
Abstract
Background:
There is widespread debate about the language used to describe autistic people; many professionals prefer person-first language (e.g., “person with autism”), and many autistic people prefer identity-first language (e.g., “autistic person”). Although prior surveys of the autism community’s terminology preferences have reported participants’ evaluations of individual terms, limited research has directly compared evaluations of discrete categories of identity- and person-first terms. Additionally, there is a need to more fully understand participants’ evaluations of terms relevant to autistic people outside of the identity- and person-first debate.
Methods:
In total, 784 North American adults (Nautistic = 611; 78%) evaluated two identity-first terms (“autistic” and “autistic person”) and five person-first terms (“person with autism,” “person with autism spectrum disorder,” “person with autism spectrum condition,” “person on the autism spectrum,” and “person diagnosed with autism”). Participants reported which terms they would use, ranked the terms in order of their preference, and rated how much they liked each term and how offensive each term was. In open-ended responses, participants explained their highest and lowest rankings and provided definitions of (the autism) “spectrum,” “high functioning,” and “low functioning.”
Results:
Both autistic and non-autistic participants were more likely to use identity-first terms than person-first terms, ranked identity-first terms more highly than person-first terms, and liked identity-first terms more than person-first terms. Participants’ open-ended responses provided some context for the quantitative findings and highlighted their critical views of functioning labels.
Conclusion:
Consistent with other recent work with different samples and different methodologies, the North American participants in the current study preferred identity-first terms over person-first terms. That said, there was variability, with some autistic and non-autistic participants strongly preferring person-first terms. We end by providing recommendations on incorporating our findings into future research and practice.
Community Brief
Why is this an important issue?
The words that are used to describe groups of people can influence how others view and treat those groups. Autistic people should have a say in the words that are used to describe them, so it is important to know how autistic people want to be talked about.
What was the purpose of this study?
The purpose of this study was to learn more about what autistic people think about words used to talk about autistic people. We also asked non-autistic people who know autistic people about their opinions to see if these opinions were similar or different from autistic people’s opinions.
What did the researchers do?
We conducted a survey with 784 adults (611 of whom were autistic) living in North America. In the survey, the adults shared their opinions about two identity-first terms (“autistic” and “autistic person”) and five person-first terms (“person with autism,” “person with autism spectrum disorder,” “person with autism spectrum condition,” “person on the autism spectrum,” and “person diagnosed with autism”). They told the researchers which terms they would use, which terms were their favorite and least favorite terms (and why), how much they liked each term, and how offensive each term was. The adults in this study also shared what (the autism) “spectrum,” “high functioning,” and “low functioning” meant to them.
What were the results of the study?
Most of the people in this study preferred identity-first language more than person-first language: They liked identity-first language more, used it more, and ranked it more highly than person-first language. There was some variety in people’s opinions, so not everyone liked identity-first language better than person-first language. Most participants had negative opinions of functioning labels such as “high functioning” and “low functioning,” and they defined the autism “spectrum” in many different ways.
What do these findings add to what was already known?
These findings can help us be more confident that autistic people, overall, prefer identity-first terms. We also learned about some of the reasons for participants’ opinions about autism-related language. This information can help people make decisions about how to talk about autistic people. Our findings provide a deeper understanding of autism-related terminology preferences.
What are potential weaknesses in the study?
Most participants in this study were English-speaking, non-Hispanic White autistic adults who primarily use speech to communicate. Future surveys with people who speak languages other than English and people who do not primarily use speech to communicate would help us learn more about the perspectives of autistic people.
How will these findings help autistic adults now or in the future?
These findings can help bring more attention to the perspectives and preferences of autistic adults, who have expressed that they prefer identity-first terms more than person-first terms. These findings can also serve as a resource for people who do not know what terms to use when talking about autistic people.
Background
Marginalized groups can exercise agency by expressing their preferences for the terminology used about them within a societal context that has historically denied their empowerment. 1 For example, disabled people have reclaimed labels that, in the past or when used by out-group members, can be considered demeaning. 2 However, even when groups have communicated their preferences regarding labels, these assertions of agency are often disregarded.3,4 The labels and terminology associated with autism are currently the subject of substantial debate.4–7
In the study reported here, we investigated how a large sample of North American autistic a and non-autistic adults evaluate autism-related terminology and their reasoning behind these evaluations. In addition to asking participants to evaluate person- and identity-first constructions, we also solicited their definitions of the word “spectrum” and of functioning labels.
Person- and identity-first language
When autism was first introduced as a diagnostic category, individuals identified as belonging to that category were called “autistic” or “autistic people.” 8 In response to stigmatizing attitudes surrounding disability, disability rights advocates in the 1970s and 1980s began calling for person-first language—terminology that literally placed the person first (e.g., “person with autism”).9,10 Proponents of person-first language argue that it emphasizes the humanity of the person with a disability.7,11 They argue that labels placing the descriptor before the person (e.g., “autistic person”) contribute to essentialist thinking, whereby individuals with a particular label are assumed to share an underlying essence that fundamentally separates them from other people.7,11,12
A number of disabled advocates have criticized person-first terminology in favor of “identity-first” terminology (e.g., “autistic person”). For example, Sinclair 13 argued that while person-first terminology implies that a person can be separated from their disability, some people see their disability as an integral and valuable part of their identity. Indeed, proponents of identity-first terminology argue that it serves to value and affirm the identity of autistic people. 14
In studies conducted in Australia, 15 the United Kingdom, 16 and the United States, 17 a majority of autistic adults surveyed preferred identity-first compared with person-first constructions (but see Flowers et al. 18 ). The Kenny et al. 16 and Bury et al. 15 surveys are frequently cited by researchers to justify their choice to use identity-first rather than person-first terminology in papers about autistic people. However, the findings from these surveys are more equivocal than they are sometimes made out to be. For example, Kenny and colleagues 16 explicitly noted that their findings “clearly demonstrate that there is no universally accepted way to describe autism,” 16 (p. 453) a caveat that was also noted in a recent study of terminology preferences across 30 countries. 19 Further, Bury and colleagues 15 found that while 37.9% of their Australian autistic sample rated “autistic” as their most preferred term, 28.3% rated it as their least preferred term. Indeed, Bury and colleagues 15 use both person- and identity-first terminology in their writing.
