is possible that this prevalence discrepancy is due to how the questions were asked (e.g., use of the word “transgender” only in the former survey vs. a broader description of gender diversity in the latter survey). A review of studies from multiple countries estimated the proportion of gender diversity in the general adult population to be between 0.5 and 4.5%, 17 however, each study used different definitions and methodologies.
Prevalence of autism in gender-diverse individuals
A growing literature points to an overlap between gender diversity and autism.6,18,19 Most studies that explore the relationship between gender identity and autism focus on the prevalence of diagnosed autism and/or autistic traits in adolescents who have been referred to gender clinics (i.e., gender-referred individuals). Studies of gender-referred youth in the United States, England, and the Netherlands report autism prevalence rates between 6% and 13% when autism diagnostic procedures are implemented, 20 which contrasts with documented prevalence rates of autism in 2.8% of children in the United States. 21 In addition, van der Miesen, de Vries, and colleagues found that 14.5% of children and adolescents (n = 542) referred for gender dysphoria in the Netherlands had clinically significant characteristics of autism. 22 In a nonclinical sample of over 2000 children (without a developmental/mental health diagnosis) ages 6–12, in Canada, gender diversity was associated with higher levels of at least some autistic traits. 23
In older adolescents and adults, Warrier and colleagues examined the relationship between gender diversity and autism or autistic traits across five large UK-based datasets (including over 600,000 individuals) and found that the odds of being autistic were 3.03 to 6.36 times greater among gender-diverse individuals than among cisgender peers. 6 In their study, Stagg and Vincent reported that gender-diverse adults demonstrated higher levels of autistic traits and autism diagnoses than cisgender participants. 24 Another study of adults found that not only did autistic transgender people report higher levels of autistic traits than autistic cisgender people, but also that nonautistic transgender individuals reported more autistic traits than their nonautistic cisgender peers. 3
Prevalence of gender diversity in autistic individuals
In addition to the literature investigating autism and autistic traits in gender-diverse individuals, several studies explore rates of gender diversity in autistic individuals, although none to date examined US-based adults. Strang and colleagues investigated “gender variance” in children and adolescents with and without neurodevelopmental conditions in the Washington DC area of the United States. 25 They found that parents of autistic participants were 7.59 times more likely to report gender variance in their children (as defined by their child’s desire to be of the opposite sex) than parents of children without neurodevelopmental conditions. In a study of children aged 10–13 years in the Central Southern United States, both autistic children and their parents reported higher levels of gender diversity among the autistic children than was reported in the nonautistic comparison group. 26 A study examining electronic records (n = 919,898) from pediatric hospitals in the United States found that the odds of an adolescent (defined as 9–18 years old) being diagnosed with gender dysphoria were three times higher among those who had an autism diagnosis compared with those who did not. 27
In their study of autistic adolescents and adults (n = 675) from the Netherlands Autism Register, Walsh and colleagues reported a rate of trans and nonbinary identities of 15%. 28 In the same dataset, Dewinter and colleagues provided a detailed characterization of the breakdown of the participants’ endorsement of each gender identity response option. 29 Although the rates differed for people who were AFAB (21.6% reporting gender diversity) versus people who were assigned male at birth (AMAB) (7.8%), both groups evidenced an overrepresentation of gender diversity. In comparison, just 3.9% of the general population in the Netherlands had a trans or nonbinary identity. 30 A subsequent study found that 6.5% of autistic adolescents (n = 573) and 11.4% of autistic adults (n = 807) self-reported a desire to be a gender different from their sex assigned at birth, compared with 3.1% of adolescents aged 11–18 years old in the control sample from the general population. 31 In a study examining gender identity in adult females, autistic females were more likely to report being gender diverse (19.4%) than their nonautistic female counterparts (8.7%). 32
Mental health, gender diversity, and autism
A significant body of literature reports higher rates of mental health challenges among gender-diverse adults33–36 and adolescents37–39 compared with their cisgender peers. This includes elevations in suicidality, depression, and anxiety, among other psychiatric conditions. For example, Stanton and colleagues, 36 in examining self-report measures in medical records from 2015 to 2018, found that between 44% and 56% of gender-diverse adults (n = 29,988) at a large community health center in the United States met clinical cutoffs for anxiety and/or depression, compared with 30% of cisgender adults.
In addition, adolescents and young adults who are both gender diverse and autistic (or who have high levels of autistic traits) have been found to exhibit higher levels of internalizing conditions, such as anxiety and depression, than their peers who are only either gender diverse or autistic.5,40–42 Minority stress and societal pressures to conform to norms, 43 as well as stressful life experiences, including hostile environments, discrimination, victimization, marginalization, and abuse, provide potential explanations for elevated vulnerabilities for a range of psychiatric challenges. 6 Individuals who are both gender diverse and autistic may be particularly vulnerable to mental health issues, and may require specialized health care services and psychological supports, especially in the absence of societal-level change. Understanding more about the prevalence of mental health conditions, especially among autistic adults who are gender diverse, may lead to increased awareness among medical and mental health practitioners, of potential concerns, and ultimately specialized support strategies, that could lead to improved care outcomes for this population.
