
Abstract
Background:
Autistic people commonly report social anxiety. There may be distinctive aspects of the autistic experience of social anxiety, as well as aspects of therapy for social anxiety that need to be adapted for autistic people. This study investigated these issues through the firsthand perspectives of autistic people.
Methods:
Fifteen autistic adults took part in semistructured interviews about their experiences of social anxiety and cognitive behavioral therapy (CBT) for social anxiety, the first-line intervention for social anxiety. Interviews were analyzed using reflexive thematic analysis.
Results:
Autistic people perceived differences in their experience of social anxiety compared with non-autistic people. These included the impact of (1) autistic traits, (2) traumatic experiences of living in a neurotypical world, and (3) nonsocial factors that contribute to anxiety in social situations for autistic people. Participants also questioned the cognitive and behavioral components of conventional CBT for social anxiety (as they had experienced it); argued for a trauma-informed approach to social anxiety; and explained how the social process of therapy needed adaptation for autism.
Conclusion:
These perspectives will help therapists and researchers refine their formulation of social anxiety in autistic people and inform the development of autism-adapted social anxiety interventions.
Community Brief
Why is this an important issue?
Social anxiety is very common in autistic people. We need to know more about the factors affecting social anxiety in autistic people. This will help us treat it effectively if someone seeks therapy. In addition, we know that autistic people are often failed by mental health services. However, we know very little about how autistic people experience particular therapies. This includes cognitive behavioral therapy, which is the first-line therapy for social anxiety.
What was the purpose of this study?
The first aim was to understand the perspectives of autistic people on what is unique about the autistic experience of social anxiety. The second aim was to understand autistic people’s experiences of cognitive behavioral therapy for social anxiety.
What did the researchers do?
We interviewed fifteen autistic adults to see whether a theory of social anxiety relevant to the general population matched their own experience of social anxiety. We also interviewed them about their experiences of cognitive behavioral therapy for social anxiety. We analyzed common themes across the interviews.
What were the results of the study?
Interviewees highlighted that autism traits, trauma, and nonsocial factors needed to be considered in social anxiety of autistic people. Interviewees felt that cognitive behavior therapy did not meet their needs for social anxiety. They said it wrongly assumed their social fears were irrational; encouraged inappropriate modification of behaviors; and did not consider trauma sufficiently. They also thought therapists did not always adapt therapy sessions to their social/communication needs.
What do these findings add to what was already known?
The findings support other research showing that different factors are important in social anxiety for autistic people compared to non-autistic people, including autism-related and environmental factors. The findings extend previous research by providing novel reflections based on the lived experience of autistic people about an important theory of social anxiety that underpins how we understand and treat social anxiety in the general population. The findings agree with other studies that therapy needs adaptation for autistic people. However, this study goes further by highlighting autistic people’s perspectives on flaws in the fundamental principles of cognitive behavioral therapy for social anxiety.
What are potential weaknesses in the study?
We cannot be sure of the quality of the therapy the participants had received. The participants who were interviewed may have chosen to take part because they had a bad experience of mental health services, which might not be reflective of other experiences. Most participants were highly educated, White autistic adults, who were diagnosed in adulthood, and we cannot know whether their experiences are similar to other autistic adults.
How will these findings help autistic adults now or in the future?
The findings include recommendations to therapists in working with autistic adults with social anxiety. The findings will also help researchers further develop modified therapies for mental health difficulties in autistic people.
Introduction
Autistic people commonly experience social anxiety. As many as half of autistic adults may meet the criteria for social anxiety disorder. 1 Social anxiety disorder is diagnosed when an individual experiences clinically significant distress about social situations due to fears of being negatively evaluated by others. 2 Theoretical models propose that autistic people have a broad-based sensitivity to anxiety in general arising from autism-related traits, including differences in processing uncertainty, emotions, and sensory experience.3–4 Autistic people may have additional risks for development specifically of social anxiety, including difficulties with social interaction and communication, in part, arising from adverse social experiences. 1
Among non-autistic people, the first-line treatment for individuals seeking support for social anxiety is cognitive behavioral therapy (CBT). Clinical guidelines suggest one-to-one CBT 5 informed by the cognitive model of either Clark and Wells 6 or Rapee and Heimberg. 7 These models hypothesize that individuals develop negative expectations about others’ responses to them, which are maintained by several features, including “safety behaviors” (behaving in such a way to prevent a feared social outcome) and self-focused attention (focusing attention on one’s own thoughts and feelings during a social interaction). These features block re-evaluation of the individual’s expectations, provide biased information, and potentially interfere with the social situation. CBT for social anxiety encourages shifts in behavior and attention to test out the individual’s negative expectations surrounding social situations. This therapy has shown high effectiveness in the general population. 8 However, we do not know whether it helps autistic people, as evidence for individual CBT for social anxiety in autistic people is limited to several case studies. 12 Two studies have shown reduced social anxiety following group CBT,10–11 however, these studies lacked control groups and effect sizes were relatively small. Looking more broadly, CBT may be helpful for general anxiety and depression in autistic people, although there is uncertainty about effectiveness. 9
There is growing consensus that autistic people need an adapted approach to therapy. Autistic people highlight a need for adaptations when accessing services (relating to the sensory environment, clinical and service context, and clinician knowledge and communication) but rarely receive these adaptations. 13 Cognitive behavioral therapists acknowledge that the process and content of therapy require adaptation for autistic people, favoring a formulation-driven approach that guides therapy based on the individuals’ specific presentation of anxiety. 14 This latter point is especially important if autistic people experience the presenting issue differently from non-autistic people, which seems to be the case for anxiety. 15 In the case of social anxiety, qualitative studies suggest some commonalities (e.g., tendency to self-monitor) but also differences among autistic people (e.g., the impact of sensory factors, nonautistic communication partners, and stigma)16–17 . The present study developed this topic, directly asking autistic people about their social anxiety experiences in relation to the cognitive model of social anxiety. 6 This was an opportunity to gain an “experts-by-experience” perspective on whether current understanding of social anxiety is adequate to autistic people’s needs. In addition, no existing research has asked autistic people about their experiences of CBT for social anxiety, as the first-line therapy offered in routine clinical practice. 5 Given the lack of clinical studies of effectiveness, this is a helpful starting point to gauge the acceptability of current interventions.