Beyond person- and identity-first language
Labels such as “low functioning” and “high functioning” are sometimes used to group autistic people based on perceived cognitive or speech abilities.20,21 However, rather than serving as informative clarifications, such labels may simultaneously underestimate individuals labeled as “low functioning” while denying the support needs of individuals labeled as “high functioning.”22,23
To our knowledge, only three studies have investigated autistic adults’ perspectives on functioning labels. Lei et al. 24 asked an international e-learning sample about the terms they use when talking about autism, and Keating et al. 19 and Kenny et al. 16 probed participants’ reasons for their preferred and nonpreferred terminology. Participants in the three studies described functioning labels as a way to divide autism into subcategories and as harmful, misleading, and overly simplistic. However, in these three studies, participants responded to a single open-ended question in which they could elaborate on any of their terminology preferences. As such, only some participants chose to explain their opinions on functioning labels, making it possible that only those with the strongest (positive or negative) views about functioning labels were represented. Explicitly prompting all participants to define these terms may provide further insights into the perceptions and stereotypes associated with autistic individuals.
Current study
The current study contributes to the autism-related terminology literature in three ways. First, some of the most influential surveys on terminology have reported only descriptive statistics.16,25 In the current work, we additionally analyze whether autistic people prefer some identity-first and person-first terms significantly more than other terms and whether their preferences significantly differ from those of non-autistic people. Second, unlike some past studies that have reported inferential statistics about individual terms,15,19 we compared preferences for the category of identity-first terms (i.e., “autistic” and “autistic person”) versus the category of person-first terms (e.g., “person with autism” and “person diagnosed with autism”). This seems important given that claims are made about the category of “identity-first” terms26,27 even as the studies commonly cited tend to have focused on individual terms within those categories. Third, most published studies on terminology have not specifically prompted participants to define functioning labels, which are an important element of the language debate surrounding autism.3,6 The current study contributes analyses of participants’ definitions of “spectrum,” “low functioning,” and “high functioning,” thereby broadening discussions about autism-related terminology beyond identity- and person-first debates.
In summary, the work here had three goals: (1) to compare the North American autism community’s attitudes toward identity-first and person-first terms using inferential statistics, (2) to offer general categories that characterize participants’ rationale for their terminology preferences, and (3) to analyze autism-related terminology beyond person-first and identity-first labels.
Method
All study procedures were approved by the authors’ university institutional review board (#3603) and preregistered (https://osf.io/s2ayz). We posted the survey on social media and distributed it through autism-related email lists. We also asked local, state/province, and national self-advocacy groups and community organizations that serve autistic people and their families within the United States and Canada to share the survey directly with their members. Participants were aware that the study was focused on autism-related terminology preferences from the text that accompanied the survey link. The full text of the advertisement for the study is provided in the Supplementary Materials. On the first page of the survey, we confirmed participants’ eligibility and obtained their informed consent before they moved onto the rest of the survey. The survey was open for 3 months (August 3 to November 3, 2020).
Autistic community involvement
We sought autistic community feedback throughout the study. Our research team includes autistic and non-autistic members. Additionally, we shared a draft of the survey with three autistic adults outside of our research team and incorporated their feedback into the final survey. Finally, three autistic community members joined our research team as consultants for the qualitative analyses, although one community member stepped away due to time constraints.
Participants
The final sample included 784 adults living in North America: 611 (78%) were autistic (Mage = 30.8 years, standard deviation [SD] = 10.4) and 173 (32%) were not autistic (Mage = 39 years, SD = 13.4). Of the 611 autistic participants, 376 (62%) reported having a formal diagnosis, and 235 (38%) reported a self-diagnosis. Table 1 provides additional demographic information, and Supplementary Table S1 provides information on participant gender. Participants lived in the United States (n = 701; 89%), Canada (n = 81; 10%), Mexico (n = 1), or Trinidad and Tobago (n = 1). Because this study was focused on North American adults with a connection to autism, an additional 262 respondents were excluded because they lived outside of North America (N = 251) or because they did not have a connection to autism (N = 11).
Participant Demographics
Although the “connection to autism” categories are reported as mutually exclusive, participants were able to report as many connections to autism as applied to them. For exclusive groupings, we considered participants’ closest connection to autistic people, such that self was considered closest (indicating the participant was autistic), followed by family members, then friends, then professionals or co-workers, and then “another connection.” Additionally, given the small numbers of non-autistic participants, we combined each of these groups into a “non-autistic” group in our analyses below.