Current study
No studies to date examine the prevalence of gender diversity in US-based autistic adults, and there is limited information regarding the prevalence of anxiety and mood disorders comparing autistic gender-diverse and autistic cisgender adults in the United States. Based on this gap in the literature, and the realization that we had already obtained data that would address this topic, we decided to conduct a retrospective study. In this study, we report the prevalence of gender diversity in autistic adults in the United States in both an original and a replication sample. We also examine prevalence of anxiety and mood disorders in both samples, comparing autistic gender-diverse and autistic cisgender adults. In addition, in both datasets, we explored whether there were differences in the proportion of each sex assigned at birth (male or female) within the gender-diverse groups. Specifically, we first retrospectively looked at gender identity data from an experimental study on a topic unrelated to gender diversity. Our research team conducted the experimental study from 2020 to 2021 (Dataset 1, n = 205). We next sought to replicate our findings by investigating independent data from an experimental study that our research team conducted in 2022 (Dataset 2, n = 243). For Dataset 2, we hypothesized that we would find similar rates of gender diversity (approximately 16%) and anxiety and mood disorders as we found in Dataset 1.
Methods
Study 1 (i.e., from which Dataset 1 was derived; preregistered at https://osf.io/hdyrm), conducted between 2020 and 2021, recruited autistic adults for up to three sessions of online experiments investigating predictive processing. Study 2 (i.e., from which Dataset 2 was derived; preregistered at https://osf.io/be8fc/), conducted in 2022, recruited autistic adults for a one-session online experiment investigating motor entrainment to auditory stimuli. Both preregistrations described the experimental studies mentioned, not the research questions in the current article. Following consenting, all potential participants were invited to complete a screening questionnaire to determine eligibility before participating in the study sessions mentioned above. Participant data for the current study were obtained from these two online studies. We used Dataset 2 to compare rates of gender diversity with the first cohort in Dataset 1, consistent with an increasing call for reproducibility and replication in psychological science.44,45 Participants completed the components of each study session online via a desktop or laptop computer.
The current study summarizes gender identity and mental health data from all participants who responded to the initial screening questionnaire for either online study. The screening questionnaire was not designed to investigate any additional questions about the clinical needs or experiences of the autistic participants related to their gender identity; therefore, these issues are not addressed in this article. The topic of gender identity was not included in any advertisements for the studies. The results of the experimental task sessions are reported in separate articles46,47 (as well as Cannon et al., under review). In both studies, we also recruited nonautistic adults to participate in the experimental task sessions.
Both studies were approved by the Massachusetts Institute of Technology Committee on the Use of Humans as Experimental Subjects. The research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. All individuals provided written informed consent before participating. They were able to cease participation at any time and were compensated for the portion of the study that they completed.
Nonautistic participant data
While we did obtain data about gender identity from a nonautistic control group for both studies, we did not report the nonautistic participants here as a formal comparison group because they were recruited via Prolific, an online platform based in the United Kingdom, which included a considerable number of individuals who did not reside in the United States. We were not able to separate out data for non-US-based individuals in Dataset 1 because Prolific limits researchers’ access to participant-level geographic location information. We were only able to obtain geographic information for individuals who completed the experiment, which did not include all individuals who completed the screening questionnaire (which contained the questions about sex assigned at birth and gender identity). See Supplementary Material for details.
Participants
We recruited the autistic adults included in both datasets through SPARK (Simons Foundation Powering Autism Research for Knowledge). The SPARK database currently consists of over 100,000 autistic individuals (>20,000 adults) residing in the United States, includes phenotypic and genetic data, 48 and is confirmed to have a high degree of autism diagnosis validity. 49 Autism diagnosis was ascertained at the time of participants’ registration in SPARK. In addition, since both studies involved a nonautistic comparison group, we aimed to match the assigned sex ratios and mean ages of the autistic group participants who completed the experiment(s) to the nonautistic group participants who completed the experiment(s). The nonautistic participants who completed the experiment(s) were recruited earlier in the studies’ time lines and had relatively equal assigned sex ratios. Therefore, to obtain the final samples with relatively equal assigned sex ratios within the autistic groups as well, we requested that SPARK recruit particular numbers of adults who were AFAB and AMAB. Specifically, we asked SPARK to overrecruit individuals who were AMAB, since more individuals who were AFAB would have otherwise participated. This is because more individuals who were AFAB tend to participate in SPARK’s studies (J. Toroney, MHS, email communication, January, 13, 2021). The final sex assigned at birth percentages of autistic adults are as follows: for Dataset 1, AFAB = 47.8%; AMAB = 52.2%; and for Dataset 2, AFAB = 51.4%; AMAB = 48.6%.
Group-level autistic participant demographic characteristics for Datasets 1 and 2 are reported in Tables 1 and 2. Participant data regarding race and factors associated with socioeconomic status (reported in Table 2) were retrospectively obtained from SPARK for the participants in our study for whom it was available. It was not collected in the initial questionnaire during the two experimental studies. Supplementary Table S1 includes the detailed racial demographics of participants who identified as more than one race. For both datasets, when participants completed the screening questionnaire more than once for the same study, experimenters only included the first response to the questionnaire in analyses. In the initial study (Dataset 1), 324 autistic individuals in SPARK agreed to be contacted by the researchers about the study, and 205 (20–46 years) consented and completed screeners. In the second (replication) study (Dataset 2), 515 autistic individuals agreed to be contacted about the study and 277 adults (aged 18–44 years) consented and completed screeners. One person was excluded from the analyses because they abstained from answering the question about gender identity. To avoid duplication, experimenters excluded from Dataset 2 any participant who completed the second study screening questionnaire but had already been included in Dataset 1 analyses (n = 33). Following these exclusions, Dataset 2 totaled 243 participants.