The present study asked the following two questions: (1) What specific factors need to be considered in the autistic experience of social anxiety? (2) What needs considering for autistic people accessing CBT for social anxiety?
Methods
This qualitative interview-based study received approval from the Newcastle University Faculty of Medical Sciences Research Ethics Committee (2231/13981). It was part of a larger project, including a survey-based study.
Participants
Participants took part following completion of an online survey about social anxiety.18,36 The survey link was shared through charities and social media. Individuals were eligible to be interviewed if they (1) reported a clinical diagnosis of autism, (2) had accessed CBT for social anxiety as an adult, and (3) consented to be contacted. Of 59 autistic people who had accessed CBT for social anxiety, 48 consented to be contacted about an interview. Individuals were contacted at random until 15 agreed to take part. Three people did not respond to an email invite, so 18 were contacted in total. This sample size was chosen due to constraints on time and resources, while also having a high likelihood of reaching data saturation. 19
Table 1 shows demographic and clinical variables for the 15 participants. All participants met the criteria on the social anxiety module of the Diagnostic Interview for Anxiety, Mood, and OCD and Related Neuropsychiatric Disorders (DIAMOND). 20
Demographic and Clinical Variables of Sample
Procedure
After signing a digital consent form, participants took part in an interview adapted to their communication preferences. Live interviews included three by phone, nine by video, and one face-to-face, each taking about 90 minutes. There were two asynchronous email interviews, involving five email exchanges over a fortnight. Interview transcripts had a median length of 10,067 words (interquartile range = 7294–12,440 words). One asynchronous interview was average in length; one was half the average. Participants were compensated £20 for their time.
Live and asynchronous interviews followed the same five-part sequence based on a semistructured interview schedule (see Supplementary Data S1). In asynchronous interviews, questions for each of the five parts were sent in a separate email (alongside any follow-up questions/comments). All interviews started with a brief structured assessment of social anxiety (DIAMOND 20 ). Then we explored a recent event where the individual felt socially anxious, including the nature of the event, thoughts, feelings, sensations, and behaviors. This set a context for discussing the Clark and Wells model in the third part of the interview. The researcher described the model in lay language with a visual aid, before exploring whether the model fitted the participant’s experience. The fourth part of the interview focused on the participant’s experience of CBT for social anxiety. Finally, there was time to conclude and reflect on the interview experience.
Data analysis
Reflexive thematic analysis was used to interpret the interviews. 21 This brings together (1) the data, (2) theoretical assumptions, and (3) perspectives of the researcher. The theoretical approach was interpretivist and constructivist, aligning with the focus on specific viewpoints grounded within individuals’ subjectivity. The aim was to privilege participants’ lived experience and sense-making, taking participants on their own terms without superimposing existing frameworks on their responses, while acknowledging the researcher’s role in structuring the analysis. The researcher approached the study as a clinician-researcher with experience working with neurodivergent people and CBT. The researcher was able to “think as a therapist” to hypothesize how therapy-related factors may have contributed to a person’s experiences, and used these ideas to inform follow-up questions and move the interview toward feedback that may be actionable for therapists. The approach was intended to be affirming of neurodivergence and the value of experts-by-experience.
Thematic analysis began with close-reading of transcribed interviews, followed by preliminary coding to label units of information relevant to the research questions. Then codes were collapsed or linked to group together units of information in emerging themes. Themes and codes were iteratively refined as the analysis developed. Themes were then structured to meaningfully answer the research questions. Lastly, a summary of themes with illustrative quotations was shared with participants over email for “member checking.” Participants were asked whether the analysis appeared accurate to their experience, respectful, and potentially useful for therapists. Seven participants emailed back, indicating they resonated with the analysis and the experiences described by other participants.
Community involvement
The interview schedule was discussed with two autistic lay people, who gave feedback on a draft, and later reviewed codes emerging in the analysis. The provisional themes developed from the interviews were later shared with participants for comment (as described above). The final analysis was presented in an online dissemination event to which autistic people were invited. Feedback received during the event and afterward was very supportive.