AAC, augmentative and alternative communication; GED, General Educational Development Test.
Survey questions
The survey consisted of four sections: (1) the terminology participants use to describe themselves or autistic people that they know; (2) how participants rank the terms in order of preference; (3) how the participants rate the terms (how much they liked them and how offensive they found them to be); and (4) how participants define specific terms.
The 10 terms included in the survey were “autistic person,” “autistic,” “aspie,” “person with autism,” “person with autism spectrum disorder,” “person with autism spectrum condition,” “person with Asperger’s,” “person on the autism spectrum,” “person diagnosed with autism,” and “no label.” After data collection, we removed “aspie” and “person with Asperger’s” from our analyses because they refer only to a subset of autistic people. We also removed “no label” because it is neither an identity- nor a person-first term. Thus, the identity-first terms we analyzed are “autistic” and “autistic person,” and the person-first terms we analyzed are “person with autism,” “person with autism spectrum disorder,” “person with autism spectrum condition,” “person on the autism spectrum,” and “person diagnosed with autism.”
We also asked participants about some additional terms that are used to characterize autistic people (i.e., functioning labels, severity levels, and support needs classifications) and non-English terms (for participants who spoke languages other than English). For space, we do not report on the use, ranking, and rating data of these other terms (those additional data are available upon reasonable request). But as described below, we report participants’ definitions of “spectrum,” “low functioning,” and “high functioning.”
Terminology use
We first asked participants to select which term(s) they would use to describe each level of connection they had to an autistic person. For example, someone who reported that their connection to autism was themself and a family member would be presented with the list of terms and asked, “Which of the following terms would you use to describe yourself?” and then “Which of the following terms would you use to describe your family member(s)?” Participants could select as many terms as needed for each connection to autism. If participants reported working with autistic people, they were asked to report the terms that they were “required or expected” to use to refer to the people they work with and, separately, which terms they “prefer” to use. For more information about participants’ workplace terminology preferences, see the Supplementary Materials.
Terminology rankings
Next, we asked participants to rank the seven terms listed above (as well as “aspie,” “person with Asperger’s,” and “no label”) from 1 to 10, with “1” indicating their most preferred term and “10” indicating their least preferred. Ranking ties were permitted, as long as participants selected at least one #1 ranking and one #10 ranking. Note that participants ranked all 10 terms, but we analyzed only the 7 that represent identity-first terms or person-first terms. Rankings were not adjusted, but interpretation of the relative rankings (as described below) remains the same. We also provided text boxes for participants to explain why these terms were their most and least preferred.
Liking and offensiveness
For each of the terms, participants were asked to indicate how much they liked each term (1 = “dislike a great deal”; 7 = “like a great deal”) and how offensive they found each term (1 = “not offensive at all”; 5 = “extremely offensive”).
Terminology definitions
Participants were asked three final open-ended questions: (1) “How would you define the concept of a ‘spectrum’ in the context of ‘the autism spectrum?’” (2) “What does it mean to be ‘low functioning?’” and (3) “What does it mean to be ‘high functioning?’”
Analytic plan
Quantitative analyses
Quantitative analyses were conducted in R 28 using the R Studio environment. 29 The terminology use and rating data were analyzed using mixed effects modeling with the “lme4” package in R. 30 We used the “emmeans” package in R to follow-up on any significant main effects and interactions. 31
Because of the nature of ranking data, term ranks were not independent within participants (i.e., how participants ranked some terms influenced the rankings they could give other terms). Accordingly, we analyzed term rankings using nonparametric tests appropriate for rank data: the Friedman test with Wilcoxon signed-rank tests for follow-up comparisons, using the “stats” 28 and “rstatix” 32 packages in R.
Qualitative analyses
We analyzed our five open-ended questions using content analysis.33,34 Content analysis encompasses a broad range of approaches; here, we primarily used an inductive approach. Our results are informed by a critical realist position that focused on the manifest meanings of participants’ responses, with the understanding that these responses are informed by participants’ social and cultural contexts.35,36 The focus of our qualitative approach was to create categories directly from participants’ data, which we then applied across the entire sample to analyze the most common terminology justifications and definitions.
Our approach and the results we report below were influenced by our positionality as a research team. In addition to being a mixed-neurotype group, the first three authors (Z.S.R., A.J.L., and K.M.S.) were all graduate students in a developmental psychology program (advised by the fourth author, V.K.J.) during the study design, analysis, and initial writing stages. We came to this work with a variety of connections to the autistic community: Some of us have close autistic relatives, and we had all worked with autistic people in research, educational, clinical, and/or professional settings. Influenced by prior surveys of the autistic community,15,16,25 we entered this study expecting most autistic adults would prefer identity-first over person-first language, and this is the language we typically used when referring to autistic people within and outside of the study. Many participants’ responses aligned with our own language preferences, although, as shown in the results, a substantial number diverged. Through discussion among the research team and with our community partners, we aimed to ensure that these views are represented in our analytic process and the resulting article.
The first three authors (Z.S.R., A.J.L., and K.M.S.), along with the three autistic community partners, independently familiarized themselves with the open-ended question responses and generated a list of codes for each question. Z.S.R. compiled the codes into an initial list of categories. Next, the entire research team (including the autistic community members) met to discuss the codes, proposed categories, and came to a consensus on a final list of codes and categories for each question.