Numbers, Percentages, and Ages of Autistic Cisgender and Autistic Gender-Diverse Participants
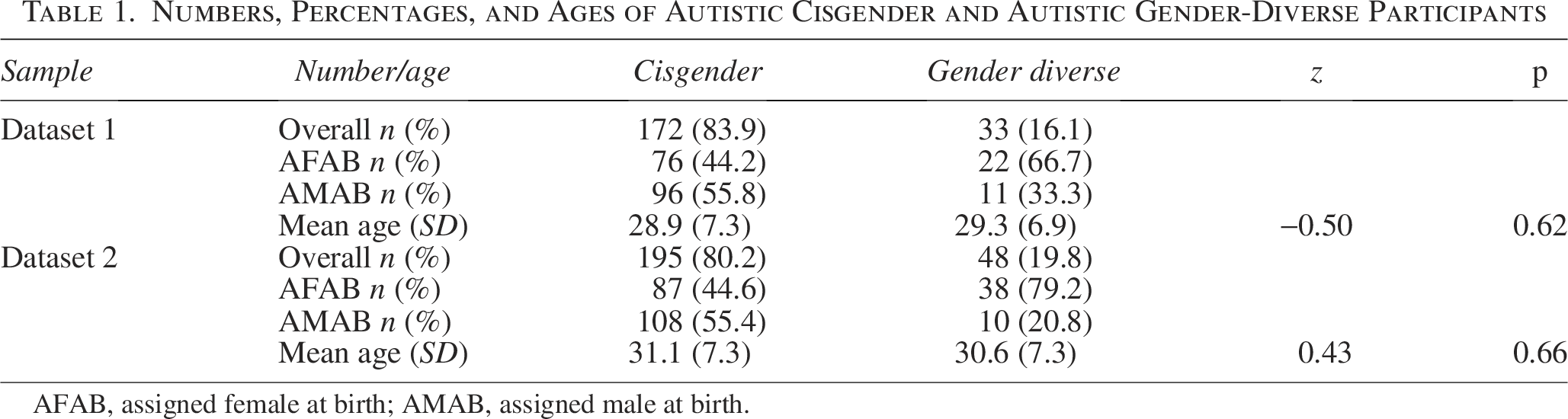
AFAB, assigned female at birth; AMAB, assigned male at birth.
Race, Highest Education Level, and Annual Household Income of Autistic Participants
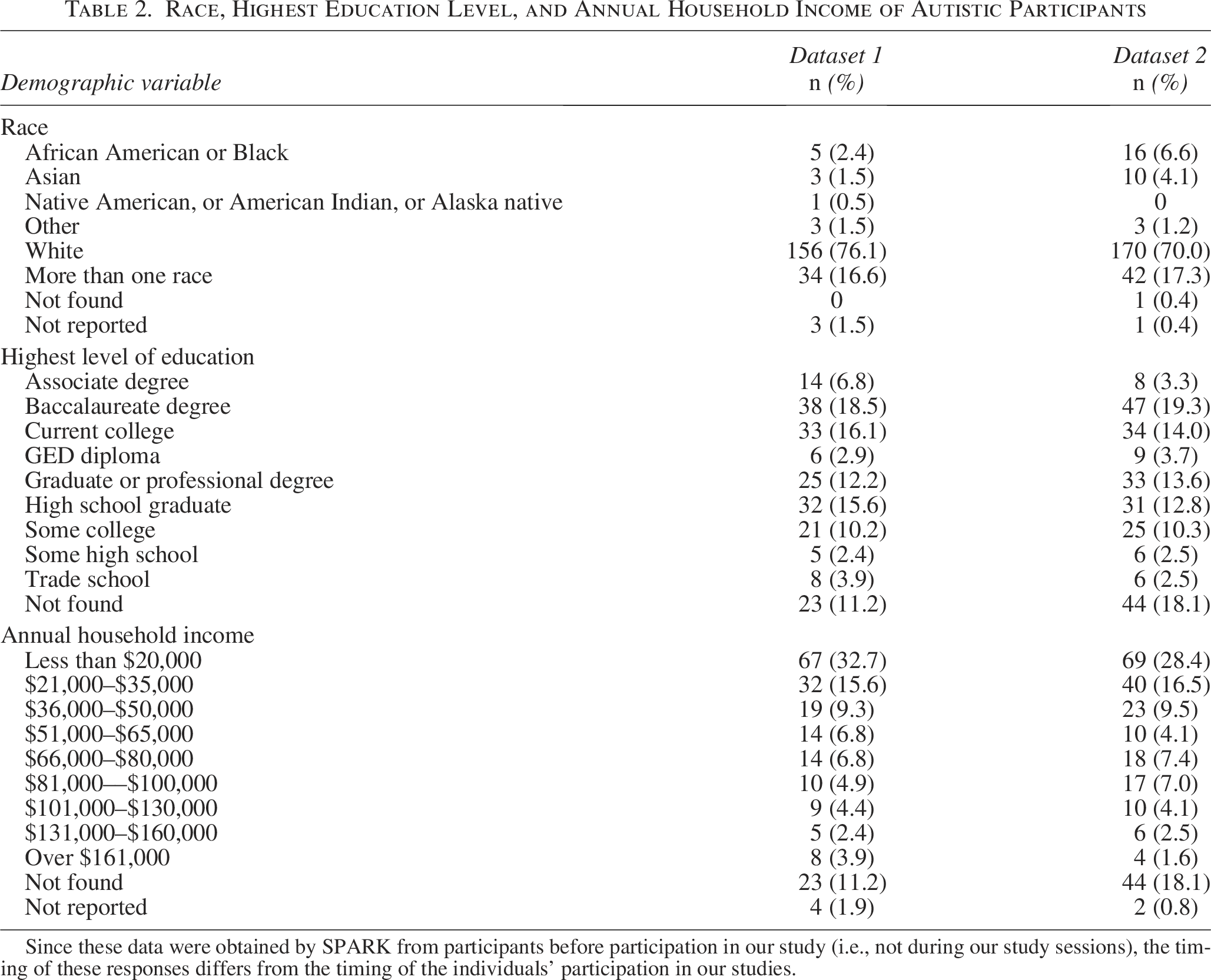
Since these data were obtained by SPARK from participants before participation in our study (i.e., not during our study sessions), the timing of these responses differs from the timing of the individuals’ participation in our studies.