Results
Question 1. What specific factors need to be considered in the autistic experience of social anxiety?
Autistic people saw some commonalities in their experiences of social anxiety compared with non-autistic people. When we discussed the Clark and Well’s cycle of social anxiety, many people could relate to it. The following captures one participant’s reaction on seeing the cycle:
Sorry I’m about to get tearful. Please don’t take too much notice. It’s … I hate all this—it’s so exhausting, having this, you know? I can relate completely. Leaving the house, I have it ninety-nine per cent of the time. (P1)
Despite relating to the cycle, all participants also felt their social experiences, and therefore, the nature of social anxiety, differed compared with non-autistic people. These differences have been categorized into three themes; see Figure 1 for a summary.
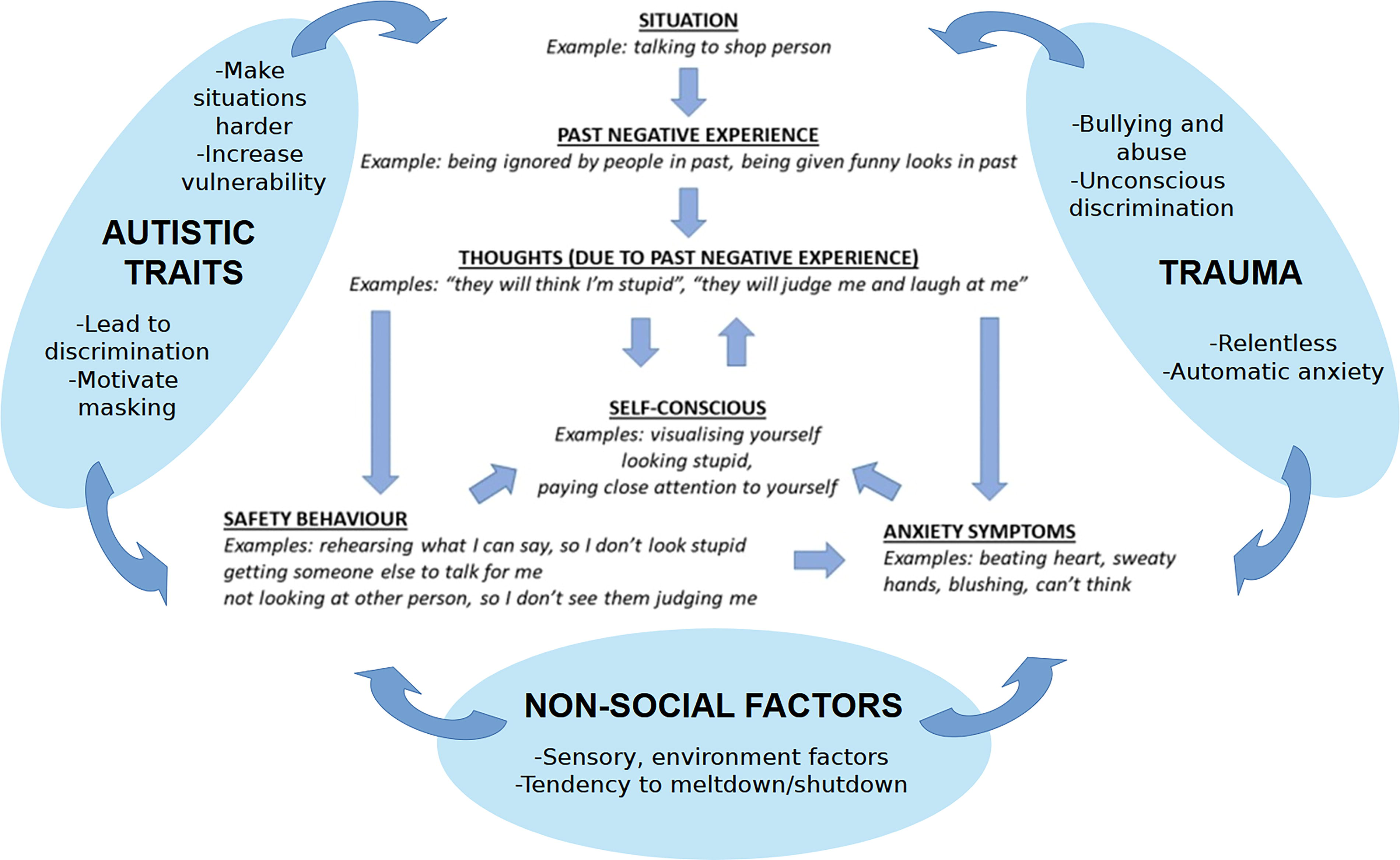
Thematic analysis showing perceived differences in factors affecting social anxiety in autistic people. The center of the figure shows the Clark and Wells (1995) model; this represents the traditional understanding of how social anxiety is experienced by the general population. The three bubbles around the model show the three key themes emerging in this study regarding additional factors important in autistic people’s experiences of social anxiety. Subcomponents of each theme are shown in smaller font in the bubbles. The three themes represented by each bubble are seen as impacting on all aspects of the Clark and Wells (1995) model.