To investigate which codes and categories were most prevalent, we trained a team of research assistants to apply as many codes as were relevant to each response. Because each response could have between one and six codes (codes were not mutually exclusive), we calculated reliability for each question using Mezzich’s κ.37,38 Values ranged from 0.50 (for the “spectrum” question) to 0.61 (for the “low-functioning” question). Whenever coders disagreed on the presence or absence of one or more codes, Z.S.R. met with the coders to discuss the discrepancies until the group reached a consensus. Once the codes were finalized, the researchers and community partners had the opportunity to provide feedback on the final, labeled data set.
Quantitative results
Use of identity- and person-first terms
Autistic b and non-autistic participants were grouped into one of three categories based on the terms they indicated they would use when referring to an autistic person (i.e., exclusively identity first, exclusively person first, or a combination of the two). As Table 2 shows, which terms were most likely to be used differed based on the participant’s neurotype, χ2(2, 775) = 70.66, p < 0.001. We conducted post hoc z-tests of two proportions, adjusting for multiple comparisons using the Bonferroni method. Autistic participants were significantly more likely than non-autistic participants to use exclusively identity-first terms (59% vs. 37%), χ2(1, 442) = 24.88, p < 0.001. They were also significantly less likely than non-autistic participants to use person-first terms (3% vs. 22%), χ2(1, 57) = 60.38, p < 0.001. The proportions of autistic and non-autistic participants who endorsed using both identity- and person-first terms did not differ (37% vs. 41%), χ2(1, 296) = 0.72, p = 1.00.
Terminology Use by Participant Neurotype and Type of Term
Ranking identity- and person-first terms
Table 3 shows the mean and median rank for each of the seven terms we analyzed, as a function of participant neurotype. As the table shows, both autistic and non-autistic participants’ mean and median ranks were higher (i.e., a lower number) for the two identity-first terms than the five person-first terms.
Mean and Median Rankings of Each Term by Participant Neurotype
Pairs of median rank entries with the same superscript differ significantly from each other.
ASC, autism spectrum condition; ASD, autism spectrum disorder; SD, standard deviation.
Omnibus Friedman’s tests indicated that ranks given to the seven terms differed for both autistic, Friedman’s χ2(6) = 2123.80, p < 0.001, and non-autistic participants, Friedman’s χ2(6) = 213.33, p < 0.001. We used pairwise Wilcoxon tests to compare term ranks within participant groups (see Table 3 and Supplementary Tables S2–S3 for individual pairwise comparisons). For autistic participants, the two most highly ranked terms were the identity-first terms “autistic” and “autistic person,” which received higher ranks than every person-first term. All person-first terms received a median rank of 5 or lower, indicating low preference. Each term’s rank significantly differed from every other term’s rank (ps <0.001), except for “person diagnosed with autism” and “person with autism spectrum disorder,” which each received a median ranking of 8.
The pattern of results for non-autistic participants was similar, although there were fewer significant differences between term ranks. The identity-first terms “autistic” and “autistic person” received the highest ranks and did not differ from one another. Interestingly, “autistic person” did not differ in rank from “person on the autism spectrum” or “person with autism.” “Person with autism spectrum disorder,” “person diagnosed with autism,” and “person with autism spectrum condition” all received ranks of 8 or 9 (see Supplementary Table S3).
Liking of identity- and person-first terms
To analyze how much participants liked identity-first and person-first terms, we calculated for each participant an average liking score for the two identity-first terms and an average liking score for the five person-first terms. Figure 1A shows these data as a function of participant neurotype. A 2 × 2 analysis of variance (ANOVA) revealed significant main effects of identity- versus person-first label, F(1, 4702) = 520.11, p < 0.001, neurotype, F(1, 942) = 37.97, p < 0.001, and a significant label by neurotype interaction, F(1, 4702) = 34.53, p < 0.001.
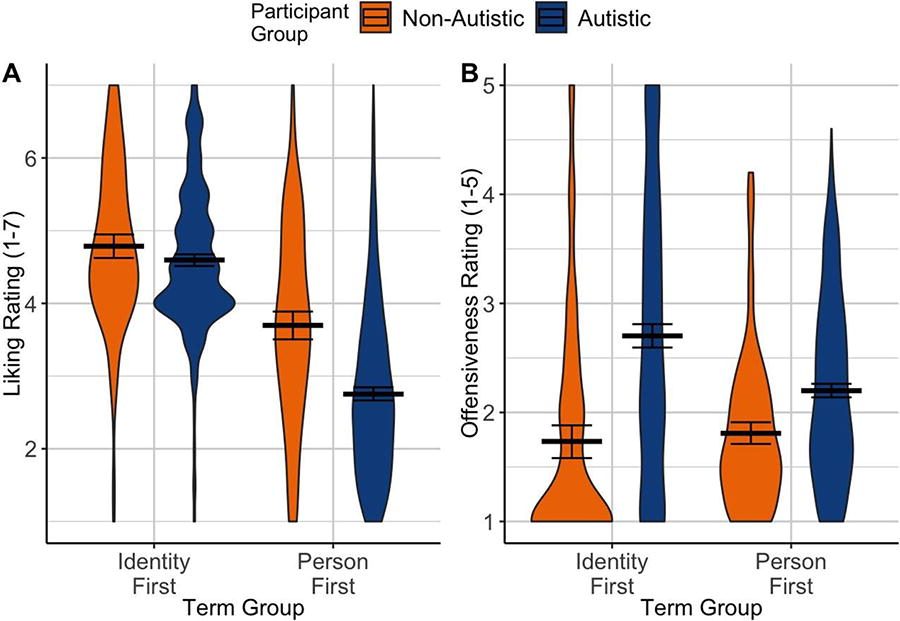
Average liking and offensiveness ratings of identity- and person-first terms by group. Horizontal black bars represent mean liking
Simple effects analyses revealed that, similar to the rankings analyses above, identity-first terms were liked more than person-first terms by both autistic, t(4702) = 30.53, p < 0.001, d = 1.03, and non-autistic participants, t(4702) = 9.59, p < 0.001, d = 0.61. Also similar to the rankings results, autistic and non-autistic participants did not differ in how much they liked identity-first terms, t(2859) = 1.49, p = 0.136, d = 0.11. However, non-autistic participants liked person-first terms more than autistic participants, t(1074) = 9.93, p < 0.001, d = 0.53.