Inclusion/exclusion
The SPARK team applied prescreening criteria to records in their database to generate a pool of participants who met the following initial criteria: legally independent adults; aged 18 years to 45 years and 11 months; with a professional diagnosis of autism; and no history of seizures, prematurity (born at 36 weeks or earlier), vision conditions, or head injury with hospitalization.
Characterization measures
We collected information about participants’ sex assigned at birth and gender identity through responses provided on the screening questionnaires, which consisted of the same questions for both datasets. We obtained sex assigned at birth from the question “What was your assigned biological sex at birth?” The response options provided were as follows: male, female, or intersex. In addition, we obtained participants’ gender identity from the question, “What gender(s) do you identify with?” in accordance with assessment approaches developed for an autism and vulnerability survey. 50 Participants were asked to select any of the following options that applied: female, male, gender neutral, nonbinary, not listed (please state). We coded individuals as “cisgender” if there was total congruence in their responses to both questions, and coded individuals as “gender diverse” if there was any incongruence in their responses to both questions. We acquired information about mood and anxiety disorders from a separate question in which participants were asked to “Please select all mood or anxiety disorders that you have been diagnosed with by a professional: anxiety disorder (panic, phobia, generalized anxiety disorder, social anxiety, obsessive compulsive disorder), depression or dysthymia, bipolar (manic depressive) disorder” including an “other” category, which they were asked to describe. We included obsessive compulsive disorder in the list of anxiety disorders in the survey, although in the DSM-5 it was moved from “anxiety disorders” to “obsessive compulsive and related disorders.” 12 In addition, the wording of the question did not specify a time frame of the mood or anxiety disorder diagnosis.
Analyses
We conducted statistical analyses with STATA software. 51 We examined descriptive statistics, including frequencies of sex assigned at birth (AFAB and AMAB), gender-diverse and cisgender identities, and anxiety and mood disorders. Due to non normality of the age variables, we performed the Mann–Whitney U tests to determine whether there were age differences between the cisgender and gender-diverse individuals in each dataset (p < 0.05). We also calculated odds ratios to determine the odds of autistic gender-diverse adults having been AFAB versus AMAB, as well as the odds of autistic gender-diverse versus cisgender individuals reporting an anxiety and/or mood disorder and the odds of them reporting an anxiety and mood disorder.
Results
Proportion of gender-diverse identities in autistic adults
Dataset 1
In Dataset 1, 16.1% of the autistic adults are gender diverse (Fig. 1). Of those who reported having been AFAB, 22.4% are gender diverse compared with 10.3% of those who reported having been AMAB. The most commonly reported gender-diverse gender was nonbinary. Participants’ gender-diverse identities are shown in Table 3. No individuals reported having intersex variations as their sex assigned at birth. The odds of an autistic adult who was AFAB being gender diverse were 2.53 times higher than the odds of an autistic adult who was AMAB being gender diverse (95% CI, 1.09–6.12). The Mann–Whitney U test showed no age difference (z = −0.50, p = 0.62) between the gender-diverse and cisgender adults. Most gender-diverse participants were in their late 20s (Table 1).