Theme one: Autistic traits
This theme included four subcomponents that relate to autistic traits as a source of anxiety in social situations. First, autistic people stressed that autistic traits make social interactions more challenging, and therefore distressing, even where others do not react negatively. One person said: “I have to put 100% more effort in and sometimes I just can’t do it because of my communication issues and that is stressful” (P2). Another person called this the “inaccessibility” of neurotypical interactions:
I would add inaccessibility to the model, as my social anxiety in part is the result of the differences between communication, experiences and needs of neurotypical and autistic people. A lot of neurotypical people value communication that is face to face, spoken, fast paced which is not accessible for me, and I have had difficulty with communicating with neurotypicals as a result as they were not willing to adapt how the conversation occurred to make it accessible for everyone. (P3)
The next element of this theme relating to autistic traits is increased vulnerability an autistic person might experience in social situations due to their processing differences. Awareness of this vulnerability may trigger anxiety. One person described the following:
I think what complicates things for autistic people—something about assessing an environment correctly. […] Quite a few people have said it to me—I’ll notice details and things that are interesting and not notice something that someone who is non-neurodiverse will notice that is necessary for them to behave appropriately. […] You know, you might not always pick up on danger so well, so it can be a safety issue. (P1)
Third, autistic people shared fears of being judged for their autistic traits and treated badly as a consequence. As one person said (of their fears), “With family, it’s of letting them down, with strangers, it’s being discriminated against because I’m autistic” (P4). This quotation illustrates the variety of fears of negative evaluation people described: some fears were typical of the general population (e.g., letting others down), whereas others related to being judged for being autistic. As another person noted, these autism-related fears arise from the noticeable differences autistic people might show in social situations and the negative reactions they receive:
It’s not so much what they think [that makes me anxious]—but will they find out I’m different? Because we are different. There’s something about the way we are or the way we are not. I see the looks, the way people talk to each other, the way they don’t talk to me. It’s happened my entire life. (P5)
An awareness of one’s autistic differences leads many to “mask” those traits. This is the theme’s fourth subcomponent. As one person indicated, “masking” is a double-edged sword, as it is motivated by social anxiety but also necessary to succeed in some contexts:
Maybe if you’re talking about autistic people, masking is really a common autistic problem. […] You’re trying to compensate for like I should look people in the eye, I shouldn’t stim […] It’s to protect yourself from people looking at you like you’re a weirdo or judging you. It’s really anxiety based […] If I didn’t mask at all, I would probably have no job. So yeah you kind of need to do it. (P6)
Theme two: Trauma
Participants described their social anxiety as “trauma-based” (P2, P6, and P7). This theme consists of four subcomponents. Individuals often had experiences of bullying/abuse where others tried to exploit their differences and vulnerabilities. One person shared the following:
Things I said would be taken out of context and twisted and used against me. I’ve had people try to convince my friends to abandon me. People saying I don’t belong. Before, I was a child. So when people treated me like that, it wasn’t considered abuse, just bullying and to be expected. What people have done to me hasn’t changed. But now there’s laws I can use. And I am not afraid to call it abuse. (P8)
The second subcomponent of the theme relates to the multiple, repeated, and relentless nature of the negative experiences described. In one person’s words:
And for autistic people because of the relentless barrage of criticism, it may be very difficult to explain the possibility of not living with that, because that’s been all your life. So it’s just normal life […] I think trauma needs to be inserted into this model, at least emotional trauma, and the relentlessness of it. (P1)
The third subcomponent acknowledges that trauma does not always consist of deliberately hurtful behavior. Sometimes it is unconscious acts of discriminatory behavior. One person shared the following:
Maybe you could add something about not being taken seriously? Because people tend to do that when they know you’re autistic […] because they think you have a mental disorder. So you should disregard that person. But that can make you feel really invalidated and anxious. […] They don’t always mean it but it’s always a thing, like should I tell people I’m autistic? Cos then people don’t always think you can make decisions for yourself. (P6)
The fourth subcomponent relates to the manner in which trauma operates in the moment as a conditioned response. Participants explained that they had been through so many difficult social experiences that anxiety was there automatically in social situations as a highly sensitized threat response. From the firsthand perspective, this did not seem to be a process mediated by thoughts. One person had the following reaction when shown the anxiety cycle; they felt conditioning was a helpful way of conceptualizing their anxiety:
My feeling, straight out, but it’s not logical. I don’t think about past negative experience or the thoughts in my head. It’s just so quick […] I’ve had sixty years of this. It goes straight into the reaction. […] It’s just Pavlov’s dog, isn’t it? (P1)
Theme three: Nonsocial factors
Autistic people stressed that nonsocial factors impacted on social anxiety. This theme had two subcomponents. One person described the first subcomponent, the impact of environmental factors on anxiety in social situations:
I suppose the other way anxiety can enter this cycle is via non-social patterns in the environment. For example, unwelcome sensory input like loud noises, crowded environment—these sorts of things can cause general anxiety to build. […] This reduces one’s threshold for dealing with social anxiety. […] And there’s fear about how you might respond to those sensory problems and fear of how that might be perceived—I think it’s a parallel system. For instance, I have an involuntary response to loud noises where I put my hands over my ears. That is acceptable in children, less so in adults. People perceive you less seriously. (P9)
Other individuals highlighted other nonsocial factors, such as change or uncertainty in the environment, that could reduce a person’s capacity for dealing with distress in social situations. The second subcomponent of this theme on nonsocial factors related to an autistic person’s heightened arousal that made them likely to have “meltdowns” and “shutdowns” under too much stimulation. These experiences were not uniquely caused by social factors but could feed into anxiety in social situations and could have social consequences. For instance, one participant shared the following regarding meltdowns:
I mean they’re awful whatever happens. But in public they’re so much worse. If you’re at home, you at least feel safe. […] You aren’t going to have to deal with the consequences down the line of people going: Oh, remember, when you did that. […] For me—I go mute, I can’t speak, lights and colours and everything is so bright, and it’s frightening to feel so exposed and vulnerable in a situation like that. (P10)
Question 2. What needs considering for autistic people accessing CBT for social anxiety?