Offensiveness of identity- and person-first terms
To analyze how offensive participants found identity- and person-first terms, we calculated for each participant an average offensiveness score for the two identity-first terms and an average offensiveness score for the five person-first terms. Figure 1B shows these data as a function of participant neurotype. A 2 × 2 ANOVA revealed significant effects of identity- versus person-first label, F(1, 4702) = 27.63, p < 0.001, neurotype, F(1, 872) = 80.01, p < 0.001, and a significant interaction, F(1, 4702) = 49.97, p < 0.001.
Simple effects analyses revealed that autistic participants gave higher offensiveness ratings than non-autistic participants to both identity-first terms, t(1933) = 10.28, p < 0.001, d = 0.85, and person-first terms, t(1933) = 5.04, p < 0.001, d = 0.35. Surprisingly given the ranking and liking results above, autistic participants indicated that identity-first terms were more offensive than person-first terms, t(4702) = 13.12, p < 0.001, d = 0.44, a finding we will return to below. Non-autistic participants gave similar offensiveness ratings to identity- and person-first terms, t(4702) = 1.03, p = 0.305, d = 0.07.
Qualitative results
In the interest of space, we provide only a brief overview of some of the common codes and categories constructed from our content analysis of participants’ responses. We focus on why participants selected their #1 ranked choice(s) and their #10 ranked choice(s), as well as their responses to questions about the definitions of “spectrum” in the context of “the autism spectrum,” “low functioning,” and “high functioning.” The full list of categories and codes is available in the Supplementary Materials (see Supplementary Tables S4–S6 and Supplementary Figs. S1–S3). The percentages reported below on endorsements of codes and categories combine autistic and non-autistic participants unless interesting differences arose between the participant groups.
Why were identity-first terms ranked highest?
To address this question, we examined the qualitative data of participants who ranked at least one identity-first term (either “autistic” or “autistic person”) in the #1 position (82% of autistic and non-autistic participants, n = 646). Percentages in this section are based on the total number of participants who ranked an identity-first term in the #1 position (i.e., using a denominator of 646). The most common category reflected explanations that focused on the connotations that a term has for how one views the nature of autism itself, what we called “meta-Comments” (72%, n = 464 of 646).
Codes that were grouped together in this “meta-Comments” category included “autism as identity,” “reminder of personhood not needed,” and “emphasizes diversity.” For example, 66% of participants (n = 423) who had an identity-first term as their highest ranked term explicitly mentioned liking the term because it affirmed autistic identities (e.g., “Autism is part of who I am. It’s part of my identity and I want to reflect that.”). Some participants (12%, n = 77) expressed that they preferred identity-first term(s) because they perceived the term(s) as rejecting the ideology behind person-first rhetoric, or because identity-first terms do not explicitly emphasize autistic people’s personhood (e.g., “People shouldn’t have to take away my identity to remember that I am a person.”). Ten percent of participants had explanations coded as “emphasizes diversity” (n = 67), which included describing the term as conveying diversity among autistic people and/or comparisons with other forms of diversity (e.g., “…Windows isn’t bad or good; it’s just an operating system. Same as Apple. With Autistics, it’s more like Linux. None are bad, it is just how you compute and relate.”).
Participants also ranked identity-first terms highest for pragmatic reasons. For example, in the “evaluations” category, 27% (n = 179) mentioned that they preferred identity-first terms because they were perceived as value neutral. In the “utility” category, 28% of participants (n = 182) who preferred identity-first terms suggested they were the simplest and easiest to use (e.g., “It is not a euphemism. It is very clear. It is an adjective that describes me.”). Finally, 50% of responses from non-autistic participants (n = 53) were placed under the category “experiential authority.” These explanations indicated that participants ranked identity-first terms highest in deference to autistic people who prefer these terms (e.g., “I have been told multiple times by my autistic friends that label-first language is much more preferred than person-first.”).
Why were person-first terms the least preferred?
To address this question, we considered the qualitative responses only from participants who ranked one or more of the five person-first terms in position #10 (60% of autistic and non-autistic participants, n = 469). Accordingly, percentages in the rest of section are based on the total number of participants who ranked a person-first term in the #10 position (i.e., using a denominator of 469).19,39c Mirroring the findings above, explanations for why person-first terms were preferred least involved explanations categorized under the “meta-Comments” category (82%, n = 385).