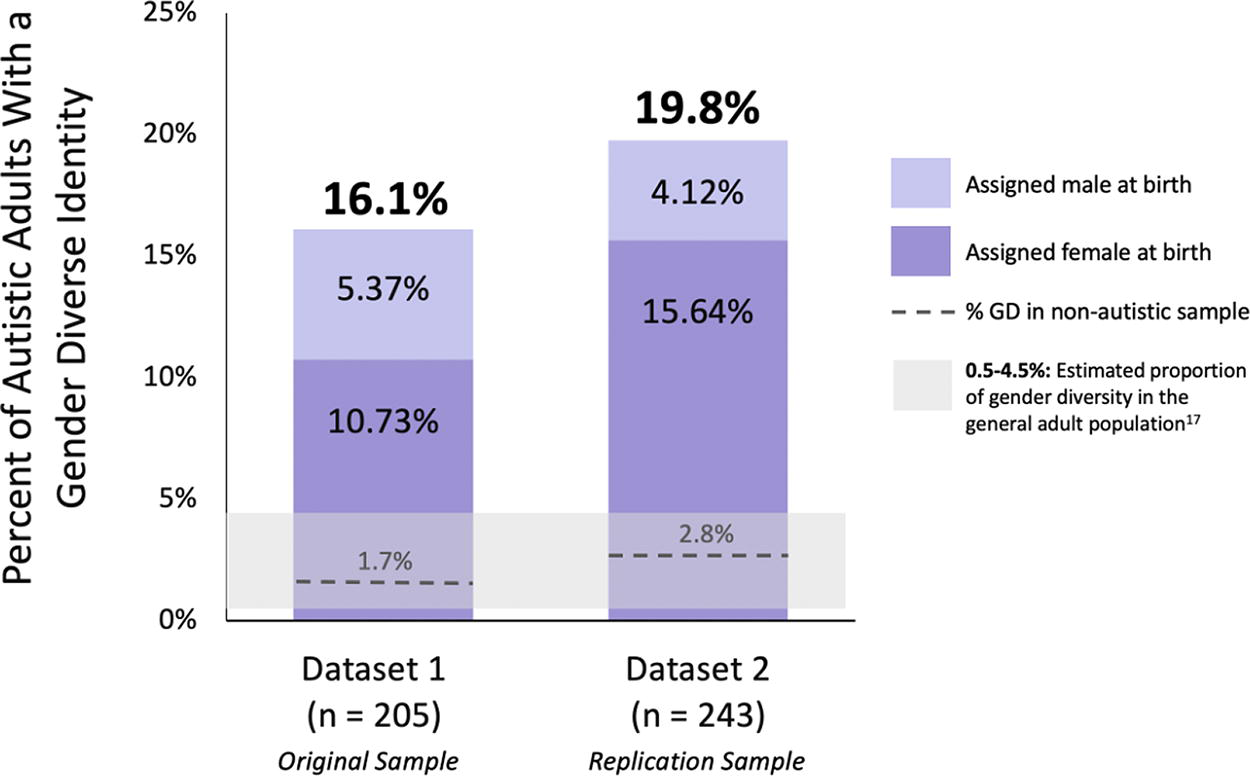
Percentages of gender-diverse autistic adults in the United States, with reference data for gender diversity in nonautistic adults and the general adult population across multiple countries. Note: See Supplementary Material for details about the nonautistic adults.
Gender-Diverse Identities in Autistic Adults
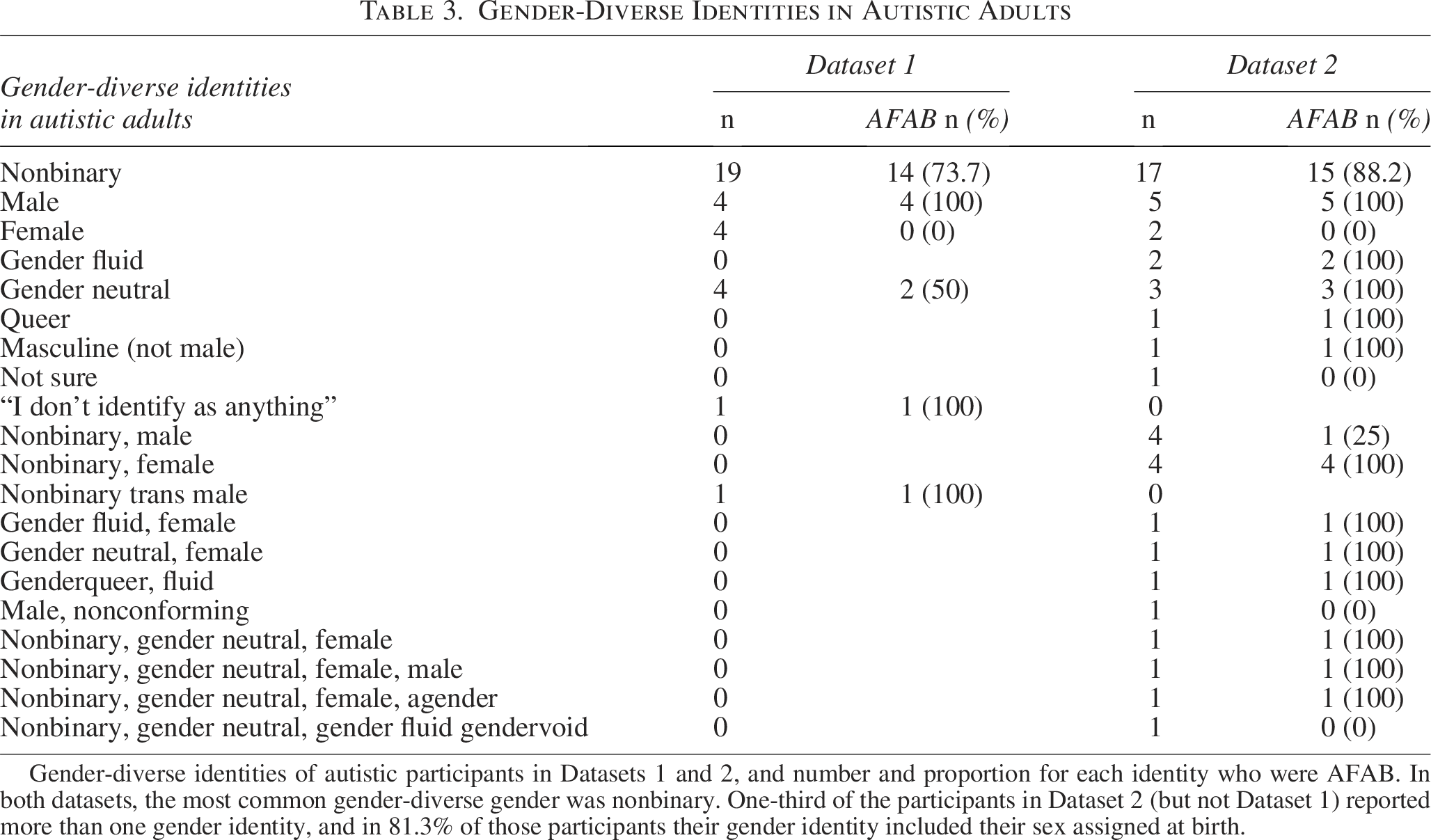
Gender-diverse identities of autistic participants in Datasets 1 and 2, and number and proportion for each identity who were AFAB. In both datasets, the most common gender-diverse gender was nonbinary. One-third of the participants in Dataset 2 (but not Dataset 1) reported more than one gender identity, and in 81.3% of those participants their gender identity included their sex assigned at birth.