Participants often felt that the cognitive and behavioral aspects of CBT for social anxiety were not appropriate to their needs and experiences. These insights are each represented as a theme, alongside two additional themes relating to the need for (1) a trauma-informed approach and (2) autism-informed adaptations to the delivery of therapy. The four themes are shown in Figure 2 and described below.
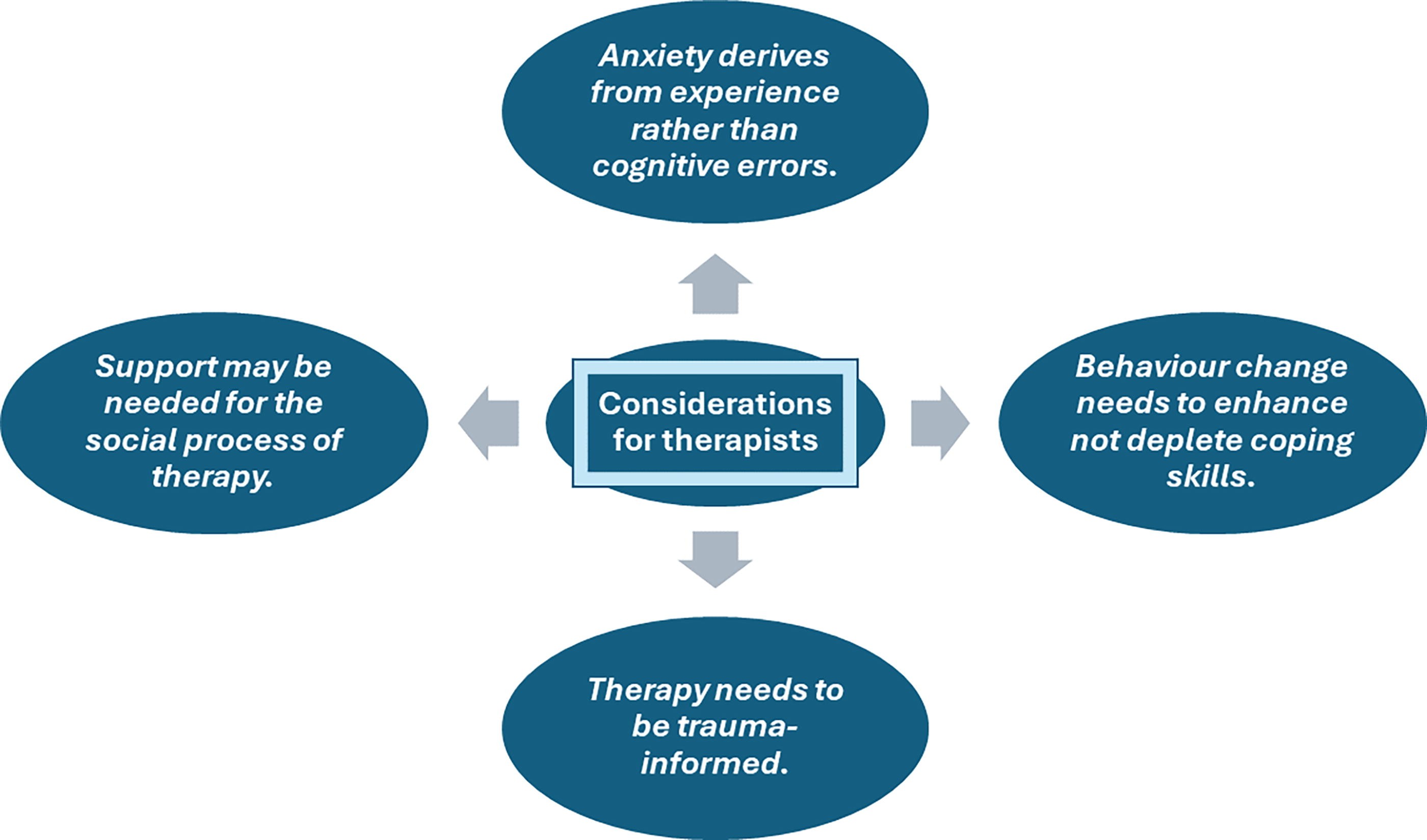
Thematic analysis of autistic people’s perspectives on cognitive behavioral therapy for social anxiety they had received in clinical services.