A common code within this category was “medicalizing”: Almost half of the participants who preferred person-first terms the least (49%, n = 229) explained they disliked person-first terms because they suggest that autism is a disease or a disorder (which these participants disagreed with) or because the term placed an undue emphasis on formal diagnoses. One participant explained that “person with autism spectrum disorder” was one of their least preferred terms because “Autism isn’t a disease. It’s not a disorder, there’s nothing wrong with the people who have it…” Other meta-comments described person-first terms as not affirming of autistic identities (42%, n = 196; “autism as identity”) and as emphasizing personhood, which participants viewed as unnecessary (18%, n = 83; “reminder of personhood is not needed”). Explanations captured by these two codes generally mirrored explanations for most preferred codes; most participants preferred terms they perceived as affirming autistic identity and not emphasizing personhood, whereas they disliked terms they perceived as deemphasizing autistic identity.
Additionally, 12% of responses (n = 57) were included in the category “utility” because they described person-first terms as lacking utility; namely, some were perceived as confusing (8%, n = 36) or unrecognizable (5%, n = 22; e.g., “It sounds very clinical. I’ve never heard ‘autism spectrum condition/ASC’ before but my reaction to it is negative”). It is worth noting that the perspectives highlighted in this section reflect the majority of participants in our sample. However, some participants displayed different or even opposite patterns in their rankings (e.g., included an identity-first term in the #10 position and a person-first term in the #1 position) and may have used different reasonings to justify their rankings. For more details, see Supplementary Figure S1 and Supplementary Table S4 in the Supplementary Materials.
“Spectrum” definitions: Why was “person on the autism spectrum” ranked in the middle?
When asked to rank specific person- and identity-first terms, participants tended to rank “person on the autism spectrum” as neither their most nor least preferred term overall. Although we did not specifically prompt participants to explain their attitudes toward the term “person on the autism spectrum,” the contradictory definitions that participants offered for “spectrum” may provide insight. The variety of definitions of “spectrum” was especially evident within our “shape of the spectrum” category (see Supplementary Fig. S2 and Supplementary Table S5).
For instance, many participants (24%, n = 188) described the autism “spectrum” as nonlinear (e.g., “It’s a kaleidoscope of traits, not a linear scale.”). A quarter of participants (26% overall, n = 193; 30% of autistic participants, n = 177; 10% of non-autistic participants, n = 16) used an analogy to describe their understanding of the spectrum. Some likened the spectrum to an ice cream bar where there were a range of characteristics (or “toppings”) that an autistic person might experience. Of participants who used an analogy to describe the spectrum, 61% of autistic participants (n = 107) and 38% of non-autistic participants (n = 6) also refuted the idea that the spectrum is linear. These participants disagreed with common understandings of the autism spectrum where one could be “a little” autistic or “a lot” autistic, sometimes referred to in the literature as high functioning/mild or low functioning/severe/profound, respectively. At the same time, some participants (4%, n = 29) indicated that “spectrum” represented a linear scale (e.g., “The spectrum goes like a band from left to right, where far left is the least level of support needed, and the far right is for those that need the most support”).
These varied definitions of “spectrum” may result in the term not providing consistent, practical information about how autistic people experience the world. Indeed, some participants (8%, n = 61) indicated that “spectrum” is “useless” or that it does “not allow for nuance.” Thus, even if a participant provided a positive definition of “spectrum,” they may not have liked or highly ranked “person on the autism spectrum” due to their impression of how “spectrum” is typically used.
Why did autistic participants like identity-first terms more than person-first terms but rate them as more offensive?
One puzzling aspect of our quantitative findings was that autistic participants ranked identity-first terms highest and liked them the most but also rated them as most offensive, on average. Although we did not identify a category that explicitly addressed this tension, some of the qualitative responses indirectly speak to this issue. Few participants described the identity-first terms as offensive in their open-ended responses, but some responses noted that referring to an autistic person as “an autistic” (rather than “an autistic person”) could be offensive. For instance, one autistic adult commented:
I usually use autistic as an adjective rather than a noun (e.g., “an autistic person said that’” not “an autistic said that”) and so that’s the [point of view] I was coming from when rating. To clarify further, I have no issue with autistic people using it as a noun… BUT I would find it sketchy and a little offensive for an allistic (non autistic) person to use it that way (e.g., “you know how much those autistics love to stim”).
Thus, ambiguity about whether participants were meant to rate “autistic” as an adjective or a noun may explain the discrepancy between liking and preference ratings versus offensiveness ratings.
Definitions of “high” and “low functioning”
In addition to explaining their terminology preferences, participants were asked to provide definitions of “high functioning” and “low functioning.” The high- and low-functioning definitions shared a large degree of thematic overlap, so these open-ended questions were grouped together in our thematic analyses (see Supplementary Fig. S3 and Supplementary Table S6 in the Supplementary Materials). The three most common categories in autistic and non-autistic participants’ definitions of high and low functioning were “capabilities,” “needs,” and “negative evaluations.”
Many participants associated functioning labels with individual capabilities, particularly in their definition of “low functioning.” Indeed, the “capabilities” category was most common among low-functioning definitions. About 40% of autistic and non-autistic participants (n = 321) described low functioning as referring to people who do not speak, have low IQ, and/or have difficulty with other specific skills. For example, one autistic participant explained that low functioning “usually refers to somebody with ASD who has difficulty accomplishing expected standard tasks without accommodations. Any independent skill useful to life like cooking, cleaning, driving, socializing, etc…” The “capabilities” category was the third most common among high-functioning definitions, where 17% of participants (n = 134) described high functioning as referring to individuals who are able to communicate through speech and/or have average to high IQ.