Dataset 2
In Dataset 2, 19.8% of the autistic adults are gender diverse (see Fig. 1). Of those who reported having been AFAB, 30.4% are gender diverse compared with 8.5% of those who reported having been AMAB. The most commonly reported gender-diverse gender was nonbinary (Table 3). No individuals reported having intersex variations as their sex assigned at birth. The odds of an autistic adult who was AFAB being gender diverse were 4.72 times higher than the odds of an autistic adult who was AMAB being gender diverse (95% CI, 2.14–11.17). There was no age difference between the cisgender and gender-diverse individuals in the Mann–Whitney U test: z = 0.43, p = 0.66, with most of the gender-diverse adults being in their early 30s (Table 1).
Co-occurring anxiety and mood disorders in autistic adults
Dataset 1
Of the entire autistic sample in Dataset 1, 74.6% reported having a diagnosis of at least one anxiety and/or mood disorder. Notably, 93.9% of the gender-diverse autistic adults reported an anxiety and/or mood disorder (see Supplementary Table S2 for details). Gender-diverse autistic adults exhibited a greater likelihood of self-reporting a diagnosis of anxiety and/or mood disorder compared with their cisgender autistic peers. The odds of a gender-diverse autistic adult reporting an anxiety and/or mood disorder were over six times higher than the odds of a cisgender autistic adult reporting an anxiety and/or mood disorder (odds ratio = 6.35; 95% CI, 1.51–56.46). In addition, the odds of a gender diverse autistic adult reporting both an anxiety and mood disorder were three times as high as the odds of a cisgender autistic adult reporting both an anxiety and mood disorder (odds ratio = 3.00; 95% CI, 1.25–7.73).
Dataset 2
Overall, 78.2% of the autistic adults in Dataset 2 reported being diagnosed with an anxiety and/or mood disorder, whereas 93.8% of the gender-diverse autistic adults reported an anxiety and/or mood disorder (see Supplementary Table S2 for details). The gender-diverse autistic individuals were more likely to have an anxiety and/or mood disorder than the cisgender autistic individuals (odds ratio = 5.17; 95% CI, 1.54–27.02). Furthermore, the odds of a gender-diverse autistic adult reporting both an anxiety and mood disorder were almost two times higher than the odds of a cisgender autistic adult reporting both an anxiety and mood disorder (odds ratio = 1.98; 95% CI, 0.98–4.12).
Discussion
In the present study, 16.1% and 19.8% of two US-based autistic adult samples exhibited incongruence between their reported sex assigned at birth and gender identity. These are among the highest rates of gender diversity reported in an adult autistic sample to date. Specifically, they range from at least 4 to upward of 30 times higher than the rates in the general global population. 17 Furthermore, they are approximately 6–11 times higher than the rates in our nonautistic samples who participated during the same time period and were matched on age and sex assigned at birth, differing only in geographical location. The present prevalence rates emerged from two online research studies (completely unrelated to gender identity) that surveyed both gender identity and sex assigned at birth in all participants who completed the studies’ screening survey. These findings, the first in a US-based autistic adult sample, add to the growing body of literature highlighting a strong association between gender diversity and autism.