Theme one: Anxiety derives from experience rather than cognitive errors
In terms of the cognitive aspect, participants felt their fears about social situations were too often framed as ungrounded “distortions” in CBT. Autistic people believed that their fears were not irrational but based on considerable evidence: they knew they were perceived as socially different to others (their diagnosis alone was evidence). In addition, many had a history of difficult social experiences and continue to experience negative reactions from others; one person described this as “pattern recognition rather than irrational fears” (P8). Another person offered the following:
At least in the CBT I have experienced, there has been the fairly dogmatic assertion that your thoughts are a distortion of reality. This might sometimes be the case. But I don’t think all autistic experience needs to be seen through this lens […] I and other autistic people have some pretty noticeable social differences that demonstrably do affect the way people see and respond to you. That’s like stating a fact about autistic people. So if you have a thought about being misunderstood, I don’t think the thought itself is the problem that needs to be addressed—I think that is missing the point and is not super helpful. Because that thought is quite realistic and grounded in reality. Whereas how you deal with the anxiety that comes with that, is maybe more helpful. (P9)
Autistic people suggested that instead of assuming their social fears are exaggerated or distorted in some way and then aiming to reframe those fears, a better approach involved understanding the full picture of their anxiety: how it had developed and how it played out in situations. This helped build self-efficacy and self-compassion. One person expressed this as follows:
For me trying to see the big picture, simply understanding all the things that happen when I’m anxious, it’s been very empowering for me. It helped me feel more in control, not through any additional control but just being aware of the process […] it helped me see how much goes into every social situation, I didn’t give myself credit for that before. (P11)
Theme two: Behavior change needs to enhance not deplete coping skills
In terms of the behavioral aspect of CBT, participants described how therapists had encouraged them to change their behavior in social situations, but in ways that were disempowering and removed their ability to cope:
I’ve actively avoided CBT because the last one was so damaging […] when you have autism you put things in place to sort of manage it. Things that I suppose in a neurotypical person might be seen as unhealthy. So one of the things I used to do was take this sort of comfort item places, because just simply being able to put my hand in my bag and touch it helped me to feel a bit calmer, but I was told as part of CBT that it wasn’t healthy to over rely on something like that and I should be trying to go out without it. […] It was the same with the over-preparing thing that I was told was counterproductive. […] But I sort of think “I need these things” and I’m being told I shouldn’t be relying on them. So now I feel worse than ever because I feel that I can’t do these things, because the autism is there in the way and I’m never going to get past it. It was kind of affirming you’re a broken person. That was never really something I thought about before going into cognitive behaviour therapy. (P10)
In this example, the individual was using strategies to regulate emotions and compensate for communication differences that the therapist wrongly identified as “safety behaviors.” Autistic people suggested a more helpful behavioral approach in therapy. Rather than making assumptions based on what might be “dysfunctional” in neurotypical people, a therapist might work with the individual’s capacity to build coping behaviors and suggest environmental changes:
The therapist could not understand why my anxiety never reduced when she asked me to make all these phone calls. […] It turns out that the reason is inaccessibility. I can’t understand what the other person is saying due to my auditory processing disorder, and I can’t make a quick response due to my speech issues from being autistic. The solution was not to keep making phone calls and thinking about how phone calls weren’t harmful, but to get an accommodation that lets me do phone calls via reading and typing. Now with that accommodation I can make phone calls on my own which I could not before, and the anxiety is much less intense. […] The issue for autistic people will often be inaccessibility. Accommodations like exemptions from face-to-face requirements/interactions, AAC, sensory aids should be encouraged, not vilified. (P3)
Theme three: Therapy needs to be trauma-informed
Several people stressed the importance of a trauma-informed approach that acknowledged their suffering as an understandable result of distressing experiences. Participants explained that a validating therapeutic relationship helped correct previous traumatizing social interactions. One person shared the following:
We’re not going to be safe until we can resist, reframe, redo the bullying, the lying, the harassment, the toxicity that can develop around us. […] What my therapist did for me is that she one hundred percent respected my reactions, she was totally and utterly curious about my reactions. She did not define any kind of sanity for me. Do you know what I mean? Sometimes certain kinds of therapy, it feels like they’re saying this is how you’re supposed to behave and we’re going to get you to this level. […] But in my therapy the gift she gave was a space where I was fully accepted, fully, deeply, humanly accepted, and that person there to help me shift my distress. And she had this respect for the traumatic aspect of being autistic in a society that has a lot of criteria for certain types of behaviours. (P1)
Theme four: Support may be needed for the social process of therapy
The final theme is about adaptation to the needs and abilities of autistic people, especially in the social process of therapy. Attention to the social process is likely to be especially important in the case of therapy for social anxiety, so it is both accessible and models a healing social interaction. Several participants highlighted how they needed support to process the complexity of the therapeutic situation:
I did not find it particularly useful any of the times I had CBT. They asked me what I wanted to get out of it, I didn’t know, and I don’t think they liked that. I think they needed to take the lead more. […] You have to identify how autism affects the person and adapt the therapy for that. For me, autism means that I sometimes have problems processing information, sometimes I need help figuring out both what the question is, and what the answer is. I say that sort of metaphorically. Sometimes I don’t know what to ask, I need help figuring out what I need to ask, and then I need help figuring out the answer. […] And when you’re asking a question, I might not understand what point it serves. If I sort of understood what was going on, I could help them to help me better. (P12)
A particular aspect of the social situation of therapy that therapists may need to hold in mind is how the autistic person communicates about emotions. One participant shared the following advice to therapists:
Don’t think that their facial expressions and their mannerisms necessarily reflect what’s going on upstairs because they might be masking. Or they might be trying to be their true self, but it might come off as lack of interest. That’s what the therapist said to me, that I wasn’t interested. Or they might be shutting down, there might be something going on and they can’t verbalize it. They can’t say what’s going on. That’s one of the things I found with therapy. There are times when I actually couldn’t tell you what I’m feeling. I think maybe a therapist might need to be mindful of that because it seems like knowing what the feeling is, that’s like the starting line of therapy, and you might not be there. (P7)
Discussion
This study asked autistic people what they perceived to be different about their experience of social anxiety compared with non-autistic people, and what they had experienced of the first-line intervention for social anxiety (CBT for social anxiety). All participants felt that social anxiety needed to be understood through the lens of being an autistic person. They also highlighted that mental health services had frequently not met their needs in treating social anxiety. They felt that the cognitive and behavioral aspects of CBT for social anxiety were often not appropriate to their anxiety, and felt that therapy needed to be trauma-informed.