The second-most common category for both functioning labels was “negative evaluations” of the terms themselves. Specifically, 33% of autistic and non-autistic participants (n = 259) described “low functioning” as offensive (e.g., “I don’t like this term, because it seems to suggest that the person is broken somehow because they can’t function ‘properly.’”) and/or meaningless (e.g., “This tells me nothing about the person…”). About 21% (n = 164) of participants provided the same critiques of the term “high functioning.” So, a substantial proportion of participants described both terms as problematic and/or useless, although participants seemed to evaluate “low functioning” more negatively than “high functioning.”
The third most common category in definitions of “low functioning” (32%, n = 254) was “needs.” Both autistic and non-autistic participants described low functioning as referring to people who need high levels of support relative to the general population (e.g., “It means to need a lot of support in their everyday life.”). Interestingly, “needs” was the most common category in the definition of “high functioning” (44%, n = 343). Some participants (24%, n = 186) described high functioning as suggesting someone needs relatively lower levels of support (e.g., “This person can function relatively well even with little support.”). But they also noted that the needs of “high functioning” individuals are often dismissed (24%, n = 186) or present but less obvious (3%, n = 23).
In the “influence on others” category, nearly a quarter of participants (23%, n = 180) explained that “low-functioning” individuals may be perceived as a burden, dependent, and/or unable to work; conversely, 14% of participants (n = 113) referred to “high-functioning” individuals as independent and productive. Importantly, a number of these descriptions, including references to “low-functioning” individuals as a burden and “high-functioning” individuals as productive, were accompanied by criticisms of these perspectives. One participant wrote, “People seem to use [low-functioning] for autistic people who are most inconvenient to neurotypicals,” and went on to explain that they view this perspective as dehumanizing. Similarly, some participants criticized functioning labels as shaped by capitalist ideologies, for example, “‘High-functioning’ is a label put on autistic people to label their ability to conform to society and participate in capitalist norms.”
About 25% (n = 192) of participants referenced the role of the (social) environment in the opportunities, agency, and autonomy provided to people who are labeled as low functioning (“others’ influence”). Interestingly, this category was much less common among responses to the high-functioning prompt (2.8%, n = 22). One autistic participant described that low functioning “means someone has medically judged that you have less capacity. The result is that you may not get opportunities or that others may not presume competence or give you the dignity of risk.” This emphasizes the harmful effects of labeling someone as low functioning because it can perpetuate underestimation of the labeled individual’s competence, limiting their opportunities to develop and exercise agency.
Discussion
In this study, both autistic and non-autistic participants ranked identity-first terms higher than person-first terms, liked identity-first terms more than person-first terms, and used identity-first terms (or a combination of identity- and person-first terms) most often. These findings extend the descriptive statistics reported in Kenny and colleagues’ 16 highly influential study and inferential analyses, which have generally focused on analyzing terms individually.15,19 Researchers (including some authors of this article) often make a claim of community preference for the category of identity-first terms (e.g., “We use identity‐first language because most autistic people prefer it…”). 26 (p. 1322) But until this study, there was not a robust analysis of whether the category of identity-first terms was indeed preferred more than the category of person-first terms. 1 7 d
An interesting and seemingly contradictory finding was that autistic participants rated identity-first language as more offensive than person-first language, even though they also preferred and used identity-first terms at higher rates. As noted, this may reflect the ambiguity of the word “autistic” when used without context. In line with a prior study, 19 some of our participants explained that the use of “autistic” as a noun, especially by non-autistic individuals, would be offensive. At the same time, other studies have reported that participants rated “autistic” (i.e., devoid of context) more highly and used it more often than “autistic person.” 16 Thus, it is important to continue to investigate the nuances of how individual terms are understood and used. For example, perhaps referring to autistic people as “autistics” is viewed as acceptable when it is done by an autistic person but would be inappropriate if done by a non-autistic researcher.
When researchers are hesitant to use identity-first terms or are unsure of an individual’s preference, one recommendation has been to use the term “person on the autism spectrum.” 40 This is, in part, due to past findings that “person on the autism spectrum” has been highly rated and preferred.15,16 However, participants in the current study had relatively neutral attitudes toward “person on the autism spectrum,” ranking it as neither most nor least preferred. As noted, this neutral attitude may reflect that some participants viewed the word “spectrum” as being vague and meaningless, whereas others seemed to appreciate it as representing nonlinear heterogeneity among autistic people. Future research should address the role of variations in interpretation on attitudes toward these terms.
We also asked participants to define “high functioning” and “low functioning.” Many participants criticized both terms as vague and offensive, echoing perspectives reported in prior work.16,19 While participants associated both terms with individual weaknesses and strengths, they also expressed that functioning labels may cause people to overlook labeled autistic individuals’ support needs (especially those of people labeled as “high functioning”) and/or to deny them opportunities and agency (especially for people labeled as “low functioning”). These categories coincide with recent advocacy efforts to move away from blanket categorizations of individual functioning (including the DSM-V levels of severity and support needs or the recently proposed “profound autism”)3,4 and to instead provide specific characterizations of individuals’ strengths and needs on a case-by-case basis.6,41,42
Limitations and Future Directions
Our findings reflect the perspectives of English-speaking adults in North America who were interested in responding to a survey about autism-related terminology preferences. The two primary limitations of this study were (1) generalizability based on our particular respondent demographics and (2) limitations of the approach we took to analyzing the open-ended data. Future research may build upon our study both to address these limitations and to empirically investigate how different autism labels influence perceptions of labeled individuals.