It is noteworthy that one-third of the gender-diverse participants in Dataset 2 (but none in Dataset 1) reported more than one gender identity. In addition, we found an increased odds ratio of gender diversity for autistic adults who were AFAB compared with adults who were AMAB, consistent with prior results. 28 Importantly, however, compared with the nonautistic sample, gender diversity was overrepresented in the autistic sample, in both those who were AFAB and those who were AMAB (see Supplementary Table S3). Furthermore, in contrast to prior research which suggests that approximately 1.7% of individuals in the general population are intersex,52,53 and that a much higher overlap exists between individuals who are intersex and gender diverse, 54 none of our participants reported being intersex. It is possible that our finding of no reported intersex variation may be due to having included intersex as a third option to the question about assigned sex at birth, instead of including it as a separate question as recommended, 55 since most people who have an intersex variation are not assigned intersex at birth. 55
Mental health and gender diversity
In both of our autistic samples, approximately 94% of the gender-diverse adults reported an anxiety and/or mood disorder. This is considerably higher than that of the gender-diverse population at large. 36 This is also in marked contrast to the 0% of anxiety and/or mood disorders reported by the nonautistic gender-diverse adults in both samples of our study (n = 7 nonautistic gender-diverse adults, in both samples combined; see Supplementary Table S4). Furthermore, in our samples, the odds ratio of a gender-diverse autistic individual reporting an anxiety and/or mood disorder was up to 6.35 times that of the odds of a cisgender autistic individual reporting an anxiety and/or mood disorder. This is consistent with findings showing that adolescents and young adults who are both gender diverse and autistic (or who present with a high level of autistic traits) exhibit higher levels of mental health conditions, such as anxiety and depression, than their peers who are only either gender diverse or autistic.5,40–42 Therefore, individuals who are both gender diverse and autistic may be particularly vulnerable to mental health challenges and may benefit from specialized supports.5,56
Recent literature about medical education practices highlights a substantial need to improve training related to gender diversity for medical providers to improve quality of care and reduce barriers to care for gender-diverse individuals.57–60 Gender-diverse patients have reported that they prefer a health care provider who is empathetic, knowledgeable on gender and/or sexuality issues, accepting, and provides gender-affirming care. 61 Bruce and colleagues examined the experiences of autistic adults with gender-diverse identities in accessing gender identity health care. 62 They found that the most significant contributor to participants having a positive health care experience was how knowledgeable the professional was not only about gender identity health care but also about gender-diverse identities and autism. However, autistic individuals may have difficulties accessing adequate mental health support due to limitations in mental health clinicians’ specialized knowledge and expertise about autism, especially among clinicians who work primarily with adults. Although 70.7% of psychotherapists were open to treating an autistic adult, a significant proportion of therapists (53%) reported knowing very little about psychotherapeutic approaches intended for autistic adults. 63 In an in-depth interview-based study of 22 autistic gender-diverse adolescents, almost 70% of the participants said that medical gender-related care was important for them. 20 In the same study, 32% of autistic gender-diverse participants said that their gender identity had been questioned because of their autism diagnosis.
Given the common intersection of autism and gender diversity, an intersectional care approach that accounts for this overlap may improve outcomes for some gender-diverse individuals. 64 Intersectional approaches emphasize the overlap and interaction between multiple identities and systemic factors that impact health and social experiences. 65 As related to individuals with autism and gender diversity, this should include strategies such as specialized training for clinicians, 66 increased collaboration across specialties, and interdisciplinary care approaches that help individuals achieve their gender-related goals while taking into account the individual’s neurodiverse profile, 67 which may include challenges with executive function, social communication, and other neurocognitive features related to autism that may impact their ability to navigate gender-related needs. 5 There have been calls for multipronged and evidence-based approaches to mental health care for gender-diverse people broadly, 43 and more specifically for gender-diverse autistic individuals, 68 but much more work is needed. For individuals who are both autistic and gender diverse, treating the often-intersecting mental health issues is a critical component of their overall and gender-related care. 68 Furthermore, providing clinical training that addresses issues specific to gender-diverse identities and autism may improve the overall health care and mental health support to members of the gender-diverse autistic community and reduce gender- and neurodiversity-based minority stresses.
Limitations
The present study should be considered within the context of several limitations. The gender-based results presented in this study were derived from online studies in adults with and without a diagnosis of autism, however, we did not formally compare the nonautistic adults with the autistic samples since not all individuals in the nonautistic samples resided in the United States. It is a limitation of the study that we were unable to include the data from the nonautistic samples in our primary analyses. Also, demographic data regarding race, ethnicity, and socioeconomic status were not collected in the screening questionnaire before the experiment sessions. Therefore, we retroactively obtained the relevant data that were available from the SPARK database for participants in our studies.
Our findings may not generalize to populations outside the United States due to variability in cultural and religious norms. Despite this, our findings align with other studies, including several with larger samples.25,28,29,31,32 In addition, both datasets reported in the present study were recruited with relatively equal ratios of male and female individuals based on self-reported sex assigned at birth. This is in contrast to the assigned sex ratios typically reported in the autism literature. 69 As a result, the present study has a high proportion of autistic adults who were AFAB compared with previous studies. This may limit the generalizability of these findings to a general autistic adult population. On the contrary, some studies have identified factors related to the underdiagnosis of autism in females, so the increased representation of females in our sample may also be a relative strength. Furthermore, given that approximately 50% of our autistic sample was AFAB, this may influence the higher overall prevalence of gender diversity within our autistic sample compared with other studies, especially considering that the present study and others found higher rates of gender diversity in autistic individuals who were AFAB.31,32
There is currently mixed and evolving gender terminology used in survey methods. For example, some surveys use the terms “male” and “female,”55,70 whereas others use “man” and “woman” in the wording of gender identity questions because male and female are considered sex-related terms. 55 While many recommend the two-step method of characterizing gender identities,55,71 the approach of directly asking whether someone is transgender/gender diverse has the advantage of eliminating the need to ask about sex assigned at birth, which some participants feel is not pertinent to their gender identity. 71
The participants in this study all had a professional diagnosis of autism; individuals with self-diagnoses were not included. Our results therefore do not reflect those who face barriers in seeking and obtaining an autism diagnosis and who would otherwise be professionally diagnosed.72–75 Furthermore, the mental health information is based on a diagnosis of mental health issues that does not specify a time frame, and thus may not pertain specifically to participants’ current mental health diagnoses.