Experiences of social anxiety from the autistic perspective
The autistic experience of social anxiety was summarized through three themes, which are largely consistent with previous qualitative research documenting the impact of autism-specific and systemic factors on social distress for autistic people.16–17 First, autistic traits are associated with distress in social interactions. This is for several reasons: (1) autistic people may be less equipped to deal with neurotypical social interactions; (2) potentially more vulnerable in social situations; (3) aware they may be negatively judged for their autistic traits; and (4) trying to mask those traits in an attempt to reduce the risk of negative social consequences. Second, social anxiety is associated with the trauma of living in a neurotypical world as an autistic person, where negative social interactions can cause intentional and unintentional harm and can condition an individual to expect distress. Third, anxiety in social situations may arise through nonsocial sources, including sensory and environmental factors, and heightened arousal expressed as “meltdowns,” which lower one’s threshold for dealing with social difficulties and increase the likelihood of being seen as different. Participants in this study highlighted that therapists need to consider these factors as additional contributors to social anxiety over and above what they might consider for other people.
The emphasis that participants placed on trauma was striking; they viewed their social anxiety as “trauma-based.” Distress may be seen as an understandable reaction to the autistic person’s experiences, and their behavior as an adaptation to adversity, in line with the trauma-informed model of mental health. 22 We might wonder whether social anxiety is strictly the best label for autistic experiences of social distress, as social anxiety disorder is diagnosed where social fears are out of proportion to the sociocultural context. 2 For autistic people, the sociocultural context includes prejudicial attitudes that mean others are likely to make negative interpretations of autistic people, 23 as well as a high risk of victimization by others. 24 In this context, it may be reasonable to reframe social anxiety as social trauma. The emphasis on trauma may make us wonder about the prevalence of post-traumatic stress disorder (PTSD) in autistic people, which is under-researched but may be higher than in the general population. 25 Supporting autistic people with trauma-based anxiety may require therapists to draw on therapies for PTSD, although there is currently very limited evidence base for these in autistic people. 26 There may also be a role for interventions focused on stigma, including interventions to support the individual to cope with stigma (e.g., through reframing identity, selective disclosure, and self-advocacy) and systemic intervention to reduce stigma toward autistic people from the wider population; however, there is limited evidence for these interventions. 27 There are lots of unanswered questions: a focus on trauma-informed approaches should be a priority for future autism research, as identified by a priority-setting partnership with the autistic community. 28
Experiences of CBT for social anxiety from the autistic perspective
Past studies have highlighted that autistic people often have poor experiences of mental health services, associated with systemic barriers, low clinician knowledge of autism, and inadequate adaptations to autistic people’s needs.29–30 It has been reported that autistic people often find that CBT offered in services has not met their needs, 30 although the reasons have not previously been explored in detail. This study has started filling that gap. Participants questioned the cognitive and behavioral components of standard CBT for social anxiety—they questioned both the C and the B. They did not agree that their social fears should be framed as “cognitive errors,” as autistic people have real social differences that do impact on interactions and the ways other people respond. This means that exposure to the fear may not reduce anxiety if it is grounded in reality, and attempting to reframe it may give the impression of “gaslighting” if the individual’s social differences are not acknowledged. In addition to the cognitive aspect, autistic people were skeptical of the behavioral aspect of CBT, which involves supporting the individual to drop “safety behaviors” (behaviors that may seem helpful but reinforce anxiety). Autistic people explained how this process of “behavioral modification” sometimes backfired as it removed their coping and forced them to conform to neurotypical norms. Previous qualitative research has documented overlap between coping behaviors, autistic traits, and mental health symptoms, which can lead to confusion and uncertainty in others about the behavior. 31 Therefore, the therapist and the client need to work together to understand the behavior and not just assume it is a “safety behavior.”