Our reliance on volunteer respondents to a survey explicitly advertised as about autism terminology likely drew participants with strong opinions about the topic. Future work leveraging large database samples and embedding terminology preference questions into studies on other topics may yield a wider range of opinions. For example, Buijsman and colleagues 43 found a preference for person-first terminology in a sample from the Netherlands Autism Register, a database of children and adults with autism in the Netherlands. In that study, the preference data were not collected as part of a study that was explicitly advertised as about terminology preference.
These results may not generalize to members of the autism community who speak languages other than English or who live outside of North America. Syntactic differences between English and other languages have been hypothesized to influence preferences.43–45 However, French autistic adults prefer identity-first language even though their syntactic structure places adjectives after the noun (e.g., identity first: “personne autiste,” person first: “personne avec autisme”), 46 and Dutch-speaking adults with autism prefer person-first over identity-first language, even though Dutch shares general syntactic rules with English (adjective before noun).43,44 Together, these findings suggest that cultural influences rather than language differences may influence preferences for identity- versus person-first language. More work is needed to include the perspectives of autistic people from all over the world, particularly autistic people from countries that are not primarily English-speaking.
Prior surveys of the autism community’s terminology preferences15,16 have been criticized, in part, because they may have excluded autistic people who are nonspeaking or who need support or accommodations to participate in research.4,7 We did not measure support needs in our study, but 32 autistic participants (5.24% of the autistic sample) reported that they primarily communicate using augmentative and alternative communication (AAC) methods. Future work should specifically investigate the terminology preferences of autistic people who use AAC methods.
Another limitation of this study related to our choice of analytic approach for the open-ended data. In this study, we adopted an approach that allowed us to manually apply high-level categories across hundreds of responses and to investigate which categories were most prevalent in our data. While this content analysis approach afforded great flexibility and provided additional context to understand the quantitative ratings, we acknowledge that the emphasis on breadth came at the sacrifice of depth. Future thematic analyses may be able to provide an even deeper and more nuanced picture of the autistic community’s language preferences and the meaning ascribed to common labels.
Our method of recording participant gender (free text response) was aimed at being inclusive but makes it difficult to reliably analyze group differences in terminology preferences related to gender. Past research has found that gender can be associated with autism-related terminology preferences. Specifically, identifying as nonbinary is associated with rating some person-first terms as more offensive.15,47 A large, though not unprecedented, 19 percentage of our sample described their gender in a way that we categorized as nonbinary (see Supplementary Table S1). This may influence the generalizability of our findings, as the language preferences of our sample may differ from those of more gender-conforming populations.
The study here involved a survey of explicit terminology preferences. Future work should experimentally investigate the impact of identity-first and person-first language. Although some experimental studies suggest that identity-first labels can increase stigma for some conditions (e.g., delusional disorder and alcohol use disorder), 48 other studies find no difference when autistic people 49 or disabled people in general 50 are introduced with identity versus person-first labels. Given these inconsistent findings and some interpretational issues (e.g., Gomes 50 reports “a very small p value” to mean no effect), further research is needed to determine the conditions under which identity- and person-first labels may differentially lead to stigmatization.
Recommendations and Conclusions
Consistent with prior work in this area, we documented an overall preference for identity-first terms, although there was considerable variability. Bottema-Beutel and colleagues 40 note that “Complete consensus is unlikely to be gained for a set of terms for any marginalized community.” 40 (p. 6) They note that using the lack of consensus to justify nonadoption of identity-first language minimizes the perspectives of a significant number of autistic people.
Given the variability of autistic people’s terminology preferences and potential regional and cultural variations in the evaluation of some terms, we suggest researchers include questions about participants’ preferred language in their demographic questionnaires. As marginalized groups often have little say in how they are portrayed in academic outlets, involving autistic participants in decisions regarding how they will be referred to is one way researchers can support participants’ agency. Ideally, autistic participants will complete these language preference items themselves, and researchers can support this by adapting response modalities to increase accessibility (see Academic Autism Spectrum Partnership in Research and Education guidelines 51 for designing accessible surveys). Researchers can then use the terminology preference of a given study sample to inform the language they use to describe that sample. When it is not possible to ask participants directly, the current work and many other studies15,16,19 suggest that most autistic participants prefer identity-first language.
Footnotes
Acknowledgments
The authors would like to thank Abha Basargekar for insightful comments on an earlier version of this article; the Jaswal Lab research assistants (Danning St. Martin, Emma Ziselman, Abby Napoli, Mary Isaac Cargill, and Kaylin Belcher) who contributed to data collection and qualitative data analysis; our autistic community partners (Jess Davis-Walters, EC, and GB) for their contribution to the qualitative data analysis; and all of the participants who volunteered their time to participate in this survey.
Authorship Confirmation Statement
Z.S.R., K.M.S., A.J.L., and V.K.J. conceived of the study and contributed to its design and implementation. Z.S.R., K.M.S., and A.J.L. conducted the analyses and wrote the original draft of the article. All authors were involved in review and editing, and all authors approved the final version of the article.
Author Disclosure Statement
All authors report that no competing financial interests exist.
Funding Information
The authors did not receive any funding in support of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.