In addition, we recognize the importance of engaging autistic and gender-diverse collaborators throughout the research process. We acknowledge that not having a diverse array of perspectives is a limitation of the study. Furthermore, we acknowledge that we did not make a concerted effort to recruit individuals who are autistic and/or gender diverse as part of the research team. This is a major limitation of the study. In the future, we will address this by implementing a plan during the initial phase of the study design as to how to ensure involvement of community-based collaborators in the research process.
Future Directions
The present study, along with the growing body of literature demonstrating the common co-occurrence of gender diversity and autism, suggests a need for clearly distinguishing between sex assigned at birth and gender identity in autism research study participants. Many autism research studies group participants using only “sex” or “gender” as categories, and do not clarify those terms or how the data were obtained. Given the growing literature showing proportional overrepresentation of gender diversity in autism, it is important that autism researchers be inclusive of, and report on, all gender identities within their samples and should consider using measures such as the Gender Self-Report to more comprehensively characterize gender. 76 This is especially important for work investigating “sex differences” and the “female” [sic] autism phenotype. The phrase “female autism phenotype” does not affirm genders other than female (e.g., trans males, nonbinary individuals) who may share this phenotype with cisgender autistic girls/women. Lai and colleagues proposed the term “nuanced autism phenotype” as an alternative, based on an emerging conceptualization of a subset of autistic individuals who present with a unique set of characteristics. 77 Characterizing both sex assigned at birth and gender identity could enhance our understanding of sex- and gender-related topics from a more inclusive framework. It is equally important to account for and understand the prevalence of gender-diverse identities in broader autism research as well (i.e., beyond studies that investigate sex- and gender-related topics).
Our results emphasize the importance of including a “not listed, please state” category (as recommended by Steinberg and colleagues) 71 or the option of “I use a different term,” 55 as well as allowing individuals to choose as many identities as apply, to most accurately capture how individuals describe their gender identity. The growing literature regarding the connection between autism and gender diversity highlights that assuming congruence between sex assigned at birth and gender identity within autistic samples will not accurately or comprehensively characterize these populations.
This study demonstrates that the addition of demographic questions related to both sex assigned at birth and gender identity allows for better characterization of participant samples in autism research. Adding these questions to future autism research studies would allow for improved understanding of gender-diverse autistic individuals and their unique experiences. An additional benefit of obtaining both sex assigned at birth and gender identity data as standard protocol in study design is that future studies and meta-analyses can analyze experimental results based on gender identity, as well as sex assigned at birth, to examine potential sex assigned at birth and gender identity-based differences.
Furthermore, a participatory approach that includes gender-diverse autistic individuals as collaborators in future research would better reflect the needs and lived experiences of this population, and account for certain biases that nonautistic and/or cisgender autistic researchers may bring to the process. 78 This approach can include collaborators who are part of the research team, as well as those who provide valuable input through focus groups or consultation, for example. It is important to provide compensation to such collaborators (i.e., those who are not already part of the research team) so that they are fairly paid for their time and input.
Conclusion
Our findings of a proportional overrepresentation of gender diversity in two US-based autistic adult samples add to the literature highlighting the co-occurrence of gender diversity and autism. In addition, our study extends previous findings by showing increased likelihood of anxiety and/or mood diagnoses in gender-diverse autistic individuals relative to cisgender autistic individuals. Given the growing body of research highlighting the connection between autism and gender diversity, it is important that future studies accurately characterize gender identity and sex assigned at birth. This may improve the interpretability, validity, and relevance of future autism research, and clarify previous claims about “sex-based” differences that may not have used precisely defined categories and terminology. Future research should also move beyond prevalence studies to investigate the needs and challenges experienced by gender-diverse autistic individuals, as well as strategies for improving care, such as increased specialized training and translational dialogue between gender and autism specialists. Scientific research that comprehensively examines the lived experiences of gender-diverse autistic individuals will enhance both gender- and neurodiversity-affirming clinical care and may lead to improved quality of life for this population.
Footnotes
Acknowledgments
The authors thank the individuals who participated in this research study. They appreciate the SPARK Research Match program, which facilitated outreach to, and characterization of, autistic participants. The authors also appreciate obtaining access to recruit participants through SPARK research match on SFARI Base.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Hock E. Tan and K. Lisa Yang Center for Autism Research for support of the autism outreach coordinator (to C.E.L.) and the Simons Center for the Social Brain at MIT for the grant Predictive Processes in Autistic and Neuro-typical Individuals: A Behavioral, Neural and Developmental Investigation (to P.S. and J.D.E.G.).
Author Note
L.B. is now at The Donald and Barbara Zucker School of Medicine, Hofstra University, Hempstead, NY.
J.C. is now at the Department of Psychology, Neuroscience, and Behaviour, McMaster University, Hamilton, Ontario.
Data Availability Statement
Data used in this study will be made available upon reasonable request.
Authorship Confirmation Statement
L.B., A.L.C., C.E.L., A.M.O., and J.S. contributed to the conception of this study. L.B. and C.E.L. contributed data for analysis. C.E.L. conducted the data analysis. L.B., A.L.C., C.E.L., A.M.O., J.S., P.S., and J.D.E.G., conducted the interpretation of results. All authors revised the article and approved of the final version for publication. The article has been submitted solely to this journal and is not published, in press, or submitted elsewhere.