Recommendations for therapists
Therapy should be informed by an individualized formulation of the person’s social anxiety. Autistic people in this study could often relate to the Clark and Wells model of social anxiety so this will be a useful starting point in developing a formulation of the person’s experiences. This formulation should be adapted for autistic people to include additional relevant factors, including the influence of the individual’s social differences, the high probability of traumatic social experiences, and the impact of nonsocial factors on social situations. Autistic people explained that gaining an understanding of these factors and the process of social anxiety helped them feel more in control and compassionate toward themselves. This is a trauma-informed approach, which helps a person see there is a logic to their feelings and they do not deserve to feel shame.
In addition, the therapist’s responsibility is to help the individual cope better with social anxiety. This involves working with the person’s limits, within their window of tolerance, and according to their goals to increase their coping skills. This process may differ from therapy for other people; it will be important for the therapist to face discomfort that may come with this, stay curious about what the person will find most helpful, and cultivate a collaborative, exploratory approach with the individual. Typically, in CBT for social anxiety, the therapist supports a person to drop safety behaviors and this may be helpful for autistic people—but it will backfire if the therapist mistakenly encourages the client to drop helpful coping. Therefore, the nature of the behavior needs to be clarified through a careful functional analysis to identify the reasons for and intended/unintended consequences of the behavior, and allow an informed decision about behavior change. More broadly, the most appropriate approach might be to identify the key social situations the person wants/needs to take part in, help them up-skill in coping behaviors, and find environmental adjustments and adaptations to make the situation(s) more accessible.
Limitations
Although individuals were asked in detail about their experiences of therapy, we cannot be fully confident of the nature/quality of interventions described. Individuals could describe interventions they had been offered in detail, and these seemed to be typical CBT. However, there is no way of verifying this. We therefore need to consider the perspectives heard in this study as reflecting experiences of autistic people in routine clinical practice rather than reflecting optimally delivered CBT. In addition, participants took part in different formats of interview according to their communication preferences. They appreciated this: one person said, “I couldn’t have done this without your flexibility.” This is a strength of the study, but potentially impacts the level of detail in interviews (for instance, one asynchronous interview was shorter than other interviews). The researcher did not notice any differences in the analysis process by interview format.
We cannot be confident that views expressed in this study fully represent autistic people. There was an attempt to safeguard against bias by randomly inviting individuals to interview who took part in an initial survey, but not all people consented to be contacted and survey respondents with negative experiences may have been more motivated to participate. In addition, some sample characteristics are not representative of the wider autistic population, as the vast majority were diagnosed as adults, White, and highly educated. The sex/gender ratio also did not reflect the wider autistic community. However, emphasizing the experiences of women and nonbinary people may be appropriate in a study about social anxiety, as social anxiety is more common in women in the general population, 32 and interpersonal traumas (likely a contributing factor to social distress) appear more common in autistic women and gender minorities than autistic men. 33
Lastly, this study focused on perceived differences in experiences of social anxiety, while listening for similarities too. There is a view that anxiety presentations may differ in the autistic compared with non-autistic population,3,15 so the goal was to elaborate these differences from the perspective of autistic people. However, there is a risk when looking through the lens of difference that we overstate differences. This study therefore needs to be seen alongside quantitative studies that give a scale of the similarities and differences. For instance, studies have found that features of the Clark and Wells model—safety behaviors and self-monitoring—are also important in social anxiety in autistic people, as they are in the general population.34,35 In addition, the survey study associated with this research directly compared the Clark and Wells model across autistic and neurotypical people, and found significant overlap, but some differences, in terms of greater social anxiety in autistic people than the model would predict and safety behaviors less predictive of social anxiety in autistic people. 18
Conclusion
In summary, this interview-based study heard from autistic people about their experiences of social anxiety and CBT for social anxiety. This article complements the survey-based part of this project reported elsewhere18,36; it echoes similar themes and develops them in significantly more detail through thematic analysis of extended interviews. This analysis suggested some differences in experience of social anxiety, including impact of autism-specific and broader societal/systemic influences (potentially intersecting with other aspects of a person’s social identity too), to explain why autistic individuals experience elevated anxiety in social situations. In addition, autistic people often described unhelpful experiences with CBT for social anxiety in this study, which appeared to arise from assumptions of the CBT model as well as a need for greater adaptation of how therapy was delivered. Autistic people advised that therapy needs to be trauma-informed and needs to help them find practical ways of navigating social situations with less distress, while being mindful that the social process of therapy will need to adapt around autism. Given the low acceptability of currently available therapy for social anxiety to autistic people, we need further research to develop interventions that are fit for purpose for autistic people.
Footnotes
Acknowledgments
The author warmly thanks all the participants who made this study possible and kindly contributed their time and insights. He also thanks two autistic people who commented anonymously on the interview script and early analysis, and to Autistica who supported with recruitment.
Authorship Confirmation Statement
A.C.W. conceived the study, developed the methods for data collection and analysis, carried out project administration, conducted the interviews, carried out data analysis, wrote and edited the article, and produced the figures. A.C.W., approved of the article before submission. This article has been submitted solely to Autism in Adulthood and is not published, in press, or submitted elsewhere.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.